Article Text

Abstract
Background—Infection of pancreatic necrosis has a major impact on clinical course, management, and outcome in acute pancreatitis. Currently, guided fine needle aspiration is the only means for an early and accurate diagnosis of infected necrosis. Procalcitonin (PCT), a 116 amino acid propeptide of calcitonin, and interleukin 8 (IL-8), a strong neutrophil activating cytokine, are markers of severe inflammation and sepsis.
Aims—To analyse the clinical value of PCT and IL-8 as biochemical parameters for predicting infected necrosis in acute pancreatitis.
Patients and methods—Fifty patients with acute pancreatitis entered this prospective study and were stratified into three groups according to morphological and bacteriological findings: 18 patients with oedematous pancreatitis (group I), 14 patients with sterile necrosis (group II), and 18 patients who developed infected necrosis a median of 13.5 days after the onset of symptoms (group III). After admission serum samples were drawn daily for two weeks. Concentrations of PCT and IL-8 were measured by chemoluminescent immunoassays (upper reference range 0.5 ng/ml for PCT and 70 pg/ml for IL-8). The routine parameter C-reactive protein was determined by laser nephelometry (upper reference range 10 mg/l).
Results—Median concentrations of PCT and IL-8 were significantly higher in patients with infected necrosis than in those with sterile necrosis during the observation period, whereas there was no difference in C-reactive protein. In oedematous pancreatitis overall median concentrations of all three parameters were low. By receiver operating characteristics best cut off levels for predicting infected necrosis or persisting pancreatic sepsis were 1.8 ng/ml for PCT and 112 pg/ml for IL-8. If these cut off levels were reached on at least two days, sensitivity, specificity, and accuracy for the prediction of infected necrosis were 94%, 91%, and 92% for PCT and 72%, 75%, and 74% for IL-8, respectively. After surgical treatment of infected necrosis median PCT and IL-8 values continued to be significantly higher in patients with persisting pancreatic sepsis (n=11) compared with those having an uneventful postoperative course (n=7). For the preoperative differentiation between infected necrosis and sterile necrosis guided fine needle aspiration was performed in 24 patients with necrotising pancreatitis and reached a diagnostic accuracy of 84% compared with 87% for PCT, and 68% for IL-8. There was no correlation between the aetiology of acute pancreatitis or the extent of necrosis and PCT or IL-8.
Conclusion—PCT and IL-8 are found in high concentrations in infected necrosis and associated systemic complications in patients with acute pancreatitis. The course of PCT shows the closest correlation with the presence of infected necrosis. Monitoring of serum PCT is a potential new marker for the non-invasive and accurate prediction of infected necrosis as well as for the selection of patients with persisting septic complications after surgical debridement.
- procalcitonin
- interleukin 8
- infected necrosis
- acute pancreatitis
Statistics from Altmetric.com
Infection of pancreatic necrosis is the leading complication in the course of acute pancreatitis. The overall infection rates in acute pancreatitis do not exceed 10%,1 ,2 however the presence and extent of necrosis significantly increases the incidence of infection up to 80%3-5 and is associated with high mortality and morbidity.2-6 Nowadays, most authorities agree on the necessity for surgical intervention in patients with proven infection of pancreatic necrosis; this has markedly decreased the mortality in this subset of patients.2 ,6
There is great interest in the development of a valid optimum diagnostic tool for the diagnosis of infected necrosis. Several multifactorial scoring systems7-9 as well as biochemical parameters10-12 have been shown to be good predictors of necrosis or severity in acute pancreatitis. However, various studies have shown that they are of little clinical value in indicating infection in patients with systemic inflammatory response syndrome.13-17 Currently, guided fine needle aspiration is the only invasive means for an early and accurate diagnosis of infected necrosis17 ,18 and the standard new techniques have to compete with it.
Recently, procalcitonin (PCT), a 116 amino acid propeptide of calcitonin with a long half life in the systemic circulation, was found to appear in high concentrations in patients with severe bacterial or fungal infections and sepsis (Gendrel D et al unpublished observa- tion).13-15 19-20 PCT is usually not detectable in normal controls. In non-septic inflammatory diseases, various metastatic cancers, and minor infections, normal or only slightly elevated levels are found.20 Interleukin 8 (IL-8) is an important neutrophil activating cytokine which is released in response to inflammatory stimuli.21 In a few series IL-8 was reported to be an early predictor of disease severity and the development of complications in patients with acute pancreatitis22 ,23 and adult respiratory distress syndrome24; it is not, however, measurable in healthy subjects.
The observation that both PCT and IL-8 play a major role in severe inflammation and sepsis raises the question of whether both parameters might be useful in differentiating infected from sterile necrosis in acute pancreatitis. No study has however assessed both parameters in this respect. Compared with guided fine needle aspiration as the current “gold-standard”, an accurate and readily available biochemical parameter for identifying patients who are at risk of developing infected necrosis would contribute to an easier, less invasive, and less cost intensive diagnosis. The aim of this prospective study was therefore to investigate the potential clinical value of PCT and IL-8 as biochemical markers for predicting infected necrosis in a morphologically and bacteriologically well defined patient series with acute pancreatitis.
Materials and Methods
PATIENTS
A total of 50 patients with acute pancreatitis entered this prospective study at the Department of General Surgery, University Hospital at Ulm between December 1993 and July 1996. Inclusion criteria were typical upper abdominal pain and at least threefold elevated serum amylase and/or lipase levels. The time interval between onset of symptoms and inclusion in the study was restricted to less than 120 hours and was a median of 26 (range 0–118) hours. Based on morphological criteria revealed by contrast enhanced computed tomography or ultrasound, patients were classified into necrotising or interstitial oedematous pancreatitis. In all patients with computed tomography proven necrotising pancreatitis, the extent of intrapancreatic necrosis was graded as <30%, 30–50%, and >50% of non-perfused parenchyma. According to bacteriological findings obtained by ultrasound guided fine needle aspiration and/or during surgery, necrotising pancreatitis was further classified into infected or sterile necrosis. Table 2 summarises the definitions for organ/systemic complications and multiple organ failure.
