Article Text

Abstract
Background: The available classifications of gastritis are inconsistently used, possibly because none provides immediate prognostic/therapeutic information to clinicians. As histology reporting of hepatitis in terms of stage is clinically useful and widely accepted, an international group (Operative Link on Gastritis Assessment (OLGA)) proposed an equivalent staging system for reporting gastric histology. Gastritis staging integrates the atrophy score (obtained by biopsy) and the atrophy topography (achieved through directed biopsy mapping).
Aim: To test in a prospective cross-sectional study whether OLGA staging consistently stratified patients according to their cancer risk and provided clear prognostic/therapeutic information.
Methods: OLGA staging for gastric cancer risk (0–IV) and gastritis grading (overall score of the inflammatory infiltrate, grade 1–4) were applied in 439 prospectively enrolled, consecutive, dyspeptic outpatients who underwent endoscopy with standardised biopsy sampling. Incidental neoplastic lesions and coexisting peptic ulcers were recorded. Results were presented as stage (including antral (A) and corpus (C) atrophy scores) and H pylori status (eg, A = 3; C = 2: stage IV; Hp+ve).
Results: Benign conditions (including duodenal ulcers; p<0.001) consistently clustered in stages 0–II, whereas all neoplastic (invasive and non-invasive) lesions clustered in stages III–IV (p<0.001).
Conclusions: Gastritis staging, combined with H pylori status, provided clinically relevant information on the overall status of the gastric mucosa with implications for prognosis, therapy and management.
- OLGA, Operative Link on Gastritis Assessment
- PPI, proton pump inhibitor
- gastritis
- atrophic gastritis
- OLGA staging
- precancerous gastric lesions
- non-invasive neoplasia
Statistics from Altmetric.com
Gastritis is an inflammatory condition of the gastric mucosa.1–6 The phenotypic spectrum of chronic gastric inflammation is well established, and the basic distinction between non-atrophic and atrophic patterns is both internationally accepted and consistent.7–9 Atrophy is defined as “loss of appropriate glands” and is subtyped into two main histological variants: atrophy resulting from the disappearance of glands and replacement with fibrosis of the lamina propria; and glandular loss resulting from replacement of native glands with metaplastic, “inappropriate for location” glandular structures.1,7–9 Long-term follow-up studies conducted in different populations have consistently confirmed that the extent of the mucosal atrophy parallels gastric cancer risk.10–17
The Sydney system and its Houston-updated version attempted to improve on Whitehead’s classification18 of gastritis and, at the same time, develop a reporting system to assist the pathologist.3,4,6 Although the Sydney system is widely cited, most citations refer to its four-point grading system of the histological lesions and not to the recommended format of biopsy reporting.
Currently, no reporting scheme/terminology for chronic gastritis is available that is both easily understood by clinicians and patients and also provides prognostic and therapeutic information in unequivocal terms. This situation contrasts markedly with that of chronic hepatitis, where the “traditional” histological report with descriptive labels has been replaced by a widely adopted staging system.19–21 Hepatitis staging has proved useful in simplifying medical communication, monitoring the progression of the disease and the effects of treatment, and, at the same time, expressing the cancer risk associated with the progression to cirrhosis evolution.
The successful experience of hepatitis staging prompted an international group of gastroenterologists and pathologists (Operative Link on Gastritis Assessment (OLGA)) to develop a histological staging system for gastric inflammatory diseases that would meet the same objectives as the hepatitis staging system.22,23 The OLGA system uses the biopsy sampling protocol and the visual analogue scales recommended by the Houston-updated Sydney system.7 In the OLGA staging system, gastric atrophy is considered to be the histological lesion representative of disease progression. Gastritis stage results from combining the extent of atrophy scored histologically with the topography of atrophy identified through biopsy mapping. It has been also suggested that the diagnostic report include information about the probable aetiology.22
This prospective cross-sectional study aimed to validate the OLGA gastritis staging system as a routine histology reporting system. It also tested whether the diagnostic message conveyed by the gastritis stage consistently identified patients with different cancer risk and also provided clinicians with clear prognostic and therapeutic information.
PATIENTS AND METHODS
Patients
A total of 439 consecutive dyspeptic outpatients referred to the gastroenterology unit of the Rovereto Regional Hospital between April 2004 and April 2005 were prospectively enrolled in the study. To minimise the variability in the endoscopy procedure (macroscopic assessment and biopsy sampling protocol), only patients having consecutive upper gastrointestinal endoscopy procedures performed by only one trained gastroenterologist (AM), with specific expertise in upper gastrointestinal endoscopy, were entered into the study. Patient clinical history was obtained by the endoscopist who performed the procedure, who also obtained consent from the patient to be involved in the study.
