Article Text

Abstract
Background: Smoking is a recognised risk factor for pancreatic cancer and has been associated with chronic pancreatitis and also with type II diabetes.
Aims: The aim of this study was to investigate the effect of tobacco on the age of diagnosis of pancreatitis and progression of disease, as measured by the appearance of calcification and diabetes.
Patients: We used data from a retrospective cohort of 934 patients with chronic alcoholic pancreatitis where information on smoking was available, who were diagnosed and followed in clinical centres in five countries.
Methods: We compared age at diagnosis of pancreatitis in smokers versus non-smokers, and used the Cox proportional hazards model to evaluate the effects of tobacco on the development of calcification and diabetes, after adjustment for age, sex, centre, and alcohol consumption.
Results: The diagnosis of pancreatitis was made, on average, 4.7 years earlier in smokers than in non-smokers (p = 0.001). Tobacco smoking increased significantly the risk of pancreatic calcifications (hazard ratio (HR) 4.9 (95% confidence interval (CI) 2.3–10.5) for smokers v non-smokers) and to a lesser extent the risk of diabetes (HR 2.3 (95% CI 1.2–4.2)) during the course of pancreatitis.
Conclusions: In this study, tobacco smoking was associated with earlier diagnosis of chronic alcoholic pancreatitis and with the appearance of calcifications and diabetes, independent of alcohol consumption.
- chronic alcoholic pancreatitis
- diabetes
- calcification
- tobacco smoking
Statistics from Altmetric.com
Although alcohol is recognised as the major cause of chronic pancreatitis, smoking has been described as an additional risk factor.1,2 Calcification, pancreatic insufficiency, and diabetes are common in chronic pancreatitis but little is known of the promoting role of smoking on the evolution of these complications. Using data from a retrospective cohort study originally designed to evaluate the risk of pancreatic cancer in patients with chronic pancreatitis,3 we have now investigated the role of tobacco on progression of alcoholic pancreatitis, as measured by age at diagnosis of disease and time until appearance of calcification and diabetes.
METHODS
In this report, we selected from our original historical cohort (n = 1552) those patients with alcoholic chronic pancreatitis for whom smoking status was known. We also obtained updated data from Switzerland. The final study population consisted of 934 patients with chronic alcoholic pancreatitis for whom data were retrieved from clinical records or existing computerised databases in clinical centres specialising in the management of chronic pancreatitis. The number of cases from each country was as follows: Switzerland, 239; Germany, 140; USA, 202; Italy, 315; and Sweden, 38. Centre specific clinical details, methods of diagnosis, and treatment of pancreatitis have been described in previous publications.4–9 The diagnosis was based on a combination of the following criteria: symptoms of chronic epigastric pain, steatorrhoea, or both; radiographic evidence of pancreatic calcification; evidence of chronic pancreatitis on histological or pancreatographic procedures; and results of laboratory tests (that is, exocrine insufficiency). Determination of the two end points of the study—pancreatic calcification or diabetes—was measured by the presence of calcification on abdominal radiography or by an elevated fasting blood sugar or an abnormal glucose tolerance test.
The cohort from which this series of patient derived has already been studied to evaluate the risk of pancreatic cancer in those with chronic pancreatitis and to determine which factors predict mortality.3,10 The database included information on demographic and clinical characteristics of the patients, including the presence and date of diagnosis of calcification and/or diabetes, as well as information on smoking status and level of alcohol consumption recorded at the onset of disease. Alcohol consumption, when available, was categorised as low to moderate (<5 alcoholic drinks/day), heavy (5–9 drinks/day), or very heavy (10 or more drinks/day).
Student’s t tests were used to compare age at diagnosis of pancreatitis in smokers versus non-smokers. We used logistic regression analysis to evaluate the association between tobacco and the presence of calcification or diabetes either at the time of diagnosis of chronic alcoholic pancreatitis or at the end of the follow up period. Cox proportional hazards regression analysis was used to evaluate the promoting role of tobacco on the time to development of calcification or diabetes after the initial diagnosis of chronic pancreatitis. All models were adjusted for age, sex, centre, and alcohol consumption (⩾5 v <5 drinks/day). Plots of the cumulative incidence of calcification and diabetes after the diagnosis of pancreatitis were drawn using the Kaplan Meier method. The log rank test was used to compare the incidence of calcification and/or diabetes between smokers and non-smokers. Because either calcification or diabetes may precede the diagnosis of chronic pancreatitis, we also plotted the cumulative incidence of calcification and diabetes starting from birth. Before presenting the results from the log rank tests or from the Cox models, we tested the proportional hazard assumption by introducing a constructed time dependent variable and testing for its significance. Data were analysed using SAS procedures; all tests were two sided.
