Article Text

Abstract
Aim—To evaluate the incidence of Crohn’s disease in Stockholm County between 1955 and 1989.
Methods—A cohort of 1936 patients with Crohn’s disease was retrospectively assembled. Incidence rates and changes in disease distribution were assessed.
Results—The mean increase in incidence was 15% (95% confidence intervals 12% to 18%) per five year period with a mean annual incidence rate at 4.6/105during the last two decades. The mean incidence for the entire study period was similar for men and women. The mean age at diagnosis increased from 25 years in 1960–64 to 32 years in 1985–89, partly because of an increasing proportion of patients aged at least 60 years at diagnosis. The proportion of patients with colonic Crohn’s disease at the time of diagnosis increased from 15% to 32% (17% difference; 95% confidence intervals 12% to 23%) whereas the proportion of patients with ileocaecal disease decreased from 58% to 41% (17% difference; 95% confidence intervals 10% to 24%) during the study period. Elderly patients had a higher proportion of small bowel disease and a lower proportion of ileocolonic disease compared with the younger patients.
Conclusion—The incidence rate of Crohn’s disease in Stockholm has stabilised at 4.6/105 and the proportion of elderly patients has increased during a 35 year period. Colonic Crohn’s disease has increased in frequency with a reciprocal decrease in ileocaecal disease.
- Crohn’s disease
- inflammatory bowel disease
- incidence
- epidemiology
Statistics from Altmetric.com
The first epidemiological studies of Crohn’s disease were performed during the 1960s.1 ,2 Several studies with varying study designs, numbers of patients included, and length of study periods have been published since then. Most studies are based on 200–850 patients during study periods ranging from 15 to 25 years. The incidence rate of Crohn’s disease was reported to increase gradually during the 1960s and 1970s.3-7 Thereafter most studies showed either a plateau3 ,6 or a slight increase in the incidence rate during the late 1970s and 1980s.4 ,7 ,8Some studies have indicated a more substantial increase through the 1980s.9 ,10 In a previous study of Crohn’s disease in Stockholm,11 the incidence rate of Crohn’s disease was found to increase between 1955 and 1973.
There is an apparent north-south gradient in the incidence rates of Crohn’s disease with a higher incidence rate of Crohn’s disease in Scandinavia, northern Europe, and North America3 ,5-10compared with southern Europe, Africa, and Asia.12-14
Ileocaecal Crohn’s disease used to be the most common site of disease at the time of diagnosis but colonic Crohn’s disease appears to have become more frequent in recent years.4 ,9 ,10 ,15 ,16 A possible shift in the age panorama in Crohn’s disease with a greater proportion of elderly patients may contribute to a changed pattern of disease localisation at the time of diagnosis.
The primary aim of this study was to estimate the incidence rate of Crohn’s disease and localisation of disease at diagnosis, in relation to time, sex, and age at diagnosis, in a cohort of patients in a well defined population during a 35 year study period.
Materials and Methods
STUDY AREA
Stockholm, the capital of Sweden, and its surroundings covers an area of 6490 km2 with both rural and urban parts. During the study period there were 14 major hospitals caring for patients with inflammatory bowel diseases (IBD). Traditionally, general practitioners (GPs) have rarely treated patients with IBD in Stockholm and the number of Crohn’s disease cases being treated only by GPs has thus been negligible. Furthermore, there have been few gastroenterologists in private practice in Stockholm.
POPULATION
All information about the population in the County has been obtained from the national central statistical register (Statistics Sweden).17 Before 1965 data were only available for five year intervals. The annual population and classification into sex and different age groups have therefore been estimated from the figures available for 1955, 1960, and 1965. From 1966 and onwards the data are exact.
The total population in Stockholm County increased from 1.18 million inhabitants in 1955 to 1.62 million in 1989. The increase was attributed to births exceeding deaths, and national and international immigration. The mean annual net international immigration was about 4000 (range −3086–10 695) with increasing immigration during the late 1960s, late 1970s, and 1980s. Immigration from Nordic countries was attributed to approximately 60% of immigration during the 1960s and 1970s and 30% during the 1980s. The proportion of aliens varied between 7.9% and 9.8% during the 1970s and 1980s.
The female:male ratio of the population was fairly steady during the study period with a ratio of 1.11:1 in 1955, 1.06:1 in 1974, and 1.06:1 in 1989.