Clinical severity and incidence of organ complications in patients with interstitial oedematous pancreatitis (group I), sterile necrotising pancreatitis (group II), and infected necrotising pancreatitis (group III)
Initial treatment was conservative in all patients and included maximum intensive care support. Antibiotics were either administered in a prophylactic fashion as soon as the presence of necrosis was proven by contrast enhanced computed tomography or as perioperative/postoperative prophylaxis which included only substances which are known to penetrate into the pancreatic parenchyma (for example, ofloxacin/metronidazole or imipenem). In patients with fine needle aspiration or intraoperatively documented infected necrosis, the antibiotic regimen was adjusted to the microbiological spectrum found. Surgery was indicated if fine needle aspiration was positive for bacteria or fungi and the systemic inflammatory response syndrome was present, or if organ complications or abdominal symptoms persisted despite maximum intensive care treatment in the absence of positive fine needle aspiration results.
METHODS
Blood samples were drawn from central venous lines at 24 hour intervals over 14 days after informed consent was obtained from every patient. Thereafter, samples were immediately spun at 3500g at 4°C for 10 minutes, placed into 500 μl cups, and stored at –70°C until assayed. Concentrations of PCT (upper reference range 0.5 ng/ml) and IL-8 (upper reference range 70 pg/ml) were measured using a chemoluminescent immunoassay technique as described below. C-reactive protein (upper reference range 10 mg/l) was determined by a laser nephelometric technique (Beckman Instruments Inc., Galway, Ireland) on a daily clinical routine basis.
ASSAYS
PCT was measured with the commercially available LUMI® test PCT kit (BRAHMS Diagnostica GmbH, Berlin, Germany) on a MagicLite (Ciba Corning) Luminometer which took about 120 minutes to perform. The cost of one PCT determination was DM 10.00. For the measurement of IL-8 we used the commercially available Immulite IL-8 kit on an IMMULITE® automated Luminometer (DPC Biermann, Los Angeles, California, USA) by which one sample could be analysed within 30 minutes at a cost of DM 16.00.
FINE NEEDLE ASPIRATION
Ultrasound guided fine needle aspiration was performed in all patients with necrotising pancreatitis proven by contrast enhanced computed tomography, if infection of necrosis was suspected by persisting systemic inflammatory response syndrome over at least two to three days after other possible sources of infection (for example, infected central line, urinary tract infection, pneumonia) had been excluded. The technical approach consisted of an abdominal ultrasound (Sonoline SI 450, Siemens, Germany and Sonolayer L 77B, Toshiba, Japan) to locate the areas of necrosis. After careful skin desinfection a 16 gauge sleeve needle was advanced under ultrasound guidance until the respective area was reached and a minimum of 1 ml aspirate could be obtained. Thereafter, the aspirate was immediately processed for Gram staining and culture and analysed by an experienced microbiologist. An aspirate was considered infected if either Gram stain or culture was positive for microorganisms.
STATISTICS
All variables are represented as medians. For comparison of independent samples we used the Mann-Whitney U test and for comparison of proportions, Fisher’s exact test. Values of p<0.05 at α<0.05 were considered significant. Receiver operating characteristic curves and the respective areas under the curve25 were calculated for the maximum values of each parameter reached on at least two days during the whole observation period. The best cut off was chosen as the value which optimised sensitivity (patients with infected necrosis), specificity (patients with sterile necrosis/oedematous pancreatitis), and likelihood ratio (LR = (probability of true positives + probability of true negatives)/(probability of false positives + probability of false negatives)). Statistical calculations were done with the MedCalc Software package.26
Results
Group I—Interstitial oedematous pancreatitis was diagnosed in 18/50 (36%) patients who all had a clinically uneventful course and survived. Two patients with biliary pancreatitis and accompanying cholecystitis underwent emergency cholecystectomy; in nine patients cholecystectomy was performed after acute pancreatitis had subsided.
Group II—Sterile necrosis was present in 14/50 (28%) patients with necrotising pancreatitis who had a clinically severe course. Three of these patients underwent surgical necrosectomy due to persisting organ complications; in three patients with biliary pancreatitis cholecystectomy was perfomed, and the remaining eight patients were managed by conservative means. Prophylactic antibiotics were administered in 11 patients (median start on day 4 of disease), and two patients received antibiotic treatment following a false positive fine needle aspiration result (median start on day 7 of disease). No deaths occurred in this group.
Group III—A total of 18/50 (36%) patients with necrotising pancreatitis developed infected necrosis, of whom 11 died from septic multiple organ failure. All patients in this group had severe pancreatitis and underwent surgical necrosectomy with postoperative closed lavage. Ten patients were found to have infected necrosis during the first operative intervention (primary infection) of which six received prophylactic (median start on day 3 of disease) and four perioperative/postoperative antibiotics (median start on day 13 of disease). In eight patients infection developed after surgery for severe sterile necrosis (secondary infection), of which seven received prophylactic (median start on day 3 of disease) and one perioperative (start on day 6 of disease) antibiotics. The overall median time between onset of symptoms and intraoperative diagnosis of infected necrosis was 13.5 (range 6–41) days.
Table 1 shows the patients’ age and sex distribution as well as the aetiology of acute pancreatitis in each of the three groups. Biliary pancreatitis was most frequently found in patients with oedematous pancreatitis. As shown in table 2, the incidence and severity of early organ complications as well as the disease severity according to Ranson and APACHE II scores was highest in the patient group with infected necrosis. Table 3 shows the intrapancreatic extent of necrosis, which was higher in the infected than in the non-infected group. Extended necrosis of more than 30% pancreatic parenchyma was present in 3/14 (21%) patients with sterile and in 9/17 (53%) patients with infected necrosis (p<0.03).
