Article Text

Abstract
Background—Vitamin C may be protective against gastric cancer though infection withHelicobacter pylori is associated with a reduction in intragastric concentrations of vitamin C.
Aims—To examine the effects ofH pylori infection, gastric juice pH, the severity and extent of gastric inflammation, and CagA antibody status of the individual on gastric juice and mucosal vitamin C concentrations.
Patients—One hundred and fifteen patients undergoing routine gastroscopy for investigation of dyspepsia.
Methods—High performance liquid chromatography was used to determine vitamin C concentrations. CagA antibody was detected by western blot analysis.
Results—Gastric juice ascorbic acid concentration was significantly lower in patients infected withH pylori compared with those uninfected (19.3 μmol/l (interquartile range (IQR) 10.7–44.5) versus 66.9 μmol/l (IQR 24.4–94.2), p=0.003). The reduction in gastric juice ascorbic acid concentration was inversely related to the severity of gastritis (p=0.01). CagA positive patients had significantly lower gastric juice ascorbic acid concentrations than CagA negative ones (14.8 μmol/l (IQR 7.9–52.2) versus 39 μmol/l (IQR 19.9–142.2), p=0.05). Decreased gastric juice dehydroascorbic acid concentrations were observed in patients with gastric atrophy and intestinal metaplasia. Mucosal ascorbic acid concentrations were also significantly lower in infected patients than uninfected patients (p=0.04).
Conclusions—The reduction in gastric vitamin C concentrations is related to gastric juice pH, the severity and extent of gastritis, the presence of H pylori, and the CagA antibody status of the individual. These findings may have implications in H pyloriassociated carcinogenesis.
- ascorbic acid
- Helicobacter pylori
- gastric juice
- gastric mucosa
- premalignancy
Statistics from Altmetric.com
There is compelling evidence suggesting an inverse relation between vitamin C intake and gastric cancer risk.1 2Vitamin C is an important antioxidant and can react with nitrite, preventing the formation of N-nitroso compounds.3 4 During this process, ascorbic acid, the reduced form of vitamin C, is oxidised to dehydroascorbic acid (DHA). Though DHA differs functionally from ascorbic acid,5 it alone, or in combination with vitamin B12, can specifically inhibit tumour cell mitotic activity without affecting normal cell growth.6-8 Thus, both ascorbic acid and DHA may have protective effects on gastric carcinogenesis.
Ascorbic acid is actively secreted into the gastric lumen9-11 and the concentrations in gastric juice and mucosa may be particularly important for effectively converting nitrites and nitrite derived mutagens. Helicobacter pylori infection, the main cause of chronic gastritis, increases gastric cancer risk.12-14 However, its precise role in gastric carcinogenesis is as yet unknown. It has been suggested that ascorbic acid concentration is decreased in H pylori infected patients and returns to normal afterH pylori eradication.15-18This suggests that patients infected with H pylori lack the protection of gastric juice ascorbic acid. However, the importance of DHA concentrations in the stomach has not been adequately addressed in previous studies.9 11 17 18
CagA seropositivity has been related to H pylori associated gastric cancer risk.19 Patients infected with cagA+H pylori strains have higher degrees of gastric inflammation and enhanced expression of proinflammatory cytokines such as interleukin 1 (IL-1) and IL-8.20-22Previous studies have shown that gastric juice vitamin C concentration is related to the severity of gastric inflammation. However, whether infection with cagA+ strains contributes to the reduction in gastric vitamin C concentrations is unknown.
We have therefore examined the effect of H pylori infection, gastric juice pH, the severity and extent of gastric inflammation, and CagA antibody status of the individual on gastric juice and mucosal vitamin C concentrations.