CASE IDENTIFICATION
From 1955 to 1959 all diagnoses for inpatients were registered manually. From 1960 to 1969 a gradual transition to computer registration took place and since 1969 all diagnosis registration for inpatients in Stockholm County has been computerised and stored in a central file.
Diagnoses were registered according to the International Statistical Classification of Disease (ICD-8 1966–86, ICD-9 1987 and onwards). For the years 1955 to 1974 all records that had been registered for any diseases of the gut and peritoneum were searched for possible cases. Records from previous epidemiological studies in Stockholm11 ,18 were scrutinised. Between 1975 and 1984 a survey of possible cases was made in records registered as ulcerative colitis or Crohn’s disease. The assumption of more accurate diagnostic procedures and diagnosis registration over time, resulted in a survey of possible cases among records registered as Crohn’s disease during the period 1985 to 1992. The fact that only 2% of patients originally diagnosed as having ulcerative colitis were reclassified to Crohn’s disease19 also contributed to this restriction.
Until 1993 there was only a diagnosis register for hospital admissions. Since 1993 however, diagnoses have also been registered for all outpatients attending the medical gastroenterology units. These new registers from 1993 to 1994 were therefore also investigated. Finally, gastroenterologists in private practice were also asked about possible cases and the colonoscopy reports were assessed.
CRITERIA FOR DIAGNOSIS AND ADMISSION INTO STUDY
All records mentioned above were scrutinised for fulfilling the admission criteria for the study. All patients who were citizens of Stockholm County and who were diagnosed as having Crohn’s disease between 1 January 1955 and 31 December 1989 were included in the study.
The diagnosis of Crohn’s disease was established according to the criteria adopted by Lennard-Jones.20 Only patients classified as definite or possible cases of Crohn’s disease were included. Date of diagnosis was defined as the date of first examination revealing signs of Crohn’s disease. If the diagnosis had been changed from ulcerative colitis to Crohn’s disease the first diagnosis date of IBD was considered. Date of presentation of symptoms was approximated to months with a certainty expressed as either the first or the fifteenth day of the month. In cases where only the year of onset could be estimated, the date of onset was set at 1 July.
LOCALISATION OF DISEASE AT DIAGNOSIS
The localisation of Crohn’s disease was determined based on the examinations performed at the time of diagnosis. The localisation of disease at diagnosis was classified into six groups: orojejunal disease, small bowel disease (inflammation of the small bowel excluding the distal 30 cm of the terminal ileum), ileocaecal disease (inflammation including the distal 30 cm of the ileum with or without isolated involvement of the caecum), ileocolonic disease (continuous inflammation of the ileum and the colon), discontinuous ileocolonic disease (inflammation in both the colon and the small bowel without continuous inflammation in the ileocaecal region), and colonic disease (inflammation in the colon only and/or rectum). Patients with perianal disease only were included in the latter group.
DATA MANAGEMENT
To achieve completeness of case ascertainment, data collection lasted until 1995. After fulfilling the criteria for admission all records were scrutinised. Data with reference to date of birth, date of onset of symptoms, date of diagnosis, localisation of disease at diagnosis, and sex were extracted and transferred to a data file for further calculations. The incidence was calculated for each year separately for men and women by dividing the number of new cases by the corresponding population. The annual incidence was adjusted for sex and age using the population in Stockholm County in 1975 as a standard population. The localisation of disease at time of diagnosis was classified into six groups as detailed above. For this study, those aged at least 60 years at diagnosis were considered as elderly. Age at diagnosis for birth cohorts was chosen by five year intervals ± 2.5 years. The age specific incidence for each birth cohort was achieved by dividing the number of cases in each five year group by the mean of the population of corresponding age for the particular year. Age specific incidences were then expressed as the mean for five year birth cohorts.
STATISTICAL METHODS
Incidence rates are expressed as cases per 105inhabitants. Incidence figures for five year periods are expressed as mean incidence rate with a 95% confidence interval (CI) based on the assumption that the number of cases follows a Poisson distribution. Age at diagnosis and time between symptoms and diagnosis were calculated as medians. Proportions of disease localisation are expressed as percentages of the total number of cases. The 95% confidence interval for the difference in proportions was calculated assuming a normal approximation of the binominal distribution. To study time trends in incidence rates, changes in age and sex distribution were accounted for by means of a multiplicative Poisson model which standardises for age and sex and compares each five year period with the first five year period, 1955–59, through the relative risk.21 This model was also used to estimate the average five year change in the incidence rates.
