Article Text

Abstract
INTRODUCTION Erythromycin, a motilin agonist, is a potent prokinetic. ABT-229 is a specific motilin agonist that dose dependently accelerates gastric emptying. Dyspepsia and gastroparesis are common problems in type 1 diabetes mellitus. We aimed to evaluate the efficacy of ABT-229 in symptomatic diabetic patients with and without delayed gastric emptying.
METHODS Patients with type 1 diabetes and postprandial symptoms were randomised (n=270). Based on a validated C13 octanoic acid breath test, patients were assigned to either the delayed or normal gastric emptying strata. Patients received one of four doses of ABT-229 (1.25, 2.5, 5, or 10 mg twice daily before breakfast and dinner) or placebo for four weeks following a two week baseline. A self report questionnaire measured symptoms on visual analogue scales; the primary outcome was assessment of change in the total upper abdominal symptom severity score (range 0–800 mm) from baseline to the final visit.
RESULTS The treatment arms were similar regarding baseline characteristics. There was symptom improvement on placebo and a similar level of improvement on active therapy for the upper abdominal discomfort severity score (mean change from baseline −169, −101, −155, −143, and −138 mm for placebo, and 1.25, 2.5, 5, and 10 mg ABT-229, respectively, at four weeks by intent to treat). The results were not significantly different in those with and without delayed gastric emptying. The severity of bloating, postprandial nausea, epigastric discomfort, heartburn, and acid regurgitation worsened dose dependently in a greater number of patients receiving ABT-229 than placebo. Overall, 63% of patients on placebo reported a good or excellent global response, and this was not different from the active treatment arms.
CONCLUSIONS The motilin agonist ABT-229 was not efficacious in the relief of postprandial symptoms in diabetes mellitus in the presence or absence of delayed gastric emptying.
- prokinetic
- motilin
- dyspepsia
- gastric motility
- type 1 diabetes
- controlled trial
- postprandial
Abbreviations used in this paper
- HbA1c
- glycated haemoglobin
Statistics from Altmetric.com
Motilin is a 22 amino acid peptide hormone that is expressed throughout the gut.1 Motilin stimulates interdigestive antral contractions promoting gastric emptying; the receptor has recently been identified.2 Erythromycin is a potent motilin agonist, inducing phase 3 of the migrating motor complex1; it accelerates gastric emptying in healthy volunteers as well as in patients with diabetic gastroparesis or those post-vagotomy.3 ,4
Dyspepsia is a common problem in patients with diabetes mellitus.5 ,6 Between 27% and 58% of type 1 diabetics are reported to have gastroparesis, usually affecting solids but less often liquids.7 ,8 Symptoms of diabetic gastroparesis include postprandial distress, early satiety, bloating, fullness, and nausea and vomiting, but while gastroparesis is common, only a minority have overt symptomatology.7 ,8 Moreover, these symptoms also occur frequently in diabetics who do not have objective evidence of gastroparesis.6 The underlying mechanisms remain in dispute but disturbed vagal parasympathetic function and poor glycaemic control may both be important.8 ,9 In addition, increased levels of motilin have been observed in diabetic gastroparesis which is likely to be a compensatory mechanism as motilin levels decreased with the introduction of a prokinetic.10 A prokinetic agent in diabetic gastroparesis has the potential to increase gastric emptying, improve dyspepsia, and better control plasma glucose levels.
There has therefore been considerable interest in developing new prokinetics for gastroparesis, including motilin agonists that lack antibiotic activity. ABT-229 has potent motilin agonist activity with essentially no antibiotic action.11 ,12 It dose dependently accelerates gastric emptying, and has a half life of 20 hours.11 ,12 Multidose studies have shown that the maximally effective dose was 5 mg twice daily for accelerating gastric emptying and 2.5 mg twice daily retained a modest but significant prokinetic effect.12
We aimed to test the hypothesis that ABT-229 would relieve postprandial symptoms in patients with diabetes mellitus. We further hypothesised that the maximum therapeutic gain over placebo would be observed in patients with diabetic gastroparesis on higher doses of ABT-229. To test these hypotheses, we conducted a randomised, placebo controlled, dose ranging trial in North American patients with type 1 diabetes mellitus.
