Article Text

Abstract
Background—It has been reported that the acidity of gastric contents could be an important factor in regulating jejunal flora.
Aims—To investigate the effects of omeprazole induced changes in gastric pH on jejunal flora and bile acid metabolism.
Methods—Twenty one patients with gastric ulcer and 19 healthy volunteers were studied. Deconjugation of bile acids was detected using a bile acid breath test. Jejunal fluid was aspirated using a double lumen tube with a rubber cover on the tip and deconjugation was examined using thin layer chromatography. Fat malabsorption was detected by a triolein breath test.
Results—In the bile acid breath test, expired breath samples from all patients and healthy volunteers showed significantly greater 14CO2 specific activity after omeprazole treatment (20 mg/day) than before treatment. Bacterial overgrowth was found in the jejunal fluid and gastric juice of both ulcer patients and healthy volunteers after omeprazole treatment. The following species were identified: Escherichia coli,Candida albicans, enterococcus, Lactobacillus bifidus, Bacteroides vulgatus, B uniformis, Eubacterium lentum, Eu parvum, and Corynebacterium granulosum. All of these species, except E coli and C albicans, deconjugate bile acids. There was a significant correlation between14CO2 activity and gastric pH, both before and after omeprazole treatment in both groups. The triolein breath test revealed impaired fat absorption in both groups after omeprazole treatment.
Conclusions—Both patients with gastric ulcer and healthy volunteers exhibited increased deconjugation of bile acids caused by bacterial overgrowth in the jejunum and fat malabsorption after omeprazole treatment. The bacterial overgrowth consisted of both anaerobes and aerobes with deconjugation ability and was probably associated with an omeprazole induced shift to neutral pH in the gastric juice.
- omeprazole
- bacterial overgrowth
- deconjugation
- bile acid breath test
- gastric pH
- gastric ulcer
Statistics from Altmetric.com
The reduction of gastric acidity by antacids,1-3H2 receptor antagonists,1 ,4 ,5 and omeprazole —a substituted benzimidazole that is a potent proton pump inhibitor6-8—has been reported to increase gastric bacterial colonisation. Decreased gastric acidity due to atrophic gastritis is a common cause of reduced gastric secretion, resulting in overgrowth of gastric flora.9 ,10 Omeprazole potently inhibits gastric acid secretion by altering the activity of H+/K+ adenosine triphosphatase7and reduces intragastric acidity more effectively than H2receptor antagonists.11 This decrease in gastric acid secretion with omeprazole is long lasting.12-14 Thus, omeprazole may also increase bacterial colonisation in the jejunum, by altering jejunal pH due to gastric hypochlorhydria. The clinical consequences of omeprazole induced bacterial overgrowth in the jejunum are not however clear.
We formulated the following hypothesis: increased bile acid deconjugation in the jejunum of patients receiving omeprazole occurs due to bacterial overgrowth in the jejunum, induced by gastric hypochlorhydria.
To test this hypothesis, we determined whether: (1) patients with gastric ulcer and healthy volunteers who have received omeprazole exhibit positive bile acid breath tests due to bacterial overgrowth in the jejunum; (2) the bacteria in the jejunum are capable of deconjugation; (3) the deconjugation of glycine-1-14C labelled glycocholate is related to the change in gastric pH induced by omeprazole; and (4) subjects with a positive bile acid breath test exhibit fat malabsorption.
Materials and methods
Breath tests and bacterial studies were performed in 21 patients with gastric ulcer and 19 healthy volunteers at the First Department of Internal Medicine, Yokohama City University School of Medicine. The study was approved by the Ethical Committee of Yokohama City University School of Medicine. Written informed consent was obtained from each subject.
STUDY SUBJECTS
The study involved 21 male patients with gastric ulcer (group 1) and 19 healthy male volunteers (group 2) who were treated with oral omeprazole 20 mg daily before breakfast for five weeks. The healthy volunteers (aged 24–75 years) were not taking other medication at the time of the study. The patients (aged 27–71 years) were allowed (but not encouraged) to take antacids in addition to omeprazole. Patients with benign gastric ulcer at the time of routine endoscopy were included; those who were considered suitable for medical treatment were given omeprazole and the importance of strict compliance with the treatment regimen was emphasised.
