Article Text

Abstract
Background—Interleukin 1 (IL-1) α and β are potent cytokines which play key roles in inflammation. They are controlled by IL-1 receptor antagonist (IL-1ra).
Aims—To investigate the influence of mucosal inflammation and IL-1ra genotype on the IL-1ra:IL-1 balance.
Patients and methods—IL-1α, IL-1β, and IL-1ra were measured by enzyme linked immunosorbent assay (ELISA) in biopsy specimens taken from inflamed and non-inflamed colon of 60 patients with Crohn’s disease (CD), 34 with ulcerative colitis (UC), 15 inflammatory controls, and 103 non-inflamed controls. IL-1ra genotype was determined by polymerase chain reaction and gel electrophoresis.
Results—IL-1α and IL-1β were significantly increased in inflamed mucosa in inflammatory bowel disease (IBD) (CD: 53.5 (22.4) and 409.9 (118.7) pg/mg protein, respectively; UC: 18.9 (6.8) and 214.5 (78.2) pg/mg, respectively) and non-IBD patients (19.2 (7.4) and 281.4 (121.0) pg/mg, respectively; p<0.0001) compared with normal controls (2.8 (0.6) and 30.6 (5.6) pg/mg, respectively). In CD IL-1α and β were also significantly increased in non-inflamed mucosa (6.1 (1.3) pg/mg and 88.7 (17.4) pg/mg, respectively; p<0.0012). IL-1ra:(IL-1α+β) ratios were significantly decreased in inflamed mucosa of patients with CD (182 (45); p<0.0001), UC (425 (136); p=0.0018) and without IBD (221 (76); p<0.0001), and in non-inflamed mucosa in CD (369 (149); p<0.0001) compared with normal controls (1307 (245); p<0.0001). Patients with IL-1ra genotype 2 had slightly but significantly reduced mucosal IL-1ra concentrations (p=0.003). The greatest difference was seen in colonic biopsy specimens from patients with inflamed Crohn’s disease.
Conclusion—Mucosal inflammation can modulate the balance of the IL-1:IL-1ra system in colonic mucosa.
- interleukin 1
- interleukin 1 receptor antagonist
- inflammatory bowel disease
- Crohn’s disease
- mucosal inflammation
- genotype
Statistics from Altmetric.com
- interleukin 1
- interleukin 1 receptor antagonist
- inflammatory bowel disease
- Crohn’s disease
- mucosal inflammation
- genotype
The aetiology inflammatory bowel disease (IBD) is still unknown. However, from genetic epidemiological studies there is considerable evidence that genetic factors are associated with both Crohn’s disease (CD) and ulcerative colitis (UC).1-4 A study of families with multiple members with CD identified a putative susceptibility locus in the pericentromeric region of chromosome 16.5 In patients with extensive UC, allele 2 of the interleukin 1 (IL-1) receptor antagonist (IL-1ra) gene was found to be significantly overrepresented.6 These statistical data do not however explain the development of chronic inflammation and no connection between distinct genotypes and immunological function has been described so far.
Mucosal inflammation is characterised by an infiltration with neutrophils and mononuclear cells, which on activation are important producers of cytokines and other inflammatory mediators. Among the still growing number of known cytokines, the proinflammatory cytokines IL-1α and IL-1β play key roles, as they are produced early during inflammation and induce production of many other cytokines, amplifying their proinflammatory action.7 Their great proinflammatory potential must be tightly controlled by endogenous inhibitors such as IL-1ra and soluble IL-1 receptors to prevent an acute or chronic overproduction of proinflammatory cytokines, leading to fatal consequences as seen in septic shock.8 ,9 In IBD altered concentrations or altered production of these cytokines have been found in colonic mucosa.10-20 Clinical studies21-26 and animal models provided further evidence that alterations of the cytokine balance can improve or worsen inflammatory bowel diseases.27-29 Little is known however about the factors regulating the local and systemic balance between pro- and anti-inflammatory cytokines. Two previous studies suggested a disturbed balance between IL-1α+β and IL-1ra in inflamed colonic mucosa only from patients with UC and CD.20 ,30 The inflammatory controls in these studies however had less inflammation than the patients with IBD.
