Article Text

Abstract
Background—Atropine decreases the frequency of transient lower oesophageal sphincter relaxation (TLOSR) through an unknown mechanism. Gastric distension and pharyngeal receptor excitation are two possible sources for the afferent stimulus responsible for TLOSR.
Aims—To determine whether atropine affects gastric distension induced TLOSR and pharyngeal receptor mediated lower oesophageal sphincter (LOS) relaxation.
Methods—Oesophageal manometry and pH recordings were performed in 10 healthy volunteers on two separate days in the postprandial setting, following either atropine (15 μg/kg intravenous bolus and 4 μg/kg/h as a maintenance dose) or placebo. Pharyngeal receptor mediated LOS relaxation was studied in nine subjects by rapid injection of minute amounts of water (0.05, 0.1, 0.2, 0.3, and 0.4 ml) in the pharynx before and after atropine. Gastric distension mediated TLOSR was studied in eight subjects by insufflating the stomach with 300, 600 and 900 ml of CO2 before and after atropine.
Results—Atropine reduced the frequency of spontaneous gastro-oesophageal reflux and TLOSR compared with placebo (p<0.05). Pharyngeal stimulation resulted in bolus volume dependent LOS relaxation. Atropine decreased the frequency and amplitude of pharyngeal receptor mediated LOS relaxation at bolus volumes of 0.05, 0.1, and 0.2 ml. Gastric distension resulted in intermittent episodes of TLOSR. The frequency of gastric distension induced TLOSR was significantly decreased by atropine.
Conclusion—(1) Atropine reduces the frequency of spontaneous reflux and TLOSR in normal subjects; and (2) gastric distension induced TLOSR and pharyngeal receptor mediated LOS relaxation is inhibited by atropine.
- lower oesophageal sphincter relaxation
- anticholinergic
- pharynx
- gastric distension
Statistics from Altmetric.com
Transient lower oesophageal sphincter relaxation (TLOSR) is the major mechanism of gastro-oesophageal reflux (GOR) in normal subjects and also accounts for a significant number of reflux episodes in patients with GOR disease.1 ,2 We recently reported that even though atropine reduces basal LOS pressure, it diminishes the frequency of GOR3 through its inhibitory effect on the frequency of TLOSR. The mechanism by which atropine reduces the frequency of TLOSR is not known.
TLOSR is a neural reflex that is mediated through the brain stem.4 The efferent pathway for TLOSR is in the vagus nerve; in dogs, TLOSR is completely eliminated by cooling of the cervical vagus.5 Gastric distension triggers TLOSR through stimulation of tension receptors in the proximal stomach, particularly the gastric cardia.6 Afferent fibres which signal gastric distension are known to project to the nucleus tractus solitareus (NTS) and to the dorsal motor nucleus of the vagus nerve (DMV)4in the brain stem. The evidence for a possible role of pharyngeal receptors in the afferent pathway to the TLOSR is suggested by the following: injection of minute amounts of liquid into the hypopharynx of humans7 leads to prolonged LOS relaxation; and light stroking of the pharynx in the opossum8 leads to isolated LOS relaxation. The latter depends on the afferents from the pharynx or larynx travelling in the superior laryngeal branch of the vagus and glossopharyngeal nerves and their projection to the NTS and DMV.
The aims of our studies were: (i) to reconfirm the effects of atropine on the frequency of TLOSR and GOR; (ii) to examine the effects of atropine on gastric distension induced TLOSR; and (iii) to study the effects of atropine on pharyngeal stimulus mediated LOS relaxation.
Methods
SUBJECTS
Studies were performed in 26 healthy, asymptomatic volunteers. These subjects were free from any gastrointestinal symptoms, had no history of upper gastrointestinal surgery, were not taking antacids on a regular basis, and did not take medication known to alter oesophageal motor function. Each volunteer gave written informed consent and the protocol was approved by the Human Investigation Committee of the University of Virginia.