Following diagnosis by endoscopy, an initial 14C glycocholic acid breath test (glycine test) and 14C triolein breath test (triolein test) were performed, jejunal fluid and gastric juice were sampled by a double lumen tube,15 and gastric pH was checked before omeprazole treatment. The usual dose of oral omeprazole (20 mg/day before breakfast) was given for five weeks. The same tests were performed in the healthy volunteers after endoscopy confirmed that there were no abnormal gastric findings.
The second glycine and triolein tests were performed in each subject in both groups after treatment with omeprazole for two weeks. Jejunal fluid and gastric juice were sampled using a double lumen tube, and the gastric pH was measured for the next two weeks during omeprazole treatment. Subjects with a positive glycine test underwent a third set of glycine and triolein tests after receiving oral tetracyline 1 g/day in divided doses for seven days during the 35 day course of omeprazole treatment. Generally, the triolein test was performed the day after the glycine test.
14C TRIOLEIN BREATH TEST
After an overnight fast, 14C labelled triolein (5 μCi), dissolved in 30 ml of a high energy dietary supplement (Lipomul),18 was administered between 06.00 and 08.00 hours following each 14C glycocholic acid breath test. The subjects remained at rest throughout the six hour study period during which hourly breath samples were taken; expired14CO2 was collected and measured, as noted earlier. Results are expressed as six hour cumulative14CO2 output as a percentage of the ingested activity.19-21
BACTERIAL CULTURES AND DECONJUGATION CAPABILITY
Jejunal fluid and gastric juice were aspirated through a double lumen tube with a rubber cover on the tip.15 This tube was positioned fluoroscopically at 30 cm past the ligament of Treitz in fasting subjects. The rubber cover was forced off by the instillation of saline just before the aspiration of jejunal fluid. Gastric juice was obtained by suctioning via the other lumen. Bacteria were cultured using the conventional plate method. All isolated anaerobes and aerobes were identified according to standard methods.22 ,23Jejunal and gastric colonisation were defined as more than 105 bacteria per 0.5 ml of aspirate. Bacteria normally present in the small intestine (such as lactobacilli and streptococci) were also included in the colony counts. A loopful of bacteria from the plate cultures was inoculated into 10 ml of broth that contained 0.5 ml of sterilised ox gall instead of synthetic conjugated bile acid. Anaerobes were grown in thioglycolate liquid medium while the aerobes were grown in glucose medium. Incubation was performed at 37°C for 48 hours. The broth was acidified to pH 1.0 with hydrochloric acid and extracted three times with two volumes of butanol. The three butanol phases were mixed, washed free of hydrochloric acid, and evaporated to dryness. Residues were dissolved in 2 ml methanol, and 4 μl aliquots were used for thin layer chromatographic analysis. Identification of free and conjugated bile acids was performed by thin layer chromatography, as previously reported.24 ,25
GASTRIC pH
The gastric pH was measured in the morning after a 12 hour fast with all subjects in the supine position, using a glass electrode and a digital pH meter (Shimazu Co. Ltd, Kyoto, Japan). Normoacidity was defined as a pH between 1.5 and 2.0, hyperacidity as a pH less than 1.5, hypoacidity as a pH between 2.4 and 4.0, and anacidity as a pH greater than 4.0.
MATERIALS
Glycine-1-14C labelled glycocholate and14C labelled triolein (specific radioactivity of both, 0.25 μCi/mmol) were purchased from New England Nuclear Corp. (Boston, Massachusetts, USA). Lipomul meals were purchased from Upjohn Co. (Kalamazoo, Michigan, USA). The trapping solution for exhaled CO2 (0.50 mmol/ml) was prepared using equal amounts of 1 M hyamine hydroxide (Packard Instruments Corp., Downers Grove, Illinois, USA) and absolute ethanol (containing 60 mg/l of phenolphthalein as an indicator).