In the present paper we studied the influence of diagnosis and inflammation on the production of IL-1α, IL-1β, IL-1ra, and the IL-1ra:IL-1 ratios in the colon using biopsy specimens from patients with and without IBD with similar degrees of inflammation. Furthermore, for the first time we looked for an association between IL-1ra genotype 2 and colonic IL-1ra levels.
Patients and Methods
PATIENTS
Endoscopic biopsy specimens were obtained with informed consent from the colon of 60 patients with CD and Crohn’s colitis (92 biopsy specimens) and from 34 patients with UC (52 biopsy specimens) during routine colonoscopy or sigmoidoscopy. Twenty two of the UC patients had pancolitis and 12 had left sided colitis. Whenever possible, paired biopsy specimens were taken from inflamed and non-inflamed mucosa in order to have the same effects of medication in inflamed and non-inflamed biopsy specimens. This was possible in 23 patients with CD and in 18 patients with UC. For comparison, control biopsy specimens were taken from colonic mucosa of 118 patients without IBD, of which 103 were non-inflammatory controls undergoing colonoscopy for cancer screening or polypectomy. Fifteen patients with diverticulitis (n=3) or infectious colitis (n=12) were used as inflammatory controls. The mean age (SD) of CD patients (29 males, 31 females) was 32 (11) years. Thirty one were taking corticosteroids, 19 were on 5-aminosalicylic acid (5-ASA), four sulphasalazine, and three azathioprine; 21 patients took no medication. The mean age of UC patients (12 males, 22 females) was 43 (18) years. Fourteen were taking corticosteroids, 18 were on 5-ASA, and two sulphasalazine; 12 patients took no medication. The mean age of the non-IBD patients (72 males, 54 females) was 56 (15) years. Five patients took corticosteroids; 119 took no anti-inflammatory medication.
BIOPSY SPECIMENS
The degree of inflammation at the biopsy site was assessed macroscopically as non-inflamed or inflamed. One biopsy specimen for histological assessment and two biopsy specimens for cytokine measurements and for the determination of total protein were taken from essentially the same regions. In some patients one set of three biopsy specimens was taken from an inflamed area and another set of three from a non-inflamed area. Histological assessment of the degree of inflammation correlated well with the macroscopic assessment in controls (p<0.001), CD (p<0.001), and in UC (p<0.001). All macroscopically non-inflamed control patients had no inflammation histologically. Histological grading was performed differently in CD (0 = no inflammation, 1 = discontinuous inflammation without aphthous lesion or ulcers, 2 = superficial aphthous lesions, 3 = deep ulcers or fissures), UC (0 = no inflammation, 1 = one or two crypt abscesses per viewing field, 2 = more than two crpyt abscesses per viewing field, 3 = ulcers and necrosis), and controls (0 = no inflammation, 1 = faint inflammatory infiltrate, 2 = moderate inflammatory infiltrate, 3 = dense inflammatory infiltrate).
The mean (SD) wet weight of biopsy specimens was 8.3 (2.6) mg with no difference between specimens taken from controls (8.5 (2.6) mg), patients with CD (8.2 (2.5) mg), or patients with UC (7.6 (2.4) mg). For cytokine and protein measurements biopsy specimens were washed in phosphate buffered saline (PBS) and then immediately frozen at –20°C.
PROTEIN CONTENT OF COLONIC BIOPSY SPECIMENS
The mean (SD) total protein content per biopsy specimen was 0.38 (0.36) mg. Protein content did not differ significantly between biopsy specimens from patients with CD (0.42 (0.43) mg), UC (0.35 (0.17) mg), and controls (0.36 (0.35) mg). There was no difference in protein content of the biopsy specimens from inflamed and non-inflamed regions (p=0.8). All cytokine and cytokine antagonist concentrations were normalised to total protein content of the biopsy specimens.
