Article Text

Abstract
Background: Metabolic syndrome is associated with non-alcoholic steatohepatitis and cryptogenic cirrhosis. Whether metabolic syndrome affects the severity of chronic hepatitis B (CHB) is unclear.
Aim: We aimed to study the relationship between metabolic syndrome and the risk of liver cirrhosis in patients with CHB.
Methods: We prospectively recruited patients with CHB from primary care and hospital clinics for liver stiffness measurement (LSM) with transient elastography to diagnose early cirrhosis. Probable cirrhosis was defined as LSM ⩾13.4 kPa. We analysed a subgroup of patients with paired LSM and liver biopsies to validate the accuracy of LSM.
Results: 1466 patients had reliable LSM and 134 (9%) patients had adequate liver biopsy. 188 (13%) patients had metabolic syndrome. Histological liver cirrhosis was present in 32/134 (24%) patients. Histological liver cirrhosis was more common among patients who had metabolic syndrome (38%) versus those who did not (11%, p<0.001). The specificity of probable cirrhosis on LSM for histological cirrhosis was 94%. Probable cirrhosis was present in 187 (13%) patients. Metabolic syndrome was more prevalent in patients with probable cirrhosis (24%) than those without cirrhosis (11%, p<0.001). After adjustment for anthropometric, biochemical and virological factors, metabolic syndrome remained an independent factor associated with probable cirrhosis (odds ratio 1.7, 95% confidence interval (CI) 1.1 to 2.6). The odds ratios of probable cirrhosis were 1.4 (95% CI, 0.9 to 2.3), 2.6 (95% CI, 1.7 to 4.3), 4.1 (95% CI, 2.4 to 7.1), 4.0 (95% CI, 1.9 to 8.4) and 5.5 (95% CI, 1.8 to 16.7) in patients with one, two, three, four and five components of metabolic syndrome, respectively.
Conclusion: Metabolic syndrome is an independent risk factor of liver cirrhosis in CHB.
Statistics from Altmetric.com
Chronic hepatitis B (CHB) is a global health problem affecting over 350 million people. It is the most common cause of liver cirrhosis, hepatic decompensation and hepatocellular carcinoma.1 Potential risk factors for progression to cirrhosis include older age, male gender, alcohol use, co-infection with hepatitis C virus, hepatitis D virus, or human immunodeficiency virus, elevated alanine aminotransferase (ALT) levels, high hepatitis B virus (HBV) DNA level, positive hepatitis B e antigen (HBeAg) status, and possibly HBV genotype.2 3 Liver cirrhosis is one of the most important risk factors for the development of hepatocellular carcionoma.4 5
Metabolic syndrome, comprising type 2 diabetes, hypertension, central obesity and dyslipidaemia, is increasingly prevalent worldwide. Adipokines including leptin, adiponectin and resistin, which are secreted by the metabolically active visceral adipose tissue and involved in metabolic syndrome, have gained attention in the pathogenesis of fibrogenesis in various chronic liver diseases.6–9 Non-alcoholic fatty liver disease, characterised by hepatic steatosis with or without necroinflammation and fibrosis, is strongly associated with metabolic syndrome.10 11 It may result in histological progression to cirrhosis, liver decompensation and liver cancer.12 13 Moreover, hepatic steatosis commonly coexists with other chronic liver diseases. Hepatic steatosis is present in up to 30–70% of patients with chronic hepatitis C (CHC).14 15 Patients with CHC and hepatic steatosis have more rapid progression of liver fibrosis and poorer response to peginterferon and ribavirin treatment, independently of hepatitis C genotypes.16 In patients with CHC genotypes 1 and 4, insulin resistance is associated with high viral load and significant fibrosis independent of hepatic steatosis.17 On the other hand, the relationship between metabolic syndrome and CHB is unclear.