Methods
The trial was approved by the local institutional review boards, and all patients gave informed consent.
PATIENT SELECTION
Ambulatory patients at least 18 years of age with documented type 1 diabetes were eligible to be enrolled. All patients were by definition insulin dependent. A minimum three month history of chronic upper abdominal discomfort (that is, one or more of postprandial fullness, bloating, epigastric discomfort, early satiety, belching after meals, postprandial nausea, vomiting, or epigastric pain) was required. A total of 383 patients were screened (by 33 investigators in the USA and three in Canada between June 1997 and August 1998) (fig 1). Patients were required to have a normal upper endoscopy (that is, no ulcers or erosions in the oesophagus and gastroduodenum) in the three months before randomisation. Furthermore, during the baseline evaluation over 14 days, patients had to have experienced one or more symptoms of postprandial upper abdominal discomfort on three or more days per week and on average have sufficiently severe symptoms (defined as an upper abdominal discomfort severity score of >149 mm and a postprandial fullness severity score of >29 mm on visual analogue scales, as described below). Patients were only enrolled if there were no serious comorbid illnesses and screening laboratory values were normal.
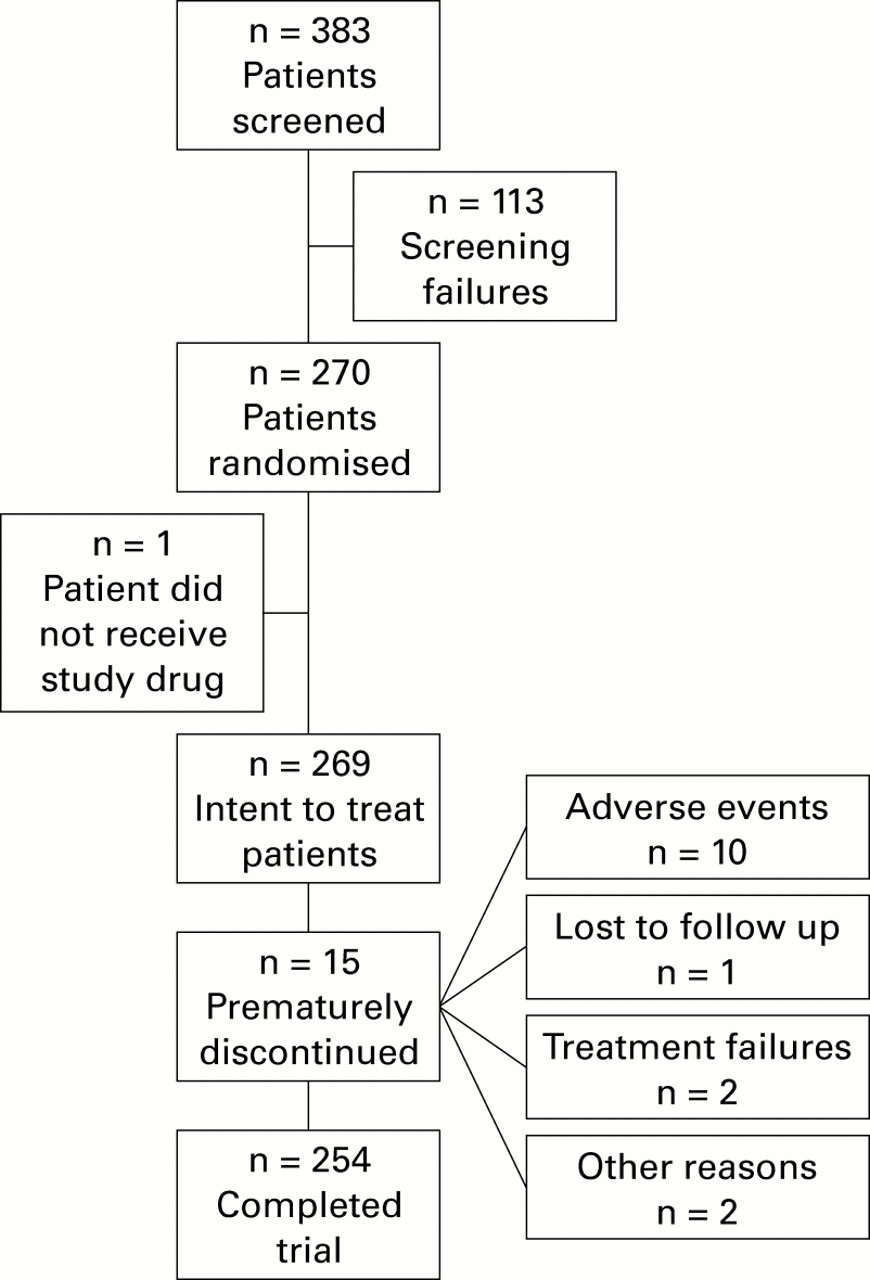
Patient flow chart.
