Article Text

Abstract
Background—It is believed that severe portal hypertensive gastropathy probably accounts for most non-variceal bleeding episodes in patients with cirrhosis. Gastric antral vascular ectasia (GAVE) also occurs in these patients. It is not clear whether it is a variant of portal hypertensive gastropathy or a distinct condition.
Patient—A patient, a 66 year od woman, with cirrhosis initially diagnosed as having portal hypertensive gastropathy and subsequently classified as GAVE is described. She required transfusion with a total of 130 units of packed red cells for gastrointestinal blood loss.
Results—The bleeding did not respond to portal decompression with TIPS or beta blockers. Following treatment with oral tranexamic acid she has not required further blood transfusion over a period of 30 months.
Conclusion—Tranexamic acid may be a useful treatment for refractory bleeding due to gastric antral vascular ectasia in patients with cirrhosis.
- gastric antral vascular ectasia
- cirrhosis
- tranexamic acid
Statistics from Altmetric.com
Patients with portal hypertension frequently develop gastric abnormalities. These may be focal, for example gastric varices, or diffuse as in portal hypertensive gastropathy.1 ,2 Portal hypertensive gastropathy is mild in most cases but may be severe and associated with gastrointestinal haemorrhage and iron deficiency anaemia. The severe form develops in about 10% of patients and is characterised endoscopically by a granular appearance of the mucosa and the presence of cherry red spots.3 ,4 The pathogenesis of the condition is controversial with studies suggesting hyperaemia or hypoperfusion of the gastric mucosa.5-7 Most patients with severe gastropathy bleed and develop iron deficiency anaemia.3 Recently attempts have been made to distinguish severe portal hypertensive gastropathy from gastric antral vascular ectasia (GAVE) or “watermelon stomach” in patients with cirrhosis.8 It is not clear whether GAVE is a variant of portal hypertensive gastropathy or a distinct condition. The optimal treatment for this condition in the presence of portal hypertension is not established.
Case report
A 66 year old woman presented in late 1992 with iron deficiency anaemia and abnormal liver function tests. She had a long history of bronchial asthma treated with inhaled bronchodilators. On examination she had hepatosplenomegaly but no jaundice, ascites, or encephalopathy. Haemoglobin was 9.2 g/dl (normal 11.5–16.5) with a hypochromic, microcytic pattern. Serum albumin was 33 g/l (normal 35–50), γ glutamyl transferase 173 IU/l (normal less than 50), and aspartate aminotransferase 54 IU/l (normal 5–40). Serum bilirubin and alkaline phosphatase were normal. Prothrombin time was 16 seconds with an international normalised ratio of 1.4. Antismooth muscle and antimitochondrial antibody tests were positive. Liver biopsy showed inactive micronodular cirrhosis. Gastroscopy showed severe oesophagitis, no varices, and “gastritis”. Diverticular disease was seen on barium enema. The portal vein was patent on ultrasound examination. Treatment with omeprazole was commenced. In April 1993 she was readmitted with dyspnoea and a haemoglobin of 4.7 g/l. Gastroscopy showed “congestive gastropathy” and grade 1 oesophageal varices but no oesophagitis. She was transfused with 5 units of packed red cells (month 1 in fig 1). Sucralfate was added to omeprazole. Over the next two years she was admitted virtually every month with symptomatic anaemia requiring transfusion (fig 1). A total of 130 units of packed red blood cells, 3 units of fresh frozen plasma, and 4 units of human serum albumin were required during this period. In the latter stages the development of multiple antibodies severely compromised our ability to find compatible blood for this patient. Multiple gastroscopies showed “congestive gastropathy” with fresh blood on the antral mucosa.