PROTOCOL 1: EFFECTS OF ATROPINE ON TLOSR AND GOR
Ten subjects (six men and four women) participated in the experiments designed to study the effects of atropine on the frequency of GOR and TLOSR. Their mean age was 27 years (range 22–47 years). Each subject underwent simultaneous oesophageal manometric and pH studies on two separate days. In this and subsequent protocols, oesophageal manometry was performed using an eight lumen catheter equipped with a reverse perfused electrode sleeve assembly. The reverse perfused electrode sleeve sensor9 monitored LOS pressure and crural diaphragm electromyogram. Side holes monitored pressures in the pharynx, three sites in the oesophagus (2, 7, and 12 cm above the LOS), and the gastric fundus. The pharyngeal side hole was not water perfused (to minimise infusion of water in the pharynx), but the remaining manometric channels were perfused at 0.5 ml/min by a low compliance, pneumohydraulic capillary infusion pump. Oesophageal pH was monitored at 5 cm above the proximal margin of the LOS with a glass electrode (Micro-electrodes, Londonderry, New Hampshire, USA). The manometric and pH signals were recorded on a sensormedics recorder (Anaheim, California) at a paper speed of 1 mm/s. Following placement of the manometric assembly, subjects were allowed to accommodate for 20–30 minutes. Subjects then ate a standardised 950 kcal meal, after which they laid in the supine or left lateral position. Recordings were performed for a 30 minute period, at the end of which subjects received either intravenous atropine sulphate (15 μg/kg bolus and 4 μg/kg/h as maintenance dose) or placebo on the two separate days. Recordings were performed for an additional hour after intravenous injection.
Data analysis
Data were analysed in a blinded fashion for the frequency of GOR and TLOSR during 30 minute intervals before and after intravenous injection. A reflux episode was defined as a drop in intraoesophageal pH of more than 1 pH unit. TLOSR was defined as an abrupt decrease in LOS pressure to the level of intragastric pressure that was not triggered by a swallow. The LOS pressure drop was at least 4 mm Hg and lasted longer than 10 seconds.3
PROTOCOL 2: EFFECTS OF ATROPINE ON LOS RELAXATION INDUCED BY INJECTION OF MINUTE AMOUNTS OF WATER INTO THE PHARYNX
Nine subjects (six women and three men) fasted for six to eight hours prior to the study. The mean age was 28 years (range 23–37 years). The nose was anaesthetised with xylocaine jelly and a light cetacaine spray was used to anaesthetise the pharynx. Subjects laid supine for the duration of the study. After placement of the manometric assembly (as in protocol 1), subjects were allowed to accommodate to the tube and surroundings for 10–15 minutes. The pharynx was then stimulated with rapid injections of minute amounts of water at room temperature, through a side hole positioned 2 cm above the upper oesophageal sphincter. Each injection took place at least 15 seconds after a swallow and subjects were instructed to avoid swallowing for as long as possible after the injection. Initially, a bolus volume of 0.05 ml water was used which was then increased to 0.1 ml and subsequently increased in 0.1 ml increments until the bolus volume that caused an irrepressible swallow was achieved. Three trials were conducted at each bolus volume. Each water injection was initiated at a time when the LOS pressure recording was stable for at least 15 seconds. After the initial series of tests, atropine sulphate (15 μg/kg) was injected intravenously and the pharyngeal injections were repeated. Pharyngeal injections after atropine were only performed if the basal LOS pressure was more than 10 mm Hg.
Data analysis
Data were analysed for the frequency of LOS relaxation response and the magnitude of LOS relaxation. LOS pressure was measured at end expiration. LOS relaxation in response to a pharyngeal stimulus was said to occur if the following criteria were met: (1) LOS pressure drop was ⩾4 mm Hg; (2) LOS relaxation occurred within five seconds of pharyngeal stimulus; and (3) duration of LOS relaxation was ⩾5 seconds. The drop in LOS pressure was also quantitated and expressed as a percentage of the pre-stimulus LOS pressure.