MEASUREMENT OF IL-1α, IL-1β, AND IL-1RA PROTEIN CONCENTRATIONS
Two biopsy specimens were homogenised by two cycles of freezing and thawing in 200 μl PBS, pH 7.2, in the presence of proteinase inhibitors (leupeptin 10 mg/ml, pepstatin 10 μg/ml, aprotinin 1 mg/ml, and EDTA 0.5 mg/ml) as described previously.31 Insoluble material was spun down at 18 000g for five minutes. Aliquots of the soluble supernatant were used for the determination of IL-1α, IL-1β, and IL-1ra (R&D Systems, Minneapolis, Minnesota, USA) by enzyme linked immunosorbent assay (ELISA) and for the determination of total protein by BCA protein assay (Sigma, Deisenhofen, Germany). Detection limits of the ELISAs were 0.2 pg/ml for IL-1α, 0.3 pg/ml for IL-1β, and 6.5 pg/ml for IL-1ra. Duplicate measurements were performed according to the manufacturers’ instructions.
DETERMINATION OF IL-1RA GENOTYPE
DNA was extracted from 5 ml EDTA preserved whole blood taken prior to endoscopy after freezing and thawing once using the Q/Amp DNA extraction kit from Qiagen (Hilden, Germany). DNA (0.1–0.5 μg) was amplified by polymerase chain reaction (30 cycles: one minute at 94°C, one minute at 37°C, one minute at 72°C, followed by five minutes extension at 72°C) using the primers described previously.6 Negative controls without DNA template were included with each reaction. All analyses were performed blinded with respect to the diagnosis and patient characteristics. The amplified DNA was separated by electrophoresis on a 2% agarose gel and visualised by ethidium bromide staining. IL-1ra genotype 1 corresponded to 410 bp, genotype 2 to 240 bp, and genotype 3 to 500 bp (see example in fig1).