Exclusion criteria were (a) any previous surgical intervention to the upper gastrointestinal tract because of either oesophageal or gastric disease, (b) incomplete gastric endoscopy procedure for whatever reason, and (c) inadequate gastric biopsy sampling (see endoscopy protocol).
The endoscopy protocol specifically required that the presence of any focal lesions be noted. The presence of peptic ulcers (active and/or scars, both duodenal and gastric) and any (flat, depressed, elevated) lesion was recorded, and biopsy samples were always obtained for histological examination (see biopsy sampling protocol).
Of 448 consecutive patients who had endoscopy procedures, nine were excluded (four male and five female; mean age 59 (range 23–73)): in three, the endoscopy procedure was incomplete; two patients did not consent to be involved in the study; one patient had undergone partial gastrectomy; in three cases the available histology samples were not consistent with the study’s aims (superficial samples or number of samples obtained was inconsistent with the sampling protocol).
According to the Sydney system, the biopsy sampling protocol required that no less than five biopsy samples were obtained: two from the antral mucosa; one from the mucosa of the angularis incisura; two from the oxyntic area.3 Biopsy samples were submitted to the pathology department in different vials labelled according to the site of the sample. Additional biopsy samples were obtained from any endoscopically detected focal lesion.
Helicobacter pylori status was assessed from both histology and clinical history. Cases were considered H pylori positive (Hp+ve) when bacteria (irrespective of their density) were histologically detected in one or more of the available biopsy samples. Patients in whom H pylori was not histologically detected at the time of the endoscopy procedure were considered Hp-negative (Hp−ve). According to the patient’s clinical history (which was double checked when needed by interviewing the patients’ general practitioner), Hp−ve cases were subgrouped as: (a) naïve Hp−ve, when H pylori infection had never been detected and no history of previous eradication was recorded; or (b) H pylori eradicated (Hp-eradicated) when a previous history of Hp+ve status was recorded (by either invasive or non-invasive tests), followed by successful H pylori eradication treatment. When possible, the time interval between eradication treatment and enrolment in the study was also noted.
The use of proton pump inhibitors (PPIs) when treatment was longer than 6 months, and even when stopped 1 month or less before the enrolling endoscopy, was noted.
Histology study
The biopsy samples were fixed in formalin (5–10%) and submitted to the department of pathology in three separate vials, labelled according to their topographic site (antrum, angularis incisura, or corpus). The paraffin-embedding procedure distinguished the biopsy samples accordingly.
Multiple histology sections (5 μm thick) were obtained from each paraffin block. Sections were stained with H&E, periodic acid–Schiff, and Giemsa (modified for H pylori). Two pathologists (GP and MR), blinded to any clinical information, jointly examined all the specimens, reaching a consensus on the score of each histological variable.
According to internationally accepted criteria, at each biopsy sample site, gastritis was distinguished in non-atrophic (ie, no loss of appropriate glands) and atrophic (ie, loss of appropriate glands). Mucosal atrophy (both phenotypes, ie, with and without metaplastic epithelial transformation (ie, intestinal metaplasia in both antral and/or oxyntic biopsy samples and pseudo-pyloric metaplasia in oxyntic biopsy samples)) was scored according to the Sydney system using a visual analogue scale (0 = absent; 1 = mild; 2 = moderate; 3 = severe).7 On the basis of the topographic locations (oxyntic and angular/antral) of the histology changes, the gastritis stage was assessed according to the OLGA proposal.22 In particular, all the biopsy samples obtained from both the antrum and angularis incisura were considered together as representative of the distal, non-oxyntic, gastric mucosa, and any atrophic changes were scored according to the visual analogue scale. The same scoring system was applied in the assessment of atrophic changes in oxyntic biopsy samples. The OLGA gastritis stage was finally obtained by combining antral with oxyntic scores (fig 1)