Materials and methods
One hundred and fifteen consecutive patients attending for upper gastrointestinal endoscopy were studied. Patients with serious underlying diseases, gastrointestinal bleeding, previous gastric surgery, or those known to have taken non-steroidal anti-inflammatory agents, antibiotics, bismuth preparations, proton pump inhibitors, or vitamin supplements within a month of endoscopy were excluded. The study was approved by the ethics committee and informed consent was obtained from all patients. Ten ml of blood was taken from each patient before endoscopy. Immediately on entry of the endoscope into the stomach, gastric juice was collected through a trap inserted into the suction line, taking care to avoid contamination with blood. Six biopsy specimens were obtained from within 2 cm of the pylorus. One was used for H pylori culture, one for the urease test, two for histological assessment, and two for vitamin C measurement. A further two biopsy specimens were taken from the corpus for histological assessment. H pyloriinfection was assessed by histology, culture, rapid urease test, and serology. Patients were considered positive if two or more of these tests were positive. CagA seropositivity was determined by western blot analysis using a previously reported technique,23 with the following modifications. A whole cell preparation of thecagA+ strain H pylori NCTC 11637 was used. Approximately 25 μg of total protein (determined by a modified Lowry technique) was loaded in each lane. Patient sera were diluted and tested at dilutions of 1/25 and 1/50. Fifty four patients were tested for CagA antibody status: 23 were CagA positive, seven were CagA negative, and 24 were withoutH pylori infection.
histopathology
Two antral and two corpus biopsy specimens were fixed in formalin, processed routinely, and embedded in paraffin wax. The 4 μm sections were cut from each specimen and then stained with haematoxylin and eosin, a combined Alcian blue/periodic acid-Schiff stain, and a modified Giemsa method. All sections were assessed “blind” by the same histopathologist according to the Sydney System.24The degree of chronic inflammatory cell and polymorphonuclear leucocyte infiltration was graded for each variable on a four point scale from 0 (absent) to 3 (severe). The scores from both antrum and body were added to give a total “gastritis score” for each patient. Similarly, figures from gastric antrum were calculated to give a total “antral gastritis score” for each patient.25
vitamin c measurement
The concentrations of ascorbic acid and total vitamin C were measured in gastric juice and gastric antral mucosal biopsy specimens using high performance liquid chromatography (HPLC).26 The concentration of DHA was determined by subtraction of ascorbic acid from total vitamin C. Immediately after sampling, gastric juice pH was measured. The gastric juice was then mixed with an equal volume of 2% (wt/vol) metaphosphoric acid, containing 0.5% (wt/vol) sulphamic acid, and was kept at −70°C until analysis. Two antral biopsy specimens were frozen in liquid nitrogen and stored at −70°C prior to analysis. The specimens were thawed, weighed, and homogenised in 1 ml of 2% metaphosphoric acid. Before analysis, both gastric juice and gastric mucosal homogenates were centrifuged and the supernatants were divided into two aliquots. To determine total vitamin C content, the supernatant was incubated with dithiothreitol (6 mg/ml) at 45°C for 120 minutes prior to analysis. The HPLC system was equipped with an HPLC pump (Model 351, ACS, UK) and an ultraviolet detector (Cecil Instruments, UK) for gastric juice vitamin C measurement and an electrochemical detector (LCA-15 with electrochemical cell and glass carbon electrode, EDT, UK) for gastric mucosal vitamin C measurement. A Hypersil, 5 μm, ODS, 100×4.6 mm HPLC analysis column (Phenomenex Ltd, UK) was used. The mobile phase consisted of 0.1 M sodium acetate/acetonitrile (85/15 vol/vol) containing 10 mM octylamine. The final pH was adjusted to 4.3 with glacial acetic acid. The flow rate was 2 ml/min and the retention time of ascorbic acid was three minutes. Gastric juice vitamin C concentrations were measured in 62 patients, gastric mucosal vitamin C concentrations in 87 patients, and both gastric juice and mucosal vitamin C concentrations in 34 patients. The intra-assay and interassay coefficients of variation in both gastric juice and mucosal vitamin C measurements were <5% and <10%, respectively.
statistical analysis
Data were analysed using SPSS software (Version 6.1) and are presented as group medians with interquartile ranges (IQR). Differences in non-parametric data were analysed using Mann-Whitney U, Kruskal-Wallis one way analysis of variance (ANOVA), and Cuzick’s trend tests.27 The correlations between the severity of gastritis, gastric juice pH, and vitamin C concentrations were tested using Spearman correlation coefficient. Values of p<0.05 were considered significant in all analyses.