Clinical data and aetiology in patients with interstitial oedematous pancreatitis (group I), sterile necrotising pancreatitis (group II), and infected necrotising pancreatitis (group III)
Results of contrast enhanced computed tomography (CT) in patients with sterile and infected pancreatic necrosis
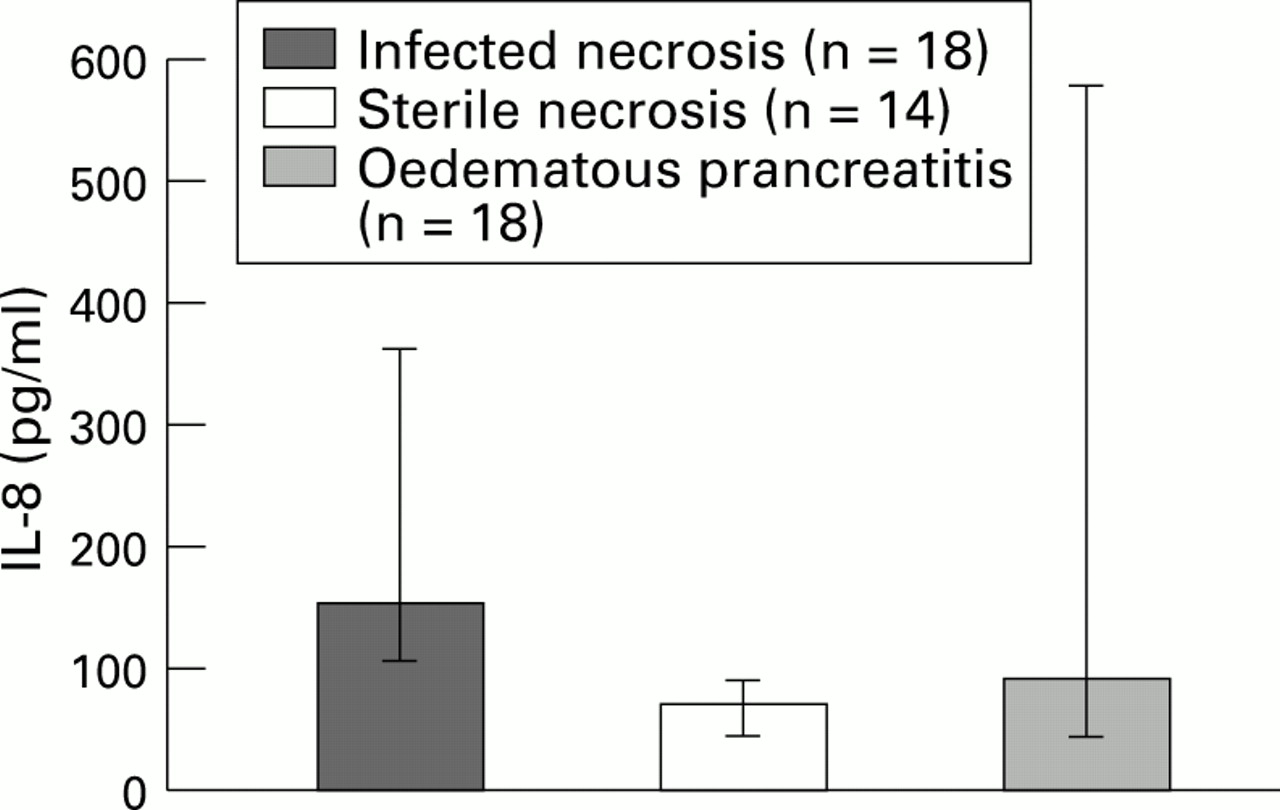
In patients with infected necrosis PCT and IL-8 concentrations were markedly elevated and reached significantly higher median peak levels compared with the groups with sterile necrosis and oedematous pancreatitis, in which generally low or only slightly elevated PCT levels were found (figs 1 and 2). The degree of PCT elevation reflected the systemic severity of infection in terms of associated organ failure (median PCT peaks in infected necrosis with multiple organ failure 28.8 ng/ml, range 3.1–186.2 versus infected necrosis without multiple organ failure 3.8 ng/ml, range 1.7–5.8, p<0.001). The presence of early toxic organ failure in patients with sterile necrosis did not cause a relevant increase in PCT concentrations (median PCT peaks in sterile necrosis with multiple organ failure 1.0, range 0.6–1.7). Whereas PCT levels were found to be elevated early in the course of the disease, IL-8 levels usually rose in parallel to the development of accompanying septic multiple organ failure during the second week after onset of symptoms. Early toxic multiple organ failure in patients with sterile necrosis was not associated with persistently elevated IL-8 concentrations (median peak IL-8 in septic multiple organ failure 160 pg/ml, range 39–10 000 versus toxic multiple organ failure 93 pg/ml, range 65–133, p<0.05).

: Peak concentrations of PCT reached on at least two days during the observation period in patients with infected necrosis, sterile necrosis, and oedematous pancreatitis (p<0.0001, infected versus sterile necrosis and infected necrosis versus oedematous pancreatitis).

: Peak concentrations of IL-8 reached on at least two days during the observation period in patients with infected necrosis, sterile necrosis, and oedematous pancreatitis (p<0.0001, infected versus sterile necrosis; p<0.05, infected necrosis versus oedematous pancreatitis).
Figure 3 shows the typical course of PCT and IL-8 in a patient with infected necrosis and severe septic multiple organ failure. The patient was a 66 year old woman with biliary pancreatitis who was admitted on the second day after onset of symptoms. Ranson and admission APACHE II scores were 8 and 28, respectively. The clinical course was complicated by severe non-controllable septic multiple organ failure deriving from infected necrosis. Despite four surgical interventions the patient deteriorated and died 21 days after admission to hospital.

: Typical course of PCT and IL-8 in a patient with infected necrosis and severe septic multiple organ failure.