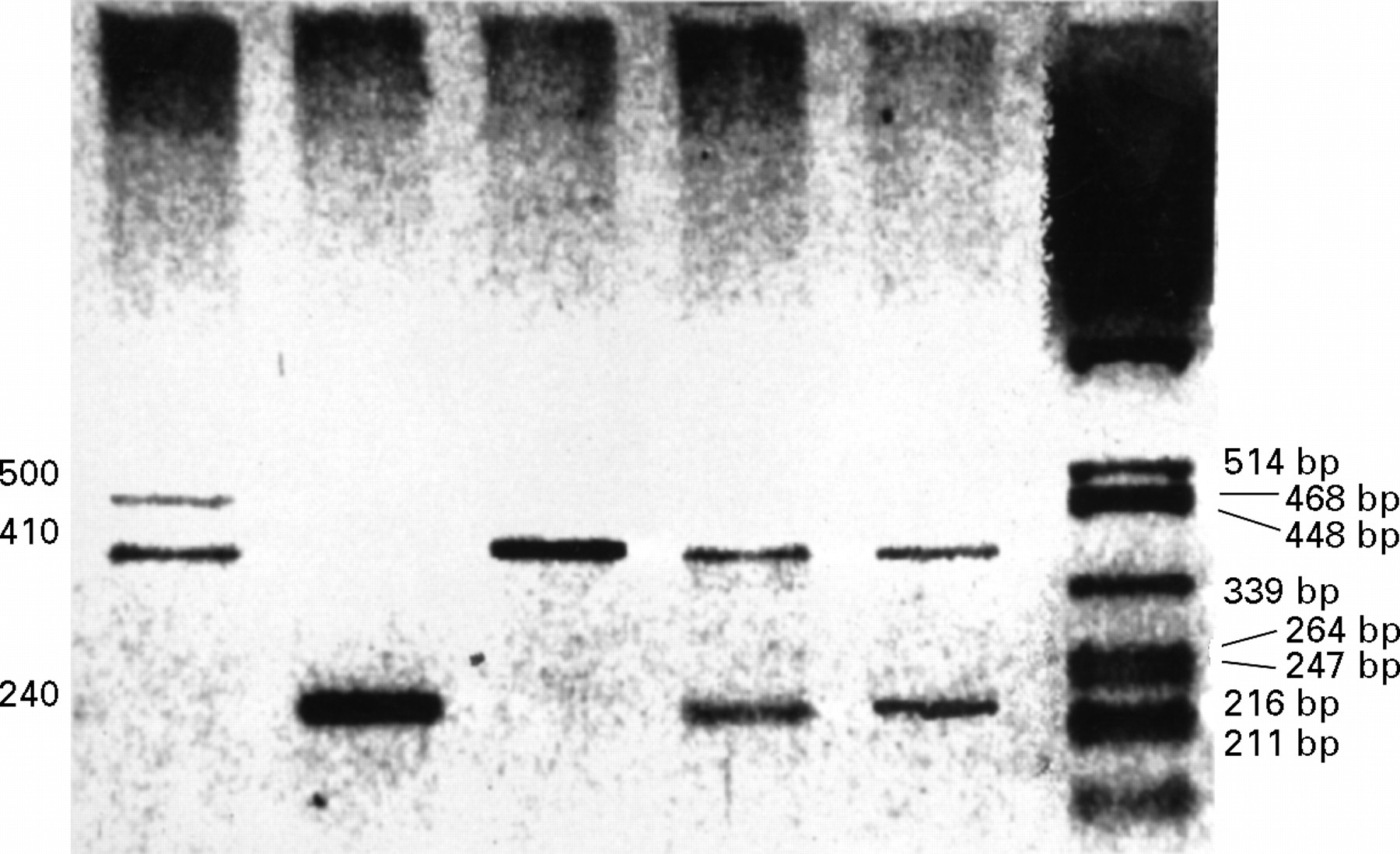
: Different IL-1ra genotypes. The following genotypes are shown (from left to right) 1/3, 2/2, 1/1, 1/2, 1/2. A λ Pst l digest was used as size standard.
STATISTICAL ANALYSIS
Group comparisons of normally distributed data were performed by analysis of variance with Bonferroni correction for multiple testing. Natural logarithms of the cytokine concentrations were used to provide normally distributed data. Correlations were analysed by the Spearman rank test. A value of p<0.05 was considered significant. Group comparisons of non-parametric data were performed by the Mann-Whitney U test or χ2 test as appropriate.
In order to exclude the influence of diagnosis and inflammation, Z normalised values of the data were calculated using the mean and the standard deviation (SD) of the respective disease and degree of inflammation groups (z = (patient’s value−mean)/SD). A Z score of 0 represents the mean of the data; Z scores of –1 and +1 represent data 1 SD below or above the mean.
The study was approved by the ethics committee of the University of Regensburg, Germany, and performed in accordance with the Declaration of Helsinki.
Results
We measured the protein concentrations of IL-1α, IL-1β, and IL-1ra in colonic mucosa and determined the ratios between IL-1ra and IL-1β as a marker for the local balance of the IL-1 system.
