Article Text

Abstract
Background—Secretory immunity is a major defence mechanism against infections at mucosal surfaces which are common in HIV infected patients.
Aims—To analyse intestinal immunoglobulin production in HIV infection in comparison with that in saliva and serum.
Patients and methods—Immunoglobulin G (IgG), A (IgA), and M (IgM) concentrations were determined in supernatants of short term cultured duodenal biopsy samples, serum, and saliva from HIV infected patients (n = 28) and controls (n = 14) by radial immunodiffusion.
Results—IgG was increased in the supernatants of short term cultured biopsy samples and saliva from HIV infected patients compared with controls (p<0.01), but IgA and IgM levels were normal. In contrast, both IgG and IgA concentrations in serum were higher in HIV infected patients than in controls (p<0.002). No correlation was found between IgA produced by duodenal biopsy specimens and serum IgA.
Conclusion—Abnormalities in mucosal immunoglobulin production in HIV infection were suprisingly small, indicating that specific secretory immunity rather than quantitative immunoglobulin production may be impaired. However, increased production of IgG could contribute to mucosal inflammation by complement activation. Our findings of normal mucosal IgA production and the lack of correlation between serum and mucosal IgA argues against an intestinal origin for the increased serum IgA levels in HIV infected patients.
- mucosal immunity
- HIV infection
- intestinal antibodies
Statistics from Altmetric.com
The local immunological defects underlying the frequent development of gastrointestinal symptoms in patients infected with HIV are poorly understood. Immunoglobulins, especially IgA and IgM, play a key role in protecting the intestinal tract from potential pathogens because they are secreted in large amounts into the gut lumen, where they bind infectious agents, thereby blocking their adhesion and entry into the mucosa. It has been shown that CD4 T cell depletion in the lamina propria is an early event in the course of HIV infection.1 ,2 This could lead to impaired secretory immunity since CD4 T cells play a crucial role in mucosal B cell differentiation and antibody production3 . Conflicting data exist on mucosal immunoglobulins in HIV infection. An early study found a reduced proportion of IgA plasma cells in the large intestine of AIDS patients,4 but increased numbers of antibody-producing lamina propria B cells of all immunoglobulin isotypes in the duodenum of HIV infected patients have also been described.5 Similarly both normal6 and decreased salivary IgA concentrations7-9 have been found when HIV infected patients and controls have been compared. IgA concentrations in duodenal fluid were examined in one study and were not different between AIDS patients and controls.10Furthermore, it is not clear whether salivary immunoglobulins correctly mirror intestinal secretory immunity, and exudation of serum proteins as well as enzymic digestion may confound analysis of mucosal immunoglobulin production in intestinal fluids. We therefore used short term culture of duodenal biopsy samples to investigate local production of immunoglobulin in the intestinal tract of HIV infected patients and controls.
Material and methods
PATIENTS
We studied 28 HIV infected patients undergoing diagnostic upper endoscopy to investigate diarrhoea (n = 14) or other gastrointestinal symptoms (n = 14). Twenty two patients had AIDS, and six were at earlier stages of HIV infection. In 13 patients an infectious agent was detected in stool or intestinal biopsy specimens (one cytomegalovirus, two coronavirus, one microsporidium, one cryptosporidium, threeGiardia lamblia, two Salmonella enteritidis, two Clostridium difficile, one Mycobacterium avium complex). Twenty five patients were homosexual or bisexual men, one man used intravenous drugs, and in two men the risk for HIV infection was unknown. The patients were 29–55 (median 43) years old and had 0–987 (median 65) CD4 T cells per μl in the peripheral blood.
The controls without any risk for HIV infection (11 men, three women) were endoscopically investigated because of suspected ulcer or tumour which could not be confirmed. They were 28–74 (median 45) years old. Control patients had no visible abnormalities as assessed by upper endoscopy and histological examination of the biopsy specimens.
The study was approved by the local ethics committee.