STATISTICAL ANALYSIS
Data are expressed as mean (SD) and as median (range). Logarithmic transformation of the AUC0–6 was used for statistical analysis. Paired and unpaired Student’s t tests were used for statistical comparisons of data conforming to normal distributions. Correlations between variables were determined using linear regression. Differences were considered statistically significant at a level of p<0.05.
Results
14C GLYCOCHOLIC ACID BREATH TEST
In group 1, the mean cumulative specific activity (percentage administered dose/mmol CO2/6 h; AUC0–6) was 2.05 (0.88) × 10−3 and the mean total exhaled14CO2 was 1.49 (0.40)% of the administered dose, before omeprazole treatment. These values were 9.74 (5.40) × 10−3 and 5.34 (2.87)%, respectively, after omeprazole treatment. There were significant differences in both parameters before and after omeprazole treatment (p<0.05, paired t test).
All 17 patients who received oral tetracycline for seven days exhibited flat curves. The mean cumulative specific activity in this group was 1.65 (0.34) × 10−3, and the mean total exhaled14CO2 was 1.27 (0.27)%. Before the administration of tetracycline, these values were 10.71 (5.48) × 10−3 and 5.79 (2.96)%, respectively, in this group. Thus, these parameters were significantly reduced by tetracycline.
In group 2, the mean cumulative specific activity was 2.53 (0.97) × 10−3 and the mean total exhaled14CO2 was 1.99 (0.58)% of the administered dose, before omeprazole treatment. These values were 9.71 (5.71) × 10−3 and 5.58 (2.79)% after omeprazole treatment. There were significant differences in both parameters before and after omeprazole treatment (p<0.05, paired ttest).
All 12 subjects who received oral tetracycline for seven days exhibited flat curves. The mean cumulative specific activity in this group was 1.71 (0.33) × 10−3, and the mean total exhaled14CO2 was 1.20 (0.17)%. Before administration of tetracycline, these values were 11.44 (6.61) × 10−3and 6.50 (3.18)%, respectively, in this group. Thus, these parameters were significantly reduced by tetracycline.
BACTERIAL CULTURES AND DECONJUGATION CAPABILITY
Jejunal flora—As shown in table 1, in group 1, 19 of the 21 patients showed no growth before omeprazole treatment. The remaining two patients showed colonisation (more than 105colonies/0.5 ml) with Escherichia coli. After omeprazole treatment, however, 12 patients had colonisation and nine showed no growth. After tetracycline treatment, 11 of the 13 patients tested showed no growth. The remaining two showed colonisation with E coli and Candida albicans. In group 2, 16 of the 19 subjects showed no growth before omeprazole treatment. The remaining three subjects had colonisation (more than 105 colonies/0.5 ml) with E coli. After omeprazole treatment, 11 subjects had colonisation and eight showed no growth. After tetracycline treatment, 10 of the 11 subjects tested showed no growth. The remaining subject showed colonisation with E coli.
Jejunal bacterial flora in patients with gastric ulcer (group 1) and healthy volunteers (group 2)
Gastric flora—As shown in table 2, in group 1, 20 of the 21 patients showed no growth before omeprazole treatment. The remaining patient showed colonisation with E coli. After omeprazole treatment however, 11 patients had colonisation and 10 showed no growth. After tetracycline treatment, 11 of the 13 patients tested showed no growth. The remaining two subjects showed colonisation withE coli and C albicans. In group 2, 17 of the 19 subjects showed no growth before omeprazole treatment. The remaining two subjects had colonisation with E coli. After omeprazole treatment, nine subjects had colonisation and 10 showed no growth. After tetracycline treatment, eight of the 11 subjects tested showed no growth. The remaining three showed colonisation with E coli and C albicans.
Gastric bacterial flora in patients with gastric ulcer (group 1) and healthy volunteers (group 2)
Thin layer chromatography findings showed that isolated E coli and C albicans did not deconjugate ox gall.15 The other isolated species (enterococcus,Lactobacillus bifidus, Bacteroides vulgatus,B uniformis, Eubacterium parvum, Eu lentum, and Corynebacterium granulosum) however, were able to deconjugate ox gall.