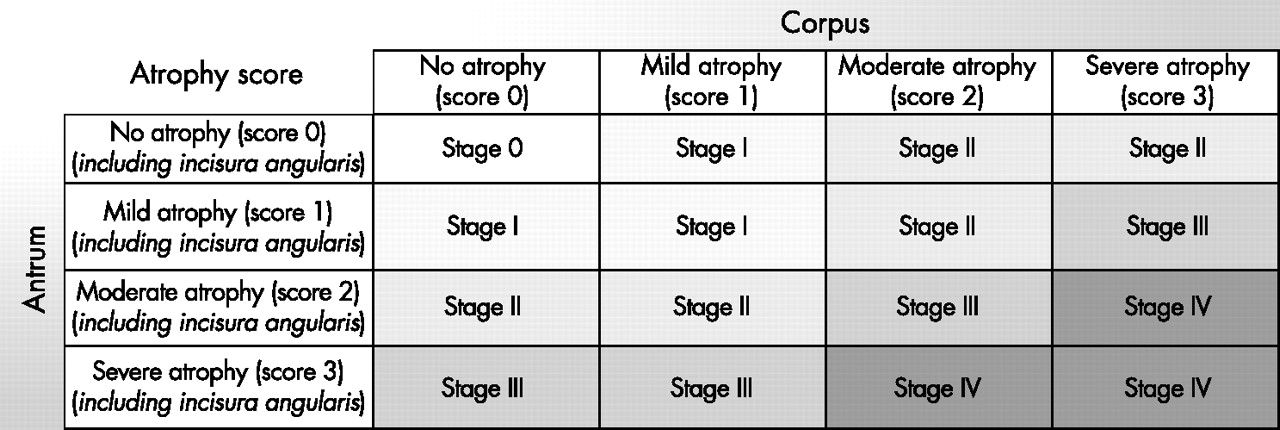
Gastritis staging: the OLGA system. Atrophy is defined as loss of appropriate glands (with or without metaplasia). In each compartment (ie, mucous-secreting antral and oxyntic/corpus mucosa), atrophy is scored in a four-tiered scale (0–3) according to the visual analogue scale of the Houston-updated Sydney system. The stage result from the combination of atrophic changes was assessed in the two mucosal compartments considered.
Visual analogue scales (0 = absent; 1 = mild; 2 = moderate; 3 = severe) were used as reference in grading mucosal inflammation at the level of each biopsy site. An overall score for mucosal inflammatory infiltrate was generated by combining the scores obtained from each biopsy sample (grade of gastritis).
Invasive gastric adenocarcinoma and non-invasive neoplastic lesions were histologically assessed according to internationally validated criteria.24,25
Statistical analysis
The t test and one-way analysis of variance were applied for statistical calculations. Odds ratios (ORs) and 95% CI were calculated to assess the strength of association between variables, using the ordinal logistic regression model (OR = 1 indicating no association). Stata software (Statistics Data Analysis V8.1; http//stata.com) was used for all calculations. p<0.05 was considered significant.
RESULTS
Table 1 summarises the main basic and clinical characteristics of the patients in the study. The H pylori status of patients is reported as histologically Hp+ve (187) or Hp−ve (subgrouped as naïve Hp−ve (192) or Hp-eradicated (60)). For the 187 Hp+ve patients, the male/female ratio was 1/1.07, and the mean age 56 (range 20–85). The mean age of the naïve Hp−ve patients (192; male/female = 1.04/1) was 51 (range 17–88), and the mean age of the Hp-eradicated patients (60; male/female = 1/1.06) was 61 (range 27–82). Information about the time of the eradication treatment for the Hp-eradicated patients was available in 43 of 60 cases; the mean time between eradication treatment and enrolment was 22 months (range 6–51).
Basic and clinicopathological data for the patients entered in the study
Table 1 reports PPI treatment: 65 out of 439 patients had taken a PPI for longer than 6 months. According to the H pylori status, the prevalence of PPI treatment was as follows: Hp+ve, 11%; Hp−ve/naïve, 5%; Hp-eradicated, 27%.
Overall, 34 peptic ulcers were detected, 29 duodenal and five gastric. Duodenal ulcers (22 active; seven scars) were slightly more common in male patients (male/female 16/13), with no significant association with the age intervals considered (table 2). Twenty-three out of 29 (79%) duodenal ulcers were detected in H pylori-positive patients (Pearson’s χ2 p = 0.0003). Gastric ulcers (two active; three scars; male/female ratio 2/3) were located 6–11 cm from the pyloric ring, and three out of five occurred in H pylori-positive patients.
Gastritis staging in the 439 patients entered in the study
Five cases of neoplastic lesion were detected: one invasive adenocarcinoma (pT1N0M0; pathological stage IA)26; one high-grade non-invasive neoplasia; three low-grade non-invasive neoplasia. In two additional patients, lesions indefinite for non-invasive neoplasia (ie, hyperproliferative intestinal metaplasia) were detected. The mean age of patients in whom a neoplastic lesion (either invasive or non-invasive) was detected was 71.6 (range 64–80); the mean age of patients with a lesion indefinite for non-invasive neoplasia was 65. Table 1 shows the locations.