The study was approved by the Ethics Committee at Huddinge University Hospital.
Results
PATIENTS
Table 1 presents data for the 1936 patients included in the study. A total of 1415 patients (73%) had a definite diagnosis of Crohn’s disease and 521 patients (27%) had a possible diagnosis of Crohn’s disease. Case identification by the outpatient register identified 63 cases that never had been hospitalised, 22 patients that had been reclassified from ulcerative colitis to Crohn’s disease as outpatients, and 17 patients previously hospitalised due to various other diagnoses. Of 16 additional patients found at the gastroenterologists in private practice, 10 were diagnosed during outpatient attendance and six patients had been reclassified from ulcerative colitis to Crohn’s disease.
New cases of Crohn’s disease in Stockholm County 1955–89 grouped by five year intervals of diagnosis in relation to sex, age at diagnosis, and localisation of disease at diagnosis
Information on localisation of disease at diagnosis was not available for three patients and information on time for onset of symptoms was not available for 13 patients.
INCIDENCE
Table 2 presents incidence rates. The highest annual incidence rate was found in 1973 with 5.9 cases per 105 inhabitants. During the last two decades of the study period the incidence remained stable at a mean of 4.6. The mean incidence over the entire study period was similar in men (3.6, 95% CI 3.1 to 4.1) and women (3.8, 95% CI 3.3 to 4.3), although there was a tendency to a higher female incidence during 1970–84.
Standardised annual incidence 1955–89
The mean increase in incidence per five year period in subjects aged 15 years or more was estimated to be 15% (95% CI 12% to 18%) for both sexes combined (14% (95% CI 10% to 18%) for men; 15% (95% CI 11% to 19%) for women).
