Article Text

Abstract
Patients with gastro-oesophageal reflux disease (GORD) who are not responding to proton pump inhibitors (PPIs) given once daily are very common. Various underlying mechanisms have been shown to contribute to the failure of PPI treatment. These include weakly acidic reflux, duodenogastro-oesophageal reflux, residual acid reflux and functional heartburn, as well as others. Diagnostic evaluation of patients with GORD who have failed PPI treatment may include an upper endoscopy, pH testing and oesophageal impedance with pH monitoring. Commonly, doubling the PPI dose or switching to another PPI will be pursued by the treating physician. Failure of such a therapeutic strategy may result in the addition of a transient lower oesophageal sphincter reducer or pain modulator. Anti-reflux surgery may be suitable for a subset of carefully studied patients.
Statistics from Altmetric.com
It has been estimated that between 10% and 40% of patients with gastro-oeophageal reflux disease (GORD) fail to respond symptomatically, either partially or completely, to a standard dose proton pump inhibitor (PPI).1–4 During a period of only 7 years (1997–2004), there was an increase by almost 50% in the usage of at least double-dose PPIs in patients with GORD.5 Additionally, it appears that less than 50% of patients with GORD are satisfied with their medical treatment, and only 58% of those receiving PPIs report a high level of satisfaction with it.3
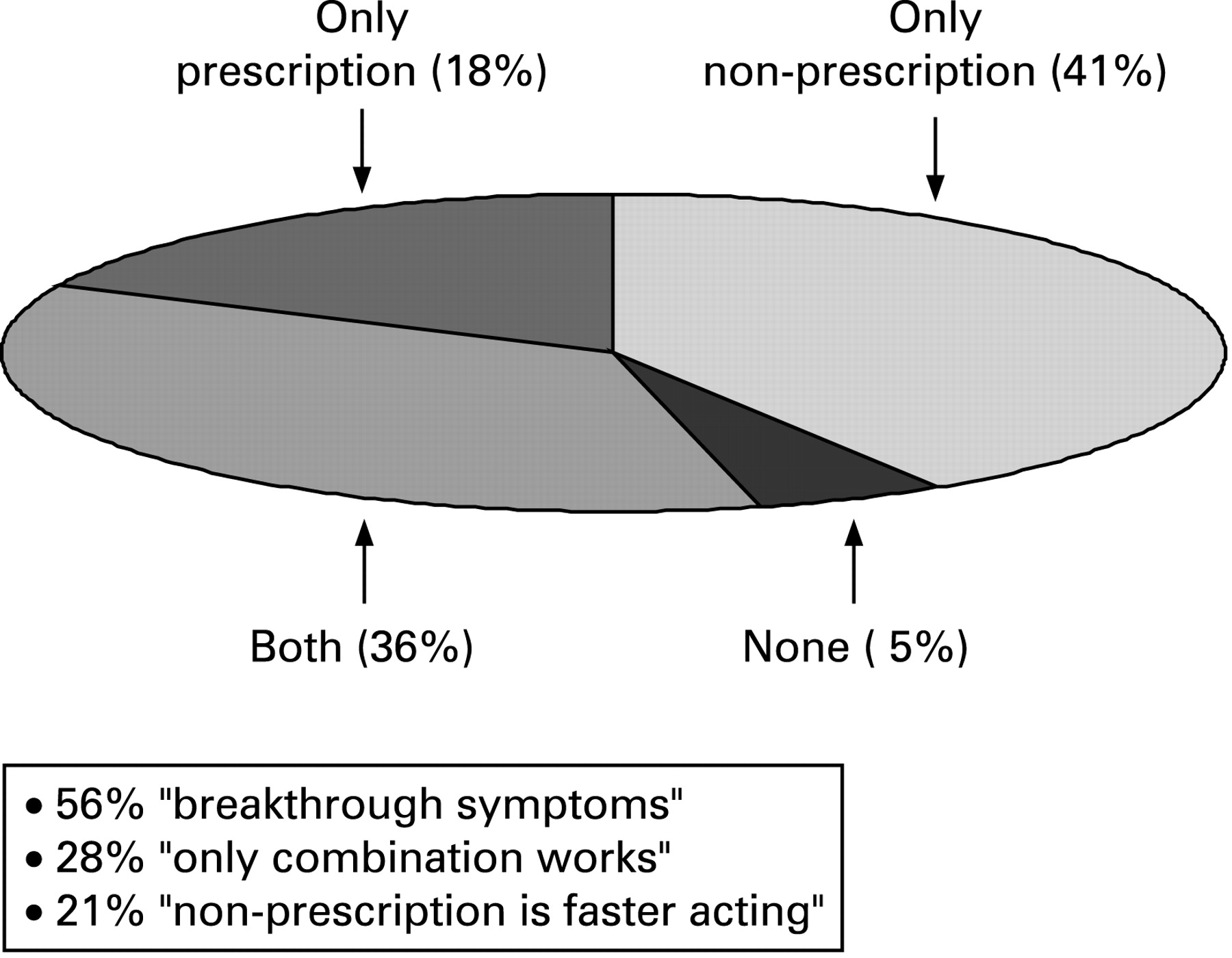
In the 2000 Gallup Study of Consumers’ Use of Stomach Relief Products, 36% reported taking non-prescription medication in addition to a prescription medication for GORD (fig 1).4 Of those, 56% stated that they use their prescription medication daily but still need to supplement it with non-prescription medication for breakthrough symptoms. Interestingly, 28% stated that only the combination of prescription and non-prescription medications relieves their symptoms, and 24% reported that prescription medication works better in the long run but non-prescription medication is faster acting.