Gastritis staging
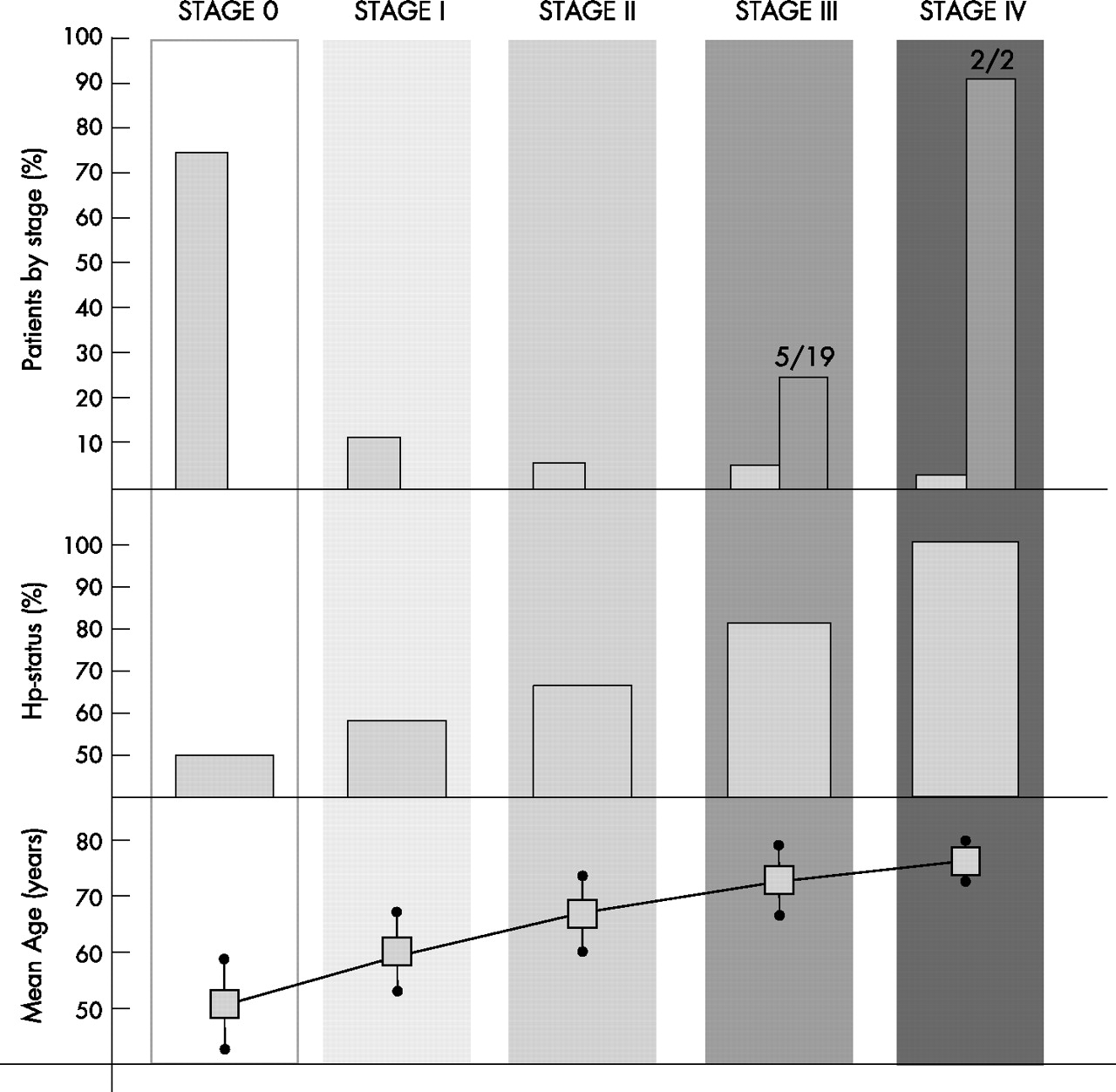
Table 2 shows patient distribution by gastritis stage. The mean age of the patients increased significantly from stage 0 to stage IV (mean (SD) age: stage 0, 52 (16.3) (range 17–88); stage I, 61 (15.3) (range 22–85); stage II, 64 (13.5) (range 34–84); stage III, 66 (13.5) (range 37–85); stage IV, 73.5 (6.4) (range 69–78); non-parametric test for trend p = 0.006) (fig 2). Table 2 shows H pylori status (Hp+ve versus Hp-eradicated versus Hp−ve/naïve). The prevalence of H pylori infection (active or eradicated) progressively increased from stage 0 (51%) to stage IV (100%) (χ2 for ordered groups p = 0.003) (fig 2).