Figure 1 shows the change in age specific incidence for Crohn’s disease over time. The mean increase in age specific incidence per five year period varied between 10% (95% CI 7% to 14%) for the patients aged 15–29 years and 22% (95% CI 12% to 33%) for elderly patients. The moderate mean increase in the younger age group was due to a decrease in the incidence among men between 1970–74 and 1980–84.

: The age specific incidence rates of Crohn’s disease between 1955–59 and 1985–89. The relative risk of Crohn’s disease for each five year period is compared with the first period (1955–59).
AGE AT DIAGNOSIS
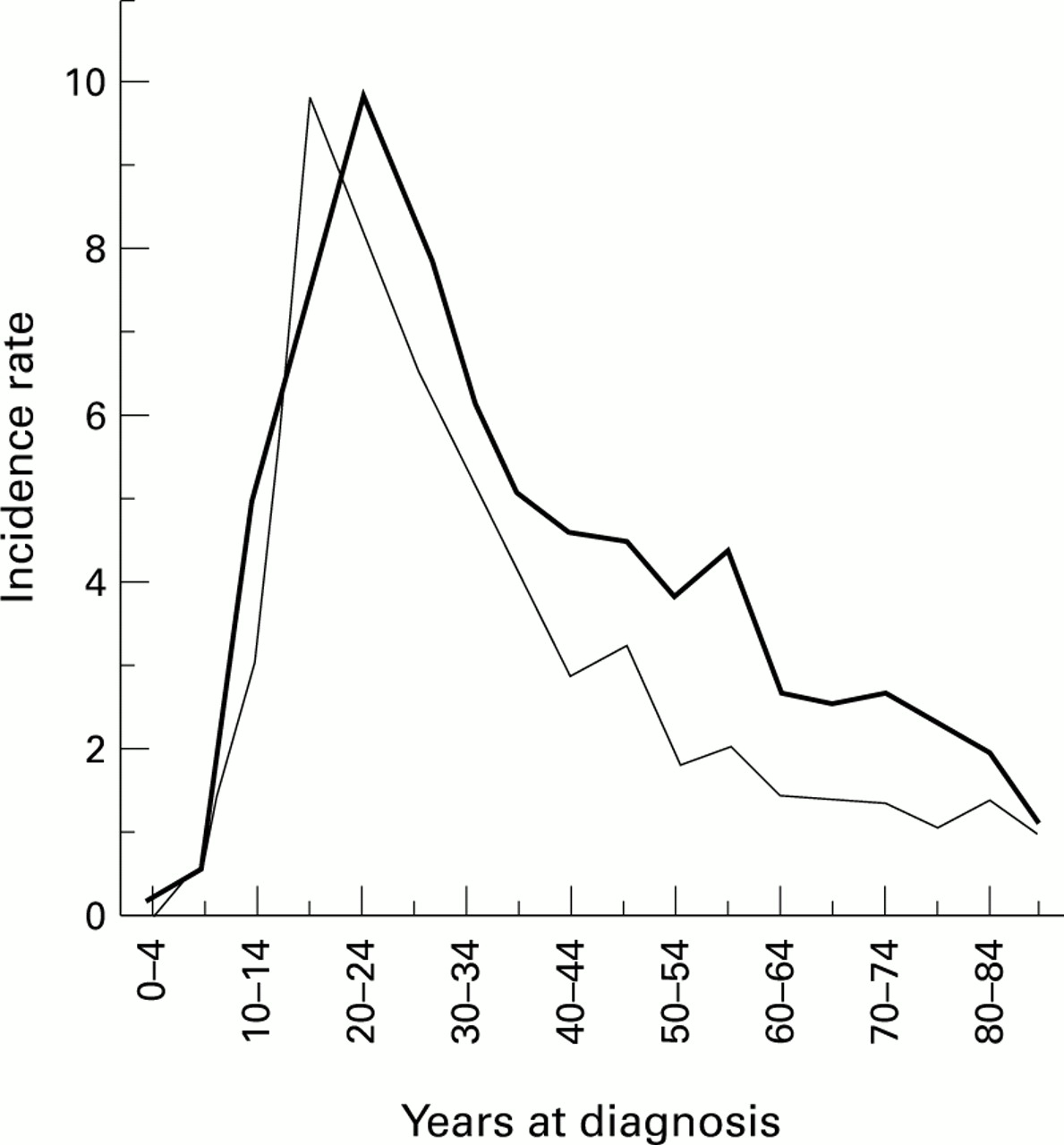
The highest age specific incidence was found among those aged 15–29 years (fig 2). Thereafter the incidence declined with increasing age without any indication of an overall second peak in the elderly. However, there was an indication of a second peak in the incidence for those aged 55–59 years at diagnosis during 1975–89.
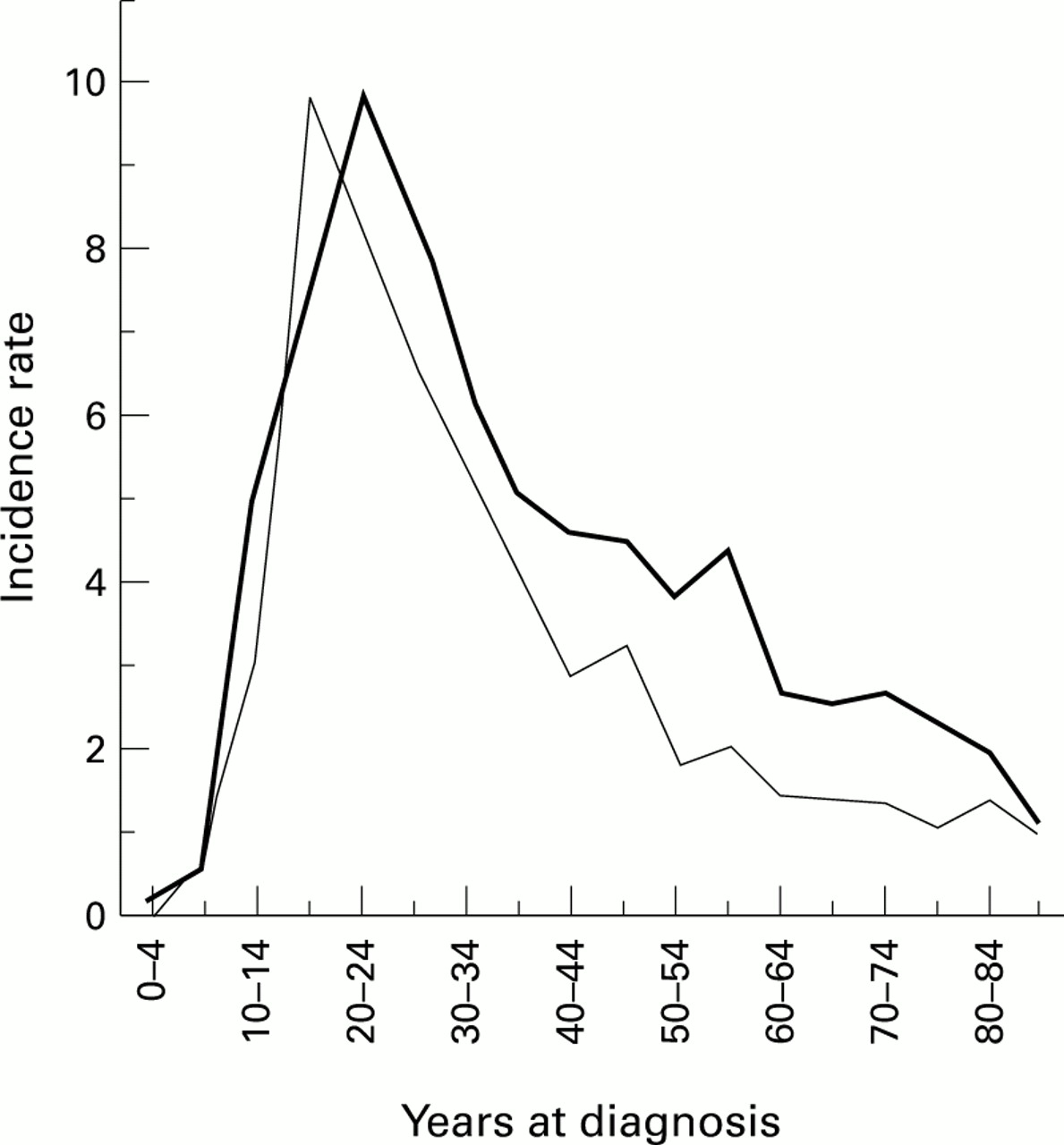
: Age specific indicence rates of Crohn’s disease per 105 inhabitants as mean of two 15 year periods (1960–74, thin line; 1975–89, thick line).
The median age at diagnosis (table 3) for the whole period was 29 years (range 3–89 years). Ignoring the first five year period, the median age increased from 25 years in 1960–64 to 32 years in 1985–89. Simultaneously, the proportion of elderly patients increased from 3.4% to 12.2% with a difference in proportions of 8.8% (95% CI 4.5% to 13.1%). When the elderly patients (n=170) are excluded, the median age at diagnosis still increased from 23 to 29 years during the period.
Median age at diagnosis
TIME BETWEEN ONSET OF SYMPTOMS AND DIAGNOSIS
The median time between onset of symptoms and diagnosis for the whole period was seven months (range 0–599). The longest time span between onset of symptoms and diagnosis was found in 1955–59 (10.5 months), although there was only a few months difference between all five year periods.
BIRTH COHORTS
