Article Text

Abstract
BACKGROUND AND AIMS The pulmonary symptoms of patients with lung disease may be ascribed to gastro-oesophageal reflux although a causal relationship between acid reflux and coughing or wheezing has not been proved. Does cough cause reflux or does reflux cause cough? The aim of this study was to evaluate 24 hour oesophageal pH tracings of asthmatics with gastro-oesophageal reflux to determine the temporal association between acid reflux and coughing or wheezing.
METHODS The oesophageal tracings of 128 asthmatics from the outpatient clinics who underwent oesophagogastroduodenoscopy, oesophageal manometry, and 24 hour oesophageal pH monitoring were analysed. Three possible temporal relationships between the occurrence of acid reflux and the occurrence of coughs or wheezes were evaluated: (1) pulmonary symptoms preceding reflux; (2) reflux preceding pulmonary symptoms; and (3) unrelated occurrence of both events.
RESULTS Of 128 asthmatics, 53 recorded five or more coughs and 19 recorded three or more wheezes during the 24 hour recording period. Mean acid contact time was similar in asthmatics with and without pulmonary symptoms (12.2 (1.2)% v 10.4 (0.6)%). Of all coughs and wheezes, 46% and 48%, respectively, were associated with acid reflux. For the individual asthmatic, the likelihood of reflux induced coughing increased as the number of coughs increased.
CONCLUSIONS Half of all coughs and wheezes in asthmatics are associated with acid reflux into the oesophagus. While an occasional coughing episode can lead to reflux, it is rather the reflux episode in the vast majority of instances that leads to cough.
- asthma
- gastro-oesophageal reflux disease
- erosive oesophagitis
- oesophageal pH monitoring
- lung disease
- pulmonary symptoms
Abbreviations used in this paper
- GORD
- gastro-oesophageal reflux disease
- FEV1
- forced expiratory volume in 1 s
Statistics from Altmetric.com
- asthma
- gastro-oesophageal reflux disease
- erosive oesophagitis
- oesophageal pH monitoring
- lung disease
- pulmonary symptoms
Gastro-oesophageal reflux is common in asthmatic patients, and an increased prevalence of gastro-oesophageal reflux disease (GORD) has been observed in both children and adults with asthma.1-6The association between GORD and pulmonary disease is further supported by the reduction or even disappearance of asthmatic symptoms after surgical or medical treatment of acid reflux.7-11Similarly, there is a group of patients in whom medical control of their pulmonary disease also decreases gastro-oesophageal reflux.12 Using prolonged oesophageal pH monitoring in a group of 102 patients with chronic cough, Irwin et al attributed the cough to asthma in 24% of patients and to gastro-oesophageal reflux in 21%.13 In 43% of GORD patients, cough was the sole clinical manifestation.13 Inget al also used prolonged oesophageal pH monitoring to show that chronic persistent cough without obvious pulmonary aetiology was likely to be associated with episodes of otherwise asymptomatic gastro-oesophageal reflux.14
Two mechanisms have been postulated by which GORD may induce asthma: firstly, microaspiration of gastric refluxate into the lung causing an exudative mucosal reaction; and secondly, a vagally mediated distal oesophageal-tracheobronchial reflex leading to bronchospasm.15 ,16 Likewise, cough from any cause can precipitate gastro-oesophageal reflux.15 Both coughing and wheezing cause an increase in intra-abdominal pressure which in turn may promote movement of gastric contents into the oesophagus. Indeed, intentional methacholine induced bronchospasm increases gastro-oesophageal reflux in asthmatic patients,17 and hyperinflation during episodes of dyspnoea facilitates gastro-oesophageal reflux by changing the relationship between the diaphragm and the lower oesophageal sphincter. Several investigators have proposed a self perpetuating positive feedback cycle between cough and gastro-oesophageal reflux during which coughing or wheezing leads to reflux, and reflux in turn leads to coughing or wheezing.15
Although in certain patients with lung disease, pulmonary symptoms can be unequivocally ascribed to gastro-oesophageal reflux, the extent of the relationship between acid reflux and coughing or wheezing has remained unclear. Does cough cause reflux or does reflux cause cough? If both scenarios are possible, which one is dominant, causing most of the morbidity? The aim of our study was to evaluate 24 hour oesophageal pH tracings of asthmatics to determine the nature of the relationship between acid reflux and coughing or wheezing.