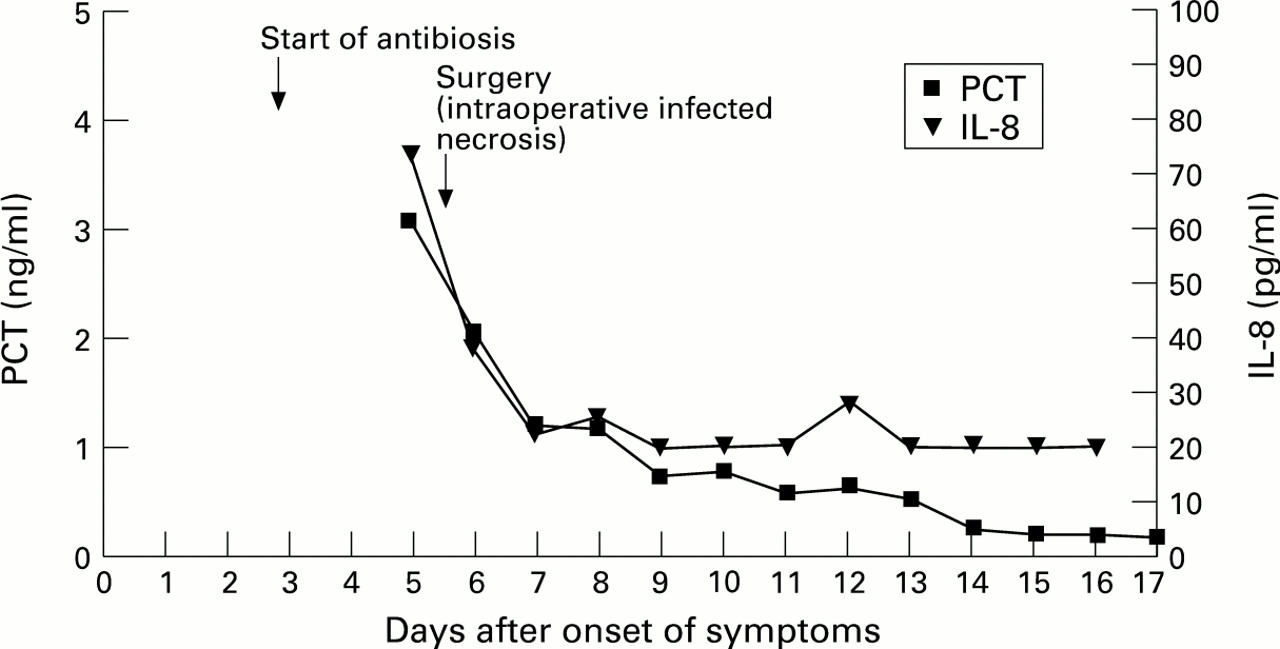
Figure 4 shows the typical course for a patient with infected necrosis and an uncomplicated course. The patient was a 40 year old man with alcoholic pancreatitis admitted on the third day after disease onset. Ranson and admission APACHE II scores were 4 and 12, respectively. The postoperative course was uneventful and no septic multiple organ failure was observed. This patient was discharged in good clinical condition after 34 days in hospital.

: Typical course of PCT and IL-8 in a patient with infected necrosis and an uncomplicated course.
Both PCT and IL-8 did not show the typical pattern of C-reactive protein, which rose to maximum levels within the first four days of acute pancreatitis and gradually decreased thereafter in all three groups.
Patients with infected necrosis and a complicated course resulting in death (n=11) had higher median preoperative peak concentrations of PCT (24.9 ng/ml, range 1.4–158.9 versus 3.1 ng/ml, range 0.7–26.3, p<0.02) and IL-8 (196 pg/ml, range 105–780 versus 74 pg/ml, range 34–161, p<0.002) compared with patients with infected necrosis and an uneventful course who survived (n=7). The same observation was made during the early postoperative period (postoperative days 1 to 3) for both PCT and IL-8. In all survivors PCT and IL-8 concentrations returned to normal levels within the first three postoperative days and overall median concentrations (PCT 1.2 ng/ml, range 0.7–4.5, p<0.04; IL-8 34 pg/ml, range 20–73, p<0.01) were significantly lower compared with the maximum preoperative values. In contrast, non-survivors had persisting median concentrations of both parameters (PCT 17.4 ng/ml, range 2.4–186, NS; IL-8 158 pg/ml, range 47–1693, NS) during the same postoperative observation period. C-reactive protein did not show any difference between the preoperative and postoperative course and between survivors and non-survivors. Surgical trauma such as necrosectomy or cholecystectomy did not result in a postoperative increase of PCT or IL-8 levels, whereas C-reactive protein uniformly increased within the first three postoperative days.