All previous histological studies, including those on CHC, represent biased populations with active disease or probable cirrhosis. On the other hand, performing liver biopsies on a large number of patients with inactive disease is unlikely to be widely acceptable. Recently, several non-invasive assessments of liver fibrosis including serum and clinical biomarkers as well as transient elastography for liver stiffness measurement (LSM) have been investigated for clinical use.18 In a systemic review19 LSM was noted to have high sensitivity and specificity to detect histological liver cirrhosis. With the advent of transient elastography, we can assess the metabolic profile and liver status of a large number of CHB patients with different disease spectrum.
In this study, we aimed to investigate the prevalence of metabolic syndrome in patients with CHB. We investigated the relationship between viral factors, metabolic syndrome and its different components, and the risk of liver cirrhosis. We also aimed to evaluate the performance of transient elastography in patients suffering from metabolic syndrome and obesity.
METHODS
Study population
We prospectively recruited CHB patients regardless of the disease activity for transient elastography. We received referrals from all primary care and hospital clinics in Hong Kong from July 2006 to February 2008. A subgroup of patients who were indicated to assess the severity of fibrosis and inflammation prior to treatment was recruited in the same period to validate the performance of transient elastography. CHB was diagnosed by positive serology tests for serum hepatitis B surface antigen (HBsAg) for at least 6 months. We excluded patients with evidence of other chronic liver disease by screening with antibody against hepatitis C virus, anti-nuclear antibody, anti-smooth muscle antibody, anti-mitochondrial antibody, serum ceruloplasmin, transferrin saturation and ferritin. We interviewed every patient with a standardised questionnaire and excluded men who consumed more than 30 g of alcohol per week and women who consumed more than 20 g of alcohol per week. Secondary causes of hepatic steatosis (eg, chronic use of systemic corticosteroids and methotrexate) were also excluded. We also excluded patients who had decompensated liver disease, complications of liver cirrhosis, hepatocellular carcinoma, previous liver surgery or liver transplantation. All patients gave written informed consent before being enrolled into the study.
Clinical evaluation
All patients received comprehensive clinical and laboratory assessment at the time of LSM. Serum HBV DNA levels were measured by the TaqMan real-time polymerase chain reaction assay with a range of detection 100 to 109 copies/ml.20 Anthropometric parameters including body weight, body height, hip circumference and waist circumference were measured. Body-mass index (BMI) was calculated as weight (in kilograms) divided by height (in metres) squared. Overweight was defined as BMI ⩾23 kg/m2, and obesity BMI ⩾25 kg/m2, according to the Asian and Chinese criteria.21 We defined moderate and severe obesity as BMI ⩾28 kg/m2 and ⩾30 kg/m2, respectively.
Metabolic syndrome was defined according to the International Diabetes Federation (IDF) criteria:22 central obesity (waist circumference ⩾90 cm for men and ⩾80 cm for women) plus two or more of the following four factors: (1) raised concentration of triglycerides: 1.7 mmol/l or specific treatment for this lipid abnormality; (2) reduced concentration of HDL cholesterol: <1.03 mmol/l in men and <1.29 mmol/l in women or specific treatment for this lipid abnormality; (3) raised blood pressure: systolic blood pressure ⩾130 mm Hg or diastolic blood pressure 85 mm Hg or treatment of previously diagnosed hypertension; and (4) raised fasting plasma glucose concentration ⩾5.6 mmol/l or previously diagnosed type 2 diabetes.