Failure of the PPI treatment to resolve GORD-related symptoms has become the most common presentation of GORD in gastrointestinal (GI) practice. Commonly, physicians will escalate the PPI dose in GORD non-responders many times beyond any added efficacy (three or more times a day). This is the result of a “knee jerk” approach to the complaints of these highly challenging patients instead of proper identification of the underlying mechanisms that result in lack of response to PPI treatment. Unfortunately, as more PPIs become generic or available over the counter, PPI dose escalation is likely to become even more prevalent in the treatment of refractory GORD.
Whilst cost analysis of PPI failure has yet to be carried out, it is likely an expensive clinical problem due to repeated utilisation of healthcare resources such as clinic visits, diagnostic tests and prescription medications.4
Most of the patients with GORD who are not responsive to PPIs originate from the groups with non-erosive reflux disease (NERD) and functional heartburn, primarily due to the relatively large size of such groups among the patient population with heartburn (up to 70%) and low response rate to PPIs once daily (pooled symptomatic response rate to PPIs once daily at 4 weeks is only 37% for patients with NERD).5 6 In contrast, patients with erosive oesophagitis account for only 30–40% of the GORD population, and their symptom response rate is significantly higher than has been reported in patients with NERD (pooled symptomatic response rate to PPIs once daily at 4 weeks is 56%).5
Patients with normal endoscopy and normal pH testing exhibit the lowest symptom response rate to PPIs once daily when compared with NERD patients. In one study, only 45% of these patients reported sufficient relief of heartburn symptoms when compared with NERD patients after 4 weeks of treatment with a PPI once daily.7 In addition, it appears that patients with NERD, with only mildly abnormal oesophageal acid exposure (per cent total time pH<4; range, 4.2–9.9%), who account for most patients with NERD, also exhibit a relatively lower symptom response rate to PPI once daily as compared to NERD patients with moderate exposure to acid reflux (per cent total time pH<4 greater than 10% or patients with erosive oesophagitis) (fig 2).

The prevalence of Barrett’s oesophagus is 6–12% of all patients who present for endoscopy with GORD-related symptoms and 0.25–3.9% in unselected cases undergoing upper endoscopy.6 Most patients with Barrett’s oesophagus report sufficient symptom control on PPIs once to twice daily.9 This is despite the fact that up to 50% of the patients continue to have abnormal oesophageal acid exposure during pH testing.8 9 Overall, due to the small number of patients with Barrett’s oesophagus and their relatively good symptomatic response to PPIs, it is unlikely that this group of patients contributes significantly to the PPI failure phenomenon.
What constitutes refractory GORD remains an area of controversy. Most investigators believe that only patients with GORD who exhibit partial or lack of response to PPIs twice daily should be considered as PPI failures. However, we suggest that lack of satisfactory symptomatic response to a PPI once a day is sufficient to consider patients as PPI failures. The latter definition is much more relevant to pharmaceutical companies and third-party payers, because there is no GORD-related indication for PPIs twice a day. Furthermore, it is unclear what symptom burden during PPI consumption fulfils the definition of refractory GORD. This is likely to vary from one patient to another. Because refractory GORD is a patient-driven phenomenon, patients who are PPI failures and who seek medical attention will exhibit a different frequency and/or severity of GORD-related symptoms. Consequently, any attempt to narrow the definition of refractory GORD might exclude many true sufferers.10
UNDERLYING MECHANISMS FOR REFRACTORY GASTRO-OESOPHAGEAL REFLUX DISEASE
Presently, much of the research that is conducted in the area of refractory GORD focuses primarily on weakly acidic reflux, duodenogastro-oesophageal reflux, and oesophageal hypersensitivity. However, it is highly likely that GORD symptoms due to weakly acidic or duodenogastro-oesophageal reflux in patients who failed PPI treatment are related to oesophageal hypersensitivity. Figure 3 depicts the proposed underlying mechanisms for persistent heartburn despite PPI treatment.

Compliance
Several surveys have demonstrated that poor compliance with PPI treatment is not uncommon among patients with GORD. By the end of 1 and 6 months of PPI therapy, 55% and 30% of these patients, respectively, still consume their PPI once daily as initially instructed. In a large, population-based study, the authors demonstrated that the main factors influencing compliance were the presence or absence of symptoms, the severity of symptoms, and a personal preference about when to take treatment.11 The results of this study clearly demonstrate that GORD is a symptom-driven disease in which patients adhere to treatment instructions as long as they experience symptoms. Other general factors that affect compliance, such as knowledge about the treated disorder, desire for personal control, the prescribed drug (eg, taste, consistency), side effects, number of pills per day, concomitant therapies, age, personality, socioeconomic status, and healthcare coverage may also play a role in adherence to treatment instructions.12 Compliance should be assessed in all patients with GORD who report lack of response to PPI treatment, particularly prior to ordering any evaluative test. Unfortunately, a subset of patients may not disclose that they are poorly compliant during their clinic visit. Treating physicians should repeatedly emphasise the need to consume anti-reflux treatment on a daily basis. It is the role of the treating physician to ensure proper compliance with the prescribed PPI through patient education about the disease and the value of compliance with treatment.12
Dosing time
In addition to compliance, patients need to be evaluated for proper consumption of the PPIs because timing and frequency of dosing are critical for maximum efficacy of the medication. PPIs should be taken 30 min prior to a meal. In one study, the authors demonstrated significantly better control of gastric pH when omeprazole or lansoprazole were taken 15 min before breakfast versus without breakfast.13 Patients’ preferences and lack of physicians’ clear instructions on how to consume PPIs are commonly to blame. Gunaratnam et al14 found that out of 100 patients with persistent GORD symptoms on PPIs, only 46% dosed optimally.14 Of those who dosed sub-optimally, 39% consumed their PPI at bedtime and 4% as needed. In the 2000 Gallup survey, consumption of anti-reflux medications prior to going to bed was reported by 52% of the subjects.4 However, there is no clear evidence thus far that restoring adequate PPI dosing time improves the symptoms of patients with GORD. Despite the latter argument, most authorities emphasise the need to ensure that these patients, especially those who report refractory GORD, dose their PPIs optimally.