RESULTS
The cohort comprised 934 patients (814 males, 120 females) with a confirmed diagnosis of chronic alcoholic pancreatitis and available smoking information. Ninety three per cent of males and 91% of females ever smoked. Duration of follow up was 8.4 (SD 7.6) years. There was no difference in duration of follow up for smokers and non-smokers (p = 0.48).
Overall, smokers were diagnosed with pancreatitis at a younger age (mean 44.6 (SD 10.9) years) than non-smokers (mean 49.3 (14.3) years) (p = 0.001). The majority of patients were heavy or very heavy (⩾5 drinks/day) alcohol drinkers (65% of non-smokers v 77% of smokers; p = 0.06).
Calcification was present at the time of diagnosis of pancreatitis in 40% of males and in 34% of females. It was subsequently detected in 28% of males and 38% of females during a mean follow up period of 8.4 years. In addition, calcification was mentioned but the date of development was unknown for 6.1% of males and 5.8% of females. Similarly, diabetes was present at diagnosis of pancreatitis in 21% of males and 20% of females and developed during follow up in 30% of males and 27% of females (table 1).
Characteristics of 934 patients with chronic alcoholic pancreatitis
Smoking was associated with a higher prevalence of calcification at the time of diagnosis of pancreatitis (odds ratio (OR) 2.0 (95% confidence interval (CI) 1.1–3.8)) but was not related to the prevalence of diabetes (OR 0.9 (95% CI 0.5–1.7)) (table 2).
Risk of calcification and diabetes in relation to cigarette smoking
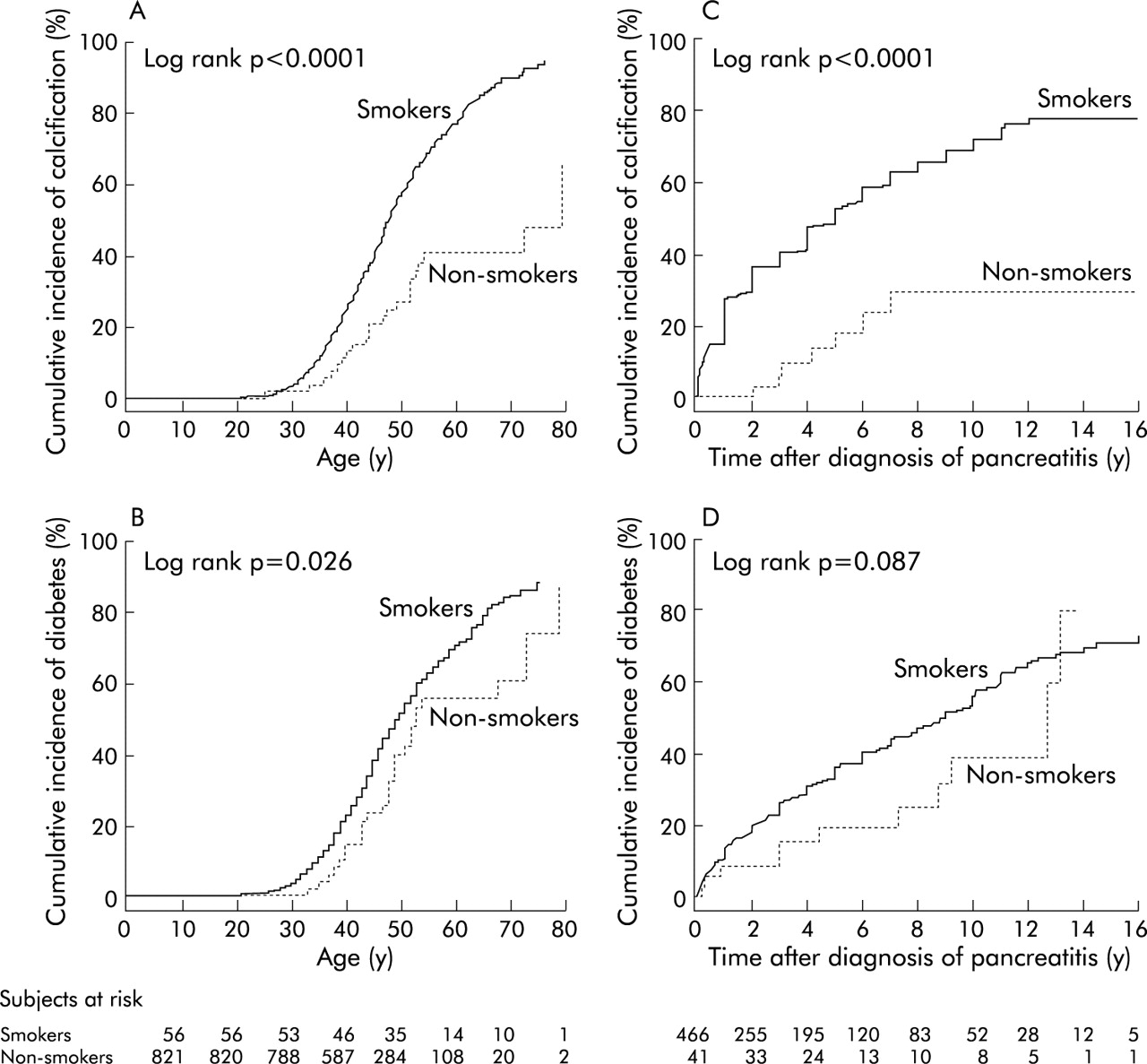
Development of calcification after the initial diagnosis of pancreatitis was significantly associated with cigarette smoking (hazards ratio (HR) 4.9 (95% CI 2.3–10.5)) (table 2). The risk was similar for moderate (<1 pack cig./day) and heavy (>1 pack cig./day) smokers. Figure 1 illustrates the cumulative incidence of calcification and diabetes according to smoking status in patients with chronic alcoholic pancreatitis. Two starting points (birth and diagnosis of chronic pancreatitis) were considered. By age 60 years, 80% of smokers had signs of calcification compared with 40% of non-smokers. Smoking was also associated with a significant increase in the risk of developing diabetes after the diagnosis of pancreatitis (HR 2.3 (95% CI 1.2–4.2)) (table 2).