SAMPLE COLLECTION
Serum was collected from peripheral venous blood. For collecting mixed saliva a commercially available Salivette system (Sarstedt, Nümbrecht, Germany) was used as described previously.11This system consists of a polystyrene two chamber centrifuge tube with a cotton wool roll in the inner chamber. The participants were asked to keep the cotton wool roll in the buccal cavity for two minutes. The roll was carefully removed, placed into the tube, and centrifuged for ten minutes at 1500 g. The fluid in the second chamber in the tip of the tube was used for the quantification of immunoglobulins.
Serum and saliva samples were stored at −70°C until assay. Three biopsy samples were taken from macroscopically normal areas of the distal duodenum in all patients and controls.
SHORT TERM CULTURE OF INTESTINAL BIOPSY SAMPLES
Culture supernatants of intestinal biopsy samples for the detection of local antibody production were prepared by a modified method described by Crabtree et al.12 Biopsy samples were immediately placed into phosphate buffered saline and extensively washed (five times) in 30 ml of this solution. All biopsy samples were weighed. Three were then incubated in 1.5 ml RPMI 1640 medium containing 10% fetal calf serum (Gibco-BRL, Berlin, Germany), 100 U/ml penicillin, 100 μg/ml streptomycin, 50 μg/ml gentamicin, and 2.5 μg/ml amphotericin (Seromed Biochrom KG, Berlin, Germany) at 37°C in a humidified 5% carbon dioxide/95% air atmosphere for 48 hours. Supernatants were stored at −70°C until assay.
DEMONSTRATION OF DE NOVO SYNTHESIS OF IMMUNOGLOBULINS
De novo synthesis of immunoglobulins in supernatants of short term cultured biopsy samples was shown by radiolabelling of immunoglobulin disulphide bonds followed by immunoprecipitation with Sepharose/anti-IgA antibody. Biopsy samples, prepared for short term culture as described above, were radiolabelled with 0.5 mCi [35S]methionine in 2 ml Dulbecco’s modified Eagle’s medium (Gibco-BRL). After 48 hours, supernatants were harvested, centrifuged at 13 000 g and incubated with Protein A/Sepharose (Pharmacia, Freiburg, Germany) alone or with Protein A/Sepharose/anti-IgA antibody (Pharmacia) for one hour at room temperature. The supernatants were washed three times with 10 mM Tris buffer containing 1% Nonidet P40, 0.5% sodium deoxycholate, and 0.1% sodium dodecyl sulphate at pH 8.0 and centrifuged at 13 000g. Samples were separated on a 10% polyacrylamide gel by electrophoresis under reducing and non-reducing conditions.
Biopsy specimens from five patients were analysed before and after short term culture for the presence of immunoglobulin. Three biopsy specimens taken from each patient were immediately shock frozen in liquid nitrogen, and another three were used for the preparation of supernatants as described above and shock frozen immediately afterwards. The specimens were stored at −70°C until assay, when they were thawed, homogenised by ultrasonication, and analysed for immunoglobulin concentration.
MEASUREMENT OF IMMUNOGLOBULIN CONCENTRATIONS
IgG, IgM, and IgA levels were determined by radial immunodiffusion using a commercial system (Partigen immunodiffusion plates; Behringwerke AG, Marburg, Germany) according to the manufacturer’s instructions. LC-Partigen immunodiffusion plates were used for saliva, supernatant from short term biopsy cultures, and biopsy homogenates. In some cases augmentation of immunoprecipitation (immunoprecipitation intensifier; Immuno, Wien, Austria) was used as suggested by the manufacturer. Immunoglobulin concentrations for the supernatants are given as mg/mg biopsy sample, those for saliva as mg/l, and those for serum as g/l. On comparing immunoglobulin concentrations of supernatants prepared from different duodenal biopsy samples from the same patient, only a small amount of intraindividual variability was observed (coefficient of variation <5%; n = 3).