Weakly acidic or alkaline reflux
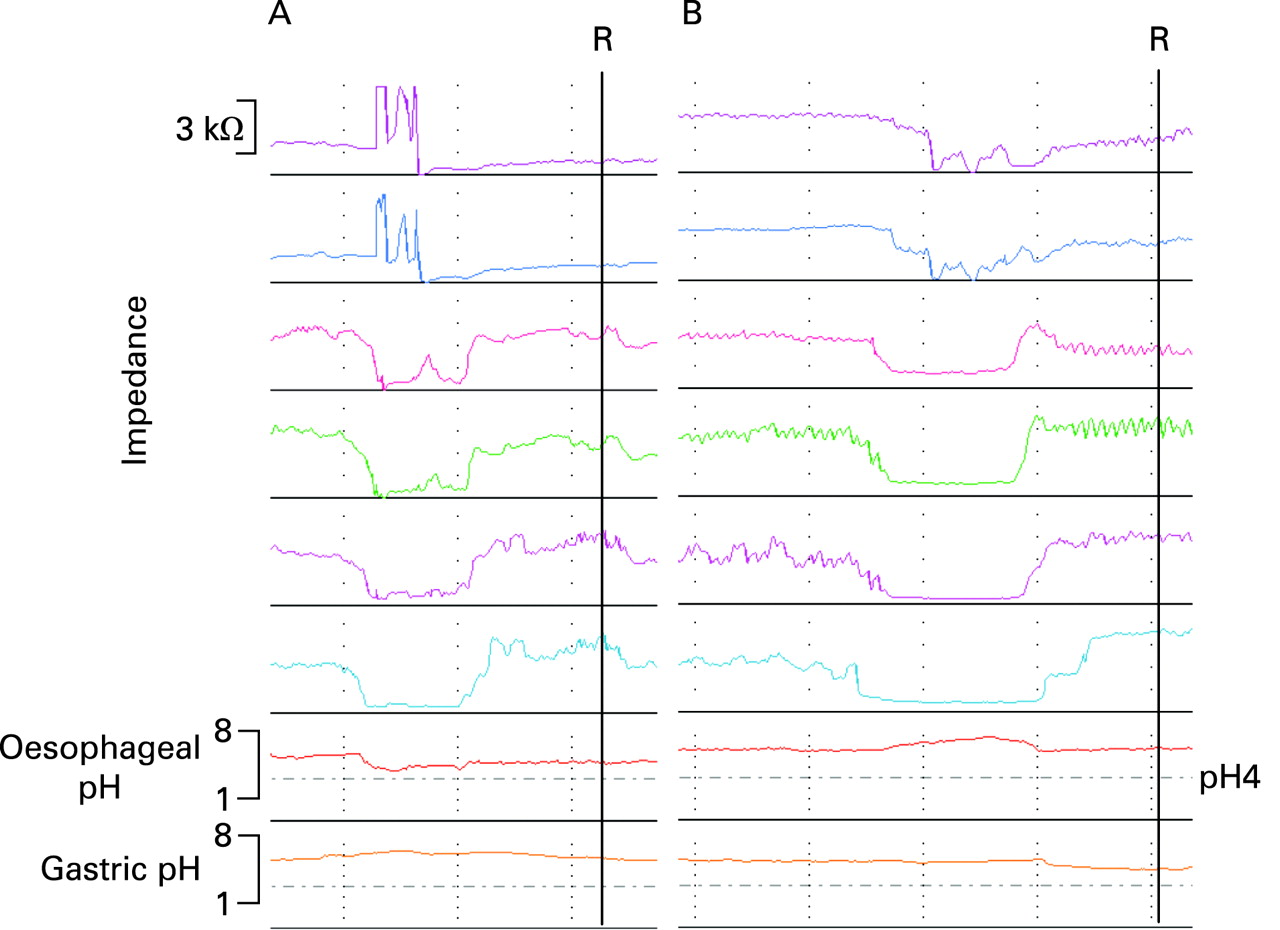
Studies have suggested that persistent typical and atypical GORD symptoms on PPIs might be due to less acidic or non-acidic reflux. Impedance–pH monitoring allows the detection of most reflux events and the distinction between acidic, weakly acidic and weakly alkaline reflux (fig 4).15
The first stationary, postprandial impedance–pH study in patients on PPI twice-daily therapy documented a profound decrease in the amount of acid reflux but with continuing postprandial reflux of weakly acidic nature. Heartburn was replaced by regurgitation, which became the predominant symptom in these patients who failed PPIs twice daily.16 Further studies using ambulatory 24 h impedance–pH monitoring in patients with refractory GORD showed that acid reflux (incomplete acid inhibition by PPIs) was associated with 7–28% of the persistent symptoms. In contrast, weakly acidic reflux preceded 30–40% of the GORD-related symptoms. About 30–60% of the GORD-related symptoms were not preceded by any reflux.17–19
A large multicentre study, using impedance–pH monitoring in 168 refractory GORD patients, showed that 11% of them had a positive symptom index (SI) for acid reflux and 37% had a positive SI for non-acid reflux.18 Similar results were obtained by Zerbib and colleagues who evaluated 71 patients on PPI treatment.19 In this study the authors performed impedance–pH monitoring in a group of patients off PPIs and in another group of patients on PPIs. In patients off PPIs, impedance–pH monitoring adds little value to the diagnostic yield when compared with pH recording alone (5–10%). In patients on PPI therapy, however, adding impedance to pH monitoring improves the diagnostic yield by 15–20% and allows better symptom analysis than the pH test alone.19
In contrast a very recent study by Hemmink et al20 compared the yield of impedance–pH monitoring performed off and on PPIs in patients with refractory GORD. The authors conclude that impedance–pH monitoring should be performed off PPIs because this approach offers the best chance to assess the relationship between symptoms and reflux episodes.
