Article Text

Abstract
Background—Most ulcers are caused, one can deduce, by Helicobcter pylori or by use of non-steroidal anti-inflammatory drugs (NSAIDs). Whether both together are worse than one alone is something that is quite unknown.
Aim—To study both factors in order to see whether they interact together positively.
Method—A case control study of ulcer bleeding in elderly patients chosen without weeding.
Results—NSAID usage increased risk substantially. So did H pylori infection (but relative risk less than three). Neither seemed to interact. Their actions were discretely intact.
Conclusion—H pylori effects ulcer bleeding in an adverse manner but does not make the risk of NSAIDs worse.
- peptic ulcer
- gastric ulcer
- duodenal ulcer
- haematemesis
- melaena
- NSAIDs
- Helicobacter pylori
Statistics from Altmetric.com
It is now established that most peptic ulcers are caused byHelicobacter pylori or non-steroidal anti-inflammatory drugs (NSAIDs).1-7 The prevalence of H pylori infection rises with age. For example, in one study, it was 29.7% in those less than 30 years old and was 63% at age 55–65.8 However, it is less clear whether H pylori or NSAIDs act independently or synergistically in the development of dyspepsia, ulcers and ulcer complications. Such information would be important in understanding pathogenesis and identifying patients at particularly high risk of ulcer complications. We therefore investigated whether H pylori and NSAID usage interacted to increase the risk of developing peptic ulcer bleeding in the elderly.
Methods
SUBJECTS AND DRUG USAGE
Our subjects were derived from 487 patients over the age of 60 who were consecutively admitted to the two acute Nottingham hospitals (University and City Hospitals) with peptic ulcer bleeding between April 1986 and January 1991, and 480 age and sex matched controls identified at the time of admission. Drug usage by cases and controls was established prospectively by using a structured questionnaire in the context of studies reported elsewhere.5 ,7
H PYLORI STATUS
In 1993, 166 cases and 205 controls were identified as still alive and residing locally. Their general practitioners were asked to identify those whom it was appropriate to approach for a blood sample. These patients were visited at home and a serum sample obtained forH pylori serology status using the Porton Cambridge Helico G ELISA test.9 The manufacturer’s recommended cut-off value of 10 units per ml, validated in our laboratories, was used to define patient serology as positive or negative.
STATISTICAL METHODS
Logistic regression analysis was used to quantify the influence of risk factors. Variables entered into the model were age, NSAID usage,H pylori status, and H pylori/NSAID interaction. We hoped to study 100 cases and 100 controls in order to have 90% power to detect anticipated differences in NSAID usage of 35% v 15% and 95% power to detect anticipated differences for H pylori prevalence of 75% v50% in cases v controls. Although only 175 subjects could be studied, the study still had 85% power to detect the anticipated differences in NSAID usage and 90% power to detect the anticipated differences in H pylori prevalence.
Results
PATIENTS
Permission was obtained to study 201 patients and blood samples were obtained from 175 (82 cases, 93 controls, 87% response rate). The groups were well matched for age and sex, but the cases were significantly more likely to have used NSAIDs, and more likely (borderline significance) to have positive H pyloriserology (table 1). Thus, 41% of patients were taking non-aspirin NSAIDs as opposed to 18% of controls. For aspirin the comparable figures were 27% v 16%. Seventy per cent of patients had serological evidence of H pylori infection as opposed to 56% of controls.
Patient characteristics
At initial presentation, the mean (SD) age of the population, from which the patients studied were drawn, was 73.3 (7.9) years. As the mean interval between presentation and current study was 34.2 months, the age of the patients studied very closely reflects that of the overall population. Similarly, 56% of those studied were male compared with 55% of the original population. Overall NSAID use in the patients studied was 59%, the same as in the original population. Thus, the patients we have studied seem to be representative of the population as a whole.