Histological assessment
Percutaneous liver biopsy was performed using a 16G Temno needle. Liver histology was assessed by pathologists specialised in liver diseases (PC-LC, AW-HC) without knowledge of the clinical data. A liver sample was considered adequate if it was longer than 15 mm and contained six portal tracts or more. Liver fibrosis and necroinflammatory activity were evaluated semi-quantitatively according to the METAVIR scoring system as follows:23 F0, no fibrosis; F1, portal fibrosis without septa; F2, portal fibrosis and few septa; F3, numerous septa without cirrhosis; and F4, cirrhosis. METAVIR activity score was defined as: A0, none; A1, mild; A2, moderate; and A3, severe. Bridging fibrosis was defined as METAVIR fibrosis score of 3 or above, and liver cirrhosis as METAVIR fibrosis score of 4. Hepatic steatosis was graded from 0 to 3 according to the percentage of hepatocytes with steatosis: 0 (<5%), 1 (5–33%), 2 (>33–66%) and 3 (>66–100%).24
Liver stiffness measurement by transient elastography
LSM was performed using transient elastography (Fibroscan) according to the instructions and training provided by the manufacturer (EchoSens, Paris, France). Details of the technical background and examination procedure have been previously described.25 The LSM was considered reliable only if 10 successful acquisitions were obtained and the success rate was over 60%. The liver stiffness was expressed in kilopascals. A higher result reflected a stiffer liver and more severe liver fibrosis.
Definition of liver cirrhosis by liver stiffness measurement
From our recent studies validating the performance of LSM by liver histology in a cohort of 133 Chinese patients suffering from chronic liver diseases (of whom 50% suffered from CHB), a LSM cut-off value of 8.4 kPa was associated with high sensitivity (93%) and high negative predictive value (96%) for histological cirrhosis. On the other hand, a LSM cut-off value of 13.4 kPa was associated with high specificity (95%) and high positive predictive value (77%) for cirrhosis.26 The results were also validated in an algorithm of LSM involving 161 Chinese patients with CHB.27 Hence, “possible cirrhosis” was defined as a LSM cut-off value of 8.4 kPa, and “probable cirrhosis” as that of 13.4 kPa. In the present study, we prospectively validated these cut-off values in a subgroup of patients with liver biopsies performed.
Statistical analyses
Statistical analysis was performed by using the Statistical Package for Social Science (SPSS version 11.5). Continuous variables were expressed as the mean (standard deviation or median (range) as appropriate). Qualitative and quantitative differences between subgroups were analysed using the χ2 test or Fisher’s exact test for categorical parameters as appropriate, and the Student t test or Mann–Whitney test for continuous parameters as appropriate. Spearman’s rank correlation coefficient was used to analyse the correlations between LSM scores and the METAVIR fibrosis scores. The overall accuracy of LSM in diagnosing cirrhosis was calculated using the receiver operating characteristics (ROC) curve and its 95% confidence intervals (95% CIs). We conducted unadjusted and multivariate adjusted logistic regression analyses to determine if the presence of metabolic syndrome was associated with odds of liver cirrhosis. The multivariate adjusted logistic regression model included covariates that were associated with liver cirrhosis (p<0.10) and were input into the enter model. The effect of different components of metabolic syndrome on the development of liver cirrhosis was calculated as odds ratios and the 95% CI. All statistical tests were two-sided. Statistical significance was taken as p<0.05.
RESULTS
Patients
One thousand, five hundred and thirty-two patients with CHB were referred from different hospitals and clinics for LSM within the study period. On thousand, four hundred and sixty-six (96%) patients with reliable LSM were included for analysis. Nine hundred and thirty-nine patients (64%) were male and the mean age was 46 (SD 12) years. Mean BMI was 23 (SD 3) kg/m2. The baseline characteristics of patients are shown in table 1. The overall prevalence of metabolic syndrome was 13% (188/1466). The prevalence of metabolic syndrome increased with age (0%, 7%, 15% and 21% for patients of age 0–20, 21–40, 41–60 and >60 years, respectively, p<0.001; fig 1). Six hundred and five (41%) patients had central obesity, 196 (13%) had hypertriglyceridaemia, 256 (18%) had reduced HDL cholesterol level, 654 (45%) had high blood pressure, and 205 (14%) had impaired fasting glucose or diabetes. Three hundred and fifty-four (25%) patients and 393 (27%) were overweight and obese, respectively. Sixty-two (4%) patients were moderately obese, and 42 (3%) patients had severe obesity.