Results
gastric juice vitamin c
Gastric juice vitamin C concentration was measured in 62 patients (36 males, 26 females) with mean age 55.4 (range 19–87) years. The median gastric juice ascorbic acid and DHA concentrations were 34.3 μmol/l (IQR 13.8–79) and 13.3 μmol/l (IQR 7.4–30.7), respectively. Gastric juice ascorbic acid concentration was significantly lower in 38 patients infected with H pylori compared with those without H pylori infection (19.3 μmol/l (IQR 10.7–44.5) versus 66.9 μmol/l (IQR 24.4–94.2), p=0.003). However, there was no significant difference in gastric juice DHA concentration between patients with and without H pylori infection (11.6 μmol/l (IQR 5.8–28.9) versus 23 μmol/l (IQR 9–40.2)) (fig 1).
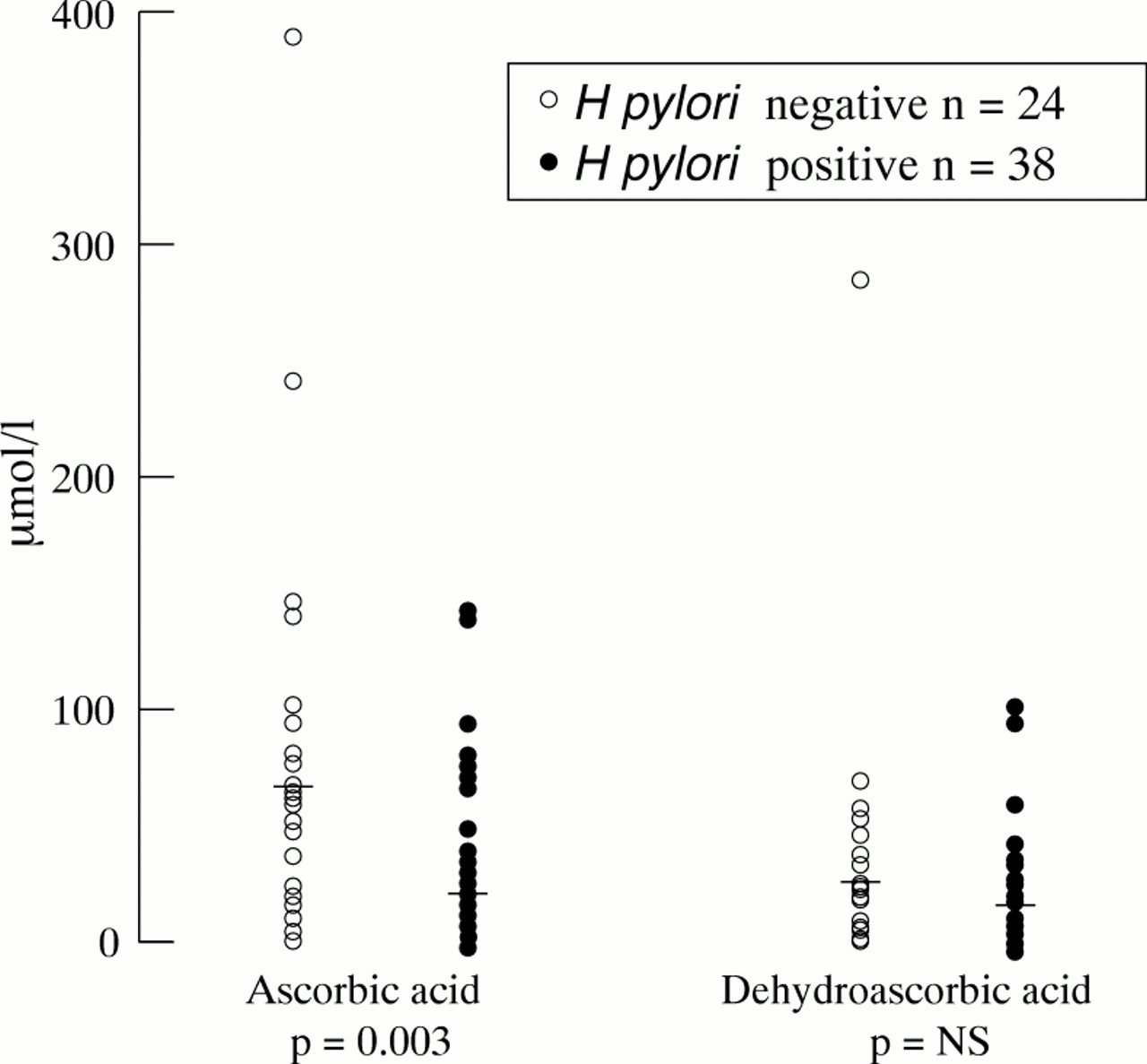
H pylori infection related to gastric juice ascorbic acid and DHA concentrations (Mann-Whitney U test).
When related to topography of gastritis, gastric juice ascorbic acid concentrations were decreased in a stepwise fashion as the extent of inflammation progressed from normal to diffuse antral gastritis and finally to pangastritis (table 1). The total gastritis score was also negatively correlated with gastric juice ascorbic acid concentration (Spearman correlation coefficient, r=−0.3, p=0.01). However, gastric juice DHA concentrations were associated with neither the extent nor the severity of gastritis. These findings indicate that both extent and severity of gastritis are important in determination of gastric juice ascorbic acid, but not of DHA concentration.
Extent of gastritis related to gastric juice vitamin C concentration