{kind=link}
{kind=link}
Case distribution (%) by gastritis staging in 439 consecutive patients. The dark columns indicate the prevalence of neoplastic and indefinite for neoplasia cases among the patients clustered in stages III and IV (no cases of neoplasia or indefinite for non-invasive neoplasia lesions were detected in stages 0, I and II). H pylori status (Hp+ve and Hp-eradicated patients are collapsed together) by stage and the mean age of patients allocated to each stage are also shown.
The majority (>68%) of duodenal ulcers clustered in stage 0, and an additional 17% was associated with stage I. The prevalence of duodenal ulcer correlated inversely with gastritis stage (χ2 for ordered groups p = 0.001).
Table 3 shows the relationship between gastric ulcers, H pylori status and gastritis stage. Gastric ulcers (active and scarred) were never detected in stage 0 or stage I. Two out of five gastric ulcers were active, and both were in Hp+ve female patients with stage III gastritis.
Focal lesions and H pylori status by stage
Table 3 also shows the relationship between neoplastic lesions and H pylori status. No cases of neoplasia were detected in naïve H pylori-negative patients; three cases of neoplastic or indefinite for non-invasive neoplasia lesions coexisted with active H pylori infection (one gastric cancer, one low-grade non-invasive neoplasia, and one indefinite for non-invasive neoplasia lesion). Four lesions were detected in Hp-eradicated patients: in three cases (one high-grade non-invasive neoplasia, one low-grade non-invasive neoplasia, and one indefinite for non-invasive neoplasia lesion), H pylori eradication had been obtained within the 12 months before the patient’s enrolment; no information was available on the time of the H pylori eradication in the remaining patient with low-grade non-invasive neoplasia.
Table 2 shows the prevalence of invasive (one case) and non-invasive (four cases) neoplasia in each gastritis stage. In stages 0, I and II, no neoplastic lesions were detected, as they were all clustered in stages III and IV (fig 2). Excluding the two cases of indefinite for non-invasive neoplasia lesions, the prevalence of definite neoplastic alterations in stages III+IV was 24% (5/21) (stage III = 3/19 (16%); stage IV = 2/2 (100%)) (fig 2). When neoplastic and indefinite for non-invasive neoplasia lesions were considered together, their prevalence in stages III+IV increased to 33% (7/21). Considering together stages 0+I+II versus stages III+IV, the association of stages III+IV with neoplastic lesions was significant, either including or excluding indefinite for non-invasive neoplastic lesions (Pearson’s χ2 (including indefinite for non-invasive neoplasia lesions) p<0.0001; Pearson’s χ2 (excluding indefinite for non-invasive neoplasia lesions) p = 0.0001; OR = 104; 95% CI = 18–549; p = 0.0001).
Most patients taking PPIs (51/65 = 78%) had stage 0 gastritis. The prevalence of PPI treatment by stage was: stage 0, 40%; stage I, 13%; stage II, 14%; stage III, 10%; stage IV, 0%.
Gastritis grading
Table 4 shows patient distribution by gastritis grade. The mean age of patients in each grade did not differ significantly (p = NS). Gastritis grade 0–1 was never detected in Hp+ve patients, and only Hp+ve patients were allocated to gastritis grade 4. Gastritis grades 0+1 included 83% and 68% of the naïve Hp−ve and Hp-eradicated patients, respectively. No Hp−ve patients (either naïve or eradicated) featured grade 4 gastritis. Collapsing grades 0+1 and grades 2+3+4, the latter were significantly associated with Hp+ve status (Pearson’s χ2 p<0.0001; OR = 2.02; 95% CI = 1.65–2.48; p<0.001).
Gastritis grading in the 439 patients in the study
Duodenal ulcers were most commonly associated with gastritis grades 2, 3 and 4 (86%) (table 4), which is consistent with the association between duodenal lesions and H pylori infection (table 3).
All five gastric ulcers coexisted with inflammatory mucosal lesions, but high-grade inflammation (ie, gastritis grade 4) was only associated with active ulcers.