{kind=link}
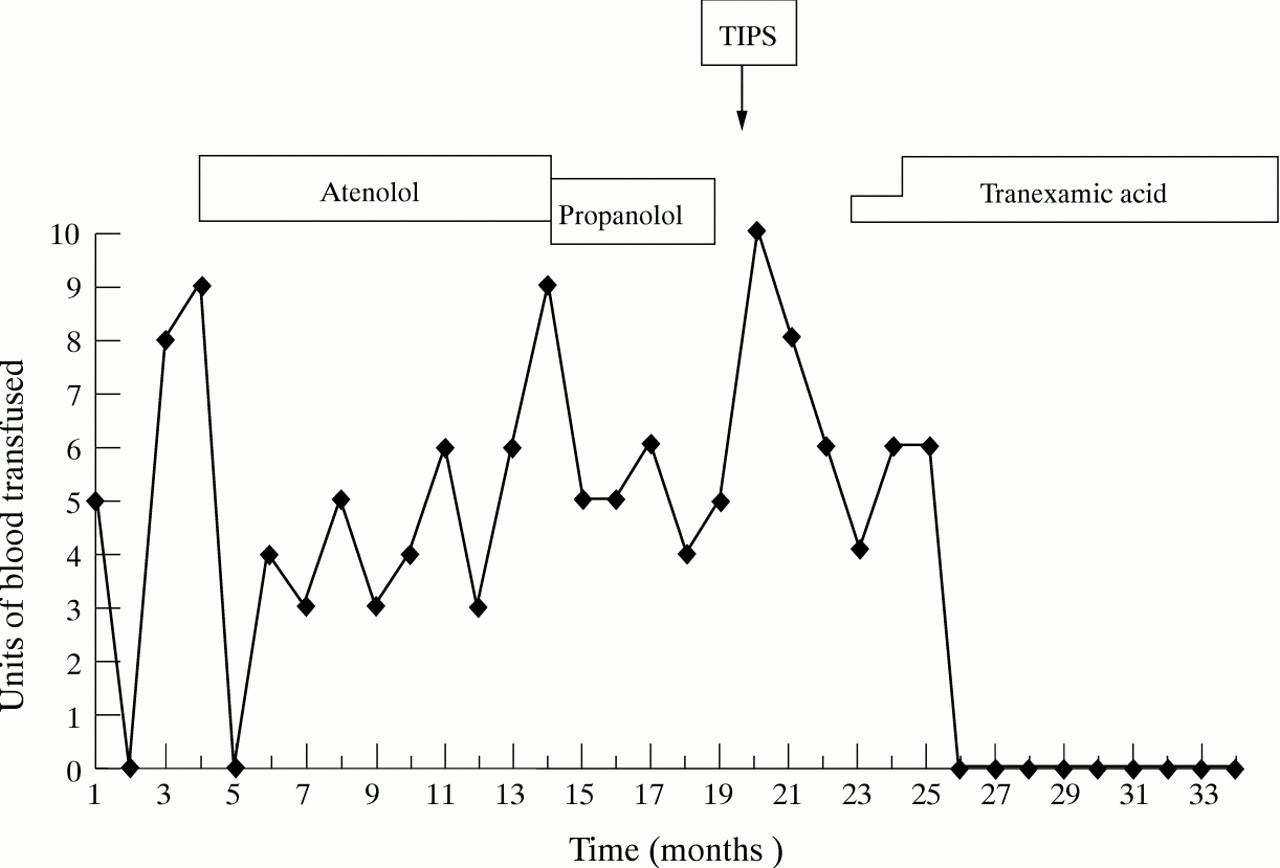
Monthly blood transfusion requirements and treatment received for blood loss from gastric antral vascular ectasia. At the time of writing the patient has not required blood transfusion for 19 months. TIPS, transjugular intrahepatic portosystemic shunt.
In July 1993 the cardioselective β blocker atenolol was started at a dose of 50 mg daily and subsequently increased to 100 mg daily. A cardioselective β blocker was chosen because of a history of asthma. She continued to bleed. Liver transplantation was considered in March 1994 but rejected because of her age and pulmonary status. The atenolol was discontinued and low dose propranolol, 10 mg three times daily, was started in May 1994. She continued to bleed and transfusion became increasingly difficult because of multiple antibodies. A transjugular intrahepatic portosystemic shunt (TIPS) procedure was performed in September 1994. An 8 cm long, 10 mm diameter Wallstent was inserted and the gradient between the portal vein and the right atrium at the end of the procedure was 12 mm Hg. Antibiotic prophylaxis with flucloxacillin and cephradine was given intravenously for 24 hours to cover the procedure. Two weeks later she was admitted in coma with a Gram negative bacillus on blood culture. The source of this infection was probably the urinary tract and the TIPS was not believed to be infected. The hepatic encephalopathy resolved with intravenous antibiotics. In November 1994 Doppler ultrasound suggested shunt malfunction. A stricture at the hepatic vein end of the shunt was dilated with a final portal vein-right atrial gradient of 10 mm Hg. Repeat antibiotic prophylaxis was given to cover this procedure. Despite this she continued to require regular transfusion. Repeat barium enema and colonoscopy showed diverticular disease. In January 1995 tranexamic acid was commenced at a dose of 500 mg three times daily and increased to 1 g three times daily in March. Since April 1995 her haemoglobin has been stable at between 10 and 12 g/dl and as of November 1996 she has required no further blood transfusion. At one point her oral iron supplements were stopped for two months and her haemoglobin dropped to 9 g/dl. This suggests that the bleeding diminished but did not completely cease on treatment. Repeat gastroscopy in November 1996 showed small oesophageal varices but no gastric varices. Multiple red spots were seen in the gastric antrum with sparing of the fundus. Biopsy of the gastric antrum showed the ectatic mucosal capillaries with fibrin thrombi, fibrohyalinosis, and fibromuscular hyperplasia typical of GAVE.
