Article Text

Abstract
Background and aims: Probiotic bacteria are being investigated as possible treatments for many intestinal disorders. The present study aimed to explore the effects of live, heat killed, or gamma irradiated Lactobacillus reuteri on cardio-autonomic response and single fibre unit discharge in dorsal root ganglia to colorectal distension in healthy Sprague-Dawley rats housed under conventional conditions. The effects of this treatment on somatic pain were also examined.
Methods: 1×109 bacteria were given by gavage for nine days. Colorectal distension occurred under anaesthesia. Heart rate was measured through continuous electrocardiography. Single fibre unit discharge was recorded from the 6th left lumbar dorsal root ganglion. Somatic pain was evaluated by the tail flick and paw pressure tests.
Results: Colorectal distension caused a pressure dependent bradycardia in the control (native medium) group. Treatment with live, heat killed, or gamma irradiated bacteria as well as their products (conditioned medium) prevented the pain response even during the maximum distension pressure (80 mm Hg). Both viable and non-viable bacteria significantly decreased dorsal root ganglion single unit activity to distension. No effects on somatic pain were seen with any treatment.
Conclusions: Oral administration of either live or killed probiotic bacteria or conditioned medium inhibited the constitutive cardio-autonomic response to colorectal distension in rats through effects on enteric nerves. These data may provide a novel explanation for beneficial probiotic effects on visceral pain.
- IBD, inflammatory bowel disease
- IBS, irritable bowel syndrome
- colorectal distension
- inflammatory bowel disease
- irritable bowel syndrome
- Lactobacillus reuteri
Statistics from Altmetric.com
Probiotics are defined as living microorganisms which, upon ingestion in adequate numbers, exert health benefits beyond inherent general nutrition.1 Commensal bacteria associated popularly with probiotic activity are Lactobacilli, Bifidobacteria, and Streptococci and non-pathogenic Escherichia coli. They are also important and normal constituents of the human gastrointestinal microflora. Probiotics have been used in the treatment of bacterial or viral induced acute intestinal infections such as antibiotic associated diarrhoea,2,3Clostridium difficile infection,4 traveller’s diarrhoea, and rotavirus diarrhoea.5,6 In recent years, some clinical studies have shown the therapeutic effects of different strains of probiotics in the treatment of chronic inflammatory bowel disease (IBD) including ulcerative colitis,7,8 Crohn’s disease,9 and pouchitis,10,11 or prevention of allergic disease12 such as atopic eczema and asthma. In addition, some investigators have reported that probiotic treatment has been effective for the attenuation of experimental colitis seen in interleukin-10 deficient mice,13,14 trinitrobenzene sulfonic acid (TNBS) or dextran sulfate sodium (DSS) chemically induced colitis in mice,15,16 and transgenic HLA-B27 rats.17
Irritable bowel syndrome (IBS) is one of the most common chronic disorders in which abnormal discomfort or pain is associated with defecation or a change in bowel habit, in the absence of other disease that could explain the symptoms.18 It is likely that various factors contribute to the causation of symptoms, but no final mechanisms have yet been agreed upon. However there is general agreement that increased sensitivity to visceral pain and/or disordered autonomic function is one of the mechanisms involved in symptom generation in patients with IBS.19–21 The autonomic pathways are also a major mediator of the visceral pain response and altered autonomic balance may alter visceral perception.22 The magnitude of the autonomic response to visceral stimulation such as distension can be used to quantify the intensity of visceral perception and of visceral autonomic function in animal models. Colorectal distension is an established technique23,24 for delivering noxious visceral stimuli to rats.
There have been a few clinical trials25,26 which have suggested that treatment with various probiotic bacteria can improve IBS symptoms. In a recent study, Kim et al reported that a probiotic formulation containing eight different probiotic species, VSL#3, appeared to be promising in the relief of abdominal bloating in patients with diarrhoea predominant IBS.27 O’Mahony et al have recently also shown that oral administration of Bifidobacterium infantis significantly improved the symptoms including the abdominal pain/discomfort score in IBS patients in a randomised controlled trial.28 However the exact mechanism of action of probiotics in IBS is poorly understood. The functional effects of probiotics on the autonomic nervous system and visceral perception have not yet been examined in otherwise unstimulated healthy animals housed under conventional conditions.