IL-1α AND IL-1β CONCENTRATIONS IN COLONIC BIOPSY SPECIMENS
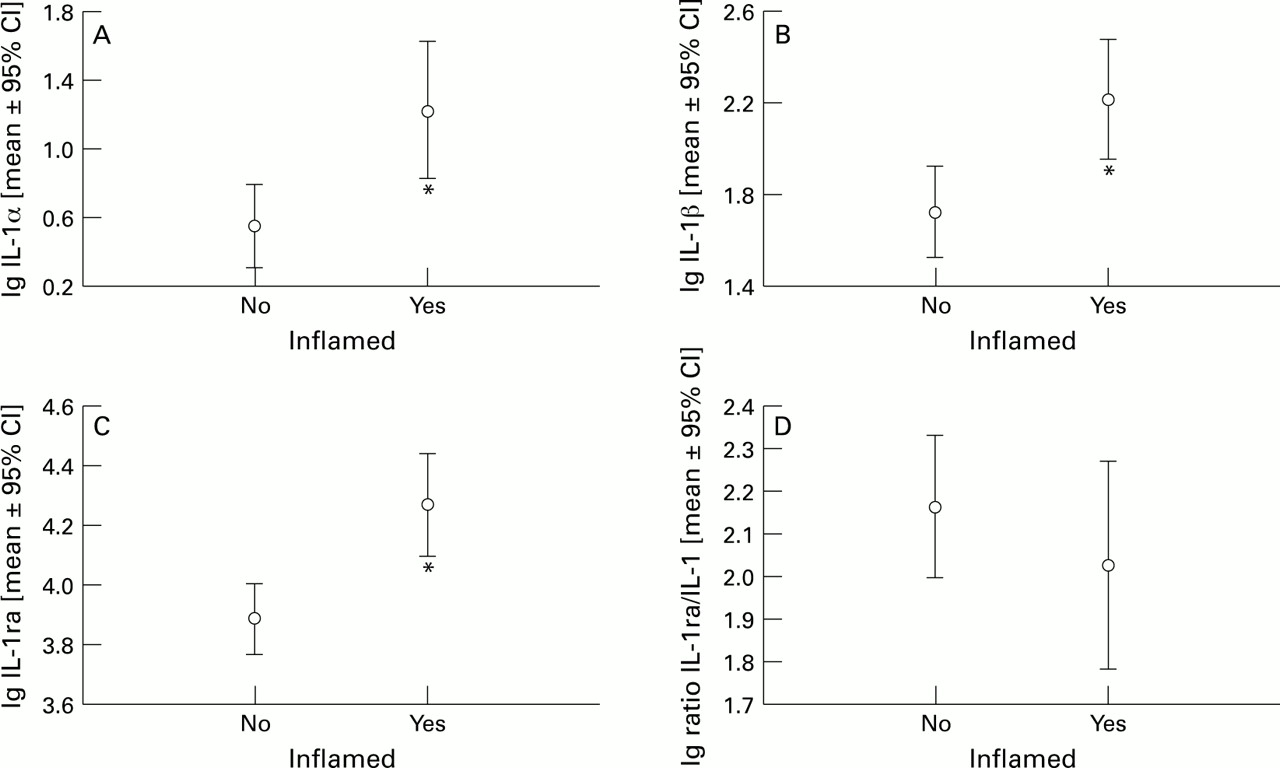
Only low amounts of IL-1α (mean (SEM) 2.8 (0.6) pg/mg protein) and IL-1β (30.6 (5.6) pg/mg protein) could be detected in normal control biopsy specimens (fig 2A, B). IL-1β concentrations were usually about 10-fold higher than IL-1α concentrations. IL-1α and IL-1β concentrations were significantly increased in macroscopically inflamed (IL-1α: 53.5 (22.4) pg/mg protein, p<0.0001; IL-1β 409.9 (118.7) pg/mg protein, p<0.0001) as well as in non-inflamed specimens from patients with CD (IL-1α: 6.1 (1.3) pg/mg protein, p=0.001; IL-1β: 88.7 (17.4) pg/mg protein; p<0.0001; fig 2A, B). In patients with UC, IL-1α (4.3 (1.5) pg/mg protein) and IL-1β (63.7 (15.7) pg/mg protein) concentrations were not significantly increased in macroscopically non-inflamed biopsy specimens (after Bonferroni correction) but were both significantly increased in inflamed colonic mucosa (IL-1α: 18.9 (6.8) pg/mg protein, p<0.001; IL-1β 214.5 (78.2) pg/mg protein, p<0.0001; fig 2A, B). IL-1α (19.2 (7.4) pg/mg protein, p<0.0001) and IL-1β (281.4 (121.0) pg/mg protein, p<0.0001) protein concentrations were also significantly increased in inflammatory controls. There was no significant difference between IL-1α or IL-1β concentrations in inflammatory controls, inflamed mucosa of CD, and inflamed mucosa of UC.

: IL-1α (A), IL-1β (B), IL-1ra (C), and IL-1ra:IL-1α+β ratios (D) in colonic mucosa. Data were logarithmically transformed (to achieve a normal distribution) and were expressed as means (95% confidence intervals). Asterisks indicate statistically significant differences compared with non-inflamed controls.
