Article Text

Abstract
Background—The influence of gastrin on the colonic mucosa is still uncertain. Some authors have suggested a stimulating effect on the growth of normal and malignant colonic epithelium, while others have shown no association between gastrin and neoplastic development.
Aims—To evaluate the effect of gastrin on colorectal cell proliferation, patients with chronic endogenous hypergastrinaemia underwent proctoscopy. Biopsy specimens were taken in order to study rectal cell kinetics.
Patients and controls—Ten patients with chronic autoimmune gastritis (CAG), six patients with Zollinger-Ellison syndrome (ZES), and 16 hospital controls took part in this study. Patients with CAG and ZES had basal serum gastrin concentrations significantly higher than controls (p<0.001).
Methods—Immunohistochemistry was performed on 3 μm sections of rectal biopsy specimens incubated with 5′-bromodeoxyuridine.
Results—The percentage of proliferating cells in the entire crypts (overall labelling index) was similar in all the groups. However, the labelling frequency in the upper two fifths of the glands (φh value) was significantly higher in patients with CAG or ZES compared with controls (p<0.01 in both patient groups versus controls).
Conclusions—Endogenous hypergastrinaemia is associated with rectal cell proliferation defects, similar to those observed in conditions at high risk for colon cancer. The effect of the increased serum concentrations of gastrin on the colorectal mucosa after treatment with drugs inhibiting gastric acid secretion should be investigated.
- gastrin
- cell kinetics
- colon cancer
- chronic autoimmune gastritis
- Zollinger-Ellison syndrome
Statistics from Altmetric.com
It is widely accepted that endogenous and exogenous gastrin increases the synthesis of DNA in both oxyntic gland mucosa and small intestinal mucosa.1 ,2 The influence of the hormone on the colonic mucosa, however, is still uncertain. Some authors have suggested a stimulating effect on the growth of normal and malignant colonic epithelium both in experimental models and in human studies,3-5 while others found no association between gastrin and neoplastic development.6 ,7
Patients with chronic autoimmune gastritis (CAG) or Zollinger-Ellison syndrome (ZES) have high gastrin serum concentrations.8 ,9These patients may be considered as a human model to evaluate the influence of gastrin on the growth of the large bowel mucosa.
We analysed the rectal cell proliferation in patients with these diseases (CAG and ZES) and with endogenous hypergastrinaemia. Immunohistochemistry was performed on sections of biopsy specimens incubated with 5′-bromodeoxyuridine (5′-BrdU).
Materials and Methods
SUBJECTS EXAMINED
Three groups of subjects were considered (table 1).
Clinical data of patients and controls
Chronic autoimmune gastritis
Ten patients (seven women; age range 22–71 years) were studied. Biopsy specimens taken during gastroscopy showed a chronic atrophic gastritis limited to the gastric body. All patients had parietal cell antibodies in the serum. Two patients in this group had a history of adenomas in the large bowel. Two patients had another autoimmune disease (thyroiditis). The diagnosis of CAG and hypergastrinaemia was made 96 months (mean) before entering this study.
Zollinger-Ellison syndrome
Six patients (three women; age range 38–71 years) were studied. They were not receiving gastric antisecretory drugs, because they entered the study at the time of first diagnosis or a few days later. One patient had multiple endocrine neoplasia (MEN 1). The diagnosis of ZES and hypergastrinaemia was made not more than one month before entering the study.
Hospital controls
Sixteen subjects (nine women; age range 35–77 years) with non-ulcer dyspepsia and without inflammatory or neoplastic diseases of the large intestine were studied.
All patients and controls gave their informed consent to the study. Blood samples for routine laboratory tests and determination of basal serum gastrin were collected at admission. The basal serum gastrin concentration was measured by radioimmunoassay (Becton Dickinson, New York, NY, USA). This method detects sulphated and non-sulphated human heptadecapeptide (hG-17), as well as human big gastrin (hG-34). Gastrin results were expressed as pg/ml, with synthetic human gastrin-17 used as a standard.
All patients and 12/16 hospital controls underwent total colonoscopy; 4/16 hospital controls had a barium enema. Examinations were performed one to three months before the cell kinetics analysis.