GASTRIC pH
Before omeprazole treatment, the mean values of gastric pH in groups 1 and 2, respectively, were 2.17 (0.90) and 1.73 (0.59). After omeprazole treatment, the corresponding values were 4.42 (1.45) and 4.44 (1.10). There were significant differences in gastric pH before and after omeprazole treatment in both groups (paired Student’st test, p<0.05). Figure 1 presents the correlations between AUC0–6 and gastric pH in both groups. AUC0–6 was significantly correlated with gastric pH both before and after omeprazole treatment in the two groups (r 2=0.570 and 0.755, respectively, in group 1 (n=21) and r 2=0.380 and 0.550 in group 2 (n=19); p<0.05).
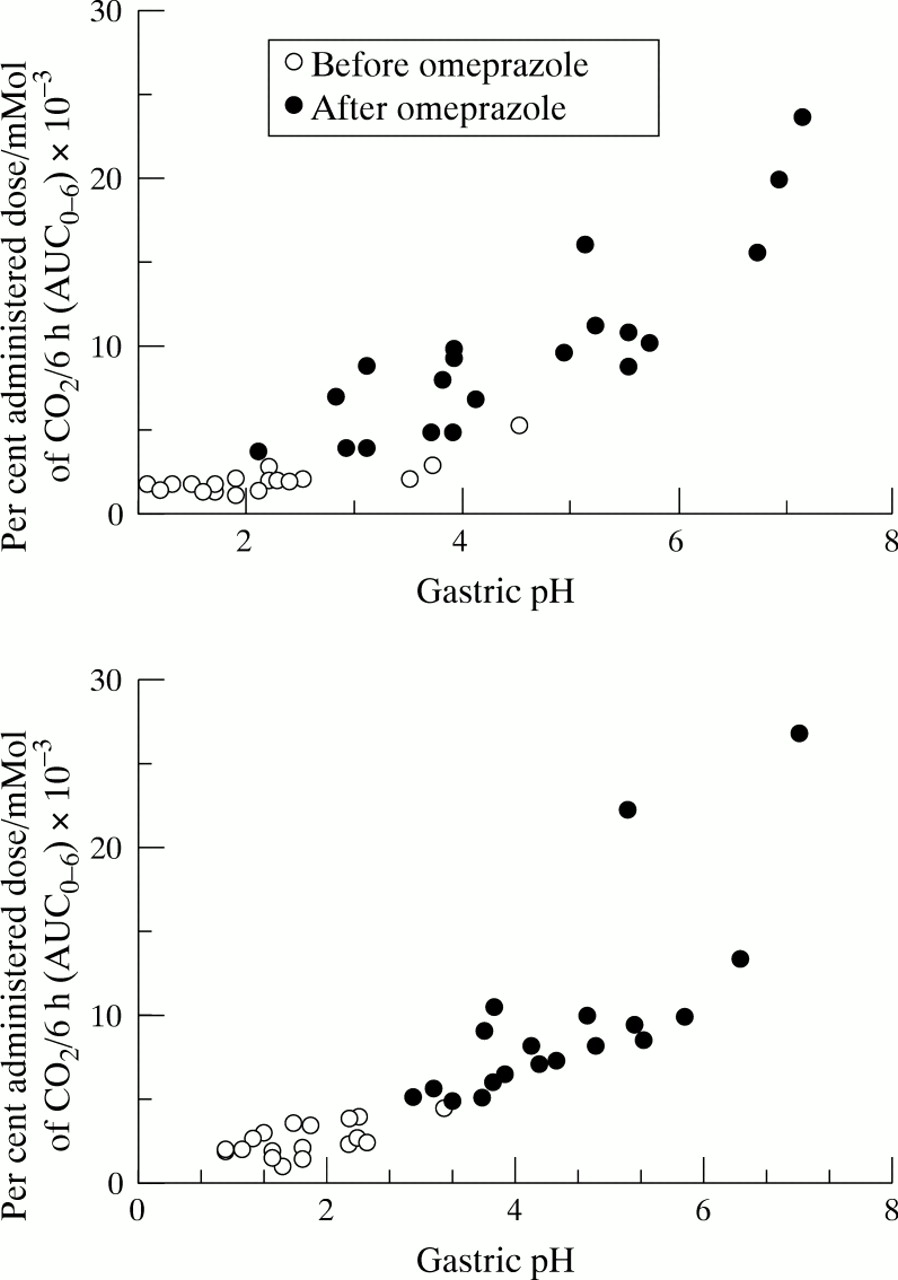
Correlation of gastric pH and AUC0–6before and after omeprazole treatment in groups 1 (upper panel) and 2 (lower panel).
