Article Text

Abstract
Background—Lymphocytic colitis is characterised by chronic watery diarrhoea with normal endoscopic or radiological findings and microscopic evidence of pronounced infiltration of the colonic mucosa with lymphocytes.
Aim—To investigate the long term clinical and histological evolution of the disease in a large group of patients with well characterised lymphocytic colitis.
Methods—Between 1986 and 1995 the histological diagnosis of lymphocytic colitis was obtained in 35 patients; 27 of these agreed to a follow up examination. All clinical, endoscopic, and histopathological records were reviewed at that time and the patients had a second endoscopic examination with follow up biopsies.
Results—The patients initially presented with the typical findings of lymphocytic colitis. After a mean (SD) follow up of 37.8 (27.5) months, diarrhoea subsided in 25 (93%) and histological normalisation was observed in 22 (82%) of the 27 patients. Progression from lymphocytic colitis to collagenous colitis was not observed.
Conclusions—Lymphocytic colitis is characterised by a benign course with resolution of diarrhoea and normalisation of histology in over 80% of patients within 38 months. Considering the benign course of the disease, the potential benefit of any drug treatment should be carefully weighed against its potential side effects.
- lymphocytic colitis
- colitis
- diarrhoea
Statistics from Altmetric.com
The term microscopic colitis was first introduced by Readet al 1 in 1980 to describe a subset of patients with chronic watery diarrhoea of unknown origin, normal endoscopic or radiological findings, and microscopic evidence of an inflammatory infiltrate in the colonic mucosa. Biopsy samples typically show a dense lymphocytic infiltration of the surface epithelial layer.2 Levison et al suggested replacing the ambiguous term microscopic colitis with lymphocytic colitis and regarding microscopic colitis as an umbrella term to cover all cases of colitis with abnormal histology but normal endoscopic or radiological appearance.2
The clinical and histopathological features of lymphocytic colitis have been well described.3-5 The long term course of the disease, however, is mostly known from case reports, and data from larger series describing the evolution of the disease are lacking. The aim of the present study was to characterise the clinical and histopathological long term course of the disease in a relatively large group of 27 patients with well documented lymphocytic colitis.
Methods
STUDY POPULATION
Between 1986 and 1995 the histological diagnosis (index biopsy) of lymphocytic colitis was obtained in 35 outpatients. These patients were asked to participate in a follow up study evaluating the clinical and histological long term course of the disease. One patient was lost to follow up, four (11%) died from unrelated causes, and three (9%) refused to have a second endoscopic examination with biopsy. Therefore 27 (77%) patients could be fully evaluated in this investigation.
CLINICAL DATA
The clinical and endoscopic records were retrospectively reviewed at the follow up visit and all patients were asked to complete a questionnaire on (a) duration of diarrhoea, (b) stool frequency, (c) stool consistency, (d) other gastrointestinal symptoms including abdominal discomfort, urgency, incontinence, and weight loss, (e) concomitant diseases before and after index investigation, (f) drug history, (g) drugs used to treat lymphocytic colitis, and (h) treatment success. Each patient was asked to grade on a visual analogue scale from 0 to 10 how he or she was affected by the symptoms of lymphocytic colitis (social impact score), 0 being not affected at all and 10 being severely affected. Diarrhoea was defined as three or more loose bowel movements per day. Stool consistency was classified as watery, viscous (like thick soup), soft (without form), or formed, as described by Readet al.1 At the follow up visit, informed consent was obtained from each patient for a follow up flexible sigmoidoscopy with biopsy.
INDEX COLONOSCOPY/FOLLOW UP SIGMOIDOSCOPY
Patients were prepared for the initial colonoscopy with 3 litres of a polyethylene glycol solution taken orally. Biopsy specimens were taken from the terminal ileum and the ascending colon in all patients. The follow up biopsy samples were taken from the sigmoid colon in unprepared patients.