STATISTICAL ANALYSIS
Results were not normally distributed and therefore are reported as medians and 95% confidence intervals. The non-parametric two tailed Mann-Whitney U test for unpaired data was used to evaluate comparative statistical significance. The non-parametric Spearman rank correlation coefficient was calculated to determine the correlation between the different compartments. p values less than 0.05 were considered to be significant.
Results
De novo synthesis of antibodies in our culture system was shown directly by means of immunoprecipitation of radiolabelled IgA from supernatants followed by electrophoresis. Under non-reducing and reducing conditions the precipitated protein migrated at 160 and 55 kDa respectively, which are the expected molecular masses for intact IgA and its heavy chain respectively (fig 1).

Autoradiography of short term cultured biopsy supernatants after 35S-labelling of immunoglobulin disulphide bonds. The two autoradiographs (A, non-reducing conditions; B, reducing conditions) show in lane 1 the Protein A/Sepharose precipitate and in lane 2 the Protein A/Sepharose/anti-IgA precipitate. Under non-reducing conditions the immunoglobulin remains intact and migrates at 160 kDa. Under reducing conditions the immunoglobulin is cleaved into the heavy chain migrating at 55 kDa, seen here, and a band of 25 kDa, not seen on the 10% gel used here which separates molecules in the molecular mass range 29–200 kDa.
Indirect evidence for de novo synthesis of immunoglobulin in our system results from the comparison of the immunoglobulin content in biopsy samples before and after culture. IgA and IgG levels in the supernatants are much higher than in the fresh biopsy samples. Only in the case of IgM could a significant amount be detected in the biopsy sample before culture (fig 2).

Representative example of immunoglobulin isotype (IgG, IgA, IgM) concentrations in 48 hour culture supernatant, and in biopsy samples before and after culture.
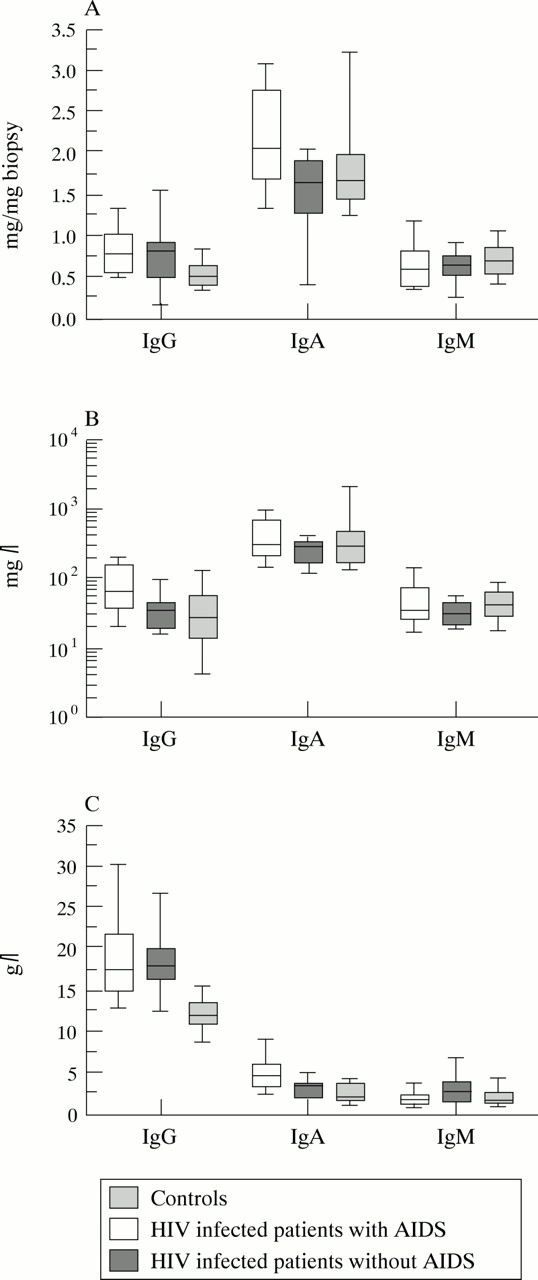
The predominant immunoglobulin found in the supernatants of short term cultured duodenal biopsy samples from both HIV infected patients and controls was IgA with an identical median proportion of 59% of total immunoglobulin. Biopsy samples from HIV infected patients produced more IgG than controls (0.77 (0.57–0.92) v 0.52 (0.38–0.73) mg/mg biopsy; p<0.01), but similar amounts of IgA (1.86 (1.72–2.15)v 1.66 (1.46–1.98) mg/mg biopsy) and IgM (0.60 (0.54–0.77) v 0.68 (0.47–0.79) mg/mg biopsy). There were no significant differences in immunoglobulin concentrations between biopsy supernatant from patients with and without AIDS, although median IgA concentrations were higher in AIDS patients than in patients at earlier stages of HIV infection (p = 0.07; fig 3).