Excluded were patients with gastro-oesophageal reflux disease, based on a normal endoscopy (only erythema was permitted), and patients with predominant symptoms of irritable bowel syndrome. Use of prokinetic or antisecretory agents within 72 hours of the screening period or during the trial was not permitted. Occasional non-steroidal anti-inflammatory drug use (<11 days per month) or aspirin (<101 mg daily) was allowed. A history of recent peptic ulceration (in the past five years if noHelicobacter pylori treatment had been received or one year if treated for H pylori) was an exclusion criterion. Patients with other serious diseases (including alcoholism and drug dependence, any bowel surgery, or malignancy) were excluded.
Overall, 113 patients were excluded on screening (20 ulcer or erosions, 11 other illnesses, eight other medications, 16 inadequate symptom level, two inadequate completion of the diary card, and the remainder miscellaneous other reasons).
RANDOMISATION
Each site was supplied with separate sets of study drug for the gastric emptying strata (normal and delayed); to ensure random assignment, patients in each strata were given a number in sequential order from a separate computer generated randomisation list.
A total of 270 patients were randomised but one was lost to follow up after the drug was dispensed and this patient was excluded. Patients treated (n=269) were randomly assigned to receive ABT-229 1.25 mg (n=55), 2.5 mg (n=58), 5 mg (n=53), 10 mg (n=55), or placebo (n=48) twice daily before breakfast and dinner for four weeks. These four doses were chosen based on the gastrokinetic effects of ABT-229 administered in healthy subjects.12 The 2.5 mg twice daily dose was only marginally significantly superior to placebo as it accelerated gastric emptying of the evening meal only. The maximally effective dose in healthy subjects was 5 mg twice daily. As the gastrokinetic effects of ABT-229 were largest in those with slower gastric emptying, a 1.25 mg dose was included in the trial. To account for the possibility that patients with diabetic gastroparesis might be more resistant to therapy and require a higher dose, 10 mg was also included. Overall, 15 patients prematurely discontinued; the reasons were adverse events (n=10), treatment failure (n=2), lost to follow up (n=1), or other reasons (n=2), and the distribution was similar in each arm (fig 1). In total, 254 patients completed the trial.
BLINDING
The placebo was identical in appearance to active therapy. All medication was supplied in double blinded multidose bottles. An administrative blind break occurred for one patient.
COMPLIANCE
Compliance, measured by a tablet count at week 4, was excellent. A minimum of 97% of patients in each treatment arm were at least 75% compliant.
ASSESSMENT OF GASTRIC EMPTYING
A standardised C13 octanoic acid breath test was used to stratify patients during screening.12-16 After fasting for 12 hours, patients consumed a 420 kcal breakfast meal comprising 50 g of ham, one fried egg, 10 g of butter, two slices of white bread, 100 ml of orange juice, and 100 ml of water (45% carbohydrates, 37% fat, and 18% protein), administered in an upright sitting position in 10 minutes. Breath samples were obtained 10 minutes before the meal and every 10 minutes for the first two hours, and then every 15 minutes for a further two hours. Breath samples were analysed at a central laboratory. In a healthy adult reference population in the USA (n=50, Abbott Laboratories, Abbott Park, Illinois, USA, data on file) using the same meal, the mean t50 was 130 (50) minutes and the 90th percentile was 193 minutes; definite delayed gastric emptying in this trial was defined a priori as >192 minutes. Overall, 29% of patients had definite delayed gastric emptying by these criteria, which are conservative, and this was similar across treatment arms. The breath test has been validated in 19 insulin dependent diabetics against scintigraphy using the same meal; the correlation coefficient for t50 was 0.73 (p<0.001) (Abbott Laboratories, data on file).