Methods
PATIENTS
A total of 128 pH tracings from 134 consecutive asthmatics (six patients refused) who were selected from the medicine and pulmonary outpatient clinics of the Veterans Affairs Hospital in Hines, Illinois were analysed. Asthma was defined as discrete episodes of diffuse wheezing and either a 20% improvement in forced expiratory volume in 1 s (FEV1) following bronchodilator administration or a 20% decrease in FEV1 after methacholine broncho-provocation performed in accordance with the American Thoracic Society guidelines.18 The presence of reflux symptoms or severity of pulmonary symptoms were not used as criteria for the recruitment of patients into the study. Endoscopy and pH metry were performed only after medical management of asthma had been optimised. Patients whose pH testing was performed within a few weeks of an asthma attack were not included. During the study, patients maintained their regular pulmonary medications. A standardised questionnaire was used to obtain a history from each patient regarding demographic characteristics, social habits, and intake of medications. None of the patients was treated with antisecretory medications prior to endoscopy and pH metry. Bronchodilators were used by 72% of patients at the time of the study. Patients who smoked cigarettes or drank alcohol during the 12 months preceding the interview were considered active smokers or drinkers. Lifetime consumption of cigarettes and alcohol was recorded as pack years and ounce years, respectively. All patients underwent oesophagogastroduodenoscopy, oesophageal manometry, and oesophageal 24 hour pH metry as part of a Veterans Affairs study that was funded to determine the effect of gasto-oesophageal reflux treatment on asthma. The study was approved by the human studies committee of the Hines VA Hospital and VA Central Office.
ENDOSCOPY
All endoscopies were performed by two endoscopists (TGS and SJS) using a set of predefined criteria to record abnormalities of the upper gastrointestinal tract. A diagnosis of erosive oesophagitis was made if endoscopy revealed an exudative break in the squamous epithelium. Oesophagitis was graded based on the scoring system developed by Hetzel and colleagues.19 A hiatus hernia was diagnosed if during quiet respirations gastric folds were seen extending at least 2 cm above the diaphragmatic hiatus.
OESOPHAGEAL MANOMETRY AND pH METRY
The manometric studies were performed after an overnight fast using a solid state catheter (Narco, Houston, Texas, USA). A transnasal catheter was passed in the supine position. The recording sites were positioned across the gastro-oesophageal junction in such a way that the most distal site was in the stomach, the most proximal site was in the distal oesophagus, and the recording sites came to lie within the lower oesophageal sphincter. The location of the sphincter was defined as the area of sustained elevation of the resting pressure that relaxed during swallowing. When resting pressure was not elevated, the point of initial peristalsis, as determined on withdrawal of the catheter, was used to define the lower oesophageal sphincter area. End expiratory pressure of the lower oesophageal sphincter was calculated as the average of five individual measurements. Mean resting pressure of the upper oesophageal sphincter, mean oesophageal contraction amplitude in the body and the distal section of the oesophagus, and percentage of peristaltic contractions in response to 5–10 ml of swallowed water were determined following previously described methodology.20
Before the actual pH metry, patients were scheduled to meet with the nurse coordinator for a two hour structured teaching session. Patients were taught on an individual basis how to use the digitrapper for symptom recording. During the training session, which included multiple simulated events, patients gained experience in activating the event monitor to discriminate between coughs, wheezes, heartburn, and other symptoms. They were instructed to remain upright (sitting, standing, or walking) during the day and to assume the supine position only when in bed during the night. Supine and upright positions were recorded by using a separate switch on the recorder. Patients were further instructed to eat their regular meals during breakfast, lunch, and dinner, and to refrain from all other food intake, including bedtime snacks. A detailed diary was kept to record all events, symptoms, meals, and body positions.