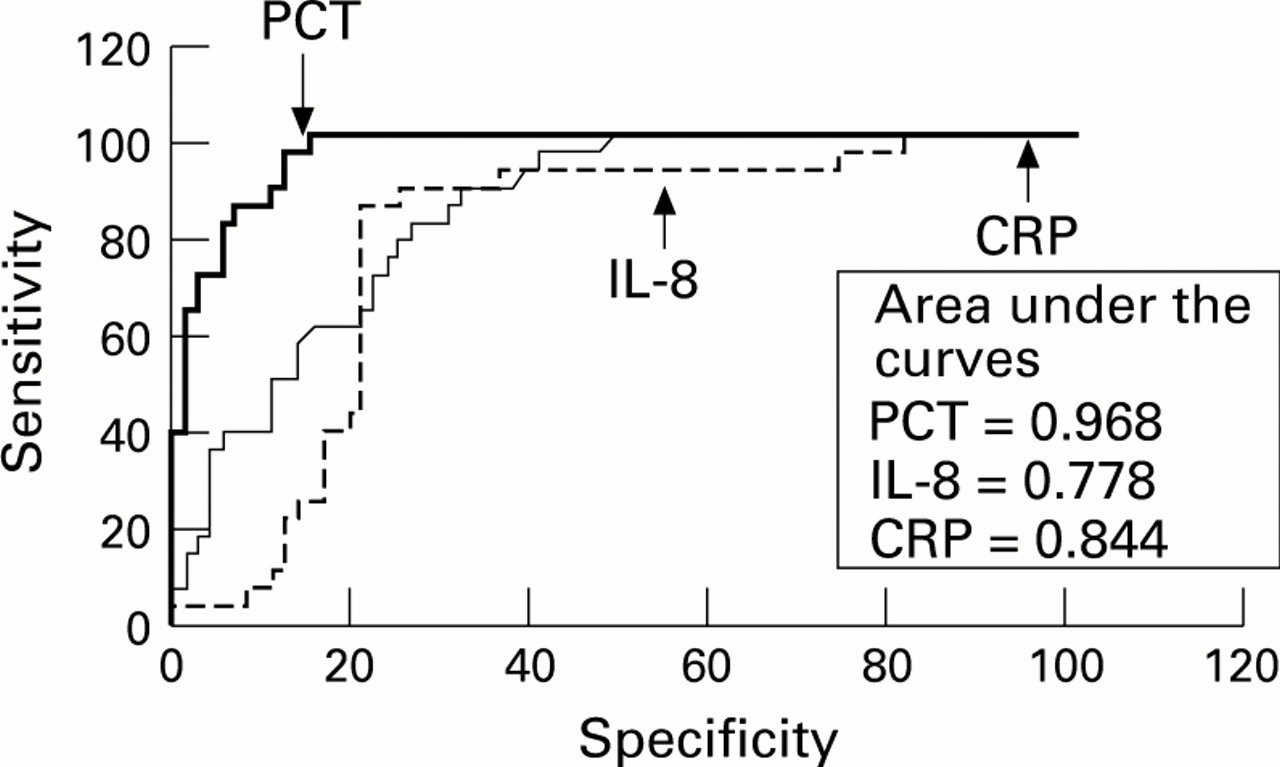
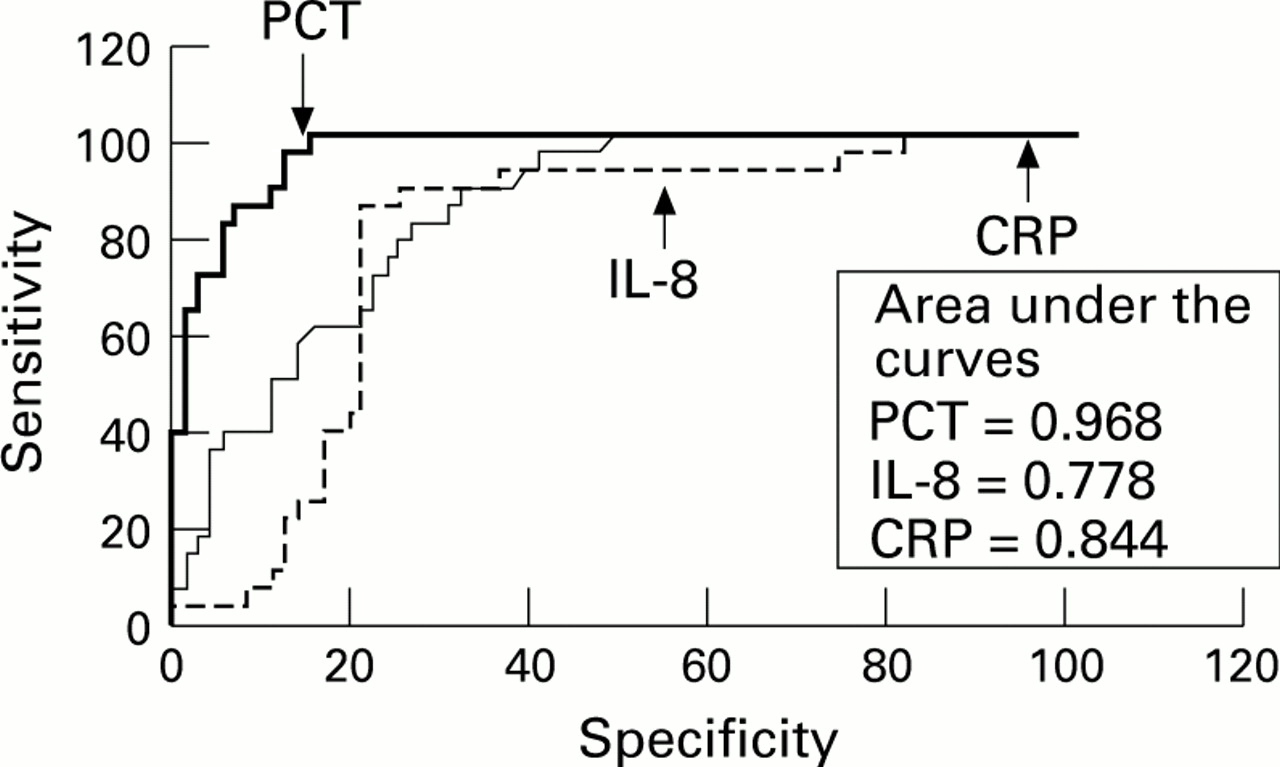
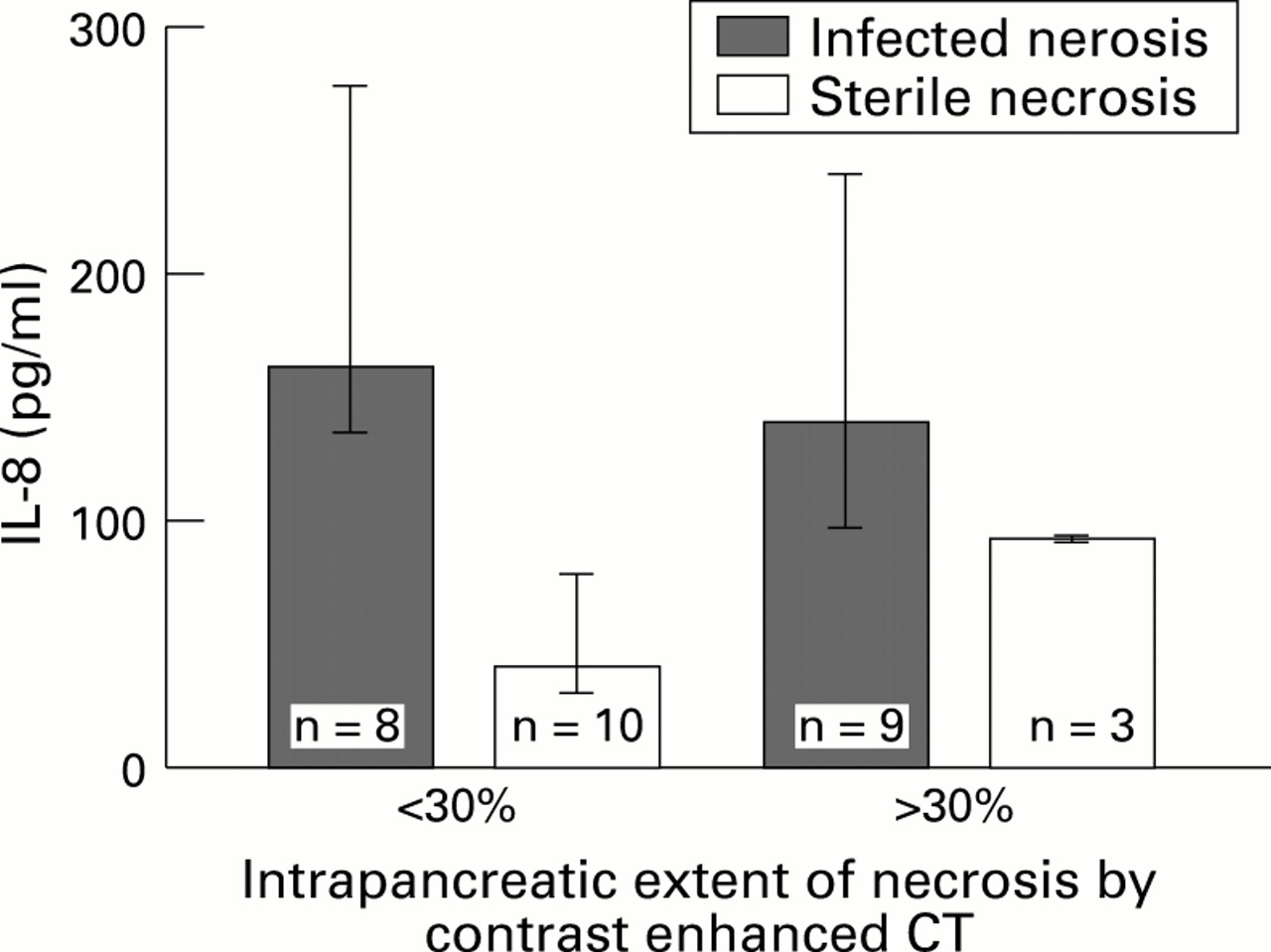
The receiver operating characteristic (ROC) curves for PCT, IL-8, and C-reactive protein in the prediction of infected necrosis (fig 5), septic multiple organ failure (fig 6), and necrosis (fig 7) have been calculated on the basis of at least two maximum values in each patient during the overall observation period. By comparison of the areas under the ROC curve, PCT was found to have the closest correlation with the presence and severity of bacterial/fungal infection of necrosis compared with IL-8 and C-reactive protein (figs 5 and 6). Table 4 shows the cut off levels with the respective sensitivity and specificity for the prediction of infected necrosis, septic multiple organ failure, death, and all three parameters. Although IL-8 showed the closest correlation to septic multiple organ failure, it was inferior to PCT and C-reactive protein in predicting infected necrosis and septic multiple organ failure (fig 6). In contrast to C-reactive protein, PCT and IL-8 were less predictive for the presence of necrosis (fig 7). There was no correlation beween the extent of intrapancreatic necrosis as shown by contrast enhanced computed tomography and PCT (fig 8) or IL-8 (fig 9), nor was there any correlation between both parameters and the aetiology of acute pancreatitis.

: ROC for PCT, IL-8, and C-reactive protein (CRP) in predicting infected necrosis. Analysis was based on at least two maximum levels of each parameter (p<0.05, PCT versus CRP; p<0.0001, PCT versus IL-8; p<0.012, CRP versus IL-8).
: ROC for PCT, IL-8, and C-reactive protein (CRP) in predicting septic multiple organ failure. Analysis was based on at least two maximum levels of each parameter (p<0.001, PCT versus IL-8; p<0.02, PCT versus CRP; NS, IL-8 versus CRP).