OUTCOME ASSESSMENTS
Patient symptom questionnaire
At baseline, and at two and four weeks, all patients completed a self report measure of the severity, frequency, duration, and impact of meal related symptoms over the prior two weeks. The eight target symptoms were postprandial fullness, early satiety, bloating, epigastric discomfort (an ache or discomfort after eating, poorly localised), epigastric pain (a sharp, easy to pinpoint pain after eating), postprandial nausea, belching after meals, and vomiting. Severity was scored for each symptom on a 100 mm visual analogue scale. The primary outcome was defined a priori as the sum of the severities of the eight symptoms, to create the total upper abdominal discomfort severity score (minimum 0, maximum 800 mm). Defining each symptom in lay person terms standardised the questionnaire. A visual analogue scale is sensitive to change and is well accepted as a tool for evaluating dyspepsia.17
Measured also were symptom frequency (from none to every day) and impact (from not at all bothersome to extremely bothersome) on five graded Likert scales, as well as duration (from not at all to continuous or almost continuous) on a seven graded Likert scale.
Patient diary
Patients completed a daily diary during the run in baseline and treatment periods. The severity of postprandial fullness, bloating, epigastric discomfort, and postprandial nausea were recorded on seven graded Likert scales from absent to cannot be ignored, prompt advice sought. The diary card assessments had been previously validated.17
Global evaluation
At week 4, patients rated the efficacy of treatment as follows: excellent (complete or near complete resolution of symptoms), good (distinct improvement), moderate (some improvement), or poor (no change or deterioration).
Glycaemic control and all other measures
Before randomisation, a serum glucose level was measured (mg/dl) by a central laboratory after fasting for 12 hours. During therapy, patients were required to conduct daily home glucose monitoring before breakfast, lunch, dinner, and bedtime, using their own monitoring system, and record the data in their diary. Glycated haemoglobin (HbA1c) levels were also measured at baseline and at the end of treatment (normal range 4.3–5.8%). A 12 lead ECG was performed at baseline and at the final visit.
STATISTICAL ANALYSES
Primary analyses were conducted on patients who received at least one dose of study medication, and who had a baseline and at least one follow up symptom assessment no more than five days after the last dose (intent to treat). All p values calculated were two tailed; the alpha level of significance was set at 0.05.
Baseline comparability among treatment groups was assessed by one way ANOVA for continuous variables and by Fisher's generalised exact test for categorical variables.
For the upper abdominal discomfort score, the sum of symptom severity scores from the patient diary, and severity scores for individual symptoms, treatment differences at baseline and for change from baseline were assessed by two way ANOVA, with factors for treatment, investigator, and treatment by investigator interaction. A linear dose-response was tested within the framework of multiple regression.
Treatment differences in the percentage of patients with worsened severity for individual symptoms were assessed by a Cochran-Mantel-Haenszel test with investigators as strata. Treatment differences for global efficacy variables were also assessed by the Cochran-Mantel-Haenszel test with investigators as strata.
A sample size of 50 patients per treatment arm was calculated to provide more than 80% power (using a two sided 0.05 level of significance) to detect a standardised treatment difference of 0.56 (the expected treatment difference divided by the standard deviation). A standardised treatment difference of greater than 0.56 was observed in previous studies testing cisapride,18 and a larger difference was considered reasonable to expect with ABT-229 in the absence of better estimates.