The standard method of determining ambulatory 24 hour acid reflux was used. The model 700 Gastroreflux Recorder (Del Mar Avionics) was used to determine the presence of acid in the oesophagus. After calibration, a transnasal pH electrode (Beckman No 39043; Fullerton, California, USA) was passed and positioned 5 cm above the superior border of the manometrically determined lower oesophageal sphincter. The degree of reflux was determined by continuous sampling and storage at six second intervals if pH <4.0 and at 30 second intervals if pH >4.0. After the test, the recorder was connected to a Gastroreflux Data Analyzer computer. All episodes of acid reflux were reported in both tabular and graphic printouts. Because of potential technical errors (for example, forgetting to change the upright/supine switch or accidentally disconnecting the lead wire, which could lead to erroneous interpretation of data), all recorder generated data were verified by a detailed review of the graphic form of the printout in the presence of the patient. Problems with inconsistencies were resolved by direct interview of the patient and analysis of the diary.
STATISTICAL ANALYSIS
A reflux episode was defined as a drop in pH to values <4 that lasted for more than 10 seconds. The acid contact time was calculated as the percentage of the total 24 hour period with pH <4. A cough or wheeze was considered to have occurredbefore a reflux episode if the cough or wheeze indicator was activated at any point within the two minute period prior to a pH drop to <4. A cough or wheeze was considered to have occurred after the beginning of a reflux episode if the cough or wheeze indicator was activated during a reflux episode up to and including the two minute period after pH had returned to 4. The two minute periods preceding and following the actual reflux episode were chosen to allow for a potential delay in the actual impact of the recording of coughing, wheezing, and acid reflux. (Lam et al showed that in the symptom analysis of 24 hour oesophageal pH data, a two minute time window preceding the onset of a symptom event provided the most reliable results.21 ,22 Other investigators considered temporal associations between reflux events and symptoms as long as five and 10 minutes.23 ,24) In a sensitivity analysis therefore the lengths of both latency periods were varied between one and 10 minutes. Coughs and wheezes that fell outside the extended reflux episode period were considered to have occurred independently of acid reflux. More than one cough or wheeze recorded within a two minute period was considered as a single episode of cough or wheeze.
For each patient, the number of reflux episodes followed by coughs was expressed as the fraction of all reflux episodes during the entire recording time. For each patient, the number of coughs preceding or following a reflux episode was also expressed as the fraction of all coughs occurring during the entire recording time. In a patient with a single cough, the temporal relationship of the cough to acid reflux could result only in an association of 0% or 100%. To avoid such error ridden extremes and to capture a more representative value for the potential associations, only patients with five or more coughs during the recording time were included in the analysis. In the sensitivity analyses, the threshold for patient inclusion for coughing was varied between five and 35 coughing episodes, and for wheezing between three and 10 wheezing episodes. The values of association between coughing or wheezing and acid reflux in individual patients were then used to calculate a population mean.
In each patient, the observed fraction of coughspreceding orfollowing a reflux episode was compared with the expected fraction of each such association. The expected fraction of coughs occurring during or shortly after a reflux episode corresponded to the total acid contact time (percentage of time pH <4). The expected fraction of reflux episodes occurring during or shortly after a coughing episode corresponded to the overall fraction of time spent coughing. The statistical significance of the average ratio R of observed over expected association in the entire patient population was assessed using a z test.