The reason we chose to study Lactobacillus reuteri was that it has been described as having a positive effect on the incidence of diarrhoea in children29 and also inhibited the onset of colitis in transgenic IL-10 deficient mice.14
In the present study, we investigated the effects of live Lactobacillus reuteri, a probiotic bacterium, on cardio-autonomic responses and single fibre unit discharge in dorsal root ganglia to colorectal distension in healthy male Sprague-Dawley rats. In addition, to explore the mechanisms of action of probiotic therapy, we tested whether non-viable (gamma irradiated or heat killed) Lactobacillus reuteri or some structural components or secreted products of this microorganism (conditioned media) were also effective. The effects of live or heat killed Lactobacillus reuteri on somatic pain were also examined.
MATERIALS AND METHODS
Animals
All experiments were performed using male Sprague-Dawley rats (Charles River Breeding Laboratories, Saint Constant, QC, Canada) weighing 360–514 g. Rats were housed in the Central Animal Facilities in micro-isolator cages equipped with filter hoods, under controlled temperature (20°C), with a 12:12 hour light-dark cycle, and free access to food and water. Animals were fasted for 18 hours before experiments, but had unrestricted access to water. All experiments were approved by the Animal Care Committee of McMaster University, and all procedures were conducted in accordance with the Guidelines of the Canadian Council on Animal Care.
Bacterial preparations
Lactobacillus reuteri were purchased originally from the America Tissue Type Culture Collection (ATCC #23272). From frozen stocks (−80°C), LR were inoculated in fresh Man-Rogosa-Sharpe liquid medium (MRS broth; Difco Laboratories, USA) and grown at 37°C under anaerobic conditions for 48 hours. Bacteria were put into 50 ml sterile tubes in 40 ml MRS broth. After two days, bacteria had grown so much that they settled on the bottom of the tubes. Tubes were centrifuged at 2000 rpm for 15 minutes at room temp, washed twice with sterile PBS until the colour was white and measured 32 (yellow) exactly in a Vitek colorimeter when appropriately diluted. This reading gives a concentration of 6×108 bacteria/ml. 8.5 ml of bacterial suspension were centrifuged in 15 ml tubes at 2000 rpm for 15 minutes at room temp; supernatants were discarded and bacteria resuspended in 1 ml of MRS broth to give a concentration of 5×109 bacteria per millilitre. Heat killed Lactobacillus reuteri were prepared by heating aliquots of viable bacterial suspensions for 20 minutes at 80°C. Resuspended viable LR cells were killed by gamma irradiation with Cobalt 60 for 20 hours at 8.05 Gy/min. The resulting viability was determined by plating on MRS agar plates under anaerobic conditions for 72 hours at 37°C. No bacterial growth was detected in either the heat killed or irradiated Lactobacillus reuteri preparations.
Treatment protocol
Rats were divided into five groups in the experiments. After handling for one week, they were fed by gavaging 1×109 organisms in 0.2 ml daily for nine days (live n = 30, heat killed n = 9, gamma irradiated n = 6, or conditioned medium n = 6). Medium preparations consisted of either native or centrifuged (cell free) medium after 48 hours of bacterial culture (conditioned medium). Rats treated with native medium served as controls. Gavage was performed every morning using an 18 gauge blunt needle in unanaesthetised animals.
Cardio-autonomic response to colorectal distension
Experimental protocol
Rats were anaesthetised with a ketamine hydrochloride (75 mg/kg) and xylazine (10 mg/kg) mixture, given intraperitoneally. Supplemental anaesthesia was given throughout the study as required. A 5 cm length plastic balloon, affixed to a Teflon catheter with a length of approximately 20 cm, was inserted intrarectally into the distal colon so that the tip was 6 cm from the anus. The catheter was connected to a barostat system composed of a flow meter and pressure control program (Distender, G&J Electronic Inc, Toronto, Canada). The cardiac response to colorectal distension was measured while inflating the balloon with air to pressures of 50, 70, and 80 mm Hg for 60 seconds. Only one set of distensions per animal per day was performed. In order to let the animal recover from the previous distension, 10 minutes’ rest was allowed between each distension.