Impedance–pH monitoring in refractory GORD patients while on PPI therapy may also include continuous gastric pH measurements. In this way, one single test can provide information about the extent of gastric acid inhibition, occurrence of nocturnal acid breakthrough (NAB), and temporal association between symptoms and gastro-oesophageal acidic or weakly acidic reflux. However, the role of nocturnal acid breakthrough in refractory heartburn is unclear. Peghini et al21 reported that 75% of all individuals (patients with GORD as well as healthy subjects) on double-dose PPIs demonstrate gastric pH<4 for at least 1 h during the night. However, there is very little evidence for a temporal relationship between NAB and reflux-related symptoms.22 Nzeako and Murray et al23 showed that 71% of the patients with GORD who failed treatment with PPIs twice daily experienced NAB, but only 36% had a correlation between symptoms and NAB.
The mechanism by which weakly acidic reflux causes GORD-related symptoms remains poorly understood. Two possible explanations have been proposed (ie, oesophageal distension by increased reflux volume and hypersensitivity to weakly acidic refluxate). Thus far, there is no evidence that weakly acidic reflux is more commonly associated with increased volume of the refluxate than acidic reflux. Although this association has been proposed, oesophageal impedance is unable to measure volume and thus substantiates this claim. Recently, several studies have demonstrated that proximal extent of weakly acidic reflux (a possible indirect marker of reflux volume) was the most important determinant of symptomatic reflux events in patients who failed PPI treatment.24 25 However, these studies also showed a considerable overlap in the proximal extent of symptomatic and asymptomatic weakly acidic reflux episodes. Consequently, it is impossible to determine individual thresholds for the point at which weakly acidic reflux episodes consistently provoke symptoms.
Tutuian et al25 have shown that, in addition to proximal extent, reflux episodes that were associated with symptoms in patients who failed PPI twice daily, were primarily composed of both gas and liquid. A preliminary study suggested that the transition zone between the striated and smooth muscle in the oesophagus is more sensitive to mechanical stimulus than the distal oesophagus, which is composed solely of smooth muscle.26 These findings may explain why proximal migration of reflux is more likely to elicit symptoms.
Thus far, studies have shown that impedance–pH monitoring increases the sensitivity for the detection of reflux-related persistent symptoms (eg, heartburn, regurgitation and cough) in patients on PPI therapy.27 The causal role of weakly acidic reflux, as detected by impedance, in the generation of refractory heartburn needs to be further studied.
Duodenogastro-oesophageal reflux/bile reflux
Although commonly considered as a synonym, bile reflux and non-acid reflux are completely different phenomena. Previous studies suggested that bile reflux probably accounts for only 10–15% of non-acid reflux. A recent study using simultaneous Bilitec and impedance monitoring showed no correlation between the per cent time of bilirubin absorbance and non-acid reflux parameters.28 The majority of bile reflux occurs concomitantly with acid reflux events, and it is believed that acid rather than bile is the dominant factor responsible for GORD symptoms.29–31
Experimental data, however, support a role for persistent bile acids in the refluxate as a potential factor involved in refractory heartburn. Although PPI therapy reduces the occurrence of both acid as well as bile reflux,32 33 it has been shown that complete acid suppression does not guarantee elimination of duodenogastro-oesophageal reflux (DGOR).34 Perfusion of bile salts with non-acidic pH can still provoke heartburn,35 and exposure of rabbit oesophageal mucosa to weakly acidic solutions containing bile acids (comparable situation to patients on PPIs), increases mucosal permeability and induces dilated intercellular spaces (DIS), a proposed histopathological mechanism necessary for the sensation of heartburn.36
A recent study by Tack et al37 suggested a possible role for DGOR in both symptoms and erosive oesophagitis in a subset of patients with difficult to manage, symptomatic reflux. In a study that included 65 patients with persistent heartburn and regurgitation while on single-dose PPI therapy, the authors demonstrated a significant number of symptoms that occurred in association with bile reflux as measured by Bilitec. Furthermore, in a carefully selected group of patients with symptoms refractory to PPI therapy, baclofen 20 mg three times a day significantly reduced the DGOR exposure as well as symptoms of heartburn. Based on these studies, the use of Bilitec may be justified in patients with persistent reflux symptoms despite PPI therapy. However, the technique is not commonly available for the practising physician and is presently limited to less than a handful of centres with interest in GI motility. In addition, patients have to follow specific dietary restrictions during the test.