Results
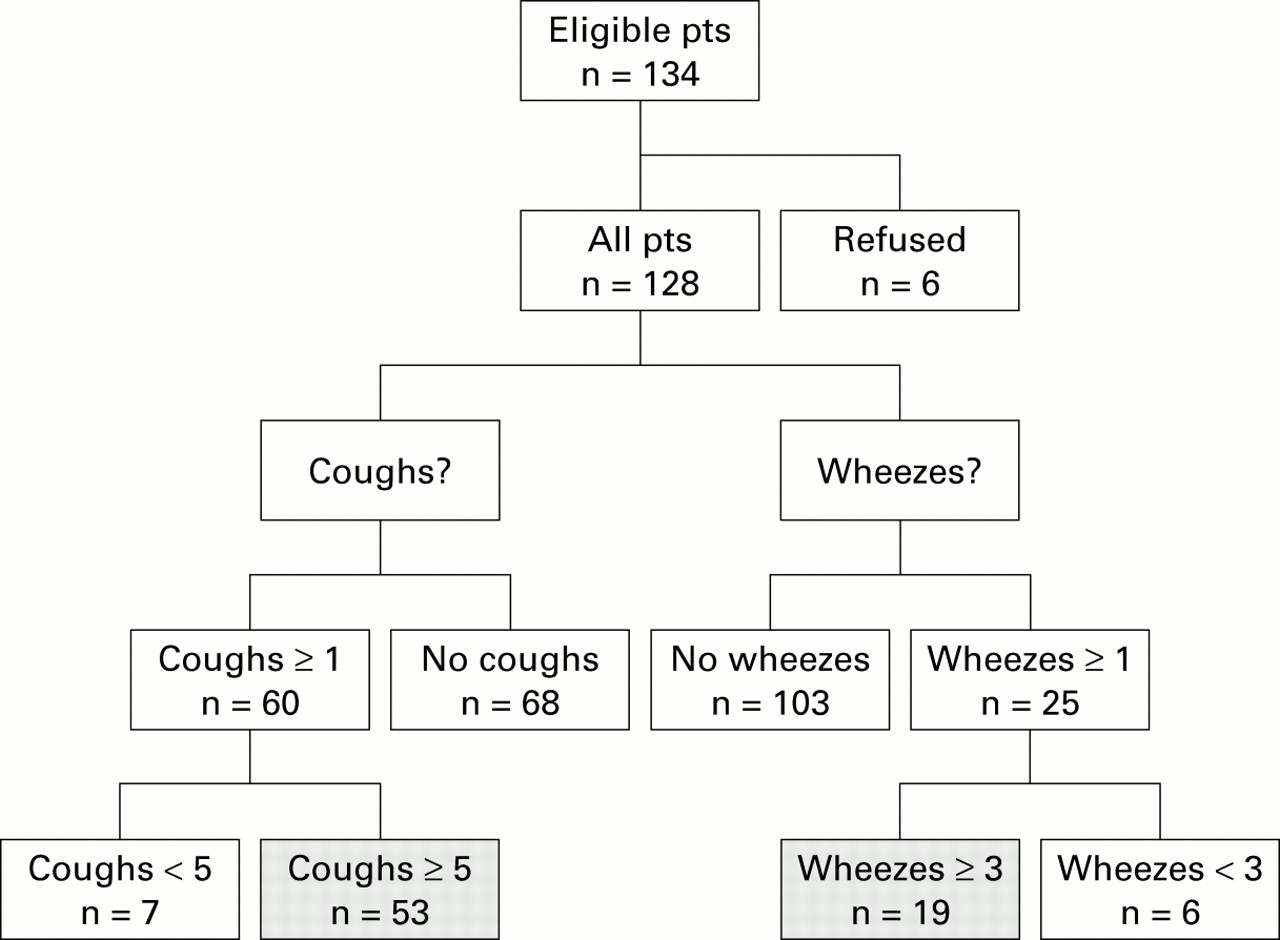
A total of 134 consecutive patients with asthma were invited to enter a Veterans Affairs study on the treatment of gastro-oesophageal reflux. All patients were offered upper gastrointestinal endoscopy and oesophageal function tests. Six patients (4.5%) declined to participate. The pH tracings of the remaining 128 patients were analysed. During the pH metry, patients did not experience more symptoms than usual, and the 24 hour recording periods proved to be typical of their presenting symptomatology. Episodes of coughing or wheezing occurred in 60 and 25 of 128 patients, respectively. The number of coughing episodes ranged between 1 and 79 (mean (SD) 21 (3)), and the number of wheezing episodes ranged between 1 and 27 (8 (1)). Among patients who coughed, five had only one cough and two had only two coughs during the entire monitoring period. Among patients with wheezing, six had one or two wheezing episodes only. These 13 patients were excluded from the subsequent statistical analyses. No abnormal oesophageal motility was recorded in all but one patient with low amplitude contractions. (This patient had only three coughs and no wheezes during the 24 hour pH metry and was not included in the further analysis.) A flow diagram of all patients is shown in fig 1. Table 1contains the characteristics of the entire patient population and the two subgroups of 53 patients with frequent coughs and 19 patients with frequent wheezes. Demographic characteristics, consumption of alcohol and cigarettes, acid contact time, prevalence of oesophagitis, and hiatal hernia were similar in all patient groups.

