Article Text

Abstract
Background—Stronger prokinetic agents which specifically enhance transit in different parts of the gut are required. R093877 is a novel 5-HT4 agonist prokinetic compound which is chemically related to cisapride but believed to have greater effect on colonic activity.
Aims—To evaluate the effects of R093877 on bowel function, upper and lower gut transit, visceral sensitivity, and sphincter function in healthy volunteers in a double blind, placebo controlled, crossover study.
Methods—The study consisted of five consecutive one week periods: no drug treatment; active drug treatment with either 1 or 2 mg daily or placebo; washout; active drug or placebo; no treatment. Seventeen male subjects maintained a detailed diary of bowel function for the entire study. Orocaecal transit (breath hydrogen), whole gut transit (radio-opaque markers), and anorectal function were assessed at the end of each of the two treatment periods. Blood testing was performed to confirm compliance and for safety analysis.
Results—One subject withdrew from the study due to side effects while on placebo. Eight subjects completed the study on 1 mg and a further eight on 2 mg. Blood testing showed non-compliance in one subject on the 2 mg dose, and he was excluded from analysis of all diary and physiological data. Treatment increased the number of stools per week (placebo versus 1 mg, 7.8 versus 13.6, p=0.003; placebo versus 2 mg, 8.9 versus 11.3, p=0.15) and the percentage of loose or watery stools (24.2% versus 61.5%, p<0.04; 9.9% versus 40.0%, p<0.02). Stool frequency and consistency reverted to normal immediately after treatment. Treatment shortened orocaecal and whole gut transit in all subjects on both doses. Treatment accelerated orocaecal (76 versus 51 minutes, p=0.007; 63 versus 47 minutes, p=0.07) and whole gut (38.2 versus 27.0 hours, p=0.05; 44.8 versus 24.0 hours, p<0.04) transit, and decreased the number of retained markers ingested 36 hours previously (4.8 versus 1.8, p=0.016; 7.0 versus 4.3, p=0.033). Gut sensitivity to distension and electrical stimulation, and anal manometry, were unchanged. Transient headache occurred in seven subjects on R093877 and one subject had mild elevation of liver aminotransferases which resolved on drug cessation.
Conclusions—R093877 is well tolerated by healthy subjects and has a marked and consistent effect on stool frequency and consistency, and upper gut and colonic transit. It does not affect visceral sensitivity or sphincter function. It holds promise for patients with large bowel symptoms or slow gut transit.
- idiopathic constipation
- enterokinetic agents
- intestinal transit
- cisapride
Statistics from Altmetric.com
Prokinetic agents such as cisapride and the motilin analogues have been used in the treatment of disordered small intestinal and colonic transit. They have been used acutely for disorders such as postoperative ileus, and long term for disorders such as idiopathic slow transit constipation or chronic idiopathic intestinal pseudo-obstruction.1-5 Although cisapride and the macrolides have major effects on gastric emptying, there are no systemically active compounds which specifically enhance colonic transit to a marked degree.6-8
R093877 is a benzofuran derivative, the first of a new class of compound. It is known from both in vitro and in vivo animal studies that this agent possesses gastrointestinal prokinetic activity in gastric, intestinal, and colonic smooth muscle (data on file, Janssen Research Foundation). Cisapride is thought to stimulate smooth muscle cells indirectly by facilitating postganglionic acetylcholine release in the myenteric plexus.9 ,10 The mechanism of action of R093877 is thought to be by facilitation of both cholinergic and non-adrenergic, non-cholinergic (NANC) neurotransmission.11
The primary aim of this study in healthy volunteers was to assess the effect of two doses of R093877 on gastrointestinal transit. Anorectal physiological studies were also performed to determine whether the drug may have some effect on visceral sensitivity and sphincter function. A third aim was to obtain further data on safety and tolerability.
Methods
SUBJECTS
Seventeen healthy volunteers with no previous ill health were studied. All had a normal bowel habit, that is a bowel frequency without straining between three times per day and three times per week, with normal consistency. Subjects were screened by physical examination, ECG, urinalysis, measurement of full blood count, liver function tests, and blood urea, creatinine, cholesterol, triglycerides, and glucose, and admitted to the study only if they were all within the normal range. Subjects also had to be within 20% of their ideal body weight for height. Subjects were on no regular medication and were only allowed up to 2 g per day paracetamol for symptoms they might develop during the study. Subjects were requested to abstain from alcohol during the study and were asked to follow the same diet during the two weeks of treatment.