DETERMINANTS OF ULCER BLEEDING RISK
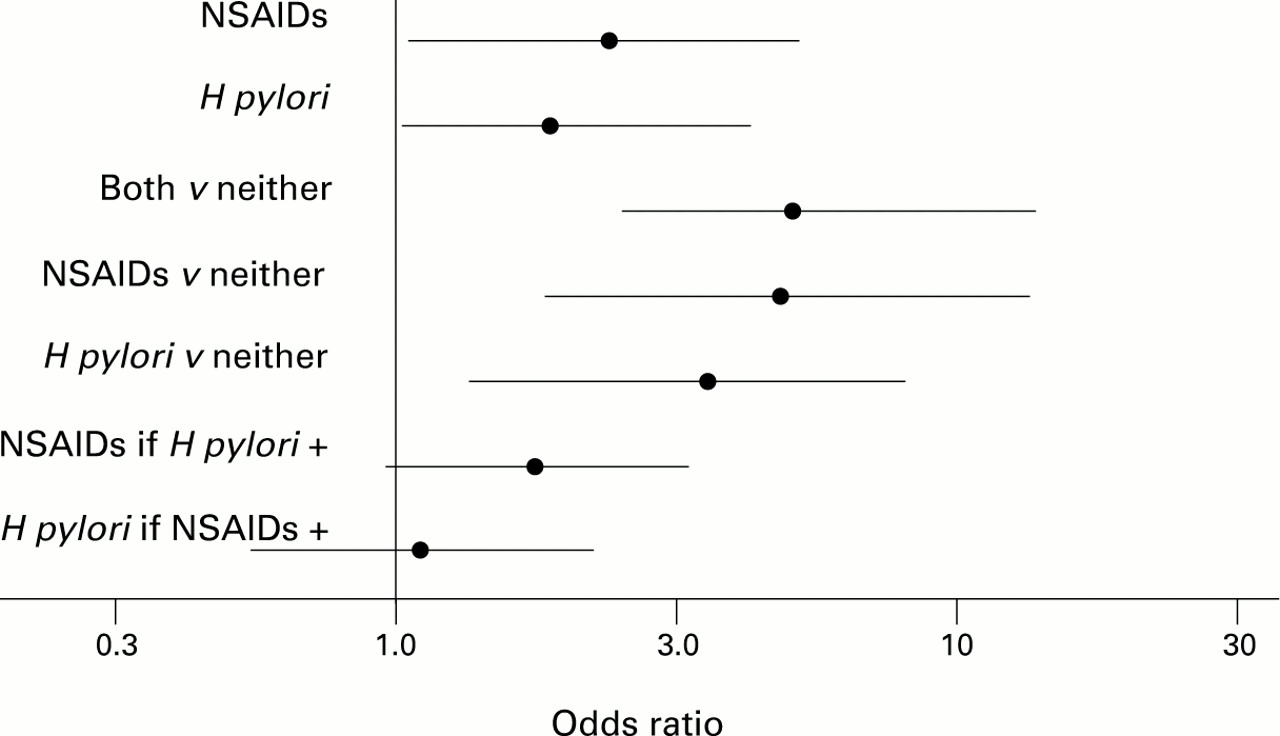
The logistic regression analysis identified both NSAID usage andH pylori as significant influences on the risk of developing ulcer bleeding (fig 1; table 2). The interaction term was less than one, with 95% confidence intervals (CI; 0.11–1.59) compatible with a relation ranging from notably less than additive through to, at most, minor synergy. In patients infected with H pylori, the further increase in risk associated with NSAIDs was of borderline significance (age adjusted odds ratio (OR) 2.04, 95% CI 0.95–4.39). In patients taking NSAIDs infection with H pyloridid not significantly increase risk further (age adjusted OR 1.16, 95% CI, 0.44–3.03 and the age adjusted OR for patients with both risk factors compared with none was only 5.72 (2.18–15.07). This was not significantly greater than the OR of 4.93 (1.63–14.88) for NSAIDs alone.

: Odds ratios for ulcer bleeding associated with NSAID usage and H pylori alone and in combination. Means and 95% confidence intervals are shown.
Logistic regression analysis: adjusted odds ratios
DUODENAL AND GASTRIC ULCER
Forty one patients had a bleeding from gastric ulceration, 39 had duodenal ulcers and two patients had both gastric and duodenal ulcers. For patients taking NSAIDs the overall OR for gastric ulcer bleeding was 5.67 (1.36–23.58, p=0.017) and for duodenal ulcer bleeding 2.24 (0.62–8.02, p=0.22). The interaction term was 0.31 (0.06–1.63). ForH pylori the overall OR for gastric ulceration was 2.89 (0.72–11.05, p=0.12), and for duodenal ulceration 2.18 (0.72–6.61, p=0.17). The interaction term was 0.64 (0.14–2.91). The data for NSAIDs alone and in combination are shown graphically in fig2.

: Odds ratios for gastric and duodenal ulcer bleeding associated with NSAID usage and H pylori infection alone and in combination. Means and 95% confidence intervals are shown. Closed circles, duodenal ulcer; closed squares, gastric ulcer.
ASPIRIN AND NON-ASPIRIN NSAIDs
Both aspirin and non-aspirin NSAIDs were associated with increased ORs for ulcer bleeding. With aspirin the overall OR (for both H pylori infected and uninfected subjects) was 2.6 (1.2–5.7). For non-aspirin NSAIDs the comparable OR was 3.3 (1.6–6.7; fig 3). Both aspirin and non-aspirin NSAIDs seemed to increase risks in H pylori infected and uninfected individuals when considered separately but confidence intervals were wide (fig3).