Flow diagram of the study population.
Patients characteristics
Table 2 shows the temporal relationships between coughing or wheezing and acid reflux. Assuming a latency period of two minutes or less, acid reflux preceded a coughing episode about seven times more often than vice versa—that is, coughing preceded acid reflux. Both types of events occurred about 2–3 times more frequently than expected based on chance alone, the outcome being statistically significant. Overall, nearly half of all coughs were found to be associated with a reflux episode. An increase in the latency period from two to five minutes increased the percentage of associations, with reflux preceding cough remaining the far more frequent relationship. About half of all wheezing episodes were associated with acid reflux (table 2). In 43% of all wheezing episodes, reflux preceded wheezing. Because of the relatively small number of patients with frequent wheezing, we abstained from a more detailed statistical analysis of the temporal relationship between wheezing and reflux.
Relationships among coughing, wheezing, and reflux
Of all reflux, coughing, and wheezing events, 81%, 78% and 80%, respectively, were recorded during the upright position. In general, separate analysis of the pH metry data by upright versus supine body position revealed rather similar patterns of association. Assuming a latency period of two minutes, 49% versus 36% of all upright versus supine coughs were associated with reflux events, reflux preceding cough in 43% and 30%, respectively. Of all wheezes, 51% and 41% were associated with reflux events during the upright and supine periods, respectively. Assuming a latency period of five minutes, 60% versus 71% of all upright versus supine coughs were associated with reflux events, reflux preceding cough in 48% and 58%, respectively. Of all wheezes, 57% and 53% were associated with reflux events during the upright and supine periods, respectively.
Figure 2 contains a sensitivity analysis of varying the length of interaction between cough and reflux from one to 10 minutes. Progressive lengthening of the coughing period raises the chances for a reflux event to fall into that period. As the duration of influence exerted by coughing is artificially extended from one to 10 minutes, an increasing fraction of coughs appears to result in a reflux episode (fig 2A). Assuming the influence of coughing on reflux to last as long as 10 minutes after the coughing event was first recorded, about 15% of all coughs appear to be followed by a reflux episode. In fig 2B, a reflux episode is assumed to exert its influence on coughing 1–10 minutes after the pH value returned to pH >4. The fraction of reflux episodes leading to coughing increases accordingly from 14% to 25%. Most importantly, the sensitivity analysis shows that the measured strength of the relationship between coughing and reflux depends in part on the type of assumptions built into the analysis. The analysis also demonstrates that, regardless of such assumptions, more reflux episodes result in coughing than coughing episodes result in reflux. When each individual patient is considered, a similar pattern is revealed. Table 3 shows the association of coughing and reflux in each individual patient. In 49 of 53 patients, acid reflux preceded a coughing episode while in 28 of 53 patients a cough preceded a reflux episode. All patients with cough preceding reflux also had reflux preceding cough. In only four patients was there no relationship between the two events.
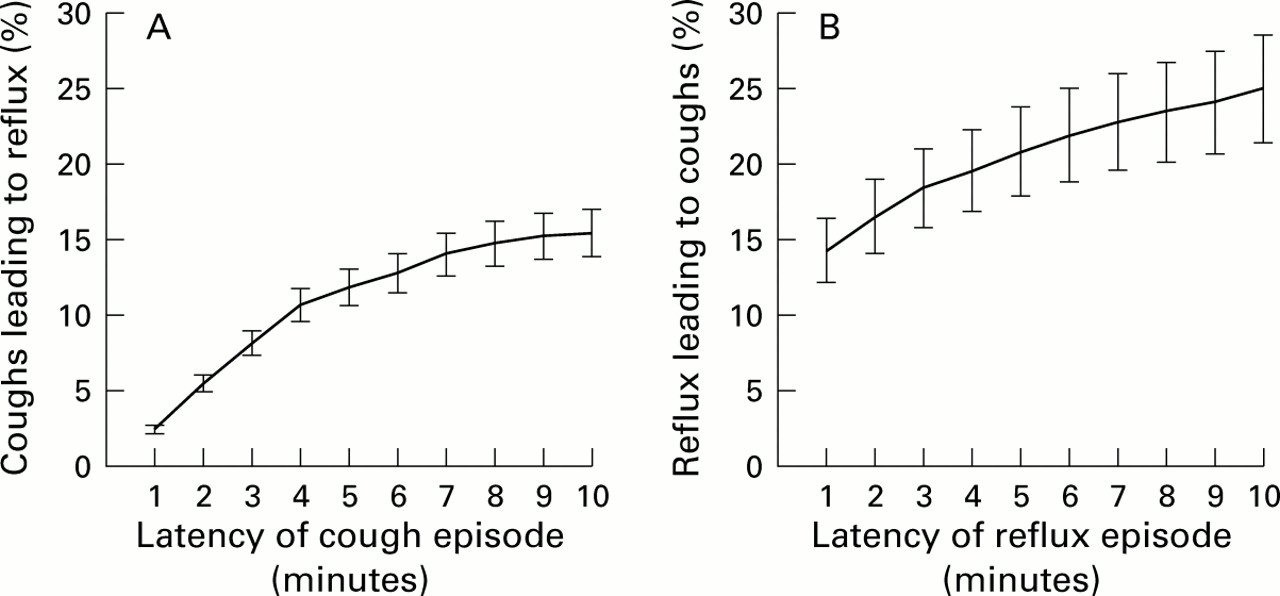