: ROC for PCT, IL-8, and C-reactive protein (CRP) in predicting necrotising pancreatitis. Analysis was based on the two highest levels of each parameter (p<0.008, CRP versus PCT; p<0.0001, CRP versus IL-8; p<0.0001, PCT versus IL-8).
Optimum cut off levels with sensitivity and specificity of PCT, IL-8, and C-reactive protein (CRP) in predicting infected necrosis (n=18), septic multiple organ failure (MOF) (n=14), and death (n=11) in acute pancreatitis

: Peak concentrations of PCT did not correlate with the intrapancreatic extent of necrosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
: Peak concentrations of IL-8 did not correlate with the intrapancreatic extent of necrosis.
Preoperative ultrasound guided fine needle aspiration was perfomed in all 10 patients with primary infections and correctly predicted the presence of bacteria in nine patients after a median of six (range 5–19) days following the onset of symptoms. This represents a sensitivity of 90%. Fourteen patients with sterile necrosis underwent fine needle aspiration, which was false positive in one patient. In two other patients Gram negative organisms were isolated; however, as both recovered completely without surgery, true pancreatic infection could be excluded. The positive fine needle aspirations might have represented contamination which was successfully treated by antibiotics, but this remains speculative and both have to be regarded as false positive results; the specificity of this procedure is therefore 79%. Table 5 shows sensitivity, specificity, and diagnostic accuracy for PCT, IL-8, and C-reactive protein in predicting infected necrosis in the same patients and during the same time period as fine needle aspiration was performed.