{kind=link}
{kind=link}
{kind=link}
Quantitative analysis of the three isotypes in (A) duodenal biopsy supernatants, (B) saliva, and (C) serum from controls, HIV infected patients with and without AIDS displayed as box plots. Bold horizontal bars represent the median; lower and upper ends of the boxes represent 25th and 75th percentiles respectively; lower and upper “whiskers” represent the 10th and 90th percentiles respectively.
As in the biopsy supernatants, IgA was the predominant immunoglobulin found in saliva from HIV infected patients and controls with a median proportion of 75 and 83% of total immunoglobulin respectively. Salivary IgG concentrations were increased in HIV infected patients compared with controls (49.5 (37–106) v 24 (10–78) mg/l; p<0.05), but concentrations of salivary IgA (313 (224–429)v 283 (156–900) mg/l) and IgM (33.5 (27–48)v 36 (24–64) mg/l) were not different. AIDS patients had higher salivary IgG concentrations than patients without AIDS (p<0.05), who had IgG concentrations similar to controls (fig 3).
In serum, IgG was the predominant isotype, and IgG (17.6 (15.6–20.4)v 11.6 (9.7–15.0) g/l; p<0.002) as well as IgA (4.7 (3.6–5.3) v 2.8 (1.4–4.1) g/l; p<0.002) concentrations were increased in HIV infected patients compared with controls, but IgM concentrations were not different (2.0 (1.6–2.7) v 1.6 (0.9–3.6) g/l). No significant differences were found in serum immunoglobulins between HIV infected patients with and without AIDS, although median IgA concentrations were higher in AIDS patients compared with patients at earlier disease stages (p = 0.08; fig 3).
Concentrations of IgG, IgA, or IgM in serum, saliva, or biopsy supernatant were not different between AIDS patients with and without diarrhoea, or between AIDS patients with or without an infectious agent in stool or intestinal biopsy samples (data not shown).
IgA concentrations produced by duodenal biopsy specimens correlated with salivary IgA concentrations in controls (r = 0.68; p = 0.025) but not in HIV infected patients (r = −0.27; p = 0.79). In HIV infected patients serum IgG concentrations correlated with IgG concentrations in saliva (r = 0.56; p<0.01) and in biopsy supernatants (r = 0.56; p<0.01), although salivary IgG (r = 0.03; p = 0.92) and IgG produced by duodenal biopsy samples (r = −0.20; p = 0.45) were independent of serum IgG in controls. No other significant correlations between immunoglobulin concentrations in the three fluids investigated were observed.
Discussion
We have clearly shown de novo synthesis of IgA and IgG in our culture system, although most IgM seems to be preformed in the biopsy samples. Because no correlation was found between IgM concentrations in serum and in biopsy supernatant, it is likely that the IgM measured was produced by mucosal B cells and released into the supernatant during culture.