Results
BASELINE CHARACTERISTICS BY TREATMENT ARM
Baseline demographic characteristics, gastrointestinal symptoms, and history of diabetic complications were generally similar in each treatment arm (table 1). Mean age of the study population was 45 years; 66% were females and 89% were White. Mean height and weight were 169 cm and 77 kg, respectively. Mean age at diagnosis of diabetes was 23 years, and mean number of years since diagnosis was 22 years. Overall, 22% were smokers. The majority of patients had a history of peripheral neuropathy (59%) which was not different across the treatment arms but autonomic neuropathy differed among the treatment groups (table 1). The total upper abdominal symptom severity score was significantly higher in those with a history of one or more diabetic complications (mean score (SEM) 382 (10.2)) compared with those who had no complications (mean score 326 (15.1); p=0.005). The prokinetic agents cisapride, metoclopramide, and erythromycin had been used in the past two years by 46%, 24%, and 10%, respectively, but use was reasonably similar across the treatment arms. A good or excellent response to previous use of cisapride, metoclopramide, and erythromycin was reported by 23%, 16%, and 22%, respectively, and a moderate response by 48%, 33%, and 33%, respectively. The distribution of half gastric emptying times in the total patient cohort is shown in fig2.
Baseline characteristics of the intent to treat study population

Distribution of gastric emptying half times (t½) in the study population.
PATIENT SYMPTOM QUESTIONNAIRE
The total upper abdominal discomfort severity score, the primary outcome, decreased in all treatment arms from baseline, based on the intent to treat analysis (fig 3). There were no significant differences between each of the active treatment arms and placebo for mean change from baseline to week 2 or week 4 (table 2).
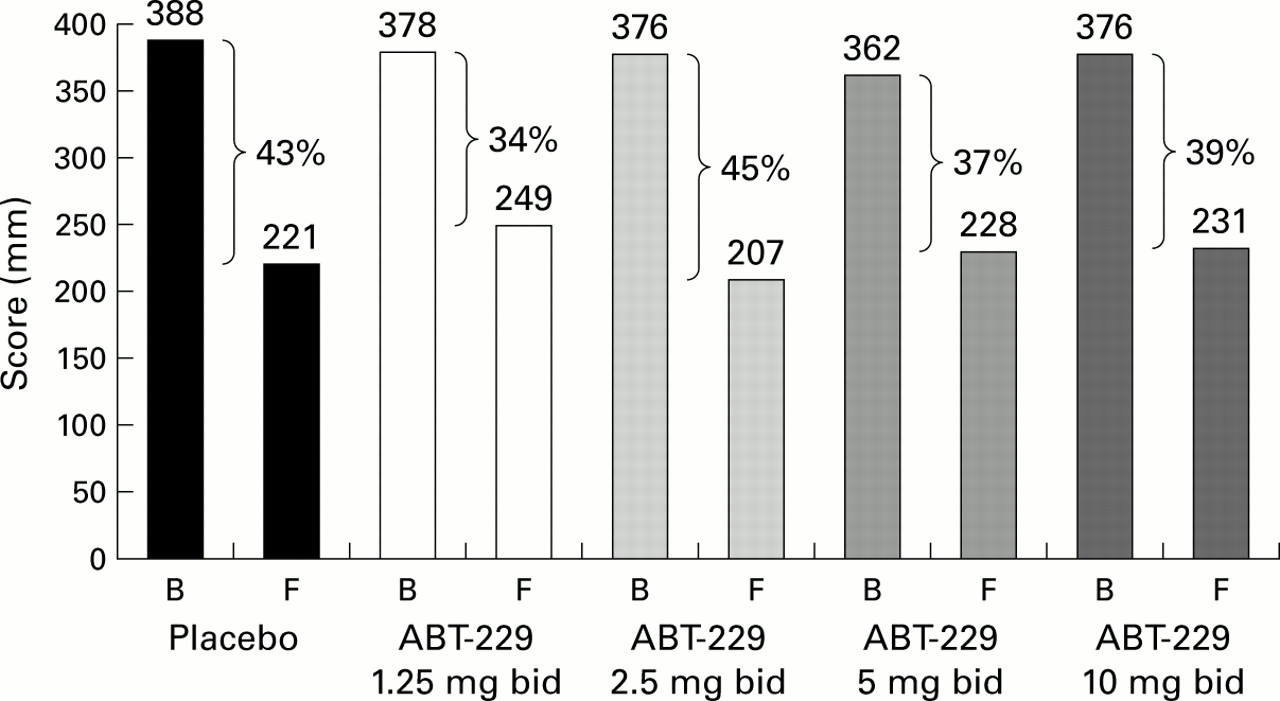
Mean upper abdominal discomfort score on combined visual analogue scales (mm) at baseline (B) and at the four week (final (F)) visit in each treatment arm.