{kind=link}
Cumulative incidence of calcification (A) and diabetes (B) since birth in smokers and non-smokers in chronic alcoholic pancreatitis, and cumulative incidence of calcification (C) and diabetes (D) developing after the diagnosis of chronic alcoholic pancreatitis.
For 80% of smokers, quantitative information on daily tobacco consumption was available. The magnitude of the association between smoking and calcification or diabetes was similar for patients who smoked <1 pack/day and those who smoked >1 pack/day (table 2). Surprisingly, patients classified as smokers but with missing quantitative data were diagnosed at an older age than ever smokers (table 2). Nearly all patients (93%) with missing quantitative data were from the US centre where we previously reported that age at diagnosis of pancreatitis was approximately 10 years older than in other centres.3 Nevertheless, even in the USA, mean age at diagnosis of pancreatitis was older for never smokers (59.4 years) than for ever smokers (52.5 years).
In order to limit the possibility of residual confounding due to alcohol, we performed a stratified analysis based on three different levels of alcohol consumption: the magnitude of the associations reported previously were similar in all groups (table 3).
Risk of calcification and diabetes in relation to cigarette smoking for various levels of alcohol consumption assessed at the time of diagnosis of chronic pancreatitis
The results were homogeneous within countries although the number of non-smokers in each single country was limited, and country specific risk estimates had large confidence intervals. In particular, the risk of developing calcification after the initial diagnosis of chronic alcoholic pancreatitis was HR = 4.1 (1.7–10.1) for non-US subjects and HR = 5.1 (1.2–21.5) for US subjects who were diagnosed with chronic pancreatitis at an older age. Finally, as some of the Italian data in this study were reported previously,1 we performed an additional analysis after excluding this centre. The findings remained unchanged but became stronger.
DISCUSSION
From our previous analysis of this data set, we reported that age at diagnosis, smoking, and drinking were major independent predictors of mortality in patients with chronic pancreatitis10 but the mechanisms or the intermediate effects were not described.