Most patients taking PPIs had grade 2 gastritis (21/65 = 32%). The prevalence of these patients by gastritis grade was as follows: grade 0, 13%; grade 1, 22%; grade 2, 14%; grade 3, 12%; grade 4, 12%.
Neoplastic (invasive and non-invasive) lesions did not significantly cluster in any of the gastritis grades considered.
DISCUSSION
There is epidemiological, clinical, pathological and molecular evidence to link H pylori-induced gastritis with gastric cancer.17,27 Gastric atrophy is considered the “cancerisation field” in which “epidemic” gastric cancer develops.10,15,17,28–30
The available clinicopathological classifications of gastritis are inconsistently used, possibly because most of them do not provide clinicians with immediate prognostic and therapeutic information. In addition, because they lack explicit ranking of severity, the descriptive labels of chronic gastritis carry the risk of being misinterpreted by both general practitioners and patients.
On the basis of the well-established clinical usefulness of histology reporting of hepatitis in terms of stage, the international OLGA group proposed a new staging system for reporting gastritis histology. Gastritis staging integrates the atrophy score (obtained by biopsy) and the atrophy topography (achieved through directed biopsy mapping). This prospective cross-sectional study tested whether the OLGA staging system consistently stratifies patients according to their cancer risk and provides clear prognostic/therapeutic information.
Gastritis staging
Standardised gastric biopsy samples obtained from a consecutive series of dyspeptic outpatients were used to test the suitability of histologically reporting gastritis in terms of the OLGA system of gastritis staging. In this study, no special procedures were applied to the biopsy handling, and the histology assessment at each single biopsy level was strictly consistent with the current guidelines.3,6,8 The OLGA staging system proved easy to use, but further tests are needed to validate its inter-centre reproducibility.
When the two basic requirements are met (ie, standardised biopsy sampling and histological scoring of the atrophic lesions consistent with current international guidelines), gastritis staging can provide an immediate evaluation of the severity of the disease, with particular reference to cancer risk. In this study, all seven neoplastic (non-invasive and invasive) events clustered in the 21/439 patients with stage III and IV gastritis. This result is consistent with the biological assumption that the extent and location of atrophy correlate with the risk of cancer10,15,17,31 and validates the efficacy of the OLGA staging, which suitably amalgamates the biologically and clinically useful messages. In fact, the clustering of the neoplastic lesions in stages III and IV (in which less than 5% of the study population was allocated) identified a restricted subgroup of patients who might be reasonable candidates for a (theoretically cost effective) surveillance programme.31–33
Most PPI users (78%) had stage 0 gastritis, with approximately half being Hp−ve (both naïve and eradicated). Duodenal ulcers consistently clustered in the “benign stages”, whereas gastric ulcers clustered in high-grade stages.34–38
Gastritis grading
The original Sydney system and its Houston-updated version score the lymph mono-plasmocyte component from granulocytes (ie, activity).3,4,39,40 In our opinion, such detailed scoring at each biopsy level provides no additionally useful information to the clinician, who is primarily interested in histology results with specific therapeutic and prognostic impact; in addition, a meticulous scoring of the inflammatory infiltrate also increases the interobserver variability.
The grading system adopted in this study conveys an overall message about the inflammatory component of the gastric disease. The correlation between gastritis grade and H pylori status supports the efficacy of the grading system, which, however, needs to be further validated in aetiological contexts other than H pylori infection.
CONCLUSION
The new OLGA staging system proved easy to use and provided intuitive and clear prognostic and therapeutic information. The OLGA stage should be given as the concluding statement of a “traditional” histology report or plotted on the “staging scale” originally proposed by OLGA (fig 1); in any case, the staging information should be combined with the aetiological hypothesis of the gastric disease (eg, Hp+ve, Hp−ve, or Hp-suspected, or histology consistent with autoimmune gastritis) as suggested by the histological features (eg, OLGA staging: stage IV (A = 3; C = 2); Hp+ve).
Prospective multicentre studies are needed to validate the proposal of OLGA in different epidemiological contexts.
Acknowledgments
This study was supported by AIRC (Italian Association for Cancer Research; Veneto Regional grant, 2006), Cittadella Contro il Cancro (CCC) and Morgagni Foundations, and by the Italian Public Health Minister (Programma Speciale ex art. 12-2C; Lett. B, DL 502/92).
REFERENCES
Footnotes
-
Published Online First 1 December 2006
-
Competing interests: None.
Linked Articles
- Digest