14C TRIOLEIN BREATH TEST
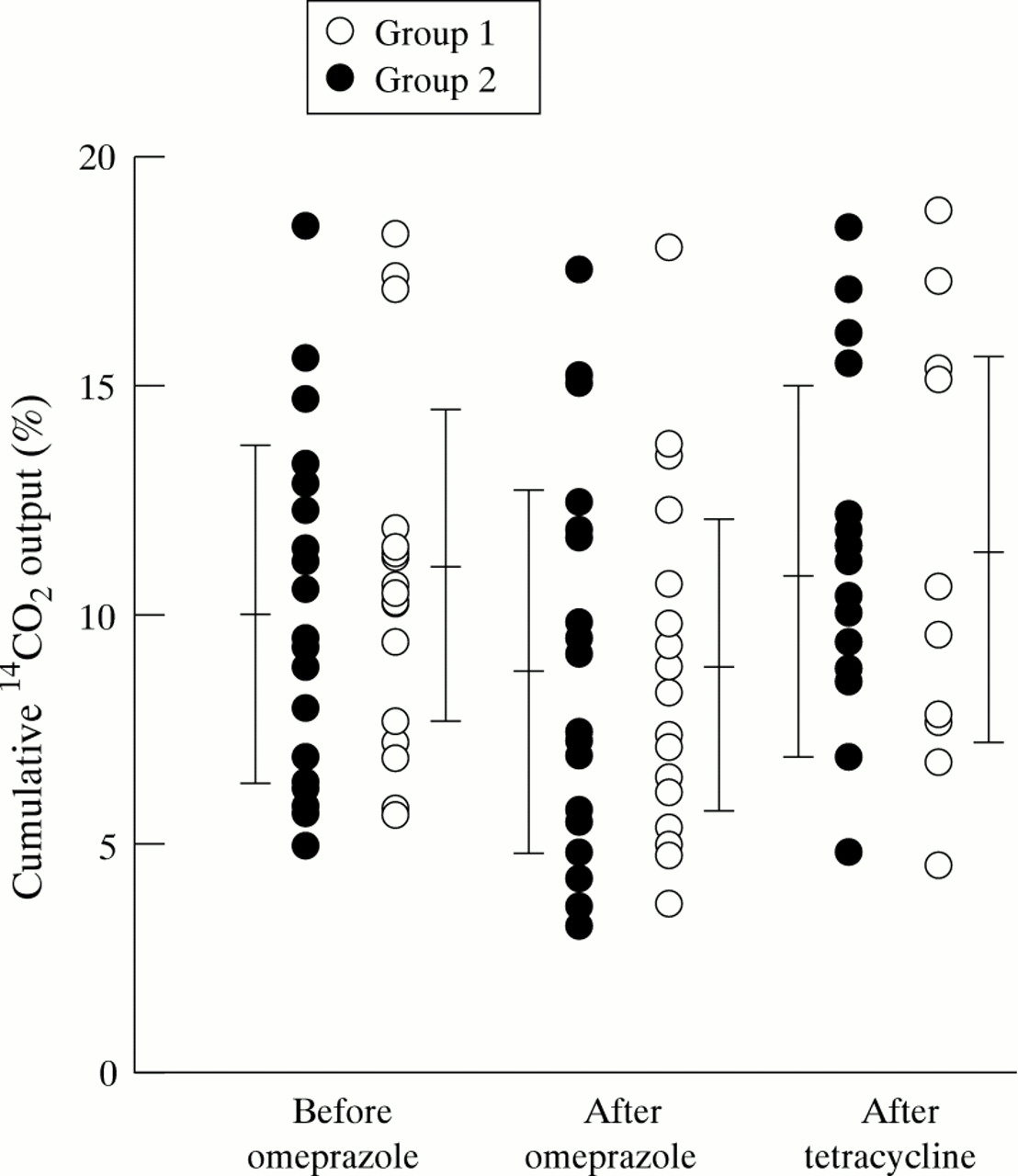
In group 1, the cumulative 14CO2 output per six hours was 10.21 (3.62)%, 8.70 (4.08)%, and 11.18 (3.97)% of the administered dose before and after omeprazole treatment, and after tetracycline treatment, respectively.