PROTOCOL 3: EFFECTS OF ATROPINE ON GASTRIC DISTENSION INDUCED LOS RELAXATION
These studies were performed in eight healthy, asymptomatic subjects (five men and three women) with an average age of 27 years (range 21–39 years). Subjects fasted for six to eight hours prior to the study. After placement of the manometry catheter as in the previous protocol, subjects were allowed to acclimatise to the assembly for 10–15 minutes. Subjects remained in an upright sitting position for the duration of the study. The subjects were subsequently given 300, 600, and 900 ml of a CO2 generating powder (E-Z-Gas II, E-Z-EM, Inc., Westbury, New York, USA; contains sodium bicarbonate, citric acid, simethicone, natural orange flavour, sodium saccharin, and excipients) at 15 minute intervals. Participants were handed a packet of E-Z-Gas II powder and instructed to place the contents on their tongue. Water was used to wash the contents into the stomach to drive the production of CO2. Atropine sulphate (15 μg/kg) was then administered intravenously and the subjects again ingested the E-Z-Gas II powder at volumes of 300, 600, and 900 ml at 15 minute intervals.
Data analysis
Transient LOS relaxations were counted in the 15 minute intervals following ingestion of the CO2 producing powder. A common cavity during TLOSR was defined as an increase in intraoesophageal pressure of more than 2 mm Hg at one or both oesophageal sites.
STATISTICAL ANALYSIS
Paired t tests, amalysis of variance (ANOVA), and χ2 analysis were used as statistical methods and data are presented as mean (SEM).
Results
EFFECTS OF ATROPINE ON THE FREQUENCY OF POSTPRANDIAL GOR AND TLOSR
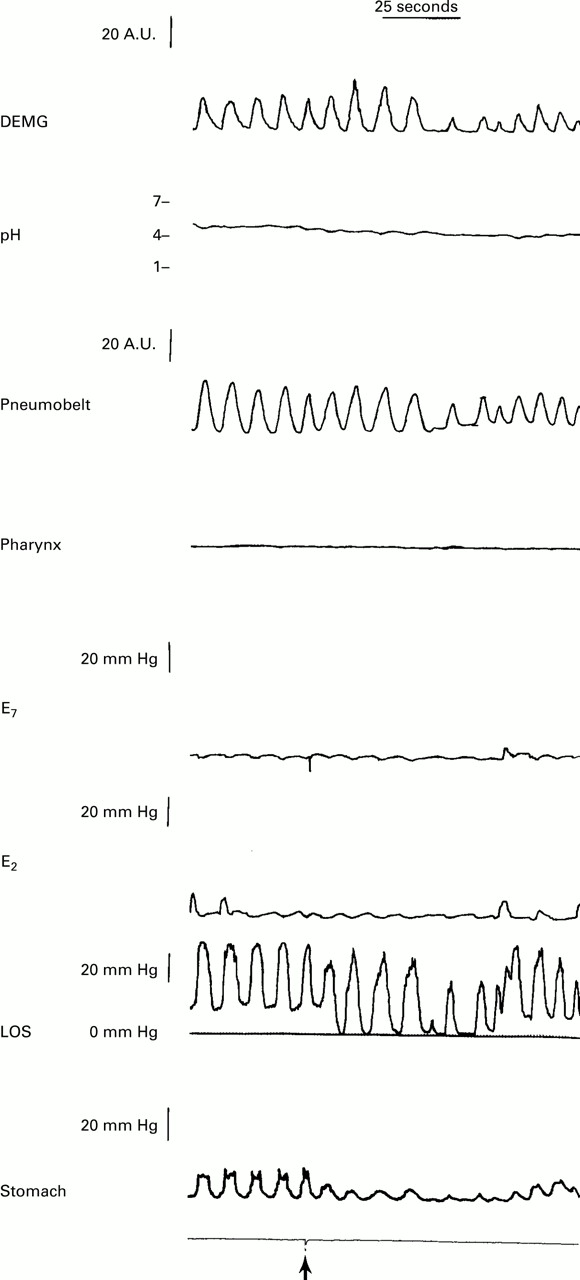
The LOS pressure tracing showed two pressure patterns: an end expiratory pressure (LOS pressure), and inspiratory pressure oscillations (crural diaphragm pressure) (fig 1). Atropine caused a reduction in the basal LOS pressure without any effect on the crural diaphragm pressure.