Data acquisition
The methodology has been published previously elsewhere.30 In brief, continuous recordings of heart rate were performed through a surface electrocardiogram (ECG), obtained through three needle electrodes applied to the left and right shoulders and the right hind leg. The signal was amplified and recorded on a personal computer using a commercial data acquisition program (Experimenter’s Workbench, DataWave Technologies, Longmont, CO, USA). Heart rate was measured for 60 seconds before, during, and after the CRD, for a total of 180 seconds. Heart rate data were presented as the average heart rate for every 10 seconds period during distension. Changes in heart rate were expressed as percent change compared to the resting heart rate prior to the distension in each animal.
Single fibre unit discharge (dorsal root ganglion) responding to colorectal distension
Four groups of rats treated with native medium (control, n = 8), viable (n = 6), heat killed (n = 6), and gamma irradiated (n = 7) bacteria were tested for effects of probiotic treatment on the visceral sensory afferent pathway response to colorectal stimuli by examining single unit discharge induced by colorectal distension.
Experimental protocol
The methodology has been previously published.31 Briefly, after anaesthesia with ketamine hydrochloride (90 mg/kg) and xylazine (20 mg/kg), a laminectomy was performed to expose the 6th left lumbar dorsal root ganglion (LL6 DRG) and its root (LL6 DR). The skin and connective tissue were used to create a pool in which nerve tissue was immersed in mineral oil at 36–37°C to protect the spinal cord and exposed LL6 DRG. Bipolar tungsten electrodes were used to record single unit discharge. The LL6 DR between LL6 DRG and spinal cord was hooked on the negative electrode. A fine filament of nerve peeled off with forceps from LL6 DR and the proximal end of the filament was wrapped around the tip of the positive electrode. The electrodes were connected to the headstage (AI-402, Axon Instruments, CA, USA).
Data acquisition
The signals were amplified and processed through the programmable signal conditioner (Cyber Amp 380, Axon Instruments, Foster City, CA, USA). The amplified signals were digitalised at 2 KHz by an A/D converter and stored on a personal computer using the same data acquisition program as for ECG data.
Somatic pain measurement
Three groups of rats treated with native medium (control, n = 5), viable (n = 6), or heat killed (n = 5) bacteria were examined for effects of probiotic treatment on somatic pain. Assessment of somatic pain was evaluated by measuring the threshold to thermal (tail flick test) or mechanical stimuli (paw pressure test).
Thermal stimuli—tail flick test
The tail of the rat was immersed, up to 5 cm from the tip, in a water bath (Poly Science Division of Preston Ind Inc, Niles, IL, USA) at a noxious temperature of 50±1°C. The latency from onset of stimulation to tail withdrawal was recorded.32
Mechanical stimuli—paw pressure test
Nociceptive thresholds, expressed in grams, were measured with the Randall-Selitto analgesimeter (probe tip diameter 1 mm) (Ugo Basile, Biological Research Apparatus, Milan, Italy) by applying increasing pressure at a constant rate on the rat paw until the paw was withdrawn.32
Microbiological analysis
Stool samples were collected before and after probiotic treatments. Each sample was weighed, homogenised, and diluted in 1 ml of 40% glycerol/PBS solution. The dilutions were spread onto Lactobacilli selective MRS agar and anaerobically inoculated in triplicate at 37°C and incubated for 72 hours. Lactobacilli colonies were counted on the MRS plate. The data were expressed as colonies/mg of faeces.
Statistical analysis
All data except somatic pain parameters were presented as mean (SEM). Student’s t test (paired), ANOVA (repeated or unrepeated), and the Newman-Keuls multiple comparison test were used as appropriate. Somatic pain parameters were expressed as median (range) and evaluated by the Mann-Whitney test. A p value <0.05 was considered statistically significant.
RESULTS
Baseline heart rate
The baseline resting heart rate was measured for each rat, for 60 seconds before colorectal distension. The resting heart rates were expressed as mean average beats per minute. In control anaesthetised animals this was between 190 and 404 per minute, with a mean rate of 246.7 (SEM 6.2) per minute. No significant differences in the resting heart rate were seen among groups (data not shown).