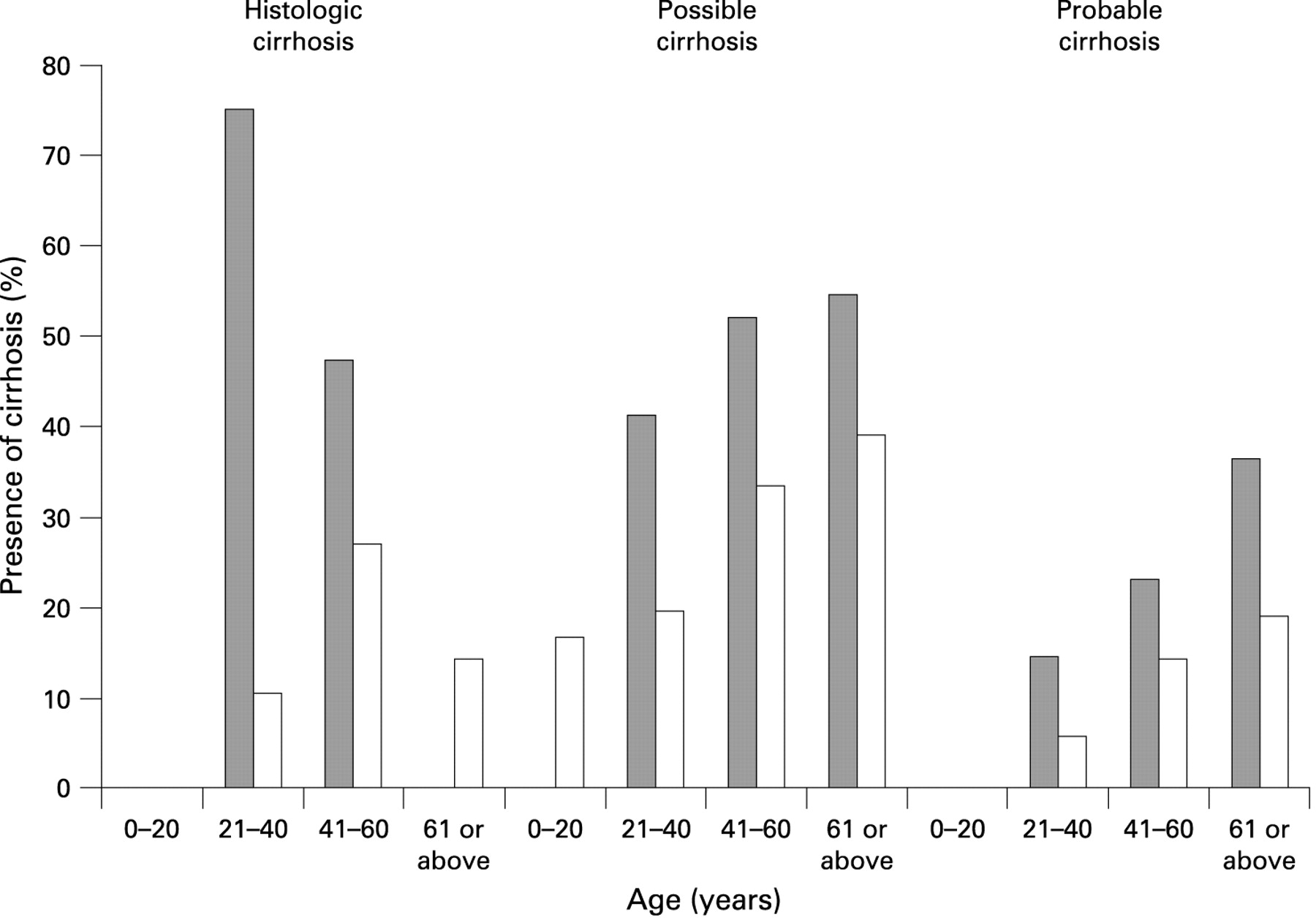
Possible cirrhosis was defined as liver stiffness measurement ⩾8.4 kPa; probable cirrhosis was defined as liver stiffness measurement ⩾13.4 kPa.