Mean change in symptoms from baseline (intent to treat)
Improvement in the total upper abdominal symptom severity over baseline scores was 37%, 34%, 31%, 29%, and 37% with placebo, and 1.25, 2.5, 5.0, and 10.0 mg of ABT-229, respectively, in patients with delayed gastric emptying. Patients with normal gastric emptying had even less improvement with the highest dose of ABT-229 (41%, 29%, 39%, 39%, and 22%, respectively, for placebo, and 1.25, 2.5, 5.0, and 10.0 mg of ABT-229) (table 2).
Almost identical results were observed applying a per protocol analysis. There was no treatment by investigator interaction, and there was no significant dose-response relationship including or excluding placebo.
When individual symptoms were analysed, ABT-229 was not superior to placebo; indeed, the severity of bloating, postprandial nausea, epigastric pain, heartburn, and acid regurgitation worsened dose dependently in a greater number of patients receiving ABT-229 than placebo (table 3).
Change in symptom severity score two weeks after treatment initiation, measured by patient symptom questionnaire (visual analogue scale, VAS): % of patients whose severity score changed
PATIENT DIARY
Diary data suggested an inverse dose-response relationship for the severity of fullness, epigastric bloating, epigastric discomfort, and postprandial nausea; the sum of their scores decreased by 42% over baseline for placebo, and by 30%, 36%, 35%, and 26% for 1.25, 2.5, 5.0, and 10.0 mg of ABT-229, respectively. There were no significant differences detected between placebo and any treatment group for the sum of the symptom severity scores, averaged over 14 day periods, except for 10 mg of ABT-229 which was significantly worse than placebo throughout the trial (fig 4). There was no significant interaction between investigator and treatment for mean change in baseline symptom scores to final evaluation. In the initial two week treatment period, epigastric discomfort severity scores were significantly worse for 10 mg of ABT-229 than placebo (p<0.05). Similarly, the improvement in postprandial fullness tended to be significantly less in the 10 mg ABT-229 arm than in the placebo group throughout the trial, and this difference was statistically significant in patients with normal gastric emptying (p<0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change from baseline for the sum of daily severity scores for fullness, bloating, epigastric discomfort, and postprandial nausea from the patient diary in the placebo and ABT-229 10 mg groups.
GLOBAL EFFICACY
A similar percentage of patients on placebo reported a good to excellent response (63%) compared with the 1.25 mg (54%), 2.5 mg (65%), 5 mg (59%), and 10 mg doses (52%) of ABT-229.
GLYCAEMIC CONTROL, AUTONOMIC NEUROPATHY, AND OUTCOME
In secondary analyses, potential confounders were evaluated. Serum glucose levels and HbA1C at baseline were strongly correlated (Spearmanr=0.42; p<0.0001). There was no significant correlation between baseline HbA1C and the baseline upper abdominal symptom score (r=−0.09, p=0.15). The upper abdominal discomfort score was weakly negatively correlated with baseline fasting serum glucose levels (r=−0.17, p=0.007). There was no evidence of correlation between change in upper abdominal symptom score when expressed as either absolute change or percentage change and corresponding changes in blood glucose or HbA1C (when expressed as either absolute change or percentage change) in the placebo (−0.05 ⩽ r ⩽ 0.21; all p>0.1), 1.25 mg (−0.23 ⩽ r ⩽ 0.15; all p>0.1), 2.5 mg (−0.05 ⩽ r ⩽ 0.15; all p>0.1), 5 mg (−0.10 ⩽ r ⩽ 0.05; all p>0.4), or the 10 mg (0.03 ⩽ r ⩽ 0.15; all p>0.3) treatment groups. There was no significant treatment difference between any ABT-229 dose and placebo when stratifying for the presence or absence of autonomic neuropathy (defined as present or absent by the investigator).