HISTOPATHOLOGY
The biopsy specimens were fixed in 4% phosphate buffered formaldehyde and embedded in paraffin wax. To avoid changes in staining quality and section thickness, 5 mm sections from follow up and recut sections from index biopsy samples were stained with haematoxylin and eosin and Masson trichrome. The coded slides were evaluated by one of us (MA). The number of intraepithelial lymphocytes was obtained by counting the lymphocytes per 100 intercryptal epithelial cells. Three areas in each specimen were examined and the mean number of lymphocytes was expressed per 100 epithelial nuclei. The thickness of the subepithelial collagen band was measured with an optical micrometer (graded in 2.5 μm) using the Masson trichrome stain. A diagnosis of lymphocytic colitis was made if an increase in intraepithelial lymphocytes (normal 4.6 (1.5) intraepithelial lymphocytes per 100 intercryptal epithelial cells) was found without a thickened subepithelial collagen layer (<8 mm) and if only a slight disturbance of crypt architecture and discrete inflammatory infiltration of the lamina propria were seen.
STATISTICAL ANALYSIS
Descriptive statistics are reported as mean (SD) and including range or frequencies as appropriate. Comparisons were tested by paired or unpaired Student’s t test. Correlations between different factors were analysed by linear regression analysis. Variables found to be significantly associated were then tested in a stepwise linear regression analysis. Statistical significance was assumed by a p value of less than 0.05 (two tailed analysis).
Results
CLINICAL, ENDOSCOPIC AND HISTOLOGICAL DATA AT INDEX VISIT
Clinical data
Table 1 shows the characteristics of the 27 patients who agreed to participate in the study. The mean (SD) age at diagnosis was 60 (12) years, range 28–74. Twenty patients were women, corresponding to a 3:1 female preponderance. Colonoscopy was performed in 26 patients because of chronic watery diarrhoea of unknown cause and in one patient for unexplained chronic abdominal pain. In the latter patient, the colonoscopy disclosed a 3 mm polypoid lesion in the left colonic flexure. The 26 patients with diarrhoea reported 4.9 (2.6) bowel movements per day which lasted for a mean of 3.8 (3.4) months (range 1–16). At the time of endoscopy, four patients already noted normal bowel habits after a mean duration of diarrhoea of 4 (1.4) months. Stool consistency was watery in six patients (23%), viscous in nine (35%), soft in nine (35%), and formed in two (8%). Fifteen patients (54%) reported mild abdominal pain, 92% urgency of defecation, and 64% suffered some incontinence. Nine of the 27 patients lost a mean of 5.6 (3.4) kg within 2.6 (1.1) months.
Characteristics of the 27 patients with lymphocytic colitis
The social impact score of 5.5 (3.2) indicates that patients were considerably affected by the disease. Simple regression analysis showed a significant correlation between the social impact score and frequency of defecation, incontinence, and urgency (p<0.05). However, in a stepwise regression analysis only frequency of defecation and incontinence independently correlated with the social impact score.
One patient was known to have coeliac disease. Five patients took non-steroidal anti-inflammatory drugs (NSAIDs) on a regular basis, three of them low dose acetylsalicylic acid for cardiovascular reasons. One patient was receiving ranitidine.
Endoscopic findings
Total ileocolonoscopy was performed in all patients. None showed changes consistent with inflammatory bowel disease. In 17 patients diverticula were observed.
Histology
All biopsy samples displayed the typical findings of lymphocytic colitis, with a notable increase in intraepithelial lymphocytes (34.7 (16.0)/100 intercryptal epithelial cells).6 In addition, the samples showed a diffuse inflammatory infiltration of the lamina propria and a flattening of the surface epithelium (fig 1A). No correlation was found between the number of intraepithelial lymphocytes and the number of bowel movements (data not shown).