All subjects gave their informed consent and ethical approval was granted by the Northwick Park and St Mark’s Ethics Committee.
DESIGN
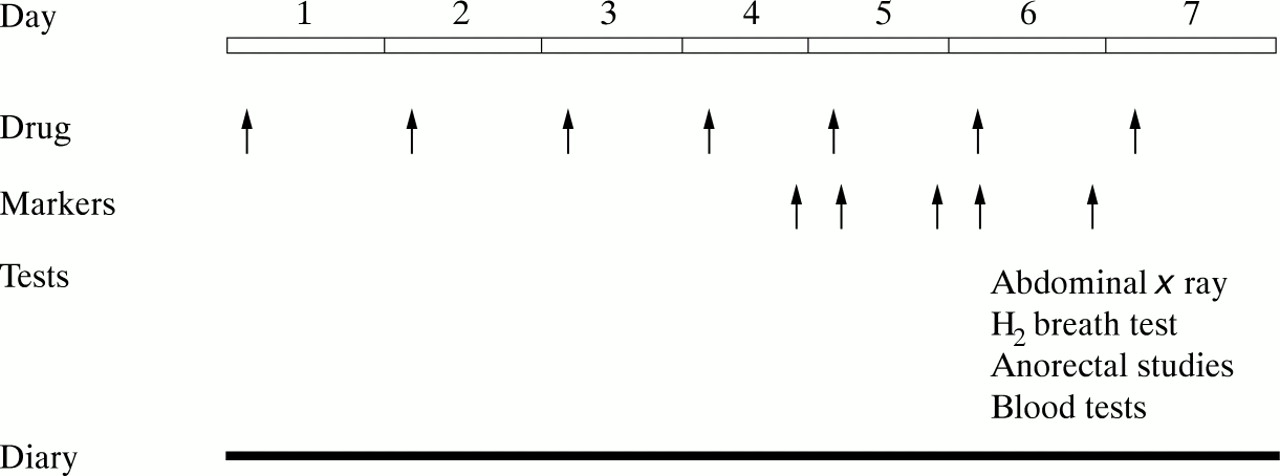
The study was a randomised, placebo controlled, crossover study, with each subject receiving placebo and one of two doses (1 mg or 2 mg per day) of R093877. The study was conducted over a five week period with each treatment period of one week being preceded and followed by a week when the patient was on no medication but continued to be monitored (fig 1).

Linear representation for study protocol during each treatment week.
Figure 1 shows the study protocol. During each of the two study weeks patients took either placebo or active medication each morning at 09.00 for seven days. Radio-opaque markers were taken twice per day for a total of five times: on the evening of day 4 and twice on days 5 and 6. Measurements were made at the end of the week to reflect steady state conditions. On the morning of the seventh day an abdominal radiograph was taken to determine transit, and blood tests were taken for safety data and to determine trough drug levels. Subjects were then given their medication, an orocaecal transit time was performed, anorectal physiological studies were performed, and finally a stool sample was collected for whole gut transit time determination.
BLOOD TESTING
For the purposes of safety analysis a blood sample was taken at enrolment to the study, on day 7 of each of the two treatment weeks, and at the end of the study. These samples were checked for full blood count, renal function, liver function, glucose, and lipid studies. Urinalysis was performed at the start and end of the study period.
To assess compliance a drug trough level was also measured on day 7 of each of the two treatment periods.
DIARY
Subjects were asked to keep a diary of their bowel function for the full five weeks of the study. This was designed to determine in the first week that subjects fulfilled the entry criteria with regard to bowel frequency, to compare the effects of placebo and active drug, and lastly to compare the weeks after the active drug and placebo to determine whether there was any carryover effect of the drug after ceasing medication.
The urge to defaecate, even if it did not result in a bowel action, was recorded. The date and time, and consistency (lumpy/hard/normal/soft/watery), of each bowel movement was recorded. Any episodes of abdominal pain (number, duration, and severity of episodes in any one day) were also recorded. The occurrence of any adverse effects and need for any concomitant medication were also documented.