Oesophageal hypersensitivity
The role of oesophageal hypersensitivity has not been specifically studied in patients who failed PPI treatment. However, most patients who do not respond to PPI therapy have NERD or functional heartburn.4 5 Approximately 50% of the GORD patients with normal endoscopy demonstrate normal oesophageal acid exposure.38 Heartburn patients, those with a negative symptom index reported having heartburn at pH<4 only 12.7% of the time as compared with 70.7% of the time in those with a positive symptom index, despite a similar mean number of heartburn episodes.38 Patients having heartburn with normal endoscopy and pH testing have consistently demonstrated lower perception thresholds for pain as compared to patients from the different phenotypes of GORD when using either oesophageal balloon distention or electrical stimulation. A recent study by Emerenziani et al39 showed that in heartburn patients with normal endoscopy and pH testing, the risk of reflux perception was significantly higher when gas was present in the refluxate. These patients are also more sensitive to less acidic reflux than oesophagitis patients. Furthermore, objective neurophysiological measures of oesophageal-evoked potential latency revealed that pH-negative NERD patients achieve equivalent latency and amplitude oesophageal-evoked potential responses with reduced afferent input, suggesting heightened oesophageal sensitivity.40 In contrast, stimulus response functions to oesophageal acid perfusion in heartburn patients with normal endoscopy and pH testing demonstrated a more mixed response, which resulted in higher mean value for time to heartburn symptoms and lower mean values for intensity and acid perfusion sensitivity score compared with patients with NERD and abnormal pH test.41 A quarter of the patients had a negative acid perfusion test. This study further supports the hypothesis that pH-negative NERD is composed of a heterogeneous group of patients. However, a significant subset of these patients is unlikely to have gastro-oesophageal reflux as the underlying stimulus for their heartburn.
Most patients in whom symptoms are associated with weakly acidic reflux do not have an increased number of reflux events, suggesting hypersensitivity of the oesophagus to less acidic refluxate.17 Furthermore, none of the studies thus far which assessed the extent and relationship between weakly acidic reflux and GORD-related symptoms, using oesophageal impedance, compared PPI failure to PPI success patients. There is no obvious reason why PPI success patients will demonstrate fewer episodes of weakly acidic reflux than those who failed PPIs. In patients who failed PPIs twice daily, Vela et al16 were clearly able to show that acidic reflux almost completely disappeared. Consequently, a similar reflux pattern in PPI success patients would be expected. If the frequency of weakly acidic reflux is similar between PPI success and PPI failure patients, then PPI failure is an oesophageal-hypersensitivity phenomenon to weakly acidic reflux.
A recent impedance–pH study in refractory patients while on PPI therapy showed that up to 68% of remaining heartburn episodes were associated with weakly acidic reflux.24 High proximal extent of the refluxate was the only important factor associated with reflux perception, suggesting an increased sensitivity of the proximal oesophagus in this group of patients. Furthermore, as compared with regurgitation, weakly acidic reflux episodes resulting in heartburn were more frequently pure liquid, slightly more acidic, had a lower nadir pH (4.8 vs 5.5), and were more commonly associated with preceding acid reflux episodes. These results suggest that perception of heartburn denotes a higher sensitivity to the chemical composition of the refluxate than in the case of regurgitation.
The Rome III Committee for Functional Gastrointestinal Disorders defined functional heartburn as episodic retrosternal burning in the absence of GORD, histopathology-based motility disorders or structural explanations.42 Unlike Rome II criteria for functional heartburn, Rome III added that symptoms related to acid reflux events in the absence of abnormal oesophageal acid exposure are now excluded from the diagnosis of functional heartburn. Furthermore, to meet functional heartburn criteria, patients with a negative symptom–reflux association should also have to demonstrate unsatisfactory response to a PPI trial. However, Rome III does not provide a clear definition of what constitutes a PPI trial (eg, dosing, duration) Most experts suggest that patients who failed to respond symptomatically to PPIs twice daily and demonstrate lack of any association between their GORD-related symptoms and a reflux event (acidic, weakly acidic or weakly alkaline) should be considered as having functional heartburn.43 44
Studies evaluating patients who did not respond to PPIs twice daily demonstrated that up to 58% of them have functional heartburn.18 45 Thus, functional heartburn is the most common cause for failure of PPI treatment. The underlying mechanisms for symptoms in functional heartburn patients as defined by Rome III remained to be elucidated. Thus far, studies used the outdated Rome II criteria to diagnose functional heartburn. Many of these studies demonstrated increased oesophageal sensitivity to chemical, mechanical and electrical stimuli35 41 46 47 in this patient population. However, the study by Shapiro et al41 suggested that not all functional heartburn patients (based on Rome II) have increased oesophageal sensitivity to intraluminal stimuli, and it is highly likely that functional heartburn represents a heterogeneous group of patients with different underlying mechanisms for their symptoms.
Residual acid reflux
Residual acid reflux has been documented in GORD patients with persistent heartburn despite PPIs once or twice daily. In one study, 38.6% of patients with GORD undergoing pH testing for persistent symptoms, while receiving standard dose PPIs once a day, had an abnormal test.48 There was no correlation between a negative pH test and age, gender, or brand of PPI. In another study, 31% and 4% of GORD subjects with refractory symptoms who underwent pH testing on PPIs once daily or twice daily, respectively, had an abnormal test.49 Recently, Karamanolis et al50 demonstrated that 16% and 32% of the symptomatic subjects on double dose and standard dose PPIs, respectively, had abnormal pH tests.50 Positive symptom index with an acid reflux event was noted in 40% and 7–11% of patients who remained symptomatic on PPIs once daily51 or twice daily,18 45 respectively.
Nocturnal acid breakthrough
Nocturnal acid breakthrough (NAB) has been defined as the presence of gastric pH<4 for at least 1 h during the night in patients with persistent heartburn on standard dose PPIs twice daily.20 It has been suggested that this gastric physiological phenomenon causes failure of PPI treatment by promoting gastro-oesophageal reflux during sleep. Presently, sleep is considered the most vulnerable period of time for the development of oesophageal mucosal injury due to reflux, primarily because of reduction in swallows and saliva production.52 53 However, early reports about NAB did not attempt to demonstrate a correlation between this gastric phenomenon and night-time GORD symptoms. Subsequent studies have shown that NAB events do not necessarily denote a temporal relationship with reflux-related symptoms.54 Furthermore, 71% of patients with GORD who did not respond to treatment with PPIs twice daily experienced NAB, but only 36% showed a correlation between symptoms and NAB events.22 Moreover, there is no relationship between NAB and nocturnal heartburn.21 Thus far, accumulating data do not support a significant role for NAB in precipitating the failure of PPI treatment.