Atrophy and intestinal metaplasia were also associated with a significant reduction in gastric juice vitamin C concentration. As the histological changes progressed from normal to chronic gastritis, atrophy, and finally to intestinal metaplasia, there was a stepwise decrease both in gastric juice ascorbic acid and DHA concentrations (table 2). No attempt was made to subtype intestinal metaplasia due to the relatively small number of intestinal metaplasia samples in the study. Gastric juice pH values were inversely associated with gastric juice ascorbic acid concentrations (Spearman correlation coefficient,r=−0.4, p=0.001). Patients (n=23) with gastric juice pH⩾4 had significantly lower gastric juice ascorbic acid concentrations compared with those with gastric juice pH<4 (p<0.003). This suggests that gastric juice pH is another important determinant of gastric juice ascorbic acid concentrations.
Gastric histology related to gastric juice vitamin C concentration
gastric antral mucosal vitamin c
Gastric antral mucosal vitamin C concentration was measured in 87 patients (51 males, 36 females) with mean age of 56.2 (range 19–96) years. Median gastric mucosal ascorbic acid and DHA concentrations were 397 μg/g wet weight (IQR 263–764) and 46.7 μg/g wet weight (IQR 5.4–178), respectively. Ascorbic acid concentration in antral mucosa was lower in H pylori positive patients (352 μg/g wet weight (IQR 224–684)) than in H pylori negative patients (476 μg/g wet weight (IQR 322–827)) (p=0.04). However, there was no statistical difference in gastric antral mucosal DHA concentration between patients with and withoutH pylori infection (43.0 μg/g wet weight (IQR 4.7–178) versus 67.2 μg/g wet weight (IQR 9.4–169, NS). No significant association was found between antral mucosal vitamin C concentration and the severity of antral gastritis (the antral gastritis score) or with the presence of atrophy or intestinal metaplasia.