Fraction of coughs preceding reflux (A) and fraction of reflux episodes preceding coughs (B) dependent on the length of the latency period of coughing and reflux episodes, respectively. Each point represents the mean (SD) value calculated from the average values of 53 individual patients.
Association of coughing with reflux episodes
In the baseline analysis, a minimum of five coughing episodes was chosen as the threshold value for including a patient in the statistical analysis. In the sensitivity analysis of fig 3, the threshold was raised progressively from five to 35 coughs per 24 hour recording period. The chosen threshold had no influence on the overall fraction of coughs leading to acid reflux (fig 3A). In patients with rare as well as frequent coughing, only a minority of coughs resulted in acid reflux. The fraction of reflux episodes leading to coughing increased as the threshold was raised from five to 35 coughs per 24 hour recording period (fig 3B). Such a pattern suggests that in patients with frequent coughs the likelihood of coughs being precipitated by acid reflux increases. Varying the threshold of total wheezes between three and 10 did not greatly affect the fraction of wheezes associated with reflux and was similar to the baseline value of 48%.

{kind=link}
{kind=link}
{kind=link}
Influence of the number of coughing episodes on the fraction of coughs preceding reflux (A) and fraction of reflux episodes preceding coughs (B). Only patients with coughing episodes equal to or exceeding the threshold shown on the horizontal axes were included in calculating the mean (SD) value.
Discussion
Gastro-oesophageal reflux has long been associated with pulmonary disease.25-27 By analysing 24 hour pH tracings of asthmatic patients, we showed that half of all episodes of coughing or wheezing were associated with acid reflux. Acid reflux was far more likely to precede than follow a coughing episode. This temporal sequence between reflux and cough suggested that the reflux event was frequently responsible for coughing and that only rarely did coughing cause acid reflux. The likelihood of reflux induced coughing increased as the number of coughs increased in the individual asthmatic patient.
The study population comprised an unselected series of adult asthmatics in a VA hospital who were referred from the outpatient medicine and pulmonary clinics to participate in a study on the treatment of gastro-oesophageal reflux in asthmatics. Patients represented the entire spectrum with respect to pulmonary disease severity. A bias towards more or less severe asthma was unlikely as almost all patients approached agreed to participate in the study. Twenty eight per cent of all patients did not use bronchodilators on a permanent basis, indicating an appreciable fraction of patients with relatively mild or intermittent disease only. Placebo controlled studies using prolonged pH monitoring have failed to show any effect of either theophylline or β agonists on the severity of gastro-oesophageal reflux.28 ,29 Our patients therefore were instructed to use their bronchodilators as needed. Cessation of therapy might have resulted in bronchoconstriction, hyperinflation, flattening of the diaphragm, and a subsequent increase in acid reflux.30Indeed, an increase in gastro-oesophageal reflux has been demonstrated during methacholine induced bronchospasm.17 Thus any potential beneficial effect on acid reflux gained by discontinuation of bronchodilator medications could be negated by the adverse effects of worsening dyspnoea on acid reflux.