Birth cohorts were chosen as five year birth cohorts between 1931 and 1965 (fig 3). All cohorts were not completely represented as the study period lasted between 1955 and 1989. Those in the early cohorts who were diagnosed at a young age and those in the later cohorts who were diagnosed at a higher age are not shown. Those born in 1946–50 had an overall higher age specific incidence at age 20–30 years. This cohort had a total higher mean incidence compared with those born in 1941–45 (8.4 (95% CI 6.8 to 10.0) versus 5.7 (95% CI 4.7 to 6.7)) but not compared with any other cohort.

: Age specific incidence rates of Crohn’s disease per 105 inhabitants for different birth cohorts as means of five or 10 year cohorts.
LOCALISATION OF DISEASE AT DIAGNOSIS
Figure 4 shows the localisation of disease at diagnosis. The only difference with respect to sex was found in the group with small bowel disease: 7.4% of the men had small bowel disease compared with 4.4% of women (3% difference, 95% CI 0.9% to 5.1%).

: Localisation of disease at diagnosis. Mean proportions of total cases in 1955–64 and 1980–89.
Comparing the patients with the highest age specific incidence (15–29 years at diagnosis) with the rest of the patients yielded a significantly different pattern of disease localisation at diagnosis. Those who were diagnosed at the age of 15–29 years particularly had more ileocolonic disease (21.5% versus 12.7%, difference = 8.8%, 95% CI 5.4% to 12.2%) and less ileocaecal disease (43.3% versus 50.0%, difference = 6.7%, 95% CI 2.2% to 11.2%) compared with the rest of the patients. The proportion of colonic disease was similar in the two groups (26.1% versus 26.6%).
Among the elderly patients, there was a higher proportion of disease involving the small bowel (13.7% versus 5.0%, difference = 8.7%, 95% CI 3.4% to 14.0%) and a lower proportion of ileocolonic disease compared with those below the age of 60 at time of diagnosis (9.5% versus 17.3%, difference = 7.8%, 95% CI 3.0% to 12.6%). Again, the proportion of colonic disease was found to be similar in both groups.