the relation between h pyloricaga seropositivity and gastric vitamin c concentrations
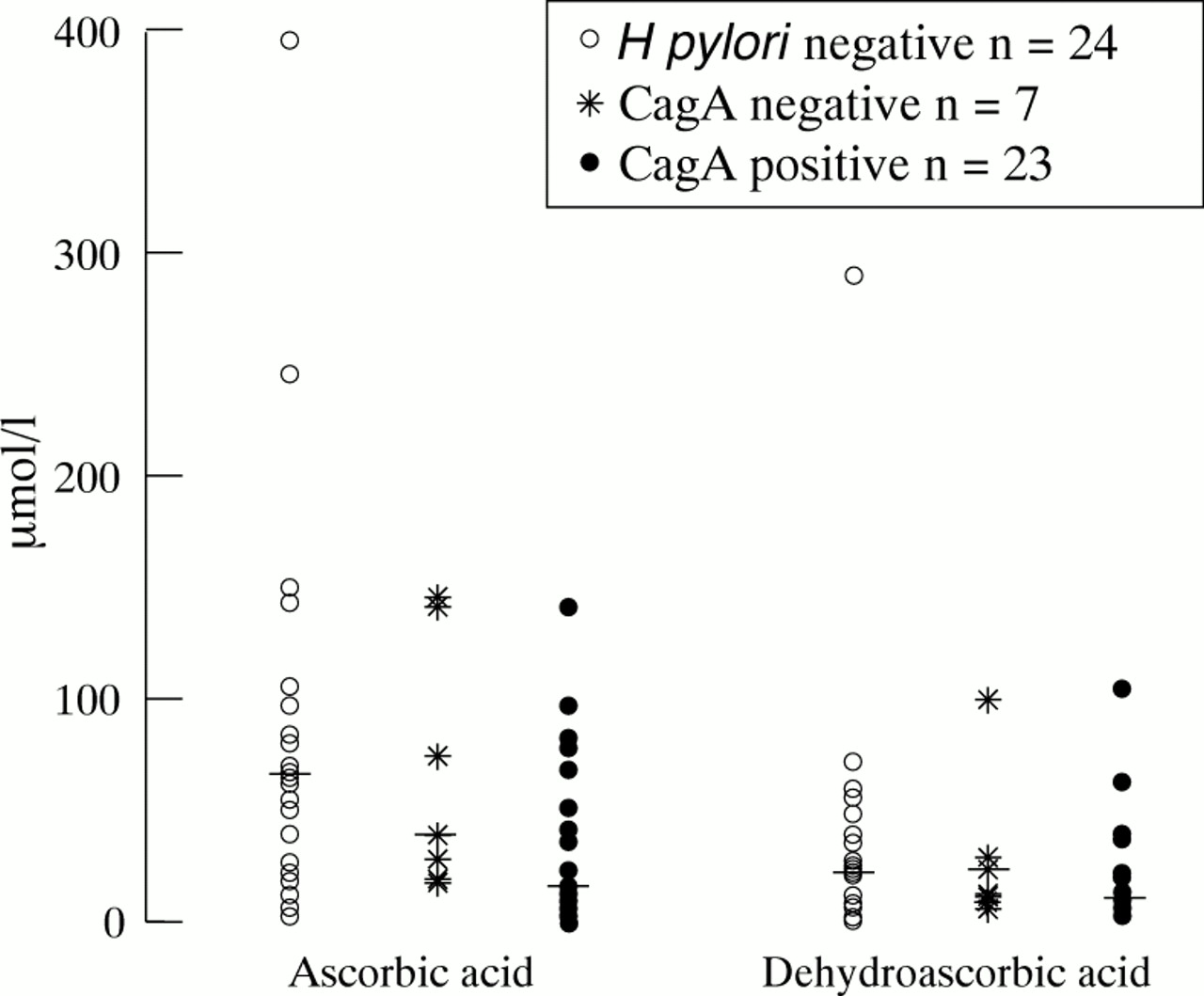
Gastric juice ascorbic acid concentrations were significantly lower in CagA positive patients (14.8 μmol/l (IQR 7.9–52.2)), compared with those who were CagA negative (39.0 μmol/l (IQR 19.9–142)) and to those without H pyloriinfection (66.9 μmol/l (IQR 24.4–94.2)) (fig 2). There was no significant association between gastric juice DHA concentrations and CagA status of the individual. Further analysis suggests that CagA positive patients had a significantly higher gastritis score (p=0.03) and more gastric atrophy/intestinal metaplasia compared with CagA negative patients (p=0.04). However, there was no significant association between CagA seropositivity and antral mucosal vitamin C concentrations.