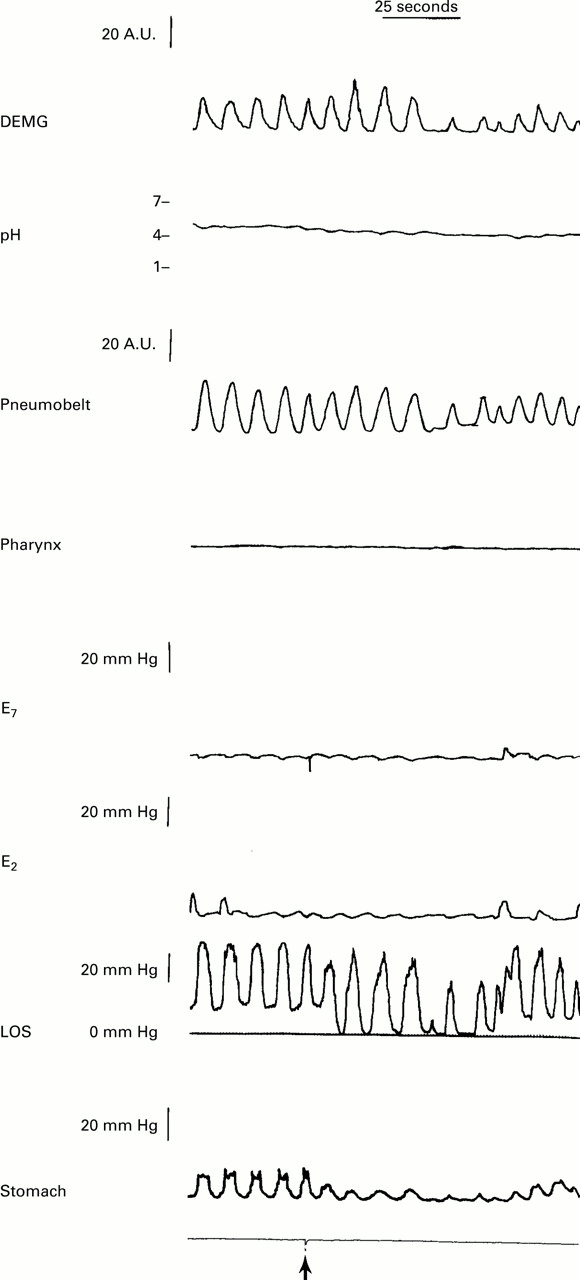
: Effects of pharyngeal stimulus on LOS relaxation. A manometric record of the effect of injection of water in the pharynx (marked by the arrow) on LOS pressure. Note that soon after the injection of water the LOS relaxes for 30 seconds. There is no relaxation of the crural diaphragm as shown by continued inspiratory pressure oscillations in the LOS pressure tracing and crural diaphragmatic electromyographic activity.
There was a significant reduction in the frequency of GOR, from 2.6 (1.2) in the control period to 0.2 (0.1) in the first and 0.4 (0.1) in the second half hour periods following atropine injection (p<0.05) (fig 2). One subject who showed 11 episodes of reflux in the first 30 minutes after the meal had only one reflux event in the first half hour period after the injection of atropine and none during the second half hour period.

: Effects of atropine on the frequency of postprandial GOR and TLOSR. Mean (SEM) data on the frequency of TLOSR and GOR in 10 subjects. Data were collected in the postprandial periods.
In nine of 10 subjects reflux occurred exclusively during periods of TLOSR. In one subject the predominant mechanism of reflux was related to long periods of LOS relaxations induced by multiple swallows. The decrease in the rate of reflux episodes after atropine was the result of a significant decrease in the frequency of TLOSR. The frequency of TLOSR was dramatically reduced by atropine (2.5 (0.4), 0.3 (0.2), and 0.6 (0.2) in the control and two post-atropine periods respectively; p<0.05) (fig 2). One subject who showed reflux due to multiple swallow also ceased to reflux after atropine injection. Placebo had no effect on the frequency of GOR and TLOSR.