Effect of Lactobacillus reuteri on heart rate response to colorectal distension
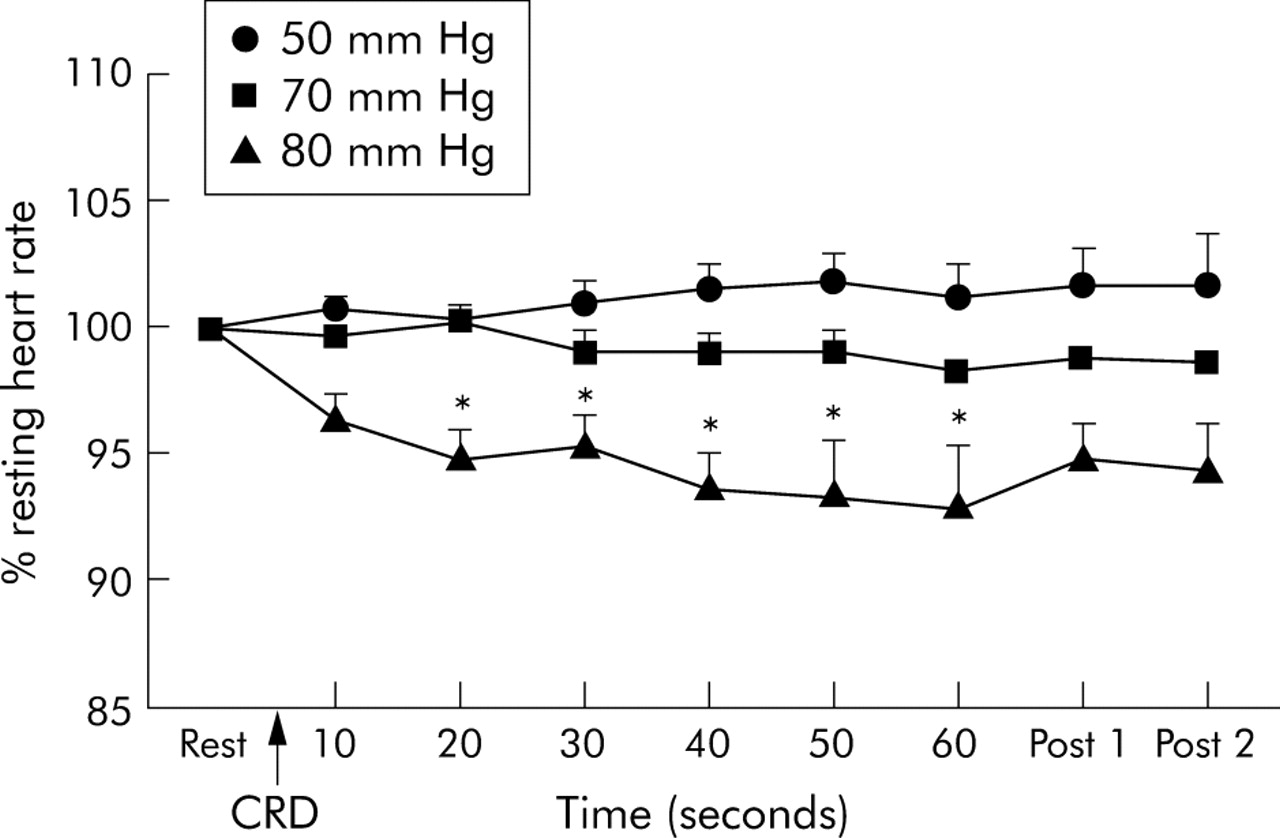
Colorectal distension caused a decrease in heart rate in the control group (n = 10) that peaked at various times post distension, depending on the distension pressure (fig 1). The response began at the moment of balloon inflation and persisted throughout distension. This response to the colorectal distension was not observed in the group treated with live Lactobacillus reuteri, even during the maximum distension pressure (80 mm Hg) (fig 2). The inhibition of heart rate response to colorectal distension by Lactobacillus reuteri remained significant compared to the control in a subgroup analysis based on animals’ body weight.