Psychological co-morbidity
Patients with poor correlation of symptoms with acid reflux events display a high level of anxiety and hysteria as compared with patients who demonstrate a close correlation between symptoms and acid-reflux events.56 Anxiety and depression have been shown to increase GORD-related symptoms reported in population-based studies. Thus, it has been proposed that patients who did not respond to PPI treatment are more likely to have psychosocial co-morbidity than are those who were successfully treated with PPIs. A recent study demonstrated for the first time that patients who responded less well to PPI treatment were more likely to experience psychological distress.55
Eosinophilic oesophagitis
Dysphagia, sometimes presenting as acute food impaction, is almost always present in patients with eosinophilic oesophagitis. In contrast, only about a third (range, 10–43%) of these patients also report classic heartburn symptoms.57–62 It is very uncommon for patients with eosinophilic oesophagitis to report heartburn as the sole symptom. The relationship between eosinophilic oesophagitis and GORD is unknown, although a recent study ruled that acid or non-acid reflux is a significant contributor to the pathogenesis of eosinophilic oesophagitis.63 An overlap between eosinophilic oesophagitis and GORD has also been proposed where both disorders coincide in the same individual.64 Regardless, eosinophilic oesophagitis is a relatively uncommon disorder and is thus unlikely to be responsible for a significant portion of those who do not respond to PPI treatment. Moreover, the prevalence of eosinophilic oesophagitis in GORD patients unresponsive to PPIs is still unknown.
Miscellaneous
An area that has been scarcely studied is the relationship between refractory GORD and the presence of gastroparesis. A recent study has demonstrated that botulinum toxin injection of the pylorus in GORD patients with gastroparesis and failure to respond to PPI treatment significantly improved their symptoms, albeit for a short time.46
In one study, patients with GORD who also suffered from irritable bowel syndrome (IBS) perceived their symptoms as more severe and tended not to achieve the same degree of symptom improvement during PPI treatment as compared with patients with GORD who do not suffer from IBS.55
Other potential underlying mechanisms, such as reduced PPI bioavailability, rapid PPI metabolism and, specifically, mutations in the 2C19 isoform of cytochrome p450, PPI resistance, and Helicobacter pylori status have all been shown to play a limited role in PPI failure. Pill-induced oesophagitis, skin diseases with oesophageal involvement, Zollinger–Ellison syndrome, and achalasia are very unusual causes for PPI failure and are rarely confused with GORD alone.65 Additionally, there are no data to support an important role for these oesophageal disorders in precipitating lack of response to PPIs in patients with GORD.
DIAGNOSTIC OPTIONS
Management of a patient with refractory GORD requires a high level of certainty about the initial diagnosis of GORD which prompted the PPI treatment.66 It is necessary to determine whether the diagnosis of GORD was based solely on symptoms (subjective findings) or if other objective tests, such as upper endoscopy or pH testing, were used. Additionally, it is helpful to know if patients have erosive oesophagitis, NERD or functional heartburn. Box 1 summarises the currently available diagnostic techniques for refractory heartburn.
Upper gastrointestinal endoscopy
The value of upper endoscopy in patients who failed PPI treatment has been scarcely studied. Overall, it appears that most of these patients have normal endoscopy.67 In patients with refractory GORD, the sensitivity of endoscopy in demonstrating GORD-related findings is low due to the predominance of NERD in this group of patients and the excellent efficacy of PPIs in healing erosive oesophagitis. Studies have demonstrated that the healing rates of erosive oesophagitis in patients receiving standard dose PPIs range from 75% to 95%.68 69 In general, endoscopic healing of erosive oesophagitis is commonly accompanied, although not always, by symptom relief. Therefore, persistence of symptoms despite PPI treatment may reflect failure in healing oesophageal mucosal injury, particularly in those with more severe grades of erosive oesophagitis.
It must be kept in mind that a recent use of PPIs may mask the presence of mucosal injury prior to initiation of anti-reflux treatment. Hetzel et al68 showed that 80% of the patients with reflux oesophagitis recur after 6 months of interruption in omeprazole treatment. However, the rate of erosive oesophagitis recurrence after a shorter period of PPI cessation remains unknown.
In patients with refractory GORD, endoscopy can reveal an alternative diagnosis, which could explain patient symptoms. For example, refractory oesophagitis might be the result of Zollinger–Ellison syndrome, pill-induced oesophagitis, and skin diseases with oesophageal involvement.67 Moreover, eosinophilic oesophagitis and persistent gastric or duodenal ulcer can be identified.
Even if conventional endoscopy is normal, refractory heartburn might still be due to microscopic oesophageal mucosal abnormalities. Patients may prove to have minimal changes in the distal oesophagus related to GORD by using specialised techniques such as magnification endoscopy.70 Similarly, these patients might have abnormalities during histological examination of oesophageal biopsies such as dilated intercellular spaces (DIS).71
Oesophageal biopsies and dilated intercellular spaces
Oesophageal histology has been proposed to improve detection of GORD. Basal cell hyperplasia and papillary elongation have been suggested as markers of the disorder.72 73 However, subsequent studies have not confirmed their diagnostic value.74 75 More recently, oesophageal histology resurged with the recognition of DIS as a potential mechanisms for symptoms in GORD.76 77
Several studies using transmission electron microscopy found wider intercellular spaces in patients with GORD as compared with normal controls.71 76 78 In patients with NERD, the mean diameter of intercellular spaces was at least two times longer than in controls. Studies using light microscopy scored DIS as present or absent and also revealed that DIS were significantly more common in patients with GORD.