BIOPSY AND CELL KINETICS ANALYSIS
Each subject underwent proctoscopy without bowel preparation. All colonoscopies were performed during the morning (0900–1100 am) in order to avoid as much as possible bias due to circadian variations in proliferation.10 During endoscopy six biopsy specimens were taken from flat mucosa 10–15 cm from the anal verge in the anterior rectal wall using biopsy miniforceps. The specimens were cut in 1 mm thick fragments and oriented mucosa side up on filter paper in small Petri dishes. The culture medium was Eagle’s basic solution supplemented with 10% fetal calf serum plus 5′-BrdU 320 μM/l. The dishes were placed in a rolling chamber at 37°C for one hour with an atmosphere of 95% O2 and 5% CO2. After incubation, the specimens were fixed in 70% ethanol, dehydrated, and embedded in paraffin wax according to routine histological procedures. Non-consecutive 3 μm sections were cut and mounted on the slides to obtain samples of different crypts. The slides were processed using the avidin-biotin peroxidase complex technique (Vectastain ABC kit; Vector Laboratories, Burlingame, CA, USA) using an anti-BrdU monoclonal antibody (Becton Dickinson) diluted 1 in 100 in PBS. Denaturation of DNA was done prior to the immunohistochemical procedure with 2N HCl for 20 minutes at 37°C. Finally, slides were stained with diaminobenzidine (DAB) solution (Sigma) and weakly counterstained with haematoxylin.
For cell kinetics evaluation, 10 to 20 longitudinally oriented glands (mean 17.4) were blindly evaluated for each subject in the study. To study the height distribution of labelled cells and to compare crypts of different size, each gland was divided into five compartments of equal size, numbered from 1 (bottom) to 5 (surface).
In each case both the overall and the compartment labelling index (LI) and the labelled cell frequency in the upper 40% of the crypts (φh value) were assessed. This parameter, corresponding to the ratio between the number of labelled cells in the upper two fifths of the colonic crypt (compartments 4 and 5) and the total number of labelled cells, quantifies the shift of the proliferative compartment towards the surface, which occurs in subjects at high risk for colon cancer.11