Effect of metabolic syndrome on liver histology
A subgroup of 167 patients underwent liver biopsy and 134 (80%) had adequate liver biopsy samples for histological assessment. The liver biopsy specimens were 19 (SD 4) mm in length containing 11 (SD 5) portal tracts. The inter-observer agreement was 0.93 for fibrosis staging and 1.00 for the presence of F3 fibrosis or above. Sixty-one (46%) patients had F3–4 disease (bridging fibrosis), and 32 (24%) had F4 disease (cirrhosis). The mean LSM score was 8.3 (SD 6.3) kPa. Correlation of LSM with METAVIR fibrosis score was good (r = 0.59, p<0.001). The area under the ROC curves of LSM for cirrhosis (F4 fibrosis) was 0.89 (95% CI, 0.83 to 0.94, p<0.001). The cut-off value of possible cirrhosis (8.4 kPa) was associated with high sensitivity (94%) and negative predictive value (97%) for cirrhosis (with specificity of 75% and positive predictive value of 54%). The cut-off value of probable cirrhosis (13.4 kPa) was associated with high specificity (94%) and positive predictive value (79%) for cirrhosis (with sensitivity of 69% and negative predictive value of 91%).
Histological liver cirrhosis, which was present in 24% (32/134) of patients whounderwent liver biopsy, was associated with male gender, higher BMI, greater waist and hip circumference, higher blood pressure, presence of metabolic syndrome, higher ALT and higher α-fetoprotein levels (table 1). The distribution of the histological liver cirrhosis across different age groups was 0%, 16%, 31% and 11% for patients of age 0–20, 21–40, 41–60 and >60 years, respectively. Liver cirrhosis was commoner among patients who had metabolic syndrome (p<0.001, fig 2). When the different components of metabolic syndrome were independently analysed, histological liver cirrhosis was associated with hypertension and diabetes mellitus. On the other hand, liver fibrosis was more severe in patients who had metabolic syndrome (median METAVIR fibrosis stage = 4) than those who did not have metabolic syndrome (median METAVIR fibrosis stage = 2, P = 0.002). Severity of steatosis (median Kleiner grade 1 vs 0, p<0.001, table 2), but not necroinflammation (median METAVIR Activity score 4 vs 4, p = 0.6), was also significantly more severe in patients with metabolic syndrome than those without. By logistic regression analysis, histological cirrhosis was independently and significantly associated with male gender, obesity (BMI⩾25 kg/m2), metabolic syndrome, and hypoalbuminemia (serum albumin<40 g/l, table 3).

{kind=link}
{kind=link}
Metabolic syndrome and risk of possible and probable cirrhosis
Four hundred and sixty-five patients (32%) had LSM ⩾8.4 kPa and were defined as possible liver cirrhosis (table 1). One hundred and eighty-seven (13%) patients had LSM ⩾13.4 kPa and were defined as probable liver cirrhosis. Patients who had possible and probable liver cirrhosis were predominantly male, older, had higher BMI and blood pressure. Metabolic syndrome and its components were more prevalent in patients with possible and probable cirrhosis. The prevalence of possible and probable cirrhosis was significantly higher in the presence of metabolic syndrome at different age groups (fig 2). Biochemically, cirrhotic patients had lower serum albumin, higher serum bilirubin, higher alkaline phosphatase and higher ALT. Their serum HBV DNA levels were also higher. On multivariate logistic regression analysis, the presence of metabolic syndrome, together with male gender, age >40 years, lower serum albumin, higher serum alkaline phosphatase and higher ALT were independently associated with both possible and probable cirrhosis (table 4). Other factors including obesity, serum total bilirubin and serum HBV DNA level did not have a consistent effect on the risk of possible and probable cirrhosis.