SAFETY
All doses were well tolerated, and side effects were similar across the treatment arms. Headache, nausea, vomiting, abdominal pain, diarrhoea, infection, and hypoglycaemia were the most common adverse events. Study treatment was discontinued because of adverse events in only four patients on placebo and five on active treatment. The QT interval (normal defined as <450 ms) was not significantly prolonged from baseline in any of the treatment groups.
Discussion
Between 27% and 58% of type 1 diabetics have gastroparesis7 ,8 ,19-21 although the condition is not associated with a poorer prognosis.22 The risk of delayed gastric emptying is considered to be increased in those with type 1 diabetes of more than 10 years' duration who also have peripheral or autonomic neuropathy.7 Baseline symptoms correlate poorly with gastroparesis in diabetes but acceleration of gastric emptying is considered central to the management of dyspepsia in diabetes.23 In an open study of 24 patients with gastroparesis followed for two years, cisapride improved gastric emptying in 10 patients and seven showed a greater than 20% improvement in overall symptom score.24 However, only a minority had diabetic gastroparesis and no control group was evaluated.24 Other placebo controlled studies of prokinetics in type 1 diabetes however have been more disappointing.25
Erythromycin appears to be a more potent prokinetic than cisapride, domperidone, or metoclopramide.26 ABT-229 is similarly a potent promotility agent.12 ,27 The current trial results however suggest that ABT-229 does not relieve meal related upper gastrointestinal symptoms in type 1 diabetes mellitus. Indeed, the symptom outcomes were similar regardless of whether there was delayed or normal gastric emptying in this population. ABT-229 worsened the severity of fullness, bloating, epigastric discomfort, postprandial nausea, heartburn, and acid regurgitation in one third to a half of patients, and on average did so in twice as many patients compared with placebo. While the 1.25 mg dose was significantly less detrimental for bloating than the other doses, this may represent a chance finding (because of multiple comparison testing). The data were consistent regardless of the outcome assessments applied, and adjustment for possible confounders did not alter the conclusions. We chose doses based on preliminary data clearly demonstrating a dose dependent acceleration of gastric emptying in healthy subjects.12 In these studies, twice daily dosing with 5 mg of ABT-229 accelerated gastric emptying at breakfast, lunch, and dinner; three times daily dosing on 5 mg or higher doses were not more effective.12There is also no evidence that the effect of ABT-229 is subject to tachyphylaxis.12 Therefore, we do not consider it likely that incorrect doses were chosen for testing. While an evaluation of gastric emptying was not repeated on treatment, which is a limitation of the present study, a high enough dose was chosen to ensure a gastrokinetic effect. Moreover, in case this prokinetic drug was more potent in the diseased stomach than in health, a very low dose was also chosen.
Gastrointestinal symptoms in diabetes are usually attributed to disordered motor function, secondary to irreversible autonomic (vagal) neuropathy.7 However, symptoms tend to correlate poorly with the rate of gastrointestinal transit,28 and indeed in the present study only approximately one in four symptomatic patients had definite gastric emptying delay. The C13 octanoic acid breath test is considered less accurate than scintigraphy but the test does provide reasonably accurate intraindividual comparisons in diabetics, and is non-invasive.14 ,15 ,28 There is evidence that blood glucose concentration can influence upper gut motor function and symptoms such as fullness and nausea.29 ,30We found no significant correlation between changes in symptom scores on treatment and changes in glycaemic control, as measured by HbA1C or recorded blood glucose levels on therapy. No association between symptom outcome and diabetic complications was observed although the baseline total upper abdominal symptom severity score was modestly higher in those with diabetic complications. However, data on diabetic complications (autonomic neuropathy, peripheral neuropathy, renal insufficiency, and retinopathy) relied on the judgement of the attending endocrinologist, and therefore the study may have underestimated the prevalence.