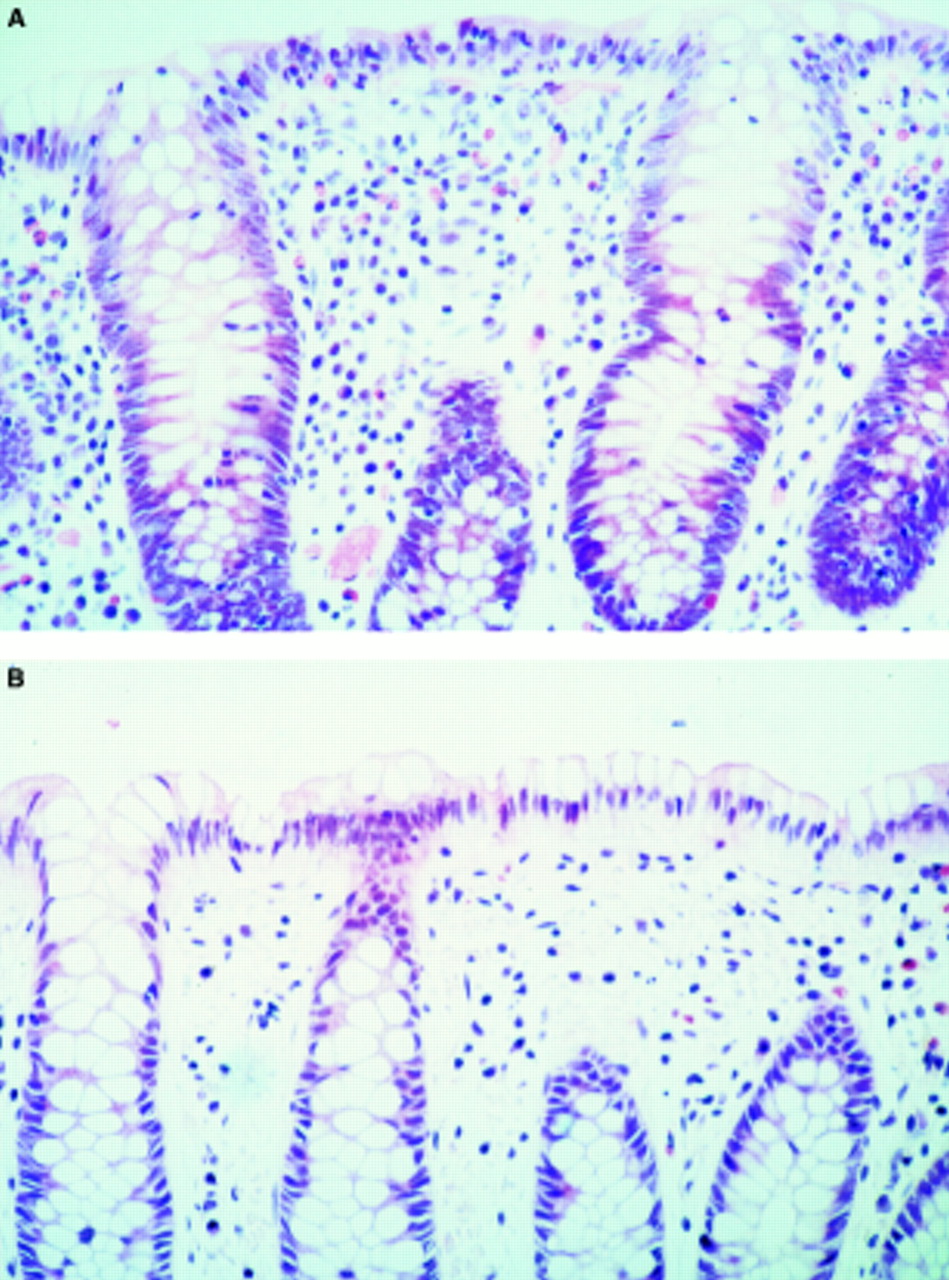
Histological findings at presentation (A) and follow up (B). Staining was with haematoxylin and eosin, original magnification was × 250. (A) Diffusely increased surface intraepithelial lymphocytes and surface epithelial damage can be seen. In addition there is a chronic inflammatory infiltrate in the lamina propria and mild crypt distortion. (B) The intraepithelial lymphocytes as well as the inflammatory infiltrate in the lamina propria have disappeared and the surface epithelium is composed of tall columnar epithelial cells.