Patients with more components of metabolic syndrome according to the IDF criteria were at higher risk of cirrhosis. The ORs for development of possible and probable cirrhosis had an increasing trend with increasing numbers of components of metabolic syndrome (table 5). The risk of histological liver cirrhosis did not show a consistent increasing trend, probably due to relative small numbers of patients in all groups (table 5).
DISCUSSION
In this study, we have demonstrated that metabolic syndrome was strongly associated with increased risk of severe fibrosis and cirrhosis in patients with CHB. There may be additive effect of individual different components of metabolic syndrome on the risk of liver cirrhosis. To our knowledge, this is the first prospective population-based study reporting the association of metabolic syndrome, using recently proposed Asian-specific definitions, with liver cirrhosis in CHB. The increased risk found in the study was independent of other important and well-studied risk factors such as age, gender, ALT levels, HBV DNA, and HBeAg status.2 3
Our findings echoed the results from a recent study involving 317 patients suffering from chronic viral hepatitis (95 and 176 patients suffering from chronic hepatitis B and C, respectively) and non-alcoholic fatty liver disease (NAFLD).28 An independent association of metabolic syndrome with severe fibrosis was noted in both chronic viral hepatitis and NAFLD. This study was limited by the heterogeneous patient population in which a minority suffered from CHB. The relatively small number of patients with CHB also did not allow any meaningful statistical adjustment of the potential confounding factors for liver cirrhosis.
The underlying mechanism of the progression of fibrosis in relation to metabolic syndrome could be a direct stimulation of liver stellate cells by hyperinsulinaemia and hyperglycaemia, resulting in increased production of the connective tissue growth factor and subsequent accumulation of extracellular matrix.29 Mechanisms linking steatosis and liver fibrosis are probably related to the oxidative stress generated from fat accumulation within hepatocytes, with subsequent secretion of inflammatory cytokines and activation of stellate cells.30 These processes may contribute to further hepatic injury from other common factors such as hepatitis B virus.31 However, metabolic syndrome but not steatosis was independently associated with liver cirrhosis in our cohort. One possible hypothesis would be insulin resistance as the major driving force for liver fibrosis progression. This would be in line with evidence from patients with CHC, as previous studies found that steatosis was not associated with severe liver fibrosis.32 33 On the other hand, hepatitis B virus does not seem to induce insulin resistance, as insulin resistance was more frequent in patients with CHC than in a group of matched patients with CHB.17
The prevalence of metabolic syndrome in this cohort was 13%. This was comparable with the results of a recent cross-sectional study of 7473 subjects, in which the age-standardised prevalence of metabolic syndrome was 13.9% in Hong Kong.34 Recent surveys across the Asia–Pacific region showed a consistent increase in the prevalence of metabolic syndrome.35 As CHB is also highly prevalence in the Asia–Pacific region, the additive effect of metabolic syndrome and CHB on liver fibrosis poses significant risk on patients suffered from both conditions. Early recognition and management of metabolic syndrome in CHB patients may have a positive effect in the long term. Lifestyle modifications including physical activity,36 weight loss21 and diet37 38 favourably affect the various components of metabolic syndrome, at least in the short term. These lifestyle modifications may have potential therapeutic or preventive role for liver fibrosis in CHB patients, particularly in CHB patients suffering from metabolic syndrome. The treatment strategies for CHB patients might also be altered by the presence of metabolic syndrome because of the increased risk of cirrhosis. A lower threshold for initiating anti-viral therapy might be considered.