{kind=link}
{kind=link}
{kind=link}
: Odds ratio for ulcer bleeding associated with aspirin (open triangles) and non-aspirin NSAID (closed triangles) usage in relation to H pylori status.
Discussion
Our data show that NSAID usage and H pylori infection both increase the risk of bleeding peptic ulcer in the elderly. For NSAIDs, this relation is well known.1-6 For H pylori several previous studies have drawn attention to a relative under representation of H pylori in a series of bleeding or perforated peptic ulcers.10 ,11 In one study, the prevalence of H pylori in patients presenting with duodenal bleeding ulcer was only 72%.10Likewise, in a study of ulcer perforation, 47% of patients with a perforated duodenal ulcer had evidence of H pyloriinfection compared with 50% of controls.11 Unfortunately, in these studies NSAID usage was not determined in a systematic prospective fashion.
In our study, NSAID usage was determined prospectively using a structured questionnaire administered to both cases and matched controls who were subsequently tested for serological evidence ofH pylori infection. Fifty six per cent of our control patients had serological evidence of H pylori infection, consistent with previous reports in patients of similar age in the United Kingdom.8 ,12 Only 70% of patients presenting with ulcer bleeding had serological evidence of infection. For both gastric and duodenal ulcer there were similar numbers of H pylorinegative patients. Our data thus support the relative under representation of H pylori seen in earlier studies.
The results of our study permit some estimate of the extent to which there is any interaction between H pylori and NSAIDs as risk factors, although the relatively small size of the study means that such estimates should be treated with considerable caution. Nevertheless, although the 95% confidence intervals for the interaction term in our study were wide, the upper confidence interval does not exceed unity by a substantial amount, making it unlikely thatH pylori status has a major synergistic effect on the risk of ulcer bleeding associated with NSAID usage. Indeed, it seems more likely from our data that H pylori does not substantially affect the risks of NSAID usage. Direct comparison of risk in NSAID users who were infected with H pylori with those that were not showed a 1.1 (0.4–2.9) fold difference only. Similar data supporting the notion that NSAIDs and H pylori act independently or at most interact to a limited extent have recently been presented to the American Gastroenterological Association.13
Our study had several potential weaknesses. Cases and controls were not matched directly. However, they came from originally matched populations and were very similar. NSAID usage and H pylori status were not defined simultaneously. However, none of those studied had H pylori eradication treatment and were in an age group where spontaneous acquisition or elimination of the organism are rare. H pylori status was established serologically but there is good correlation between serology and other measures of infection.14 Serology was well suited to our study compared with breath or mucosal urease testing, being unaffected by use of proton pump inhibitors, and more likely to identify as positive infected patients who had become H pylorinegative since the original presentation. As reported elsewhere,8 the death rate following admission with gastrointestinal bleeding was higher in cases than controls. This was mainly from respiratory conditions and from cancers not known to be associated with H pylori infection. There was also a higher cardiovascular death rate. As ischaemic heart disease has been suggested to be more common in patients infected with H pylori,15 it is possible that selective depletion of patients with H pylori could have occurred. However, whether there is a true and unconfounded association between H pylori and ischaemic heart disease is controversial.16 ,17 Moreover, even if true, such an association would have a limited impact in our study. In our earlier study of the population from which the present patients were drawn there was an excess of cardiovascular mortality amounting to 9.2 deaths or 1.55 pro rata for the population we studied. Even if all excess cardiovascular deaths had been associated with H pylori,this would only have had a marginal impact on the estimates of risk associated with H pylori in the present study.
Our data are therefore good evidence that H pylori and NSAIDs act as largely independent risk factors. In addition, it is more likely that any interaction between them is a negative rather than a synergistic one. This could arise if NSAIDs and H pyloriincreased the risk of bleeding peptic ulcer by independent mechanisms and in different populations, or if one risk factor partially abrogated the hazards of the other to an extent roughly equal to its own toxicity. One possibility is that H pylori, by stimulating prostaglandin synthesis thereby partially reverses the intrinsic toxicity of NSAIDs.18 In practical terms, our data do not suggest that H pylori is a useful marker of increased risk in patients taking NSAIDs. Likewise our findings do not support the growing tendency to eradicate H pylori infection in NSAID users. Only a clinical trial can determine whether this is beneficial, valueless or harmful.
Acknowledgments
We thank Dr Ian Harris for blood group analysis, Mrs Mary Stevenson and Miss Sarah Smith for assistance with data entry and analysis, Mr Robert Cave for the large amount of time he has contributed and Miss Donna Hall, Miss Claire Spencer and Mrs Rosemary Dainty for preparation of the manuscript.
References
Linked Articles
- EDITORIAL