CLINICAL, ENDOSCOPIC, AND HISTOLOGICAL DATA AT FOLLOW UP
Clinical data
Patients were interviewed after a mean follow up of 37.8 (27.5) months (range 4–101). In 25 of the 27 patients (93%), stool frequency was normal. Two patients (7%) had persistent diarrhoea with 4.0 (1.4) bowel movements a day. Stool consistency was soft and viscous respectively. Information on treatment results was obtained in 22 patients; in two patients the data could not be evaluated, one had no diarrhoea, and two patients received no drug treatment. Six patients were treated with more than one medication. Normalisation of stool frequency was observed in three of six patients (50%) treated with 5-aminosalicylic acid or sulfasalazopyridine. Diarrhoea ceased in seven of 13 patients (54%), who received spasmolytics. Two of four patients (50%) treated with loperamide and all three patients receiving antibiotic treatment showed normalisation of bowel habits (table2).
Medical treatment regimens
Histology
In 22 patients (82%) the inflammatory infiltrate had completely disappeared (fig 1B) and in five patients the lymphocytic colitis persisted (19%). Progression from lymphocytic to collagenous colitis was not observed. Normalisation of bowel habits (25 out of 27) was associated with a statistically significant (p<0.001) decrease in intraepithelial lymphocytes (fig 2). Of these 25 patients, 22 had normal biopsy findings and three still had lymphocytic colitis despite normal bowel habits. However, none of the patients with persisting diarrhoea had a normal colonic biopsy result at follow up, and in all patients with normal colonic biopsy results diarrhoea had stopped (fig2). Mean follow up time of patients with normal histology was 40 months as compared with 29 months in patients with persisting inflammatory change (p>0.05).

{kind=link}
{kind=link}
Persistence of diarrhoea plotted against percentage of intraepithelial lymphocytes. Results are expressed as mean (SEM).
Discussion
Lymphocytic colitis is a recently described disease, which is characterised by chronic watery diarrhoea of unknown cause, essentially normal endoscopic and radiological findings, and pronounced lymphocytic infiltration of the colorectal mucosa.1 ,6 The clinical and histological features of lymphocytic colitis have been well described, but the natural history has only been poorly characterised. In our long term study with a mean follow up of 38 months, we found that lymphocytic colitis is characterised by a benign course. Diarrhoea persisted in only two and the lymphocytic infiltrate in five patients. Normal histology at follow up was associated with normalisation of bowel habits in all patients, and unremitting diarrhoea was associated with persisting inflammatory changes of the colonic mucosa. Very divergent outcomes of lymphocytic colitis have been described, based mostly on case reports or studies with small patient numbers. At one end of the spectrum, lymphocytic colitis is described as a mild self limiting disease.3 ,4 At the other end, one case has been reported with a fulminant course requiring colectomy.7 At least as conflicting are the histological follow up data. Some authors report the disappearance of the inflammatory infiltrate with time.8 Others describe persisting inflammation, in some cases with progression to collagenous colitis.3 According to our data, lymphocytic colitis should be considered a benign disease with complete clinical and histological normalisation in over 80% of patients within three years.
In our study, we did not observe any progression from lymphocytic colitis to collagenous colitis. It is still unclear whether lymphocytic and collagenous colitis should be considered as one disease, lymphocytic colitis representing the first phase of collagenous colitis,9 ,10 or whether they are related but distinct entities.11 The lack of progression from lymphocytic colitis to collagenous colitis observed in our study and the distinct immunological differences between the two diseases3support the hypothesis that lymphocytic colitis and collagenous colitis are related but distinct diseases.
Three patients in our series presented without diarrhoea at follow up but with persistent lymphocytic colitis, a course that has previously been described.4 ,8 It is noteworthy that the mean follow up time of patients with normal histology was 40 months compared with 29 month in patients with persisting inflammatory changes. Even though this difference did not reach statistical significance, probably because of the small sample size, one might argue that the longer the follow up, the higher the likelihood of histological normalisation. The persisting inflammatory infiltrate seen in patients with resolved diarrhoea may suggest that clinical normalisation precedes histological normalisation.
The intraepithelial lymphocyte count significantly correlated with the presence or absence of diarrhoea, but not with its severity. A correlation between stool weight and lamina propria cellularity was previously observed in patients with collagenous and microscopic colitis.12 Both studies therefore suggest that the inflammatory infiltrate, triggered by some unknown, probably luminal, factor is involved in the pathogenic process leading to chronic diarrhoea.