The current hypothesis concerning symptom generation (heartburn) in NERD is that the presence of DIS allows acid to reach and activate chemosensitive nociceptors present in sensory afferents of the oesophageal epithelium.78 In other words, the presence of DIS promotes higher activation of sensory nerve endings. DIS is a non-specific feature and can be found in up to 30% of asymptomatic subjects, as well as in patients with Candida infection of the oesophagus, food allergy, eosinophilic oesophagitis and oesophageal cancer.79–82
Calabrese et al83 studied the reversibility of DIS after omeprazole 40 mg daily. After 3 months, most patients showed the disappearance of DIS and resolution of symptoms. However, the rate of reversibility of DIS after a shorter duration of PPI treatment was less pronounced. In another study,84 patients received esomeprazole or ranitidine for 4 weeks. The PPI treatment normalised intercellular spaces in 25–29% of patients. A recent preliminary report suggests that NERD patients refractory to PPIs have persistence of DIS.85 In these patients, other refluxate components may be responsible for maintenance of both DIS and symptoms. Furthermore, experimental exposure of the oesophageal mucosa to weakly acidic solutions containing bile acids (similar to what could happen in NERD patients on PPIs) can still provoke increased oesophageal permeability and even DIS (fig 5).86

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
These observations suggest that new endoscopic modalities with unique capabilities to diagnose DIS could have a role in the evaluation of patients with refractory heartburn. However, assessing the presence of DIS in a busy general GI practice may be time consuming and costly, but at the same time may provide the clue that clinicians are seeking to confirm that reflux is still the cause of the patient’s symptoms.
Box 1: Current diagnostic techniques for refractory heartburn
Upper gastrointestinal endoscopy
Oesophageal biopsies for dilated intercellular spaces
Ambulatory 24 h oesophageal pH monitoring
Ambulatory 24 h oesophageal impedance–pH monitoring
Oesophageal Bilitec
Oesophageal pH monitoring
Both catheter and wireless oesophageal pH monitoring allow for the quantification of oesophageal acid exposure and assessment of the temporal relationship between symptoms and acid reflux events.87 88 Oesophageal pH monitoring is commonly used in the evaluation of patients with refractory GORD. In the assessment of such patients, pH monitoring can be performed off PPIs to test if the initial diagnosis was correct (ie, heartburn was due to acid reflux) or on PPIs to test whether the symptoms are due to residual acid reflux.
In refractory GORD, pH monitoring is most commonly done while patients are taking PPIs twice daily. Inclusion of a symptom–reflux correlation measure such as symptom index (SI) and symptom association probability (SAP) helps to identify heartburn episodes associated with acid reflux regardless of whether the oesophageal acid exposure is normal or abnormal. The symptom–reflux correlation is considered positive if the SI is higher than 50% and/or the SAP is higher than 95%. Some authorities have suggested that the threshold for an abnormal pH test should be lowered in patients having the test on PPI treatment. Kuo and Castell89 proposed a cut-off of 1.6% based on a 95% confidence interval obtained from a study in healthy subjects treated with omeprazole 40 mg once daily.89
A positive pH monitoring on PPIs suggests that patients’ persistent heartburn might be related to ongoing acid reflux. If an abnormal pH is present, then insufficient acid inhibition should be suspected. In contrast, if the pH test is normal, then heartburn induced by physiological levels of acid exposure could be the explanation. GORD-related symptoms due to oesophageal acid exposure can occur in 7–10% of GORD patients with persistent symptoms on twice-daily PPI treatment.18 19 49
A negative pH test on PPIs (ie, normal oesophageal acid exposure and negative symptom–reflux correlation) suggests that the patient’s heartburn is not related to ongoing acid reflux. However, a negative 24 h pH test on PPIs does not necessarily exclude the possibility of an underlying acid reflux in a patient who is adequately suppressed on PPIs. Acid reflux could be missed because of poor tolerability of the pH probe, which can result in a significant decrease in reflux-provoking activities.90 Recent studies using wireless pH monitoring for 4 days showed a certain degree of day-to-day variability in symptom reflux association and therefore proposed testing patients both off and on PPI treatment during one session of pH testing.91 Studies with the wireless pH system over a period of 48 h demonstrated a significant number of patients who do not experience reflux on two consecutive days.92 The prolonged recording period with the wireless pH capsule can also increase the sensitivity of the test for the detection of symptoms that correlate with acid reflux episodes.93 At present, more studies are needed to confirm the usefulness of prolonged wireless pH testing to better detect persistent acid reflux in patients who are refractory to PPI treatment.
Recent studies using either a catheter or wireless pH test with sensors located or clipped immediately above the squamocolumnar junction have shown the occurrence of short segment acid reflux episodes.94–96 Acid exposure just above the squamocolumnar junction, not detected by conventional pH studies, may play a role in patients with persistent reflux symptoms despite PPI treatment. Further studies are needed to assess the association between heartburn and short segment gastro-oesophageal reflux.