EFFECTS OF PHARYNGEAL STIMULUS ON LOS PRESSURE AND CRURAL DIAPHRAGMATIC PRESSURE BEFORE AND AFTER ATROPINE
Injection of minute amounts of water in the pharynx resulted in LOS relaxation without relaxation of the crural diaphragm. The absence of crural diaphragm relaxation was seen in both the inspiratory LOS pressure oscillation and crural diaphragm electromyogram recordings (fig 1). The incidence of LOS relaxation and magnitude of LOS relaxation in response to pharyngeal stimulus were volume dependent (fig 3). The incidence of pharyngeal stimulus response was significantly decreased (p<0.05, ANOVA) after atropine at bolus volumes of 0.05, 0.1, and 0.2 ml. LOS relaxation was nearly complete or 100% complete at volumes of 0.4 and 0.5 ml (figs 4 and 5). The LOS pressure drop was significantly reduced (using ANOVA) following atropine injection at bolus volumes of 0.05, 0.1, 0.2, and 0.3 ml. As the reduction in magnitude of LOS pressure drop by pharyngeal stimulus could be due to the effects of atropine on the basal LOS pressure, we also compared the percentage LOS relaxation. The percentage LOS relaxation was also significantly reduced at bolus volumes of 0.05 and 0.1 ml with a trend towards significance at 0.2 ml (using χ2 analysis). The duration of LOS relaxation in response to pharyngeal stimulation was generally 10–60 seconds and occasionally longer but was not related to the bolus volume.
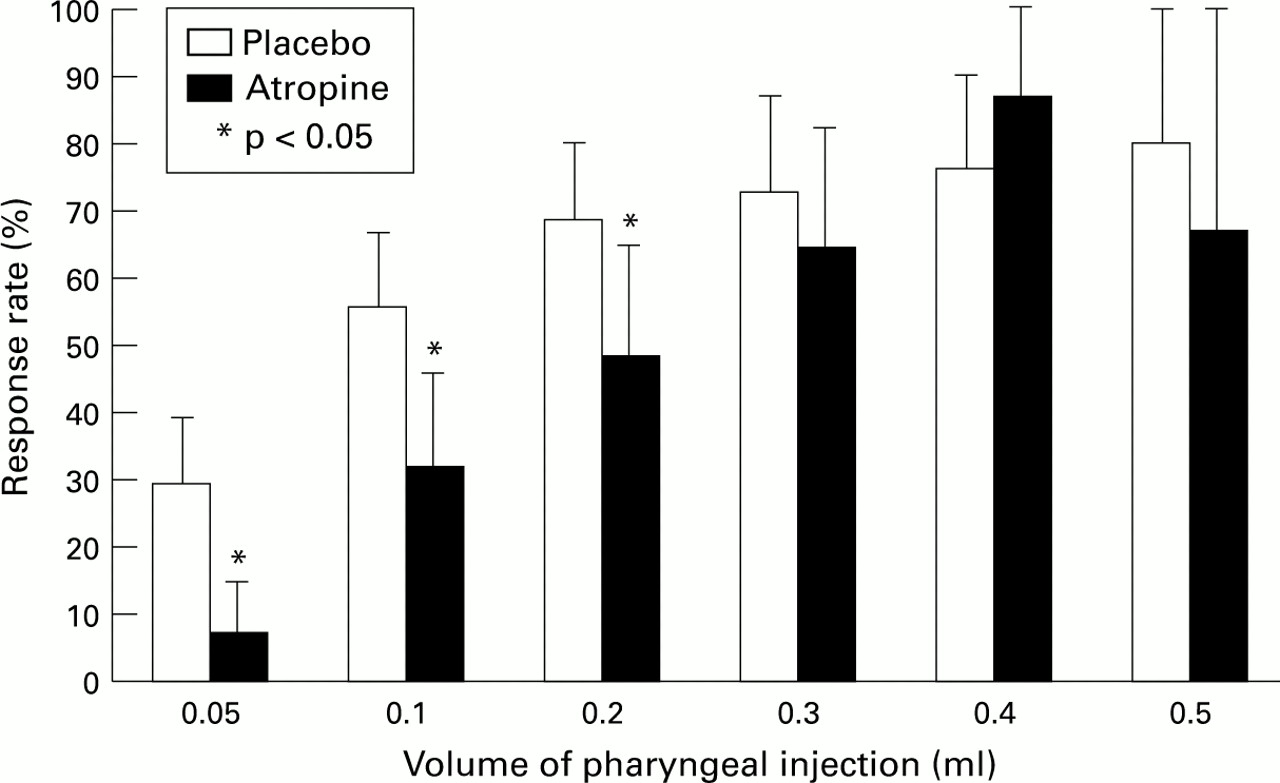
: Effects of atropine on the incidence of pharyngeal stimulus induced LOS relaxation. Mean (SEM) data in nine normal subjects. The LOS response to pharyngeal stimulus was defined as a decrease in LOS pressure of more than 4 mm Hg.