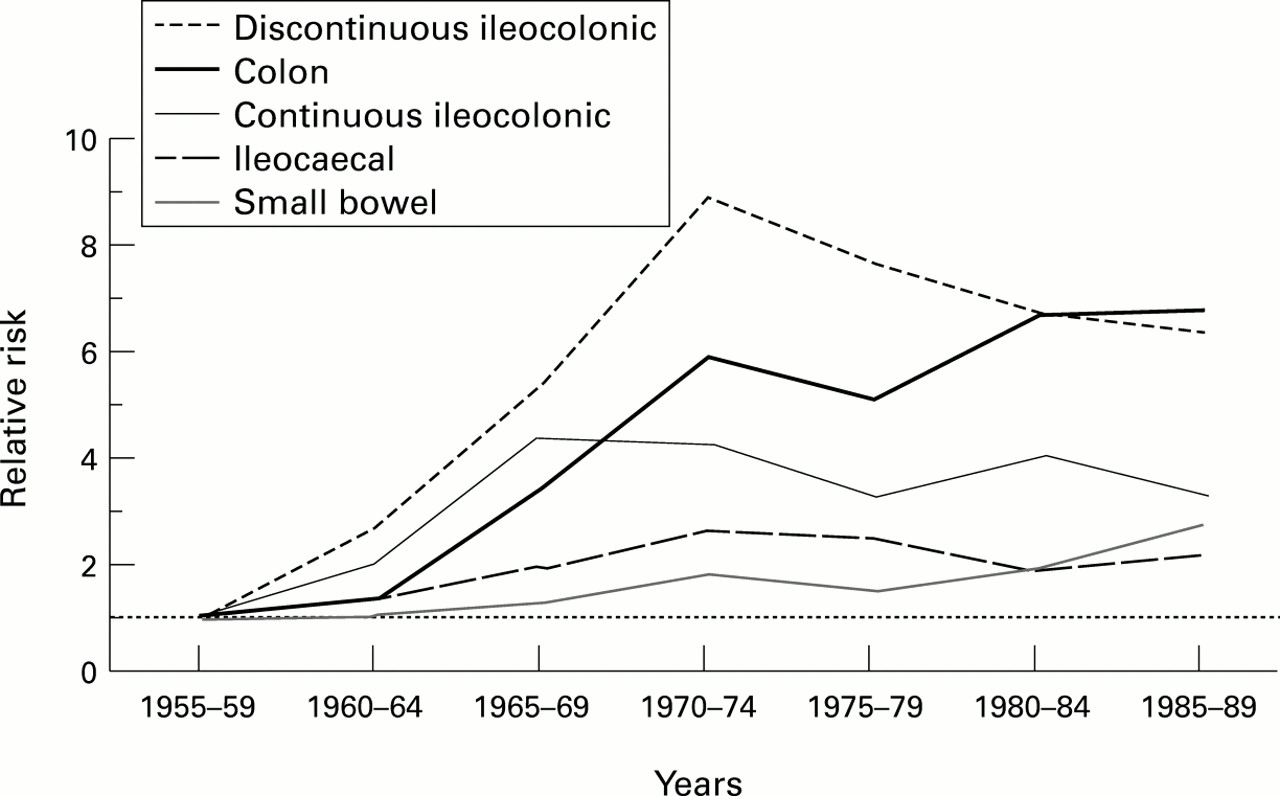
Figure 5 shows the incidence rates by localisation of disease at diagnosis, in patients aged 15 years or more, over time. The mean increase in incidence of colonic disease was 28% (95% CI 22% to 34%) per five year period while the corresponding increases for ileocaecal disease and continuous ileocolonic disease were 9% (95% CI 5% to 13%) and 11% (95% CI 4% to 17%) respectively. Discontinuous ileocolonic disease and small bowel disease incidences increased with a mean of 16% (95% CI 1% to 35%) and 19% (95% CI 7% to 32%) respectively per five year period. Between the first and last 10 year periods of the study, the proportion of colonic disease doubled from 15% to 32% (17% difference, 95% CI 12% to 23%) while the proportion of ileocaecal disease decreased from 58% to 41% (17% difference, 95% CI 10% to 24%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
: The incidence rates of Crohn’s disease between 1955–59 and 1985–89 by localisation of disease at diagnosis. The relative risk of Crohn’s disease for each five year period is compared with the first period (1955–59).