STATISTICAL ANALYSIS
Data were expressed as mean (SEM). The Mann-Whitney U test was used to compare cell kinetics data in patient groups and in controls.
Results
No haematological abnormalities were found. In particular, patients with CAG had no signs of pernicious anaemia. Basal serum gastrin concentrations were significantly higher in patients than in controls (p<0.001) (table 1). No patient with CAG or ZES had basal serum gastrin concentrations falling in the range of the controls (pg/ml). Neither polyps nor cancer were found at total colonoscopy or barium enema. Finally, rectal biopsy specimens did not show any histological abnormality. In particular, no dysplasia was found.
Table 2 shows the mean proliferative parameters in the three groups of subjects. The overall LI did not show any significant difference between groups.
Pattern of epithelial cell proliferation
However, the frequency of labelled cells in the upper 40% of the crypts (φh value) was significantly higher in CAG and ZES patients than in control subjects (p<0.01 CAG v controls; p<0.01 ZES v controls). No differences were found between CAG and ZES patients (figure 1).
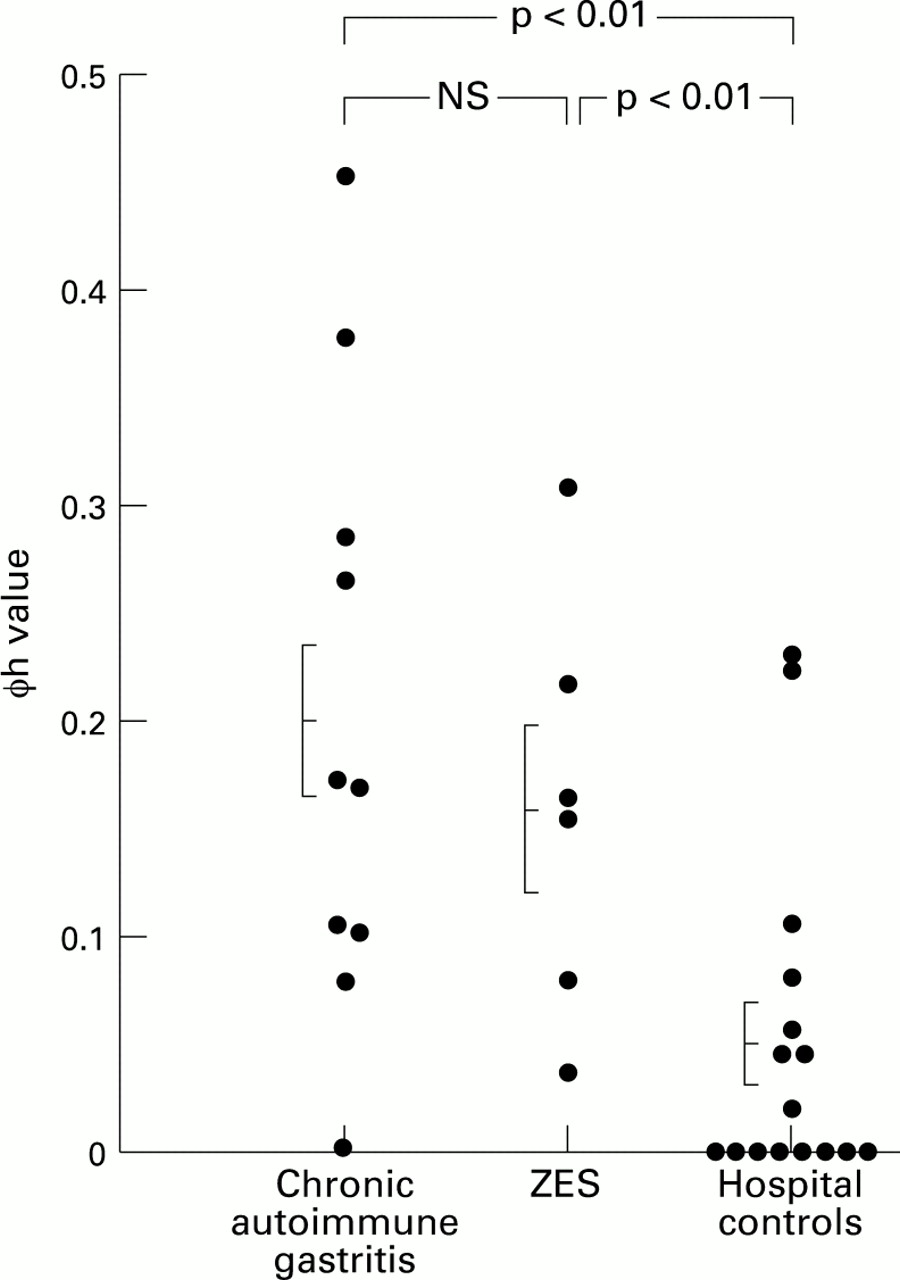
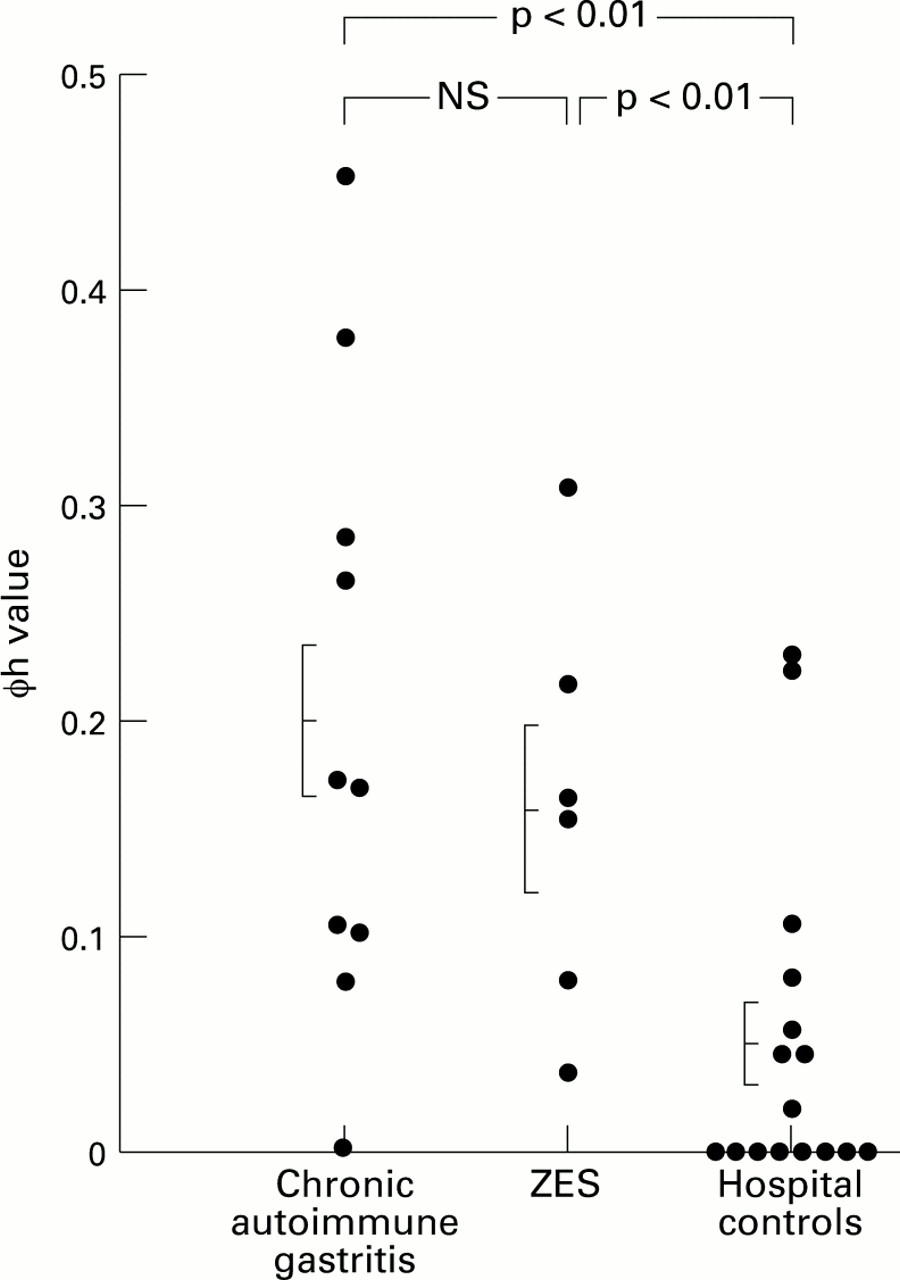{kind=link}
: Individual and mean (SEM) φh values in patient groups and controls (Mann-Whitney U test).
No correlation was found between serum gastrin concentrations and any proliferative index in either patient group or in controls.
Discussion
Patients with autoimmune CAG or ZES show an abnormal pattern of rectal cell renewal. An upward shift of the proliferative compartments in glandular crypts is a constant finding. The percentage of proliferating cells in the entire crypts was similar in patients and controls. Results suggest that the upward expansion of the proliferative compartments is not related to the increase in cell turnover but rather to a defect of cells migrating towards the surface.