IL-1α and IL-1β were also significantly increased in inflamed mucosa of inflammatory controls, of patients with CD or UC, and in the non-inflamed mucosa in the subgroup of patients with CD who were not taking medication (p<0.0001). A statistically significant difference for IL-1α or IL-1β concentrations was not found in any group when patients on anti-inflammatory medication were compared with patients without medical treatment.
IL-1RA CONCENTRATIONS IN COLONIC BIOPSY SPECIMENS
IL-1ra concentrations were much higher than IL-1β concentrations in all mucosal biopsy specimens (fig 2C). Compared with normal controls (9970 (1250) pg/mg protein) IL-1ra concentrations were significantly increased only in specimens from inflamed mucosa of patients with CD (24 000 (4840) pg/mg protein, p=0.002) and UC (22 700 (3350) pg/mg protein, p<0.0001; fig 2C). In inflammatory controls IL-1ra concentrations tended to be higher than in non-inflamed controls (16 000 (4450) pg/mg protein) without reaching statistical significance (p=0.2).
IL-1ra was also significantly increased in inflamed mucosa in the subgroup of patients with CD (p=0.002) or UC (p<0.0001) without medication. A statistically significant difference between IL-1ra levels determined in patients treated with glucocorticoids, 5-ASA, or sulphasalazine was not found when compared with patients without medical treatment.
RATIOS BETWEEN THE CONCENTRATIONS OF IL-1RA AND IL-1A+B IN COLONIC BIOPSY SPECIMENS
In order to determine changes in the balance between pro- and anti-inflammatory components of the IL-1 system the ratios between IL-1ra and IL-1α+β were calculated (fig 2D). As the increase in IL-1α and IL-1β during inflammation was more pronounced than the increase in IL-1ra, the ratios between IL-1ra and IL-1α+β were lower in inflamed biopsy specimens than in non-inflamed specimens. Compared with non-inflamed controls (1307 (245)) the ratios were significantly decreased in the inflamed mucosa of patients with CD (182 (45), p<0.0001), UC (425 (136), p=0.0018), and non-IBD patients (221 (76), p<0.0001; fig 2D). Interestingly, the IL-1ra:IL-1α+β ratio was also significantly decreased in non-inflamed CD mucosa (369 (149), p<0.0001).
The ratios of IL-1ra:IL-1α+β were also significantly decreased in the inflamed mucosa of patients with CD and in the inflammatory controls in the subgroup of patients without medication. The ratios were not significantly different in patients with or without medication.
INTRAINDIVIDUAL CONCENTRATIONS OF IL-1α, IL-1β, AND IL-1RA, AND IL-1RA:IL-1α+β RATIOS IN COLONIC MUCOSA OF PATIENTS WITH CD
In 23 patients with CD paired biopsy specimens were taken from inflamed as well as from non-inflamed colonic mucosa. As shown in fig 3IL-1α (68.0 (23.0) versus 36.8 (17.0) pg/mg protein; p=0.001), IL-1β (333.3 (62.3) versus 210.5 (48.9) pg/mg protein; p<0.0001), and IL-1ra (29 000 (4920) versus 19 100 (3810) pg/mg protein; p=0.005) were significantly higher in inflamed mucosa than in non-inflamed mucosa. The ratios of IL-1ra:IL-1α+β tended to be lower in inflamed mucosa without reaching statistical significance (fig3D). In UC and in the inflammatory controls IL-1α, IL-1β, and IL-1ra were also higher in the inflamed than in the non-inflamed mucosa. Due to smaller numbers these differences were not statistically significant (data not shown).
: Intraindividual concentrations of IL-1α (A), IL-1β (B), IL-1ra (C), and IL-1ra:IL-1α+β ratios (D) in inflamed and non-inflamed colonic mucosa of patients with CD. Data were logarithmically transformed (to achieve a normal distribution) and were expressed as means (95% confidence intervals). Asterisks indicate statistically significant differences between inflamed and non-inflamed regions.