In a negative study, the possibility of a type II error needs to be considered. The present study was, we believe, adequately powered. Although few data are available to accurately estimate the likely therapeutic gain, the study was powered to detect a therapeutic gain similar or superior to that reported for cisapride in dyspepsia. Hence we cannot dismiss having missed a small effect but this is unlikely to be of clinical significance. The gastrokinetic effects of erythromycin may be less during hyperglycaemia than euglycaemia31 ,32and theoretically prokinetics may alter glycaemic control33 ,34 but this was not observed in the present trial. Because even high doses of ABT-229 were not efficacious and we found no association between glycaemic control levels and treatment outcome, any such bias is unlikely to explain the negative results.
Mechanisms that may be relevant to the generation of dyspepsia in diabetes include slow gastric emptying, changes in antral or fundic tone associated with an abnormal meal distribution, and visceral hypersensitivity.35-37 It is conceivable that ABT-229 did not relieve dyspepsia in this study, despite probably increasing gastric emptying, primarily because it failed to enhance fundic relaxation.38 Failure of fundic relaxation appears to be an important mechanism in a subset of patients with functional dyspepsia,35 and may also be relevant in patients with diabetes who have vagal neuropathy but normal gastric sensation.39 Erythromycin has been shown to enhance fasting gastric tone at low dose but at high dose reduced the duration of meal induced relaxation.40 While similar data are not available for other specific motilin agonists, it is likely they also impair fundic relaxation; indeed, ABT-229 was not efficacious in functional dyspepsia in a recent large randomised controlled trial.41
In conclusion, in patients with type 1 diabetes and postprandial distress, the prokinetic ABT-229 failed to provide symptomatic relief compared with placebo. At the highest gastrokinetic dose of 10 mg twice daily, ABT-229 appeared to worsen the severity of most symptoms in up to half of the patients. The results suggest that prokinetic therapy with the new specific motilin agonist drug class will not be of value in diabetic dyspepsia.
Acknowledgments
This study was sponsored by Abbott Laboratories, Abbott Park (Illinois, USA). The assistance of Patricia Wozniak with the statistical analyses is gratefully acknowledged. The following investigators contributed patients to this trial: N Chiba MD, Raleigh, Ontario, Canada; B A Connor MD, New York, USA; M D Dalton MD, Fort Worth, Texas, USA; J M Dorf MD, FCCP, Chicago, Illinois, USA; A Dubois MD, PhD, Bethesda, Maryland, USA; R N Fedoriak MD, FRCP (C), FACP, Alberta, Canada; R S Fisher MD, Philadelphia, Pennsylvania, USA; R Gilbert MD, Boston, Massachusetts, USA; J M Gordon MD, Cleveland, Ohio, USA; R Hardi MD, PC, Chevy Chase, Maryland, USA; J Johanson MD, Rockford, Illinois, USA; D G Kogut MD, Statesville, North Carolina, USA; D G Mangels, MD, Cincinnati, Ohio, USA; J R Mathias MD, Houston, Texas, USA; P B Miner Jr MD, Oklahoma City, Oklahoma, USA; P Molloy MD, Pittsburgh, Pennsylvania, USA; J S Morgan MD, Asheville, North Carolina, USA; J Muchmore MD, Oklahoma City, Oklahoma, USA; B Overholt MD, Knoxville, Tennessee, USA; P Poitras MD, Quebec, Canada; E B Portnoy MD, Westlake Village, California, USA; C Schmitt MD, Chattanooga, Tennessee, USA; H I Schwartz MD, Miami, Florida, USA; S Schwartz MD, San Antonia, Texas, USA; L J Siegel MD, San Antonio, Texas, USA; W Snape MD, Long Beach, California, USA; C A Sninsky MD, Gainesville, Florida, USA; E E Soffer MD, Cleveland, Ohio, USA; R Summers MD, Iowa City, Iowa, USA; A Thannoun MD, Amarillo, Texas, USA; G Tougas MD, CC, Ontario, Canada; A Wald MD, Pittsburgh, Pennsylvania, USA.
Conflict of interest: N Talley received a research grant from Abbott.
Abbreviations used in this paper
- HbA1c
- glycated haemoglobin