In group 2, the cumulative 14CO2 output per six hours was 10.72 (3.72)%, 8.61 (3.78)%, and 11.41 (4.48)% of the administered dose before and after omeprazole treatment, and after tetracycline treatment, respectively.
After omeprazole treatment, both groups had significantly lower cumulative six hour 14CO2 outputs, consistent with impaired fat absorption (p<0.05, paired t test). There was no significant difference between the two groups (fig 2).
{kind=link}
{kind=link}
14C triolein breath test. Breath cumulative output of 14CO2 (% administered dose/6 h) after ingestion of 5 μCi of 14C triolein in 30 ml of Lipomul. All data indicate mean values with 1 SD error bars.
Discussion
Our data show bacterial overgrowth in the stomach and jejunum of patients with gastric ulcer and in healthy volunteers after treatment with omeprazole. These bacteria alter the metabolism of bile acids and induce fat malabsorption, as evidenced by increased14CO2 output after the administration of glycine-1-14C labelled glycocholate and decreased14CO2 output after the administration of14C triolein. Most of the observed species of bacteria had deconjugation capability. The bacterial overgrowth appeared to be associated with an omeprazole induced shift to neutral pH in the gastric juice. There were no significant differences in gastric pH or AUC0–6 between the two groups.
An increase in deconjugation of bile acids due to bacterial overgrowth in the upper small intestine has been shown in patients with several diseases using a breath analysis technique based on glycine-1-14C labelled glycocholate. Increased deconjugation is detected by an increase in the excretion of14CO2 in expired air and an early rise in14CO2 output.16 ,17 Possible and classic causes of bacterial overgrowth include blind loop syndrome and ileal bypass, which cause stasis of jejunal fluid, and anatomic abnormalities of the intestine, which permit rapid bacterial overgrowth.16 ,17 Pharmacologically, omeprazole induced hypochlorhydria produces periods during the day in which the gastric juice is at or near a neutral pH when omeprazole is given once daily.11 The findings of the present study showed that hypochlorhydria not only was clearly sufficient to induce major changes in the gastric flora, but also affected the pH of the jejunal fluid sufficiently to allow bacterial overgrowth in the jejunum. Several published studies have examined the influence of gastric pH on bacterial growth in the jejunum and the source of bacterial overgrowth in the jejunum. Gastric juice pH has been reported to be an important factor influencing bacterial growth in the small intestine; gastric and jejunal contents of patients with partial gastrectomy, gastroenterostomy, or pernicious anaemia permitted significant growth of coliform bacilli.26 The effect of gastric hypochlorhydria on the distribution of bacteria in the intestines could be sufficiently predicted from these results.27
The number of bacteria passing from the stomach to the small intestine undoubtedly increases during hypochlorhydria. In a study using long tube aspiration in 19 healthy volunteers,28 the small bowel microflora was found to consist of small numbers of streptococci, lactobacilli, staphylococci, and fungi. In addition, the most common bacteria in the distal ileum (the anaerobes Bacteroides,Eubacterium, and Corynebacterium) were detected in these samples.28 We also found these anaerobic species in our jejunal fluid samples (table 1). Our results suggest therefore that the bacterial overgrowth in the jejunum contains anaerobes from the distal ileum as well as bacteria passing from the stomach (table 2), although the possibility is not ruled out that overgrowth of bacteria naturally living in the jejunum also occurs. Interestingly, the omeprazole induced shift to a more neutral pH in the gastric juice may promote the migration and growth of anaerobes from the distal ileum.