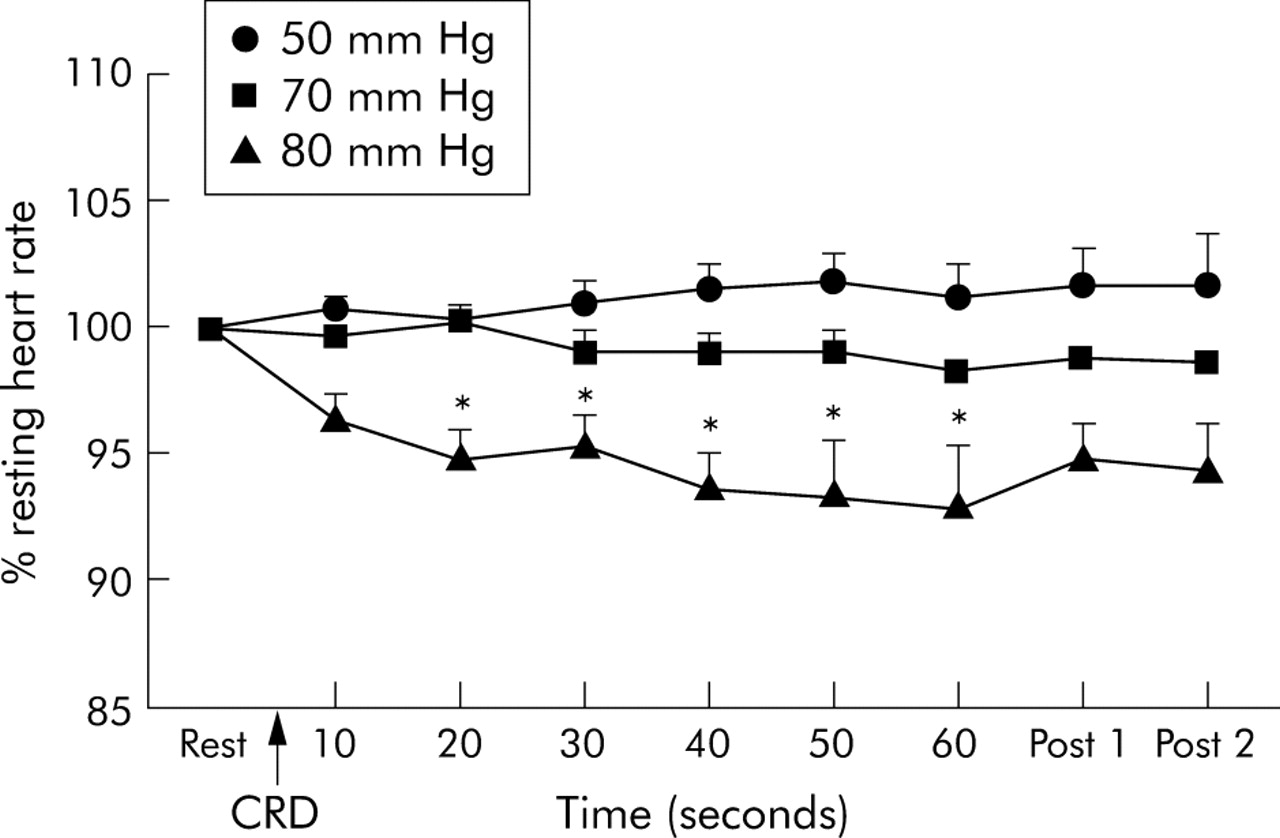
Time course of cardiac response to colorectal distension (CRD) of 50, 70, and 80 mm Hg in control (native medium) group rats. Post 1 and 2 represented an average of heart rate response during first and last 30 seconds after distension. Data presented as mean (SEM) of % change in heart rate compared with resting heart rate (n = 10). *p<0.05 versus resting.

Effect of oral administration of live Lactobacillus reuteri on cardiac response to colorectal distension of 50, 70, and 80 mm Hg. Data presented as mean (SEM) of maximum % change in heart rate during distension compared with resting heart rate. Treatment: control (n = 10), viable LR (n = 30). *p<0.01 versus control.
Similar inhibition of cardio-autonomic responses was seen in the heat killed, gamma irradiated, and conditioned media groups (fig 3).

Effect of various probiotic treatments on cardiac responses to colorectal distension. Data presented as mean (SEM) of maximum % change in heart rate during distension compared with resting heart rate. Treatment: control (n = 10), viable LR (n = 30), heat killed LR (n = 9), gamma irradiated LR (n = 6), conditioned media group (n = 6). *p<0.01 versus control.