Tobacco has been described as an important risk factor for chronic pancreatitis and is the strongest known environmental risk factor for pancreatic cancer.1 Patients with chronic pancreatitis are at high risk of developing pancreatic cancer but whether this is a true association or the result of confounding by smoking has been controversial.11,12 It has recently been reported that smoking accelerates the onset of pancreatic cancer in high risk groups.13,14
In the present large multicentre study, we have shown that smoking contributes to deterioration of pancreatitis, as measured by the appearance of calcification and diabetes, confirming previous reports. Initially, in 1994, Cavallini et al first described the effect of tobacco and alcohol on pancreatic lithogenesis in the course of chronic pancreatitis. They found that medium to heavy smokers had a significantly increased risk of developing calcifications but found no effects of alcohol.15 Imoto and DiMagno also found that cigarette smoking increased the risk of pancreatic calcification in late onset idiopathic chronic pancreatitis in those who never consumed alcoholic beverages, providing further evidence of the independent effect of smoking on the development of calcification.16 In our study, adjustment for alcohol consumption or stratification for different levels of alcohol consumption (moderate, heavy, very heavy) did not change the results. Smoking is also responsible for calcification in many other organs. In particular, it is strongly associated with coronary artery and aortic arch calcification17,18 and with placental calcification.19,20
The mechanism by which smoking contributes to pancreatic injury or by which smoking accelerates the pancreatic inflammatory process is still unknown but laboratory studies have found that activation of multiple signal transduction pathways due to nicotine exposure results in high levels of intracellular calcium release and may be responsible for cell cytotoxicity and cell injury.21
Little has been published on the association between calcification and pancreatic cancer, unlike its association with diabetes which has long been noted. The nature of this association and whether diabetes is a true aetiological risk factor for pancreatic cancer or solely associated with the development of the tumour remain unclear. Heavy smoking, which has been identified as a risk factor for non-insulin dependent diabetes mellitus in several studies,22–24 could in part act as a confounder in the relation between longstanding diabetes and pancreatic cancer.25 This is supported by our study which showed that smoking enhanced the development of diabetes in patients with chronic pancreatitis, with a risk of the same magnitude as that for developing pancreatic cancer in long term diabetics. Cigarette smoking has also been associated with abnormal fasting glucose levels26 while light to moderate alcohol consumption has been associated with a decreased risk of developing type 2 diabetes mellitus.27,28 However, the mechanism by which cigarette smoking increases the risk of impaired fasting glucose and type 2 diabetes remains unclear. Laboratory studies have indicated that cigarette smoking may cause insulin resistance in peripheral tissues.29 In an experimental control trial using two oral glucose tolerance tests, smoking acutely impaired glucose tolerance and acutely increased serum insulin and C peptide levels.30 In addition, levels of counterregulatory hormones to insulin, such as catecholamines, increased by substances in cigarettes, may lead to insulin resistance.31
The epidemiological evidence linking smoking and pancreatic damage is further supported by pathology reports and recent advances in molecular biology. In 1986, Auerbach and Garfinkel identified histological changes in the pancreas in relation to smoking and coffee drinking habits.32 Since then, development of new molecular technology has allowed identification of the k-ras oncogene which is mutated in over 90% of pancreatic cancers. It is generally accepted that ras mutations are a frequent33 early event in the pathogenesis of a variety of neoplastic and non-neoplastic pancreatic lesions. Furthermore, k-ras mutations are about the only molecular alteration found in chronic pancreatitis and in those ductal hyperplasias known to bear the highest malignant potential.34,35
Recently, the appearance of k-ras mutations in benign and malignant pancreatic diseases has been associated with tobacco.36–38 In particular, Malats et al found high rates of k-ras mutations in patients with exocrine pancreatic cancer who only smoked and in patients who only drank.36 Berger et al confirmed the association with smoking using non-neoplastic pancreata from individuals who smoked more than two packs of cigarettes/day for 20 or more years.37
We recognise the limitations of our study. In particular, information on smoking and drinking was from patient clinical records or from existing computerised databases, and were not collected prospectively and in a standardised fashion directly from the patient. As a result, these data were missing or incomplete for a large number of patients from the original cohort, which weaken the study results. Also, detailed information on age of onset and duration of smoking and drinking was not available, and hence there is potential for residual confounding of smoking behaviour by drinking behaviour, especially if smokers started drinking earlier than non-smokers.
In conclusion, we found that exposure to tobacco smoking was associated with an earlier diagnosis of chronic alcoholic pancreatitis (by approximately five years) and predisposed to the development of both calcification and diabetes. Further epidemiological studies using newer biomolecular techniques should provide new insights into the pathogenesis of benign and malignant pancreatic diseases.
Acknowledgments
This study was supported by grants from the CD Smithers Foundation, Solvay Pharmaceuticals Corporation, A Waring Foundation Zurich, and the Italian Association for Cancer Research (AIRC).
REFERENCES
Footnotes
-
Conflict of interest: None declared.