Discussion
Gastric antral vascular ectasia is characterised by the presence of red spots or streaks in the antral mucosa, vascular ectasia on pathological examination, and gastrointestinal blood loss.8 The findings of spindle cell proliferation and fibrohyalinosis on biopsy are claimed to be relatively specific.8 In contrast, in portal hypertensive gastropathy the mucosal changes are more notable in the fundus than in the antrum.2 ,9 Diffuse red spots in the mucosa may also occur in actively drinking alcoholic patients, with or without portal hypertension. These may represent superficial mucosal haemorrhages and probably are distinct from GAVE or portal hypertensive gastropathy.10 Quintero et al described 11 cirrhotic patients bleeding from gastric red spots.4Biopsy revealed diffuse capillary ectasia. They found hypergastrinaemia and low serum levels of pepsinogen in patients with this condition and concluded that it also represented a distinct entity.4 In contrast the patients described by Payen et al with GAVE and portal hypertension had lower serum gastrin levels than controls or cirrhotics with portal hypertensive gastro- pathy.8 It is not clear whether these various entities are distinct conditions or represent part of the spectrum of portal hypertensive gastropathy. The fact that most patients with GAVE (70%) are not cirrhotic would suggest that it is a different conditon.11 Many patients with GAVE are middle aged women with various autoimmune conditions. Portal hypertension may be an incidental or aggravating factor. An additional point of differentiation between portal hypertensive gastropathy and GAVE may be the response to treatment. Portal hypertensive gastropathy usually responds to β blockade or portal decompression therapy.12 ,13 Spahr et alfound that rebleeding recurred in 6/7 patients with GAVE and portal hypertension despite treatment with β blockade (n=7), TIPS (n=6), or end to side portacaval shunt (n=1).14 In our patient, β blockade and portal decompression with a TIPS shunt were also ineffective. In contrast treatment with the antifibrinolytic agent tranexamic acid dramatically reduced the blood transfusion requirement although the endoscopic appearances remained unchanged.
Tranexamic acid is an antifibrinolytic agent used in the treatment of a variety of bleeding conditions.15 A meta-analysis of six randomised double blind placebo controlled trials in patients with upper gastrointestinal bleeding reported a 20–30% reduction in rebleeding, a 30–40% reduction in the need for surgery, and a 40% reduction in mortality.16 There is one previous report of benefit with tranexamic acid in a patient with GAVE.17That was in a 49 year old woman with alcoholic liver disease, no varices, and bleeding from haemorrhagic antral gastritis. Gastric biopsy showed dilated capillaries with microthrombi. The authors state that the haemorrhage was reduced after treatment but no details are given. Four other patients in that report were treated with blood transfusions, surgery, or endoscopic laser therapy with variable results.17 Treatment with tranexamic acid is not without potential hazard. In a controlled trial of patients with subarachnoid haemorrhage rebleeding was reduced (24% versus 9%) but there was an increased incidence of ischaemic complications (24% versus 15%).18 Pulmonary embolism and central venous stasis retinopathy have also been described following its use.19 ,20 In our patient further blood transfusion was becoming increasingly difficult because of antibodies. The option of partial gastrectomy with its attendant risks in an elderly cirrhotic patient was being considered. In this context we felt that the risks of thrombosis were acceptable. It is interesting that there was a delay before the transfusion requirement fell to zero. The reason for this is unclear but it suggests that a trial of a few months therapy with adequate dosage may be required.
A number of treatments for persistent bleeding due to GAVE have been suggested. Antrectomy offers a definitive cure but is a high risk procedure in patients with this condition who are often elderly and have coexistent liver disease. There are isolated case reports of response to treatment with corticosteroids or oestrogen-progesterone preparations.21 ,22 Successful treatment with local laser treatment to affected areas of the stomach has also been described. In a series of eight patients with GAVE, five responded to neodymium:YAG laser photocoagulation.23 Three to four treatment sessions were required to obliterate the abnormal vascular pattern; the only side effect noted was minor ulceration. Other authors have reported success with the use of the argon laser.24
In view of the dramatic effects we observed in this patient, we suggest that tranexamic acid could be considered as a treatment for recurrent severe haemorrhage from GAVE in cirrhotic patients. Ideally a controlled trial should be performed to establish its value in this situation. Because of the relative rarity of this condition such a trial would require multicentre collaboration.