Sensitivity, specificity, and accuracy of preoperative ultrasound guided fine needle aspiration (FNA), and PCT, IL-8, and C-reactive protein (CRP) concentrations in predicting infection in necrotising pancreatitis, (24 patients, 14 with infected necrosis, four with sterile necrosis)
Discussion
Infected necrosis is the overall determinant in the course of acute pancreatitis. Even if the extent of necrosis is substantial,3 ,4 mortality rates remain low as long as the necrotic process remains sterile.4 ,27 As infection of pancreatic necrosis is an absolute indication for surgical intervention, much effort has been put into the search for an optimum diagnostic tool for its early diagnosis. Several scoring systems such as the multiple organ failure,7 sepsis severity,8 and APACHE II scores,9 as well as various blood parameters10-12 are known to be good predictors of necrosis or overall severity in acute pancreatitis. Studies in patients with various diseases associated with systemic inflammatory response syndrome have however shown that none of them are reliable indicators of infection and sepsis.13 ,15Surprisingly, in acute pancreatitis only a few of the mentioned parameters have been investigated with respect to their clinical usefulness in differentiating patients with pancreatic infection from non-infected patients.16 ,17 ,28 As a result, guided fine needle aspiration is still the “gold-standard” for the early and accurate diagnosis of infected necrosis.17 ,18Unfortunately, the demand for high standard technical equipment and experienced personnel as well as the potential risk of complications such as bleeding or iatrogenic infection prevent it from being an easily available and cost effective procedure. In our experience with ultrasound guided fine needle aspiration in necrotising pancreatitis over the past eight years we obtained a sensitivity of 88% and a specificity of 90% (Rau et al, unpublished observations). Although we did not observe major complications such as bleeding, aggravation of pancreatitis, or death, there were false positive results in which iatrogenic infection could not be definitely excluded and thus could represent a risk factor for the patient. A non-invasive and readily available biochemical parameter for identifying patients with infected necrosis would therefore definitely contribute to an easier and safer diagnosis.
Recently, PCT, a 116 amino acid propeptide of calcitonin, was reported to be a new potential marker for severe bacterial or fungal infections and sepsis (Gendrel D et al, unpublished observation).13-15 19-20 The diagnostic and prognostic properties of PCT in severe inflammatory diseases were first reported in a series of patients with burns in 1992.29 Subsequent studies showed that only bacterial or fungal infections or sepsis were associated with a significant increase in PCT and that a strong correlation exists between the degree of the increase and the clinical severity of infection.14-16 19-20
Little is known about the cellular origin and mechanism of PCT production in bacterial or fungal infection and sepsis. Histochemical studies indicate that, in these conditions, the neuroendocrine cells in the lung may be the primary source of PCT production.30 In addition, the temporal relationship between the onset or control of infection and PCT concentration as well as its pathophysiological role and exact position within the inflammatory mediator cascade are poorly understood. However, recent studies in humans show that bacterial endotoxin induces the release of PCT systemically within three to four hours which is preceded by a peak in tumour necrosis factor α (TNF-α) and followed by a gradual increase in interleukin 6 and C-reactive protein.31 Compared with the relatively short half lives of cytokines such as TNF-α and interleukin 6, the half life of PCT in the systemic circulation is, at 25 to 30 hours, rather long.31
Interleukin 8 is an important neutrophil activating cytokine which is mainly produced by activated resident macrophages and endothelial cells.21 Stimuli for IL-8 release from activated mononuclear cells are bacterial lipopolysaccharide, interleukin 1, and TNF-α; in epithelial cells, fibroblasts, and hepatoma it can only be induced by cytokines. In patients with acute pancreatitis, neither the source nor the inducing factors of circulating IL-8 are known; however, a strong correlation with neutrophil elastase has been shown and both have proved to be early predictors of disease severity.23 ,24 This observation further underscores the hypothesis of the predominating role of polymorphonuclear leucocytes in the pathogenesis of complicated pancreatitis.32 In normal subjects, IL-8 levels are usually around 20 pg/ml and do not exceed 70 pg/ml.
Our data show for the first time that PCT closely correlates with both the morphological features of infected necrosis and the severity of associated systemic complications, whereas IL-8 is indicative of septic multiple organ failure in patients with severe acute pancreatitis.
PCT had the closest correlation to the presence as well as to the severity of infection. Among 18 patients who developed infected necrosis 17 were correctly identified before or at least parallel to the time when infection was intraoperatively confirmed; PCT concentrations were higher in patients with associated septic multiple organ failure. In patients with primary infected necrosis fine needle aspiration was found to have the same diagnostic accuracy in detecting infection as obtained by PCT assessment. In the postoperative course PCT proved to be a sensitive indicator as to whether infected necrosis had been successfully evacuated, but surgery itself did not result in a postoperative increase as long as infection was absent. The fact that PCT monitoring reflects response or non-response to treatment has also been reported by other authors.13 ,14 ,20 In contrast, acute phase parameters like C- reactive protein or IL-6 are elevated in response to both infectious and non-infectious (for example, postoperative) stimuli,14 ,15 so that an estimation as to the presence or absence of infection is not possible, which we could confirm for C reactive protein.
Despite our encouraging results is has to be emphasised that PCT is a non-specific indicator of bacterial/fungal infection and sepsis and does not provide any information about the underlying source of infection. In our series three patients had persisting PCT levels of at least 1.8 ng/ml although they did not suffer from infected necrosis: one patient had sterile necrosis and developed adult respiratory distress syndrome (ARDS) due to pneumonia (Pseudomonas) and clinically severe sepsis (PCT peak value 37.2 ng/ml), and two had mild biliary pancreatitis, complicated in one by cholecystitis (peak value 3.5 ng/ml) whereas in the other no cause of PCT elevation (peak value 13.2 ng/ml) could be found. In all three patients, however, PCT concentrations had returned to normal within one week of treatment. Pulmonary insufficiency and subsequent progression into ARDS is a frequent complication in severe pancreatitis (table 2). In the case of bacterial superinfection, elevated PCT levels are not able to differentiate between a pulmonary or pancreatic source of infection and guided fine needle aspiration is still necessary to prove or exclude infection in the pancreatic region. On the other hand, early organ complications in acute pancreatitis are generally not due to infection, but are a consequence of activated mediators and enzymes such as phospholipase A2, leukotrienes, oxygen radicals, and various cytokines10 and do not result in a PCT increase as observed in five patients with sterile necrosis and severe pulmonary insufficiency who required mechanical ventilation.