Effect of Lactobacillus reuteri on single fibre unit discharge in response to CRD
LL6 DR basal single unit discharge at rest in the control group was significantly higher than that of any other groups. The stimulus-response curve is shown in figure 4. A pressure dependent colonic afferent fibre response to colorectal distension is evident in all groups. Responses to 60 mm Hg were significantly reduced to <60% of the control group by the feeding of viable or non-viable (heat killed and gamma irradiated) bacteria. The administration of viable and both types of non-viable bacteria significantly decreased single unit activity to colorectal distension compared with the control group at all pressures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of various probiotic treatments on LL6 DR single unit discharge to colorectal distension. Data are presented as mean (SEM). Treatment: control (n = 8), viable Lactobacillus reuteri (n = 6), heat killed Lactobacillus reuteri (n = 6), gamma irradiated LR (n = 7). *p<0.05 versus various treatment groups.
Effect of Lactobacillus reuteri on somatic pain
Tail flick latencies and paw withdrawal thresholds due to pressure were used as the thermal pain and mechanical pain parameters, respectively. Table 1 shows the results of these tests in each group. There were no significant differences between the control, viable, and heat killed groups in either the tail flick or paw pressure tests.
Effect of probiotic treatment on somatic pain
Microbiological evaluation
After administration of live bacteria, the faecal concentration (67.4 (SEM 23.6)×105 colonies/mg faeces) of Lactobacilli increased significantly when compared with the basal level (1.5 (SEM 1.4)×105 colonies/mg faeces). Numbers did not change in any of the other groups (n = 6–15).
DISCUSSION
We examined the effects of oral treatment of a probiotic bacteria, Lactobacillus reuteri, on the cardio-autonomic response to colorectal distension in Sprague Dawley rats. The findings of this study were as follows:
-
Noxious colorectal distension caused a decrease in heart rate in anaesthetised healthy control rats.
-
Oral administration of both live and non-viable (heat killed and gamma irradiated) Lactobacillus reuteri attenuated the cardiac and colonic afferent fibre responses to colorectal distension. This inhibitory effect on pain was also reproduced with conditioned medium.
-
There were no effects of these treatments on somatic pain.
It is widely accepted that the intestinal microflora play an important role in the health of the host and also possesses immunomodulatory capacity.33–35 A disturbance in the balance of normal intestinal microflora, or the host response to this, has been shown to play a critical role in the pathogenesis of IBD.33,36 Non-pathogenic bacteria may modify immune responses of the intestinal mucosa through interaction and signaling at mucosal surfaces. Probiotic bacteria offer a means of modifying the enteric microflora, and their therapeutic effects may include competitive interaction with commensal and pathogenic flora, production of antimicrobial metabolites, or influence the immune response by modulating mucosal and systemic immunity,33,34 epithelial function,33,37 and improving nutritional and microbial balance in the intestinal tract. However, the exact mechanisms of probiotic action are not well understood.
The most interesting finding in this study is the elimination of any cardio-autonomic response to the highest colorectal distension pressures in normal rats after treatment with live or dead probiotic bacteria and even after treatment with conditioned medium. The existence of brain-gut relations suggests that autonomic pathways through sensory afferent nerves are involved in informing the brain of the physiological and pathological events that occur in visceral organs. Several models of visceral perception have been demonstrated23,24,30 in animals based on the study of visceromotor or cardiovascular responses to gastrointestinal and colonic distension. Cardiovascular responses to colorectal distension reflect the intensity of sensory perception or the integrated autonomic function. In IBS patients, some investigators suggest that visceral hypersensitivity is involved in the aetiology of the disorder, while others emphasise the importance of disturbed autonomic function.38 Our results suggest that a particular probiotic, live or dead, or even products found in culture medium, can reduce the normal visceral sensitivity to colorectal distension.
There is little evidence from published research that similar effects of probiotic organisms have been seen before on the autonomic nervous system. Kamm et al have recently shown in pigs that a probiotic yeast, Saccharomyces boulardii seemed to decrease the number of calbindin positive myenteric neurons.39 This was the only marker of many tested which showed any change following probiotic treatment: these included calcitonin gene related peptide, nitric oxide synthase, vasoactive intestinal polypeptide, and substance P. L farciminis treatment inhibited a delayed hypersensitivity model of colitis in rats, probably through NO release.40 Monocontamination of germ free rats with L acidophilus or Bifidobacterium bifidum has been shown to reduce the migrating myoelectric complex period.41 In the latter study neuropeptide Y was decreased in the blood following conventionalisation with full intestinal microflora, suggesting reduced inhibitory control of intestinal propulsion.