Discussion
The results from this large long term retrospective study are in accordance with former published studies showing an increased incidence rate of Crohn’s disease during the 1960s and the 1970s with a subsequent stable incidence during the 1980s. Only one study5 has shown a decreased incidence during the last years of the study period. Case ascertainment during the last years of a study period are often more unreliable, thus resulting in a false low number of identified cases. However, in this study there was a tendency towards an increased incidence during the last five years of the study period although this was not statistically significant. This may be due to the relatively long period of case ascertainment after the study period (seven years).
Assessment of outpatient registers and gastroenterologists in private practice contributed 6% of the total number of patients. The number of patients that had never been hospitalised due to Crohn’s disease was small (n=73, 3.8%), indicating that most Crohn’s disease patients become hospitalised sooner or later and consequently hospital based Crohn’s disease studies such as ours should be regarded as reliable for epidemiological purposes.
There are obvious differences in incidence rates around the world and even some variations between areas close to each other and in the same country. An incidence variation of five to seven per 105inhabitants was found between three different areas in Sweden (Malmö,22 Uppsala,3 and Örebro6). The incidence rate in this study is lower than in any of those studies even though registers of inpatients, outpatients and private gastroenterologists were reviewed. Differences in incidence could be explained by different study designs, case ascertainment, and diagnostic criteria; the present study has nevertheless been performed in an almost similar manner to the other Swedish studies. Bias due to significant age differences in the general population in Sweden is unlikely as the age specific incidence in the highest exposed group (15–29 years) was found to be lower in Stockholm compared with the three other areas. About 2% and 4% respectively of patients originally diagnosed as having ulcerative colitis in Stockholm between 1955 and 1984 were subsequently reclassified as Crohn’s disease during two different subsequent time periods. Theoretically, the annual mean incidence could thus have been also underestimated in the subsequent five year period 1985–89, but this was unlikely to have been by more than 0.15 per 105 (3% of an overall incidence of approximately 5 per 105). As the diagnostic accuracy has improved during the 35 year study period the possible risk of underestimation due to misclassification between ulcerative colitis and colonic Crohn’s disease has most probably become lower. Moreover, most of such overlooked patients would probably have been found by the outpatient register review, and the number of possible additional cases should thus be very limited.
According to the north-south gradient an increased number of international immigrants might cause a dilution effect with a false low incidence rate. Some of the difference between the incidence rate found in our study and other Swedish studies could be explained by a 5% and 3% higher proportion of immigrants in Stockholm County compared with Örebro and Uppsala respectively. However, the total standardised incidence in Stockholm is similar to that found in northern Sweden,23 Copenhagen,7Germany,24 ,25 and France26 but lower than the incidence in Great Britain.4 ,8-10
Generally, it is believed that the incidence rate is higher among women than among men4 ,5 ,7 ,8 ,10 ,26 although several studies have not found any difference.6 ,16 ,23 ,24 ,27 In this study, the mean incidence for the whole period was similar for men and women although there was a higher incidence rate among women during the period 1980–84. Nevertheless, the total increase of the incidence during 1985 to 1989 was due to a higher incidence among men.
The highest age specific incidence was found among those aged 15–29 at diagnosis in agreement with all previous studies. This was the only age specific group with a declining incidence through the latter part of the study period. As smoking is an established risk factor for Crohn’s disease,28-30 changed smoking habits in Sweden during the past 30 years may hypothetically have influenced the incidence of Crohn’s disease during this period. The age specific incidence decline was principally caused by a decreased incidence among men. Men have gradually tended to smoke less since the 1960s whereas women tended to smoke more during the same period,31-33 even though the prevalence of cigarette smoking has generally decreased in Sweden from 1977 onwards. A corresponding hypothesis about the impact of changed smoking habits on the incidence of ulcerative colitis has previously been presented.34
The disease incidence among women between 1980 and 1984 is in accordance with recent reports from other areas.16 ,25
Some studies have showed a bimodal9 ,10 ,35 or even a trimodal36 age specific distribution with a second peak in the elderly. Considering all cases together we could not find any clear second peak in this study. If the material is subdivided into two groups: those diagnosed during 1960–74 and during 1975–89, a second peak at the age of 45–49 appears during the first period and a second peak at the age of 55–59 during the last period. The latter peak, however is made up of only 17 men aged 55–59 diagnosed between 1985 and 1989. Further investigation is required as to whether this is a cluster, a real second peak, or a chance finding.