OROCAECAL TRANSIT
Using the method of O’Brien et al,12orocaecal transit time (OCTT) was assessed using 20 g lactulose, a poorly absorbed carbohydrate, in 400 g of heated cream of chicken soup (Heinz); the subsequent rise in hydrogen in the exhaled breath was timed. Test samples were obtained every 10 minutes and analysed immediately (GMI Medical Instruments). The test was only conducted if the baseline breath hydrogen measurement was less than 15 parts per million. The orocaecal transit time was taken as the first reading of at least three consecutive samples which showed a breath hydrogen concentration of at least double the baseline.
WHOLE GUT TRANSIT TIME
Abdominal radiograph
Whole gut transit time was measured after ingestion of five different sets of radiologically distinguishable radio-opaque markers (P and A Mauch, Munchenstein, Switzerland) at 12 hourly intervals on days 4 to 6 of each treatment week starting at 20.00 on day 4, intake being timed to coincide with food. The total number of each of the sets of markers remaining in the bowel as seen on an abdominal xray taken at 09.00 on day 7 was determined by two observers independently, and then agreement reached on a final figure. A comparison was then made between the treatment and placebo arms for the number of markers remaining. This was only applied to the markers ingested 24 and 36 hours previously, as they were felt to be the most sensitive to changes in transit. Those taken earlier were felt likely to have passed in both treatment and placebo phases, and therefore to be insensitive to measuring an effect of the drug. Similarly the set of markers taken 12 hours previous to the x ray were felt likely to be still in the gut in both treatment arms; these were therefore also not compared.
Stool radiograph
In order to calculate the total intestinal transit time (TITT), the first stool on day 7 (or the earliest subsequent stool) was collected and subjected to x ray analysis. The number of each type of marker was counted and the transit time calculated, using all sets of ingested markers, by means of a well validated formula.13
ANORECTAL PHYSIOLOGICAL STUDIES
These studies were carried out on day 7 of each treatment week by the same investigator on each occasion using techniques validated in our laboratory.14 ,15 Anal sphincter manometry was performed using a closed water filled microballoon station pull through method to assess maximal resting pressure which is predominantly a reflection of internal anal sphincter tone. Assessment of rectal sensation was performed by both mucosal sensitivity to electric current using a bipolar ring electrode (Dantec, Denmark) and by balloon distension (Sainsbury, UK).
STATISTICAL ANALYSIS
The subjects in each of the two dose groups were compared for age, smoking and alcohol intake, height, weight, blood pressure, and pulse rate using the Mann-Whitney U test (for continuous and ordinal variables) and Fisher’s exact test (for nominal variables). Data from the diaries, whole gut transit studies (both abdominal and stoolx ray studies), orocaecal transit studies, and anorectal physiological data were all compared using the paired ttest if the data were normally distributed, or the Wilcoxon rank tests for non-parametric data. All tests were two tailed and a p value of less than 0.05 was regarded as reflecting a significant difference between measured parameters.
Results
One subject left the study during the first treatment period, due to abdominal pain. Subsequent unblinding of the study revealed that he had been on placebo only. His data were included only in the analysis of adverse events and not in any other results. The remaining 16 subjects all completed the study and form the basis of the presented results.
Eight subjects completed the study, ingesting 1 mg R093877 each day for a week and placebo each day for a week. A separate eight subjects completed an identical study with 2 mg R093877.
BLOOD TESTS—COMPLIANCE
Active drug was found in the serum of all subjects after the active treatment period except in one subject in the 2 mg group. The results for diary data are presented for all 16 subjects. The results for orocaecal transit time and whole gut transit time are presented in two ways: including all 16 subjects, and 15 subjects excluding the subject in whom no active drug was found in the blood tests.
When comparing the two groups of eight subjects plasma concentrations of the drug were significantly higher (mean 2.40 (SEM 1.26) ng/ml) in the 2 mg group than in the 1 mg group (1.40 (0.22) ng/ml) (p<0.05). The mean value in the 2 mg group after exclusion of the subject with no drug detected was 2.74 (0.88) ng/ml.