The use of transient elastography, a validated and non-invasive tool to diagnose liver cirrhosis, has enabled us to investigate the effect of metabolic syndrome in a general CHB population. This has been a no-man’s-land in the past when liver biopsy was the only tool for the assessment of fibrosis but was deemed not ethical and feasible for a large number of patients with relatively normal liver function tests. Transient elastography also has the theoretical advantage of measuring a volume of liver tissue at least 100 times larger than a biopsy sample, even though liver biopsy is still the “gold standard” for the assessment of liver fibrosis.39 In this study, the use of transient elastography has been internally validated by liver histology and two LSM cut-off values were to use define possible and probable cirrhosis to improve the reliability of our results.26 In the present study, 4% of patients were excluded from analysis due to failed LSM, while 91.4% and 99.0% of patients with and without central obesity have reliable LSM results, respectively. Most previous studies of transient elastography reported a failure rate of 5–8% due to obesity and other reasons,18 19 and these patients were more likely have high BMI and central obesity. Hence central obesity might pose a potential limitation for the use LSM to detect metabolic syndrome in patients with fatty liver disease. We expect the failure rate of LSM among Caucasian patients who are in general more obese than Asians may be higher.
There were some differences between the factors associated with histological cirrhosis and cirrhosis diagnosed with LSM. One major difference was that the serum ALT level was found independently associated with LSM but not histological cirrhosis. It might be due to the larger sample size of LSM such that there was enough power to detect the difference. Another possibility would be higher LSM was partly related to hepatic necroinflammation. Two recent studies showed that the degree of fibrosis evaluated by transient elastography could be over-estimated in the presence of hepatitis exacerbations.40 41 However, unlike patients from these two studies, the majority of the patients in the current study had normal or only mildly elevated ALT. We and other investigators have demonstrated that the use of a high LSM cut-off value may ensure a high specificity of liver cirrhosis for patients with mildly elevated ALT levels.26 42
Our study has a few other limitations. First, most of the patients of our study were referred from specialists and might represent a more severe end of the disease spectrum. The prevalence of liver cirrhosis might be an over-estimate of the general population. Nonetheless, 39% of our patients had HBV DNA fewer than 10 000 copies/ml and 66% of our patients had normal ALT levels. We believe our results can be generalised to other CHB patients either under the care of hepatology specialists or general practitioners. Second, this was a cross-sectional study such that most patients were assessed for once at a snapshot. Although the severity of liver fibrosis may change with time, we believe the potential bias of disease fluctuation can be partly compensated by the large number of patients studied. Third, transient elastography was used instead of liver biopsy as the standard for liver cirrhosis. Although transient elastography has been widely validated, most patients in the previous studies were suffering from CHC instead of CHB.18 19 Hence we included a cohort of 134 patients with histological proof from liver biopsy to internally validate this tool and the LSM cut-off values used in this study have been previously validated.26 27 Last, we lacked information on the ultrasonography evidence of fatty change for analysis. Nonetheless, ultrasonography can only pick up fatty change when there is more than 33% fat on histology and it is not a very sensitive measure for fatty liver disease.43
In summary, our large-scale cross-sectional study has clearly shown that metabolic syndrome is independently associated with liver cirrhosis in CHB. Hence, hepatology specialists or general practitioners caring for patients with CHB should proactively look for the evidence of metabolic syndrome and its components, apart from the standard investigations and monitoring for the disease. As patients with CHB and metabolic syndrome are more likely to harbour early cirrhosis, diagnostic work-up for cirrhosis is warranted in these cases because of the important therapeutic and surveillance implications. Future studies are warranted to assess the benefit of therapy for metabolic syndrome among patients with CHB.
REFERENCES
Footnotes
Competing interests: FK-LC received an independent research grant and a consulting fee from Pfizer and was paid lecture fees by TAP Pharmaceuticals. JJ-YS received consulting fees from the National Health Research Institutes of Taipei, The Hong Kong Police Force, Lippincott Williams & Wilkins, and the Hong Kong College of Physicians and was paid lecture fees by AstraZeneca Hong Kong Ltd, GSK Pharmaceuticals International, and the American Society for Gastrointestinal Endoscopy. HL-YC is a member of the advisory boards of Novartis Pharmaceutics, Bristol-Myers Squibb and Schering-Plough. The other authors do not have any competing interests.
Ethics approval: The study protocol was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee, on 21 June 2006.
Linked Articles
- Digest