IL-1RA GENOTYPE AND IL-1RA PROTEIN CONCENTRATIONS IN COLONIC MUCOSA
Table 1 shows the distribution of the different IL-1ra genotypes. One or two alleles of the IL-1ra genotype 2 (240 base pairs) were found in 57% of control patients, in 55% of patients with CD, and in 67% of patients with UC. When IL-1ra concentrations in colonic mucosa of patients with and without genotype 2 were compared, IL-1ra concentrations were found to be decreased in most of the subgroups defined by diagnosis and macroscopic inflammation (fig 4) to some extent. However, only in the inflamed mucosa of CD patients was the difference highly significant (p=0.006, table 2). To combine the data we excluded the effect of diagnosis and inflammation by calculating Z scores for the respective disease and degree of inflammation. Comparing the Z scores of IL-1ra between patients with and without genotype 2 we found that IL-1ra concentrations were significantly lower in the colonic mucosa of patients with IL-1ra genotype 2 (p=0.003). The Z scores of IL-1α (p=0.8) and IL-1β (p=0.2) were used as controls and were not significantly different between patients with or without IL-1ra genotype 2. The Z score of the IL-1ra/IL-1α+β ratio tended to be lower in patients with IL-1ra genotype 2; however, the difference was not statistically significant (p=0.29).
Distribution of IL-1ra genotypes in patients with or without inflammatory bowel disease

: IL-1ra in colonic mucosa and genetic polymorphism of IL-1ra. Data were logarithmically transformed (to obtain a normal distribution) and are expressed as mean (SEM).
IL-1ra colonic mucosa in patients with or without IL-1ra genotype 2
When patients were grouped according the number of IL-1ra genotype 2 alleles, a weak but significant correlation was found between the number of type 2 alleles and the decrease in IL-1ra concentrations (r=–0.25; p=0.001; fig 5B) and in the IL-1ra/IL-1α+β ratio (r=0.15, p=0.04) in colonic mucosa (fig 5C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
: Genetic polymorphism of IL-1ra and mucosal concentrations of IL-1α, IL-1β, and IL-1ra. IL-1(α+β) (A), and IL-1ra (B) were determined and ratios of IL-1ra:IL-1α+β were calculated (C). In order to combine the data of different groups the influence of diagnosis and inflammation was excluded by Z normalisation. The Z normalised values of the data are given as mean (95% confidence interval) and grouped by the number of IL-1ra genotype 2 alleles. The asterisk indicates a statistically significant difference compared with the patients with no IL-1ra allele.
When macroscopically inflamed or non-inflamed biopsy specimens were analysed separately, IL-1ra protein and IL-1ra genotype 2 correlated much better in specimens from inflamed mucosa (r=–0.39, p=0.01) than in specimens from non-inflamed mucosa (r=–0.15, p=0.17).
Discussion
The colonic concentrations of IL-1α, IL-1β, IL-1ra, and IL-1ra genotypes were determined in order to address the questions: Is there a specific imbalance between pro- and anti-inflammatory mediators in IBD; and are IL-1ra genotypes associated with colonic IL-1ra production?
To measure the components of the IL-1 system present in the colonic mucosa we determined the mediators in homogenates of colonic biopsy specimens as previously described.31 The advantage of this method is the minimisation of artificial activation or inhibition of cytokine production which occurs when cells are isolated from the mucosa and then cultured. The disadvantage is that this method does not allow differentiation between intracellular and secreted cytokines or identification of the cells synthesising the respective cytokines. Nishiyama et al found intestinal macrophages to be the major source of IL-1ra in the mucosa by immunohistochemical colocalisation studies.20
The data presented in this paper show that IL-1α, IL-1β, and IL-1ra are increased in the colonic mucosa during inflammation. As the increase in IL-1α and IL-1β was greater than that in IL-1ra it led to a shift of the balance between pro- and anti-inflammatory components of the IL-1 system towards the pro-inflammatory side. Although the amount of IL-1ra was greater than that of IL-1β in all biopsy specimens, our data indicate an imbalance in the IL-1ra:IL-1α+β system in the inflamed mucosa, since a 100- to 1000-fold excess of IL-1ra is required to block the binding of 50% of IL-1 to its receptors and to inhibit the activation of IL-1 responsive cells.32
In our patients the imbalance in the IL-1 system was not specific for IBD but could also be found in other types of colonic inflammation. The measurement of intraindividual differences showed that the degree of inflammation is the most important factor for the production of IL-1α, IL-1β, and IL-1ra. The discrepancy between our data and those of Nishiyama et al 20 and Casini-Raggi et al 30 is probably due to the fact that in their studies the inflammatory activity of their controls was lower than that of the IBD patients. This is reflected by relatively low IL-1α+β concentrations in their inflammatory controls.20 ,30 Another explanation may be the different genetic background of the patients in the various studies.