It should be cautiously noted that biopsy specimens from index and follow up examinations in our patients were not taken from the same segment of the colon. The index investigation was always a complete ileocolonoscopy, and the follow up examination a flexible sigmoidoscopy only. Accordingly index biopsy specimens were usually obtained from the ascending colon, whereas all follow up samples were taken from the sigmoid colon. However, we do not believe that this explains the difference in intraepithelial lymphocyte counts between index and follow up biopsy samples, as lymphocytic colitis usually affects the entire colon. Thus the intraepithelial lymphocyte count is quite similar between the various segments of the large bowel.6 ,13 Therefore biopsy samples from the sigmoid colon may be considered to be representative of the entire colon.
In a minority of patients, lymphocytic colitis can be present in the absence of diarrhoea.14 ,15 This has also been documented for collagenous colitis.16 Only one of our patients did not present with diarrhoea.
Slightly more than half of our patients presented with diarrhoea, urgency, and crampy abdominal pain, symptoms compatible with irritable bowel syndrome. It has already been pointed out that there is some clinical resemblance between irritable bowel syndrome and lymphocytic colitis.3 Is lymphocytic colitis in these patients therefore an incidental finding only, unrelated to the clinical symptoms? There are several arguments against this assumption. Firstly, irritable bowel syndrome usually begins at a younger age than that of our study population; secondly, patients with irritable bowel syndrome usually complain of alternating constipation and diarrhoea; thirdly, they have a more insidious onset of the disease. Our patients with lymphocytic colitis had a sudden onset of diarrhoea, an observation also made in patients with collagenous colitis.17Importantly, the histological results of colonic biopsy specimens from patients with irritable bowel syndrome are always normal. The results of our study emphasise that, in patients with chronic watery diarrhoea and crampy abdominal pain, urgency, or incontinence, a colonoscopic investigation with biopsy is mandatory, before a diagnosis of irritable bowel syndrome can be entertained. The strongest argument, however, that lymphocytic colitis is not an incidental finding is provided by a recent study in which a marked reduction in colonic water absorption resulting from reduced active and passive sodium and chloride absorption was observed.18 Furthermore chloride/bicarbonate exchange was also reduced. The inflammatory infiltrate of the colonic mucosa is therefore associated with a reduction in colonic fluid absorption, which probably contributes to the development of diarrhoea.
Drugs such as ranitidine19 and cyclo 3 fort, a phlebotonic drug commonly used in France,20 have been implicated in the cause of lymphocytic colitis. In our study one patient was on ranitidine and none of our patients used cyclo 3 fort. It should be noted that five of our patients used NSAIDs. An association between NSAIDs and collagenous colitis has been reported, but a relation between NSAID intake and lymphocytic colitis has never been established. However, it cannot be ruled out that NSAIDs contribute to the development of lymphocytic colitis in these patients.
Half of our patients responded favourably to treatment with 5-aminosalicylic acid or sulfosalazopyridine, spasmolytics, or loperamide. Even though no bacteriological investigations were performed and there is no clear evidence for an infectious aetiology of lymphocytic colitis, it is intriguing that all three patients treated with antibiotics showed prompt resolution of their symptoms. Similar results were reported in a recent publication, in which various antibiotics induced clinical remission in 63% of patients with collagenous colitis.17 In another study, bacterial cytotoxins were found in the stool of a patient with collagenous colitis.21 In addition, faecal diversion results in clinical and histological remission, with relapse on restoration of the faecal stream.22 All these findings suggest that a luminal infectious agent may be involved in the pathogenesis of collagenous colitis and lymphocytic colitis.
In summary, our study shows that lymphocytic colitis is characterised by a benign course, with normalisation of stool frequency and histology in over 80% of patients within 40 months. None of the patients with persisting diarrhoea had normal colonic biopsy results at follow up, and in all patients with normal colonic biopsy findings at follow up diarrhoea had stopped. Considering the benign course of the disease, we believe that the potential benefit of any long term drug treatment should be carefully weighed against its potential side effects.