Other studies demonstrated cell proliferation abnormalities in patients with ZES.12 However, these authors found an overall increased cell turnover (as indicated by an increased LI), which was not found in our series. This discrepancy can be explained by differing duration of the disease or treatment, as well as differences in cell counts. However, the discrepancies are not relevant to the consideration of the role of hypergastrinaemia in inducing cell proliferation abnormalities.
The expansion of the proliferative compartment was suggested by an increased φh value in patients with CAG or ZES compared with controls. This proliferative feature may be indicative of an increased risk of colon cancer. There is, in fact, evidence that individuals at high risk for colon cancer, such as those with colonic adenomas or long-standing ulcerative colitis, have high φh values in their rectal flat mucosa.11 ,13-16
Our results agree with some clinical observations suggesting that patients with colonic neoplasia have raised gastrin concentrations.17 ,18 Because normal and neoplastic epithelial cells of the colon have receptors for gastrin,19 ,20 increased gastrin production may lead to altered proliferation and progression to neoplasia.
A clinical implication of our results relates to the safety of the treatment of acid related diseases. In particular, administration of powerful antisecretory drugs such as cimetidine, ranitidine, or omeprazole, which can increase serum gastrin concentrations.21 ,22 Some studies on animals failed to show any adverse effect on the colonic mucosa following chronic administration of gastric acid inhibitors,23 while others showed enhanced colonic proliferation and raised serum gastrin concentrations in rats treated with omeprazole.24 Studies in humans are inconclusive. Festen et al observed a significant increase in serum gastrin and pepsinogen I concentrations after treatment with omeprazole.21 Graffner et al found no influence on tumour growth of omeprazole induced hypergastrinaemia.25 Interestingly, Orbuch et al did not see any increase in the frequency of colon cancer in 97 patients with ZES despite hypergastrinaemia.26 Studies on humans are warranted because of the worldwide consumption of these compounds.
Acknowledgments
This work was supported in part by a grant from the University of Bologna (60% funds).