The median age at time of diagnosis increased from 25 years in 1960–64 to 32 years in 1985–89. A similarly increasing age at diagnosis over time was found in Örebro,6 Copenhagen,7 and Uppsala3 whereas the median age in France26was 26.5 years in 1988–90. The increase of the median age at diagnosis in our study was attributed both to a shift towards diagnosis in a five year older age specific group, and to an increased proportion of patients aged at least 60 years at the time of diagnosis. The proportion of elderly actually increased from 3% to 12% between 1960–64 and 1985–89. The increase was due to an increasing age specific incidence, as shown in fig 1, although an altered age structure in the population may also have had an influence. An increase in the median age at diagnosis could have been influenced by a long time span between onset of symptoms and date of diagnosis. In this study, however, the median time span only differed by a few months.
Finding a birth cohort with a higher incidence of Crohn’s disease may give some clue to the still unknown aetiology of the disease. There have been conflicting results in the few studies which have tried to demonstrate birth cohorts in this respect. Three studies6 ,7 ,10 could not demonstrate any cohort effect but Ekbom et al 3 found a birth cohort phenomenon for Crohn’s disease and ulcerative colitis combined for those born between 1945 and 1954. The present study confirms our previous results11 that a birth cohort phenomenon exists for those born between 1946 and 1950.
Some studies have investigated disease localisation at time of diagnosis. However, difficulties occur as there are disparate classifications in different studies. Our classification into six groups was anticipated, as there was a large cohort, to reveal differences among subgroups of Crohn’s disease patients. Crohn’s disease of the large bowel, which first was described as an entity in 1960,37 has been uniformly classified in most studies. An increasing proportion of colonic Crohn’s disease has been found in several studies,4 ,9 ,10 ,15 ,16 but some studies showed a constant proportion,3 ,7 and one study even showed a slight decrease in colonic disease.6 There have been reports of increasing colonic disease particularly among those aged at least 60 years at diagnosis.4 ,8 ,10 The overall distribution of disease at time of diagnosis in our study was almost identical to that found in Cardiff.10 The pattern of localisation of disease at diagnosis changed during the study period, with an increasing proportion of colonic disease while ileocaecal disease decreased. However, the assumption that the elderly more often have colonic disease could not be verified in this study. The increase of colonic disease was equally distributed among the elderly and those younger than 60 years at time of diagnosis. Instead, the elderly had a greater proportion of small bowel disease and less ileocolonic disease compared with the younger patients. Other conditions of colonic disease among the elderly, particularly ischaemic disease,38 may simulate Crohn’s disease and attribute to misclassification and a higher incidence of colonic Crohn’s disease. In fact those aged 15–29 years at diagnosis constituted the group having a higher proportion of continuous ileocolonic disease and less ileocaecal disease compared with the remainder of the patients.
The increased proportion of colonic disease may be explained by more accurate diagnostic procedures (ileocolonoscopy). The present study shows that the increasing proportion of colonic disease was already evident during the late 1960s although colonoscopy was not introduced in Sweden until the early 1970s. A contemporary decrease in ileocaecal disease and an unchanged proportion of continuous ileocolonic disease also cast doubt on alterations in the diagnostic procedures being the primary explanation for the increased proportion of colonic disease, although improved diagnostic stringency in general may have contributed to the increase. Previous studies7 ,25 ,39 have shown that 3.4–18% of patients with colonic IBD have had their diagnoses changed (mostly from ulcerative colitis to Crohn’s disease) during the study period. As mentioned earlier reclassification only occurred in 3% of the patients in Stockholm. Furthermore, the incidence rate of ulcerative colitis has not decreased in recent years.3 ,40
In conclusion, this large retrospective epidemiological study spanning over 35 years, demonstrates that the incidence of Crohn’s disease in Stockholm County has reached a mean plateau of 4.6 per 105per year during the past 20 years. The age specific incidence among those aged 15–29 has decreased whereas the incidence in elderly patients has increased; the median age at diagnosis has increased from 25 to 32 years. The proportion of colonic disease has increased at the expense of ileocaecal disease, but with no difference with respect to age at diagnosis. Small bowel disease is more common among the elderly than among other age groups.
Acknowledgments
This paper has been published as an abstract (Gut1995; 37 (suppl 2): A187). This study was partly supported by grants from the Karolinska Institute. Bahman Y Farahmand is gratefully acknowledged for help with computer programming.