There is one major difference between CD and UC: IL-1α and IL-1β levels are significantly increased and IL-1ra:IL-1α+β ratios are significantly decreased in the non-inflamed mucosa of patients with CD but not in the non-inflamed mucosa of patients with UC. Thus, in CD but not in UC there is an imbalance in the IL-1 system in the non-inflamed mucosa. This indicates that the intestinal immune system in CD is always activated to some extent and the pro-inflammatory component is predominant, while activation of the immune system is restricted to grossly inflamed areas in UC. This upregulation of the intestinal immune system might be a general feature of CD and may explain our previous findings of continuously elevated IL-6 concentrations in patients with CD.33
The gene for IL-1ra is located on the long arm of chromosome 2 (2q14-q21)34 on a 430 kb stretch of DNA that also contains the genes for IL-1α and IL-1β.35 Intron 2 of the IL-1ra gene contains a variable number of identical tandem repeats of an 86 base pair length of DNA. Genotype 2 of the polymorphism in the IL-1ra gene was found to be significantly overrepresented and associated with severe disease in patients with UC,6Graves’ disease,36 alopecia areata,37 lichen sclerosis,38 lupus erythematosus,39 and multiple sclerosis.40 Our data confirm a moderate overrepresentation of IL-1ra genotype 2 in patients with UC, which was not statistically significant due to the relatively small number of patients. The allelic frequency of of IL-1ra genotype 2 was higher in this study (controls 36%, CD 33%, and UC 44%) than found in the studies of Mansfield et al (controls 24%, CD 22%, and UC 35%),6 Bioque et al (controls 24%, CD 22%, and UC 35%),41 and Louis et al (controls 21%, CD 24%, and UC 25%).42 This is probably due to the genetic background of the patients studied and the relatively small number of patients (sampling effect), since we used the same method as Mansfield et al.6 This conclusion is supported by the fact that we found similiar IL-1ra genotype 2 frequencies to the other authors in a larger group of patients (controls 20%, CD 27%, and UC 29%).43 Furthermore, we found IL-1ra genotype 2 to be associated with an impaired increase in IL-1ra in the colonic mucosa. This may prevent adequate control of mucosal inflammation and therefore be a susceptibility factor for chronic mucosal inflammation. Since we did not measure IL-1ra production by peripheral blood cells of our patients, we do not know whether this is only a local or a systemic effect.
It is not known whether IL-1ra genotype 2 is directly responsible for the impaired production of IL-1ra in the colonic mucosa or whether there is a linkage disequilibrium between these IL-1ra alleles and other polymorphisms nearby.
In conclusion, we found that in the inflamed colonic mucosa there is an imbalance between IL-1 and IL-1ra, which is not specific for IBD. In patients with CD, this imbalance is also found in the non-inflamed mucosa, presumably reflecting continuous activation of the intestinal immune system. Furthermore, we found that IL-1ra genotype 2 is associated with a slightly but significantly impaired IL-1ra production in colonic mucosa, which may increase susceptibility to chronic inflammation.
Acknowledgments
This study was supported by the Wilhelm Sander Stiftung. We thank the endoscopists and nurses of the endoscopy department for providing colonic specimens and the pathologists of the University Hospital of Regensburg for the histopathological grading of the biopsy specimens.