Regarding the site of deconjugation, it has been reported that after omeprazole administration, bacterial colonisation increases in the gastric juice.11 Some of these bacteria may exhibit deconjugation capability. In the present study, we did not determine whether the stomach or the jejunum was the site of deconjugation of orally administered glycine-1-14C labelled glycocholate. We cannot rule out the possibility that the deconjugation detected in the breath test took place, at least in part, in the stomach before the passage of bile acids into the jejunum, because L bifidusand enterococcus with deconjugation capability were detected in the gastric juice. Due to the fact that several anaerobes with deconjugation capability were also present in the jejunal fluid however, it is conceivable that at least some deconjugation occurred in the jejunum as well as in the stomach. It is possible therefore that conjugated bile acids in human bile are deconjugated by bacterial species that have overgrown in the jejunum of individuals with increased gastric pH.
The possibility of adverse effects after long term treatment with omeprazole has not been explored thoroughly, although a few adverse effects have been reported in clinical trials since 1983.7 ,29 ,30 We have shown significant fat malabsorption induced by omeprazole in the present study. Saltzman et alreported that elderly subjects with bacterial overgrowth and hypochlorhydria induced by omeprazole did not exhibit fat malabsorption.31 The method for detecting fat absorption was different from that used in the present study, which may explain the different results. Judging from our data, bacterial overgrowth in the jejunum causes fat malabsorption via increased deconjugation of bile acids even in the absence of a blind loop.32
We previously reported that cimetidine, an H2 receptor antagonist, induced bacterial overgrowth in the jejunum of healthy subjects, which promoted deconjugation of bile acid.33 ,34Patients with gastric ulcer and healthy volunteers treated with omeprazole had slightly higher mean cumulative specific activity than healthy volunteers treated with cimetidine. Although this difference was not significant, the higher degree of deconjugation following omeprazole treatment may be explained by the greater reduction in intragastric acidity with omeprazole than with cimetidine35 and the increased incidence of gastric and duodenal bacterial overgrowth in patients treated with omeprazole versus cimetidine.36 Similarly, fat malabsorption may differ, as shown in the present study.
In addition, the mean value in cirrhotic patients with positive breath tests was reported as 18.70 (6.01)%, with a mean gastric pH of 6.74 (0.39).37 The cirrhotic patients also had fat malabsorption. There was a close relation between mean cumulative specific activity and gastric pH; this may be of clinical significance. Deconjugation of bile acids by bacterial overgrowth in the jejunum may lead to fat malabsorption, and this should be taken into account when long term treatment with omeprazole is being considered.
Omeprazole induced bacterial overgrowth has been shown in the upper small intestine in humans.32 ,38-40 These data were, however, fragmentary and inconclusive. In addition, insufficient evidence has been obtained concerning increased deconjugation during treatment with omeprazole. Additional questions involve the identification of bacteria that overgrow in the jejunum, the deconjugation capability of these bacteria, simultaneous examination and direct comparison of the gastric and jejunal flora, and whether subjects with a positive bile acid breath test exhibit fat malabsorption. This is the first study to investigate these questions.
In summary, we have confirmed that after long term treatment with omeprazole, patients with gastric ulcer as well as healthy volunteers show increased deconjugation of bile acids and fat malabsorption caused by bacterial overgrowth in the jejunum. The bacterial overgrowth is composed of both anaerobes and aerobes with deconjugation capability and is promoted by omeprazole induced sustained hypochlorhydria in the gastric juice.
Acknowledgments
The authors gratefully acknowledge the review of this manuscript by Dr M Tanaka and Miss E I R Bryan.
References
Linked Articles
- COMMENTARY