: Effects of atropine on the amplitude of LOS pressure drop and percentage LOS relaxation induced by pharyngeal stimulus. The data summarise the absolute LOS pressure fall and percentage LOS relaxation by pharyngeal stimulus before and after injection of atropine in nine subjects (control and atropine, respectively).
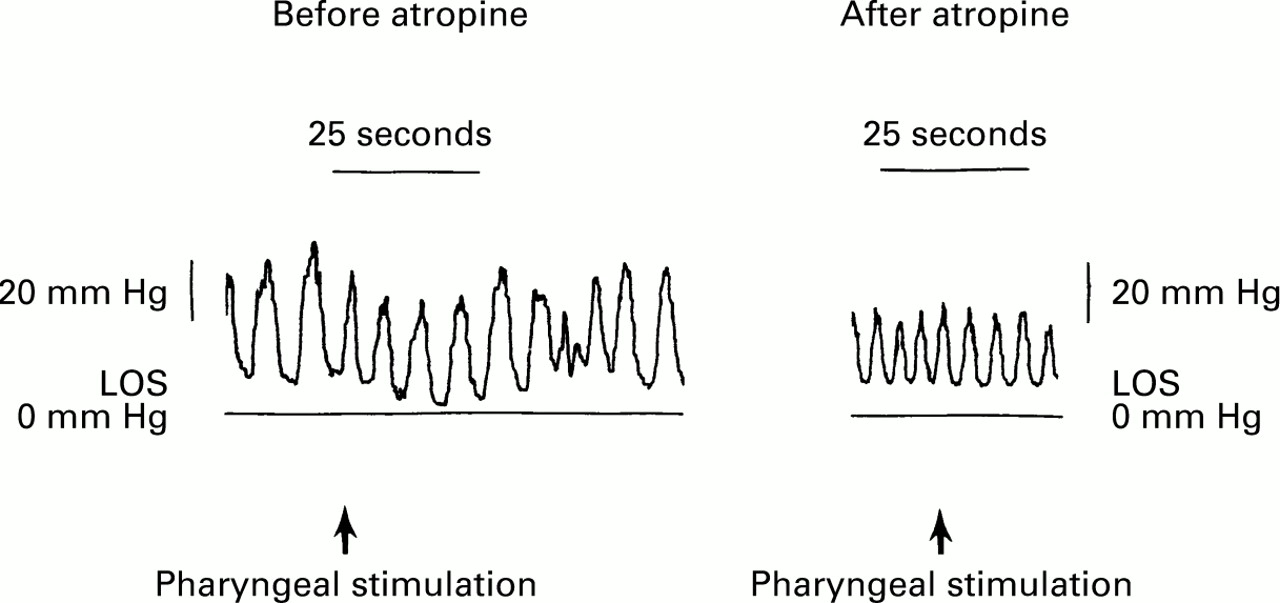
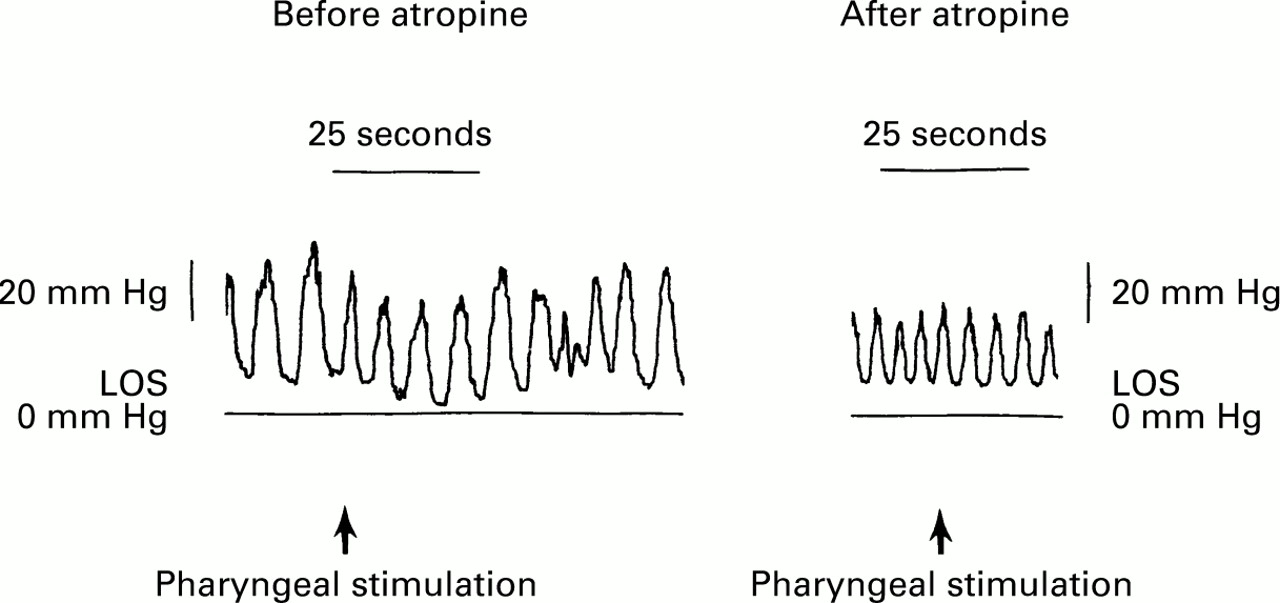
: Effects of atropine on pharyngeal stimulus induced LOS relaxation: LOS pressure tracing before and after injection of atropine in the same individual. The same bolus volume (0.3 ml) was used for both the pharyngeal stimulations. Note the absence of LOS relaxation following atropine injection. Crural diaphragmatic activity (inspiratory pressure oscillations) was not affected by pharyngeal stimulus and atropine.
EFFECTS OF ATROPINE ON GASTRIC DISTENSION INDUCED TLOSR
Gastric distension with 300, 600, and 900 ml CO2resulted in bursts of TLOSR for 5–10 minutes after the ingestion of the gas generating powder. The frequency of TLOSR was significantly greater after 900 ml compared with 300 ml CO2 (p<0.05) (fig 6). The majority of TLOSRs were associated with belches; however, some only resulted in oesophageal common cavities without an actual belch, as reported by the subjects. The number of TLOSRs at bolus volumes of 300, 600, and 900 ml were 3.8 (1), 4.6 (0.9), and 5.8 (1), respectively (fig 6). Atropine caused a significant reduction in the frequency of TLOSR at both 300 and 600 ml of stomach distension (p<0.05) and a trend for significance (p=0.06) at 900 ml distension. The post-atropine TLOSR frequencies at 300, 600, and 900 ml were 1.75 (0.5), 2.75 (0.5), and 3.63 (0.7), respectively (fig6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
: Effects of atropine on gastric distension induced TLOSR. Data are mean (SEM) in seven normal subjects. The number of TLOSRs was measured in the 15 minute periods after the ingestion of each volume of CO2.
Discussion
Our study shows that: (i) atropine reduces the frequency of postprandial physiological GOR through its inhibitory effect on the frequency of TLOSR; (ii) atropine reduces the frequency of gastric distension induced TLOSR; and (iii) atropine has an inhibitory effect on the frequency and magnitude of pharyngeal stimulus induced LOS relaxation.
Our finding that atropine reduces the frequency of GOR and TLOSR is similar to that which we reported previously.3 The experimental design of this study differs slightly from the earlier study, however. The previous study was neither placebo controlled nor randomised. The current study addressed both of these issues. We found that placebo had no significant effect on the frequency of TLOSR and GOR. In contrast, atropine caused a significant reduction in the frequency of both TLOSR and GOR.