{kind=link}
{kind=link}
CagA antibody status related to gastric juice ascorbic acid concentrations. (Mann-Whitney U test and Kruskal-Wallis one way ANOVA).
Discussion
Ascorbic acid is actively secreted into the normal stomach leading to gastric juice concentrations greater than those in plasma. This secretion is impaired in the presence of chronic gastritis.26 28 Gastric juice ascorbic acid concentrations in patients with H pyloriassociated gastritis are reduced significantly, eventually leading to a loss of both ascorbic acid and DHA.28 This reduction in gastric juice vitamin C concentration could be caused by a combination of decreased excretion, instability of the vitamin at neutral pH, oxidation by nitrite, and H pylori per se.29 In common with previous studies,17 25we have confirmed that the reduction in gastric juice ascorbic acid concentration was associated with gastric juice pH andH pylori infection. Furthermore, the changes in gastric juice ascorbic acid concentrations were also related to the severity and the extent of gastritis. Gastric juice ascorbic acid concentrations were significantly reduced when gastritis extended from the antrum to the gastric body.
H pylori is strongly associated with both duodenal ulcer and gastric cancer.30 Paradoxically, duodenal ulcer disease has been inversely associated with gastric cancer. Although the underlying mechanism is unknown, it has been suggested that patients with duodenal ulcer disease have high ascorbic acid concentrations in gastric juice.17 Similarly, our study found that patients with diffuse antral gastritis, a pattern associated with duodenal ulcer, had similar ascorbic acid concentrations to normal subjects. By contrast, patients with pangastritis and precancerous lesions, such as atrophy or intestinal metaplasia, had significantly lower concentrations of both ascorbic acid and DHA. It has been reported that DHA alone, or in combination with hydroxycobalamin (vitamin B12), can greatly inhibit tumour mitotic activity without inhibiting the activity of normal fibroblasts.6 7 31 32 These findings, therefore, suggest that patients with duodenal ulcer may be still under the protection of both ascorbic acid and DHA. Those with atrophy or intestinal metaplasia, however, lack such protection.
We have also found that the CagA seropositivity of the individual is associated with a remarkable reduction in gastric juice ascorbic acid concentrations. This may be due to the higher degree of gastric inflammation found in patients infected withcagA+ strains.33 Our data show that CagA positive patients were more likely to have severe gastric inflammation, atrophy, and intestinal metaplasia in the gastric mucosa than CagA negative patients. The further reduction in gastric juice vitamin C concentrations may contribute to the increased gastric cancer risk associated with cagA+ strain infection.
The determinants for gastric antral mucosal vitamin C concentrations are more difficult to determine. We found that mucosal ascorbic acid concentrations were decreased in H pyloriinfected patients compared with those without the infection. However, there was no significant association between antral mucosal vitamin C concentrations and inflammation in the antrum. One potential explanation for this finding is that vitamin C in the gastric mucosa may be more stable than in the gastric juice. Furthermore, leucocytes have a very high ascorbic acid content34 and infiltration of leucocytes into the mucosa in active gastritis may affect mucosal ascorbic acid concentration.
In summary, we have confirmed that H pylori infection is associated with reduced gastric juice ascorbic acid concentrations and this reduction is related to the severity and topography of inflammation, gastric juice pH, and CagA antibody status of the individual. H pyloriinfection was also associated with decreased mucosal ascorbic acid concentration. In addition, gastric juice DHA concentration was reduced in patients with atrophy and intestinal metaplasia. The reduction in vitamin C concentrations in the stomach may have implications inH pylori associated carcinogenesis.