DIARY DATA
Comparisons of each dose were performed within each group of eight subjects (see table 1). All the figures quoted are mean data. Treatment with 1 mg R093877 significantly increased the frequency of urge to defaecate, the proportion of days on which a stool was passed, and the number of stools passed. Treatment with 2 mg R093877 did not increase the frequency of urge to defaecate or the proportion of days on which a stool was passed, but did increase the number of stools passed although this did not reach statistical significance. Both doses significantly increased the proportion of stools which were loose or watery.
Effect of R093877 on stool frequency and consistency
Comparison of the week after treatment with either placebo or active drug gives an indication of any carryover effect of the treatment. Table 2 illustrates that there is no effect on the frequency of defaecation or the number of stools passed in the post-treatment week when comparing placebo with R093877 at either the 1 or 2 mg doses.
Comparison of bowel frequency and stool consistency in the week after active drug and placebo were given
OROCAECAL TRANSIT
R093877 significantly shortened orocaecal transit time in the 1 mg group (51 versus 76 minutes, 1 mg versus placebo, p=0.007). In the 2 mg group orocaecal transit time was shortened by the active drug (46 versus 61 minutes (including non-complier—eight subjects versus placebo, p=0.08); 47 versus 63 minutes (excluding non-complier—seven subjects versus placebo, p=0.07)), although this did not reach statistical significance.
WHOLE GUT TRANSIT
Abdominal x ray—retained markers
Table 3 shows that R093877 1 mg significantly decreased the number of markers retained for the markers ingested 24 hours previously (5.3 versus 6.1, p=0.05) and 36 hours previously (1.8 versus 4.8, p=0.016). R093877 2 mg also significantly decreased the number of markers retained for the markers ingested 24 hours previously (6.1 versus 7.9, p=0.048) and 36 hours previously (4.3 versus 7.0, p=0.033) (fig2).
Mean number of retained radio-opaque markers after active drug and placebo for markers ingested at various times before the radiograph

{kind=link}
{kind=link}
Whole gut transit time for each subject on placebo and active drug. Data shown for all 15 compliant subjects on both doses of active drug.
Stool x ray—transit time
In all 16 subjects except one the active drug shortened the whole gut transit time. The only subject in whom the transit time was not shortened was the only subject in whom no active drug was detectable in the serum.
R093877 1 mg significantly reduced the total intestinal transit time (27.0 versus 38.2 hours, 1 mg versus placebo, p=0.05).
R093877 2 mg also reduced the total intestinal transit time. When all eight subjects were considered this reduction did not reach statistical significance (31.1 versus 44.7 hours, 2 mg versus placebo, p=0.10). When the non-complying subject was excluded from this calculation the 2 mg dose significantly reduced the whole gut transit time in these seven subjects (24.0 versus 44.8 hours, 2 mg versus placebo, p<0.04).
ANORECTAL PHYSIOLOGICAL STUDIES
There was no significant change in the maximum resting anal sphincter pressure, rectal distension thresholds to balloon distension, or anal and rectal threshold to electrical stimulation by either dose of R093877 (table 4).
Gut sensitivity and sphincter function on active drug and placebo
BLOOD TESTS—SAFETY ANALYSIS
Table 5 shows the incidence of adverse effects during the study. The only side effect which occurred significantly more frequently in the treated group was headache. Median onset of headache was one hour after ingestion of R093877 and was more frequent in the 2 mg group. Subjects only reported headache on the first two days of ingesting R093877; the symptom did not occur with subsequent doses. The headache was described as of moderate severity in eight out of the 10 reported episodes; it occurred in seven subjects on active drug and resolved within two hours spontaneously or with use of paracetamol. Previously recorded side effects with R093877, such as abdominal pain and flatulence, were not observed with increased frequency in the active treatment group. In the higher dose group one patient vomited one hour after ingestion of the first dose of drug, but this did not occur with any subsequent doses.
Side effects with active treatment and placebo
The only biochemical abnormality noted after R093877 treatment was a mild and transient elevation of serum alanine aminotransferase (41 IU/l) and serum aspartate aminotransferase (59 IU/l) (normal range for both: 5–40 IU/l) in one subject. The other liver function tests were all normal and the transaminases returned to normal by the end of the study. No disturbances of any haematological parameters were noted.