The primary aim of our study was to evaluate the temporal relationship between acid reflux and cough and make inferences about their causal association. Patients underwent extensive training on how to use the event markers for coughing and wheezing episodes. During evaluation of the pH metry data it became obvious nevertheless that even a seemingly simple analysis of the temporal relationships was open to multiple types of bias. With frequent consecutive and overlapping episodes of reflux and cough, it was difficult to establish unequivocally a cause and effect pattern. Two minutes were chosen as a baseline latency period between two events because this time period had been reported previously to provide reliable estimates.21 ,22 If two events occurred within a two minute time frame, the first event was considered to have caused the second one. Because other investigators also used latency periods as long as five and 10 minutes,23 ,24 we decided to subject our data to a computer analysis that automatically assigned to all latency periods lengths that varied between one and 10 minutes. Although the fraction of observed associations increased with increasing latency periods, the overall pattern remained robust. Regardless of the length of the latency period, reflux of acid remained a more common event to precede cough than to follow a cough. For clinical purposes therefore the choice of a single latency period of two minutes would probably be sufficient to establish a relationship between pulmonary symptoms and reflux.21
In a second sensitivity analysis, thresholds for the total number of coughs and wheezes were varied. Patients with very few events were characterised by extreme R values and extreme fractions of coughs or wheezes associated with reflux. The thresholds of three and five events for wheezes and coughs, respectively, were chosen as a compromise between two opposing goals. On the one hand, a large number of events assured a more reliable estimate for the true fraction of associated events in the individual patient. On the other hand, the very stringent criteria of high thresholds led to exclusion of many patients. Fortunately, most parameters remained unaffected by the choice of a particular threshold. Thus the dependence of reflux induced coughing on the total number of coughs appeared to reflect an underlying pathophysiological mechanism rather than an artefact of measurement.
Fifty three of our 60 patients with cough had five or more coughing episodes during the 24 hour period, and 92% of the 53 patients had cough associated with reflux. These findings are consistent with the results of DeMeester et al and Ing et al who reported that 70% and 90%, respectively, of all patients with chronic cough also presented with abnormal pH monitoring.14 ,31 Laukkaet al attempted to establish a causal relationship between coughing and reflux in a small population of 10 patients with gastro-oesophageal reflux symptoms.32Although in the majority of instances the two events were not related, in a few instances cough preceded reflux more often than reflux preceded cough. Compared with our study however the authors investigated only a few patients, most of whom had a low acid contact time with little evidence to support reflux induced pulmonary symptoms. Raiha et al observed in a series of 105 patients undergoing oesophageal pH monitoring that respiratory symptoms did not appear unless the acid contact time of pH <4.0 exceeded 10%.33 It is presently unknown whether reflux of acid into the oesophagus is sufficient to initiate a cough or whether actual aspiration of the refluxed acid is necessary. Indeed, changes in airway calibre and resistance in response to acid in the distal oesophagus have been described in asthmatic patients as a possible reflex mechanism for reflux induced cough.34 ,35 Our results support recently published data by Harding et al who showed that among asthmatics with reflux disease, 78% of respiratory symptoms and 90% of coughs were associated with oesophageal exposure to acid.36 The statistical associations between pulmonary symptoms and acid reflux found by us and by previous investigators do not prove causality and still require confirmation by treatment trials. Studies demonstrating improvement or even cure of asthma after antireflux surgery however do lend support to the contention that gastro-oesophageal reflux contributes to the occurrence of asthma.8 ,10
In conclusion, half of all coughs and wheezes in asthmatics are associated with acid reflux into the oesophagus. While an occasional coughing episode can lead to reflux, it is the reflux episode, in the vast majority of instances, that leads to cough. Our study establishes a possible link between reflux and coughing or wheezing. The potential of antireflux therapy to break the cycle of reflux induced cough and, to a lesser degree, cough induced reflux is in need of study.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the Hines VA Hospital, Hines, Illionois, USA.
Parts of the study were previously presented at Digestive Disease Week and published in abstract form.37 ,38
Abbreviations used in this paper
- GORD
- gastro-oesophageal reflux disease
- FEV1
- forced expiratory volume in 1 s