In our study, administration of conditioned media and non-viable bacteria (both heat killed and gamma irradiated) inhibited the autonomic response to colorectal distension. Previous studies indicated that heat killed Lactobacillus acidophilus retained adhesion capacity to the epithelial receptor sites.42 Furthermore, bacterial peptidoglycan, an essential component of Gram positive bacterial cell walls, is known to activate toll-like receptors (TLR2). Indeed, the composition of lipoteichoic acid in the cell wall of a probiotic bacterium, Lactobacillus plantarum, has been recently shown to modulate both pro- and anti-inflammatory immune responses.43 Bacterial lipopolosaccharide also interacts with TLR2 and TLR4.44,45 Many commensal organisms can influence innate immune mechanisms through toll receptors. On the other hand, non-viable gamma irradiated bacteria, but not heat killed bacteria, had an attenuating effect on experimental colitis in mice, and this immunoregulation was mediated by TLR9-probiotic DNA motif interaction.15,46 However, because heat killed organisms were equally effective as gamma irradiated in our studies, we infer that there are differences between the mechanisms of action of probiotics on inhibition of mucosal inflammation through toll receptors and the elimination of autonomic responses to distension.
We found that oral administration of Lactobacilli had an inhibitory effect on constitutive discharge in colonic afferent fibres in the dorsal root ganglia. Furthermore, the measurements of single fibre discharge frequency in response to colorectal distension paralleled the cardioautonomic effects observed on colorectal distension. This clearly showed that the effect was localised to the intestine or its neuronal connections to the spinal cord. We previously demonstrated that colonic distension produced a volume dependent bradycardia mediated through sympathetic afferent and cholinergic vagal efferent pathways in Sprague-Dawley rats.47 Under anaesthesia, neither the thalamus nor the cerebral cortex are necessary for the evocation of cardioautonomic response to colorectal distension. The brainstem and hypothalamus integrate autonomic responses. We could find no effect of probiotic treatment on somatic pain in either of the standard tests employed. Taking these results on somatic pain into consideration, our results obtained with the DRG single unit discharge suggest that the observed effects were peripheral and not central (brain).
An interesting recent study has shown that another strain of Lactobacilli (paracasei) attenuated smooth muscle hypercontractility post Trichinella infection.48 This effect was heat labile and a component in the conditioned medium also had the same effect. The effect of gamma irradiated organisms was not tested. The authors concluded that the effect was likely mediated by the immune response to infection and direct effects on smooth muscle. Again Verdu et al very recently showed that administration of L paracasei or the spent culture medium prevented the antibiotic induced increase in visceromotor response and inflammatory activity, and effectively decreased immunostaining for substance P.49 In their model the direct effect of probiotic treatment on modulation of visceral perception by the autonomic nervous system in healthy animals was not tested. These results clearly show that another Lactobacillus strain can modulate inflammation associated visceral hypersensitivity responses in a murine model. In view of our findings in healthy conventionally housed rats, an additional important mechanism to explain their observations might be through a more direct effect of the probiotic on a component of the nervous system. Alternatively, the involvement of visceral pain perception resulting from inflammation may have a different functional mechanism.
In conclusion, this is the first study to examine the effect of probiotic bacteria on autonomic function and visceral perception in vivo in normal animals. Oral administration of live or dead Lactobacillus reuteri and even conditioned medium showed marked inhibitory effects on the cardio-autonomic response to colorectal distension in Sprague-Dawley rats. These data provide supportive evidence for further explanation of the effect of probiotics on visceral pain and provide a novel mechanism of the effect of probiotics in the treatment of patients with functional bowel disorders such as IBS.
Acknowledgments
The author gratefully acknowledge contributions to the support of this research for St Joseph’s Healthcare Foundation, the BRAIN network funded by the Ontario Research Development Challenge fund, and the BROAD Foundation.
REFERENCES
Footnotes
-
Competing interests: none.