Discussion
R093877 is a benzofuran derivative with gastrointestinal prokinetic activity. Animal in vitro experiments have shown facilitation of cholinergic and excitatory non-adrenergic, non-cholinergic (NANC) neurotransmission. It is the first compound known to enhance NANC transmission in colonic preparations of the guinea pig. Since cholinergic as well as NANC neurones are known to play an important part in the physiological regulation of colonic motility, it is likely that constipation will be favourably influenced by compounds facilitating NANC excitatory neurotransmission.16 In vivo and in vitro studies have shown the compound to facilitate gastric, small intestinal, and colonic motility.11 ,17 ,18
The two different dosage groups were similar in their diary and measured physiological parameters during the placebo weeks. We did not find a major difference in the effect between the two doses studied. Both doses produced a significant shortening of transit times, although the 1 mg dose had a greater effect on bowel habit. Previous studies involving multiple dosage regimes have shown a greater effect with 2 mg compared with a 1 mg or 0.5 mg dose (data on file, Janssen Research Foundation). Further studies in patients will be required to determine whether this dose effect similarity remains true.
R093877 increased both the urge to defaecate and actual stool output. In addition to the increased bowel frequency there was also a shift towards the production of a looser stool. This rapid alteration of bowel habit is in contrast to that seen with cisapride which produces its effect on the bowel after several weeks.19 ,20
With the 2 mg dose there was no change in bowel frequency despite shorter gut transit times. Bowel frequency is under voluntary control and is therefore less predictably affected by a compound which affects transit. The effect may differ if the compound is effective in patients, as opposed to healthy individuals with a normal frequency.
Orocaecal transit time was also shortened by R093877, although this technique does not allow the distinction to be made between hastened gastric and small intestinal transit.
Mean total colonic transit time, estimated by marker studies, in healthy volunteers is approximately 35 hours12 ,21 ,22 and so calculations involving markers taken up to 60 hours prior to the abdominal x ray may mask changes in transit since those early ingested markers will often be cleared by the time of the radiograph. Pharmacokinetic studies (data on file, Janssen Research Foundation) have shown that peak plasma concentrations of R093877 are achieved within three hours of ingestion and hence maximal effect occurs soon after ingestion. For these reasons calculation of total colonic transit times was not undertaken. The more sensitive measure of the clearance of markers ingested at specific times was therefore used. However additional data were derived from measuring the transit time using a single stool and several sets of markers.
Cisapride has been reported to alter rectal distension sensory thresholds and this has been postulated to relate at least in part to its effect on increased bowel frequency.23 ,24 In contrast R093877 had no specific effect on rectal distension thresholds or anorectal electrosensory thresholds, despite showing a significant effect on increasing bowel frequency. Results from this study indicate that R093877 has no obvious effect on sensory or sphincter function.
There was a dose dependent increase in plasma levels of R093877, confirming the pharmacokinetic properties of the drug shown in a prior phase I study (data on file, Janssen Research Foundation).
The only patient who withdrew due to adverse side effects was on placebo. With the exception of headaches neither dose caused more adverse clinical effects than placebo. The headaches typically occurred within an hour of drug ingestion, were of moderate severity, and usually resolved after the first two doses. Cramping abdominal pain, flatulence, and nausea which have been associated with R093877 treatment (data on file, Janssen Research Foundation) were not observed more frequently in the active treatment group compared with placebo.
Blood and urine analysis identified only one significant abnormality associated with R093877. This was a minor isolated elevation of liver aminotransferases in one patient which reverted to normal at the end of the study. In previous studies in which 115 healthy volunteers were treated either orally, subcutaneously, or intravenously with different doses of R093877 (dose range 0.06 to 5 mg), an increase in liver enzymes was only observed in one volunteer after administration of 1 mg of R093877, given subcutaneously (data on file, Janssen Research Foundation).
In conclusion, in healthy volunteers R093877 exhibits a notable and consistent effect on colonic and upper gut transit, holding promise of a new class of treatment for chronic constipation. Further studies of efficacy and dose in patients with constipation and other motility disorders are awaited.
Acknowledgments
This research was supported by Janssen Research Foundation, Saunderton, High Wycombe, Buckinghamshire HP14 4HJ, UK.