The new findings in this study are that atropine inhibits gastric distension mediated TLOSR and pharyngeal receptor mediated LOS relaxation. Paterson et al reported that low frequency stimulation of the superior laryngeal nerve or light stroking the back of the pharynx in the opossum results in isolated LOS relaxation.8 Recently, Trifan et al reported that stimulation of the pharynx with minute amounts of water causes prolonged periods of LOS relaxation.7 In addition to LOS relaxation, a pharyngeal stimulus can also induce inhibition in the body of the oesophagus.10 The inhibition caused by a pharyngeal stimulus most likely excites afferent impulses in the vagus, trigeminal, and glossopharyngeal nerves which traverse to the NTS11 and DMV in the brain stem. The inhibitory efferents travelling in the vagus nerve mediate relaxation in the oesophagus and LOS. The oesophageal and LOS inhibition is mediated by a subset of vagal fibres that have short latency periods and they respond to stimulation at low frequencies.12 It is likely that stimulation of the pharynx with minute amounts of water excites these short latency vagal fibres.
Our data show that atropine increases the threshold of pharyngeal stimulus required to elicit LOS relaxation and reduces the amplitude of LOS relaxation. Could the mild pharyngeal anaesthesia which we used for placement of the manometric catheter have affected our results? It is possible that pharyngeal anaesthesia reduced the LOS relaxation response to pharyngeal injection. To minimise the effects of anaesthesia we used a very light spray and allowed for 10–15 minutes accommodation time. If anaesthesia affected our results our data would be expected to underestimate the effect of atropine because we always tested placebo first followed by atropine.
One site of action of atropine at which it inhibits LOS relaxation may be the brain stem. In support of this concept is the observation made by Gidda et al that atropine reduces the oral phase of swallow in response to electrical stimulation of the superior laryngeal nerve in the opossum, suggesting that atropine acts at the level of the central nervous system to block a swallow reflex.13 Berger reported that cholinergic receptors are present in the swallow centre of the brain stem and muscarinic blockade inhibits the oesophageal phase of swallowing.14 Atropine may reduce the salivary secretions15 to reduce the pharyngeal bolus volume and thus the afferent stimulus. Our data do not allow us to differentiate between the effects of atropine on saliva versus the brain stem. The other possibility is that atropine may block the vagal efferent pathway at the level of the myenteric plexus.
Our finding that injection of water in the pharynx causes relaxation of the LOS but not the crural diaphragm is similar to the one that we reported recently.16 A spontaneous TLOSR, unlike pharyngeal stimulus induced LOS relaxation, is associated with simultaneous inhibition of the LOS and crural diaphragm.17Therefore, a pharyngeal stimulus mediated LOS relaxation does not resemble spontaneous TLOSR. Does pharyngeal stimulus induced LOS relaxation and the inhibitory effects of atropine on this LOS relaxation have any relevance to the inhibition of spontaneous TLOSR by atropine? LOS relaxation is an important component of a spontaneous TLOSR and atropine does interfere with LOS relaxation. Therefore, we believe that the inhibitory effect of atropine on LOS relaxation could play an important role in the inhibition of spontaneous TLOSR.
The inhibition of gastric distension induced TLOSR by atropine could be mediated at the level of the CNS or myenteric plexus because the pathway for gastric distension induced TLOSR is also through the vagal afferents, brain stem and vagal efferents.4 However, another possibility is that atropine may affect the gastric stretch mechanoreceptors that may mediate TLOSR.6 Using a barostat, Azpiroz et al found that atropine does inhibit tone in the muscles of dog gastric fundus.18 As gastric mechanoreceptors are positioned in series, relaxation of the gastric fundus muscle is likely to decrease the discharges from these receptors.19 Therefore, the inhibitory effect of atropine on TLOSR frequency may be mediated through the inhibition of gastric mechanoreceptor discharges.
Recently, besides atropine, other pharmacological agents such as morphine,20 cholecystokinin A receptor antagonist,21 and nitric oxide antagonists21have been reported to affect the frequency of TLOSR. The mechanism by which these agents reduce the TLOSR frequency is not known. These agents could work on the afferent or efferent limb of the neural reflex to the LOS. In addition, they may alter the gastric fundic tone and change the sensitivity of tension mechanoreceptors. Therapeutic agents that manipulate the basic underlying mechanism of reflux disease—that is, TLOSR, have not been available. With the possibilities that pharmacological agents can reduce TLOSR frequency, future treatment strategies may be able to target TLOSR in the treatment of reflux disease.
Acknowledgments
This research was supported in part by a grant from the Jeffress Trust, Virginia, USA.