It furthermore remains unclear why in most patients who developed infected necrosis and died in the later course of the disease excessively high PCT levels had already been present days before the diagnosis of infected necrosis had been confirmed intraoperatively. Studies in humans indicated that PCT increases time dependently following a TNF-α rise, if endotoxin is administered inravenously.31 TNF a is itself known to play a central role in the pathogenesis of various severe diseases associated with increased mortality11 ,32; in acute pancreatitis it was found to be an initiator of local and systemic damage.11Although the interaction of PCT and TNF-α is not clear, it could be hypothesised that via TNF-α, PCT is a marker of the degree of severe systemic inflammatory respone and diffuse cell damage. As a consequence, it might therefore be easier for bacteria to translocate and cause subsequent infection in the later course of the disease. Possible immunomodulatory effects of PCT may be involved, which would further explain this theory.33 Unfortunately, there are currently no data about the behaviour of PCT before the diagnosis of infection or sepsis was made. The only longitudinal study done in patients with burns in which PCT levels were monitored soon after the trauma over at least seven days, however, did not differentiate between patients with infectious complications and those without.29
We could not confirm the previous findings of Brunkhorst et al that elevated PCT levels are associated with a biliary origin of acute pancreatitis.34 In table 1 of their paper, an overview of clinical features and PCT concentrations of all patients suspected to have biliary pancreatitis is provided. A closer analysis reveals however, that PCT levels were highest (greater than 100 pg/ml) in two patients with sepsis. In six patients with PCT levels between 2 and 55 pg/ml cholecystitis was present in two and one died from necrotising pancreatitis. The difference in results is therefore most pobably due to a lack of continuous serum PCT monitoring and a proper morphological stratification into infected/septic and non-infected patients. This observation stresses the importance of monitoring these parameters (at least two or more values) to obtain any reliable information.
In our series, IL-8 assessment has proven less helpful in the prediction of infected necrosis compared with PCT and even C-reactive protein. The overall sensitivity of IL-8 in the detection of patients with infected necrosis was 72%; in patients with primary infected necrosis only 20% were correctly identified as being infected. IL-8 was found to have a strong correlation with the presence of septic multiple organ failure which was indicated by a constant rise in IL-8 concentrations to at least 140 pg/ml, usually during the second week of the disease, but was not superior to PCT and even C- reactive protein assessment. It has to be added however, that the time period in which the respective cut off levels had been reached was around the fourth day after onset of symptoms for C-reactive protein and during the second week for IL-8. Therefore, IL-8 provided important information during the later stages of acute pancreatitis, for example, in patients with persisting high PCT concentrations in whom IL-8 only increased if severe septic multiple organ failure developed and C-reactive protein rarely exceeded 300 mg/ml. Irrespective of the degree of C reactive protein elevation, IL-8 concentrations remained almost uniformly below 112 pg/ml in patients with toxic multiple organ failure and sterile necrosis as well as in patients with infected necrosis without multiple organ failure and did not rise as a consequence of surgical trauma. We can therefore not confirm the observation of other authors, that IL-8 is an early indicator of severity.22 ,23 This may be due to several reasons: firstly, in both studies patients were monitored for only the first seven days after onset of symptoms, a time when septic multiple organ failure is usually not yet present; secondly, that the overall disease severity in these series was lower than in ours; and thirdly, that the very early stages of acute pancreatitis were not addressed by our study (only nine patients with mild pancreatitis were investigated from the first day of disease) in which a possible IL-8 elevation could have been missed. However, if the patient series of Gross et al 22 is analysed closer, IL-8 concentrations were highest in patients with sepsis which is in accordance with our findings. As demonstrated for PCT, IL-8 also reflected response or non-response to surgical treatment. At this point, however, it is important to note that the administration of antibiotics alone had no effect on both elevated PCT or IL-8 levels in patients who developed infected necrosis.
As IL-8 is known to be a very potent neutrophil activating cytokine, our results further support the theory that PMN leucocytes play a central role in the development of severe acute panceatitis.32 The observation of a positive correlation between PCT and IL-8 concentrations in only those patients with septic multiple organ failure as the result of infected necrosis suggests that these parameters obviously have different pathways within the inflammatory cascade which, however, both lead to severe infection and sepsis, either Gram positive or negative, in acute pancreatitis. Since the source and the inducing factors of PCT and IL-8 production are not known, further studies are needed to clarify a possible inter-relationship.
Another noteworthy observation is the fact that there were eight patients in the group with infected necrosis who developed infection after surgery for initially severe sterile necrosis, which has already been described in the literature.27 As no prospective controlled data exist about the optimum treatment of severe sterile necrosis, is remains unclear whether infection in these patients merely represented the natural course of the disease or whether it was induced by the surgical procedure.
In summary, PCT and IL-8 are found in high concentrations in infected necrosis and associated systemic complications in patients with acute pancreatitis. PCT could be a potential new indicator for selecting patients at risk of developing infectious complications in acute pancreatitis. Monitoring of IL-8 may provide valuable information on the severity of septic complications in critically ill patients. With respect to practical aspects, both PCT and IL-8 are commercially available standardised kits. The time and equipment needed for individual PCT or IL-8 analysis are advanced enough to fit the demands for use in the laboratory routine. If further studies can confirm our promising results under prospective daily routine conditions, monitoring of PCT and IL-8 could contribute to an easier and more cost effective identification of patients in whom further diagnostic or therapeutic procedures are necessary.
References
Footnotes
↵* Both authors contributed equally to this paper.