The main abnormality found in our study was an increase of about 50% in IgG production by duodenal biopsy samples in both early and advanced stages of HIV infection, but IgM and IgA production were normal. Increased mucosal production of IgG may therefore contribute to the abnormal composition of intestinal secretions in HIV infected patients, although it only partially explains the tenfold higher IgG concentration observed in duodenal fluid from AIDS patients compared with controls,10 which is therefore probably due to the exudation of serum immunoglobulin. A decreased proportion of IgA plasma cells, and increased and normal proportions of IgM and IgG plasma cells respectively, have been found in the intestinal lamina propria of HIV infected patients,4 ,10 and another study reported sevenfold, fivefold, and 20-fold increases in isolated intestinal plasma cells producing IgA, IgG, and IgM respectively in HIV infection.5 None of these abnormalities corresponds to the alterations in immunoglobulin production by duodenal biopsy samples from HIV infected patients, which is probably because of variable amounts of antibodies secreted per cell. Counting plasma cells may therefore not be a valid method to assess mucosal antibody production.
Increased mucosal IgG production has been previously found in patients with inflammatory bowel disease, and it is thought that complement activation by IgG may promote intestinal inflammation in these patients.13 ,14 The increased production of IgG by duodenal biopsy specimens in HIV infection, which was found at early stages of the disease and was independent of the presence of intestinal infection, may therefore contribute to the inflammatory changes frequently observed in the intestine of HIV infected patients.15 However, we found no differences in mucosal immunoglobulin production between patients with and without diarrhoea, which argues against a major role for these abnormalities in the pathogenesis of gastrointestinal symptoms. On the other hand, even mild inflammatory changes might stimulate mucosal HIV replication by the induction of proinflammatory cytokines such as tumour necrosis factor α and interleukin 6 through activation of the NFκB factor.16
As in biopsy supernatant, the only abnormality found in saliva from HIV infected patients was a higher IgG concentration than in saliva from controls. Care was taken in all patients to avoid mucosal lesions during saliva collection which could confound analysis of salivary immunoglobulins. Because the oral mucosa may be more vulnerable in HIV infected patients, we cannot exclude the possibility that the increased salivary IgG in AIDS patients is due to leakage of serum immunoglobulins. Spontaneous salivary IgA secretion seems to be normal in HIV infection, in contrast with the reduced IgA secretion rate observed in stimulated saliva.8 ,9 In support of the concept of a common mucosal immune system, we found a correlation between IgA concentrations in saliva and biopsy supernatant from controls; however, such a correlation was not present in HIV infected patients, indicating that HIV induced abnormalities may be distinct within the mucosal immune system. Thus abnormalities of humoral immunity in saliva may not correctly reflect abnormalities in the intestinal mucosa. Furthermore, no correlation was observed between mucosal and serum IgA, which does not support the hypothesis of a mucosal origin for the increased serum IgA concentrations in HIV infected patients.17 Evidence for ubiquitous polyclonal B cell stimulation, as suggested by Eriksson and coworkers,5was found in our study only for IgG, which showed some correlation between serum and saliva or biopsy supernatant in HIV infection.
Differentiation of mucosal B cells, especially the switch to IgA production, is thought to be critically dependant on regulatory mucosal CD4 T cells.3 In view of the early and pronounced loss of CD4 T cells from the intestinal mucosa in HIV infection,1 ,2 the quantitative abnormalities in mucosal humoral immunity found in our study were surprisingly small. However, it has been recently shown that CD4 deficient mice had normal IgA levels in gut lavage but were unable to develop a specific mucosal IgA response after oral immunisation.18 Therefore, despite quantitatively normal mucosal IgA production, antigen specific humoral immunity may be severely impaired in the intestine of HIV infected patients. In fact, HIV specific antibodies in duodenal secretions from AIDS patients are predominantly of the IgG isotype,10 in contrast with the normal predominance of IgA in mucosal secretions.
Acknowledgments
We are indebted to Marion Lemke, Brigitta Rieger, and Sylvia Münchow for expert technical assistance, and to Ursula Littke and Wolfgang Kronitz for data documentation. This study was supported by grants III-008–91 and 01 KI 9468 from the Bundesministerium für Bildung, Wissenschaft, Forschung, und Technologie. Part of this study was presented at the 8th International Congress of Mucosal Immunology in San Diego.