Oesophageal impedance–pH monitoring
While oesophageal pH monitoring is considered the “gold standard” for gastro-oesophageal reflux detection, it may not accurately detect GORD when little or no acid is present in the refluxate. Oesophageal impedance monitoring is a technique that can be used to detect all types of GORD (acidic, weakly acidic and weakly alkaline). This technique is based on the measurement of electrical impedance between closely arranged electrodes mounted on a thin intraluminal probe. Air has a low conductivity and yields an increase in impedance, while swallowed or refluxed material has a high conductivity and yields an impedance drop. Changes in temporal–spatial patterns in impedance are identified at various levels within the oesophagus allowing differentiation between antegrade (ie, swallow) and retrograde (ie, reflux) bolus movement. In this way, impedance can be used to evaluate intra-oesophageal liquid movements (bolus transit tests and reflux monitoring) or gas movement (aerophagia and belching). Animal and human validation studies have confirmed the high sensitivity and accuracy of impedance for reflux detection and tracking of intraesophageal bolus movement.97–101 However, it is not possible at present to quantify the volume of gastro-oesophageal reflux using impedance. In healthy adults, the total rate of reflux episodes measured with impedance–pH is about 40 per 24 h with one-third being acid and two-thirds being weakly acidic and weakly alkaline. Impedance–pH monitoring should be analysed in a quantitative fashion, similar to 24 h pH monitoring, by searching for increased numbers of reflux episodes, prolonged acid or volume exposures, or increased numbers of proximal reflux events. In addition, qualitative analysis of the reflux–symptom association, using SI or SAP, is essential.
It is currently suggested that impedance–pH monitoring is useful in reaching a diagnosis in patients with refractory GORD. Around 10% of refractory GORD patients on PPIs have a positive SI for acid reflux, and 37% have a positive SI for non-acid reflux.18 A European multicentre study found similar results and showed that adding impedance to pH monitoring improves the diagnostic yield by 15–20% and allows better symptom analysis than pH monitoring alone.19 Because impedance–pH monitoring is currently the most sensitive method for reflux detection, a negative study (normal number of total reflux events and negative symptom analysis) rules out GORD as a cause of persistent symptoms. On the other hand, most patients whose symptoms are associated with weakly acidic reflux do not have an increased number of reflux events, suggesting that they have hypersensitivity of the oesophagus to less acidic refluxate.17
Oesophageal Bilitec
Studies with Bilitec have demonstrated a progressive increase in DGOR across the spectrum of GORD, with a particularly high prevalence in patients with Barrett’s oesophagus.32 102 Bilitec detection in the oesophageal lumen of any absorption near 450 nm suggests the presence of bilirubin, a surrogate marker for bile reflux. DGOR data measured by Bilitec are usually presented as per cent time bilirubin absorbance that is higher than 0.14.
Bilirubin monitoring provides different information compared to other modalities that evaluate reflux by focusing primarily on the chemical composition of the refluxate. Detection of bilirubin in the refluxate is indicative for DGOR. The impedance and pH tests can detect acidic and non-acidic reflux but cannot describe its composition. Bilitec adds information about the chemical nature of acidic and non-acidic material that refluxes into the oesophagus.
TREATMENT OPTIONS
Box 2 summarises recent treatment advances for persistent heartburn while on treatment with PPIs.
Compliance and adherence
The need to ensure proper compliance cannot be over-emphasised. Compliance should be assessed in all patients with GORD who report lack of response to PPI treatment, particularly prior to ordering any evaluative test.103 In addition to compliance, proper dosing time should be assessed as well. Explanations about the reason for taking PPIs half an hour before a meal should be provided to all patients with GORD.
Overall, evaluation of proper compliance and adequate dosing time should be the first management step when assessing patients with heartburn who are not responding to PPIs before instituting any other intervention.
Lifestyle modifications
The specific value of lifestyle modifications in patients with GORD who failed PPI treatment has yet to be elucidated. Whilst physicians recognise the importance of adopting lifestyle modifications by these patients, many do not spend the time to identify the lifestyle activities that may trigger patients’ GORD-related symptoms. In one survey, 55% of the patients with GORD were instructed by their physician to avoid certain foods, 37% to avoid caffeine, 36% to reduce the stress in their life, and 36% to lose weight.4 Heavy meals, exercise, increased alcohol consumption, and others might lead to breakthrough symptoms in patients with heartburn who are treated with PPIs. Spices used in seasonings or sauces, tomatoes, tomato sauce, tomato juice, citrus fruits and drinks are reported by more than 50% of patients with GORD to aggravate heartburn.4 However, in a recent systematic review of all publications that evaluated the value of lifestyle modifications in such patients, the authors determined that only weight loss and elevation of the bed head are effective in improving GORD.104 There were insufficient data to support any of the other commonly practised lifestyle modifications. Regardless, in patients with persistent heartburn despite PPI treatment, it is reasonable to recommend avoidance of specific lifestyle activities that have been identified by patients or physicians to trigger GORD-related symptoms.
Histamine 2 receptor antagonists
Early studies have shown that the addition of a histamine 2 receptor antagonist (H2RA) at bedtime significantly reduced the duration of NAB and the number of patients with GORD on PPIs twice daily who demonstrated NAB.105 The effect on NAB was not different between standard dose and double-dose H2RAs. Despite a lack of any clinical correlation between the presence of NAB and nocturnal GORD symptoms, the addition of H2RAs at bedtime has become common practice in GORD patients who failed PPI treatment regardless of dosing. However, the enthusiasm about the value of adding H2RAs at bedtime has been subsequently tempered by a study demonstrating rapid development of tolerance to H2RAs. There is no difference in gastric acid suppression between PPIs twice daily and PPIs twice daily plus an H2RA at bedtime after 1 week of therapy.106 None of the aforementioned studies provided any clinical information about symptom control or lack of it. A recent retrospective study by Rackoff et al107 evaluated 56 patients with GORD on PPIs twice daily who were receiving H2RAs at bedtime for variable time periods. The authors found that 72% of the patients reported improvement in overall symptoms, 74% reported improvement in night-time reflux symptoms, and 67% reported improvement in GORD-associated sleep disturbances. The latter study and the vast experience we have accumulated thus far with H2RA treatment for GORD suggest that H2RAs improve GORD-related symptoms in the long term in a substantial number of patients. If clinical tolerance has been encountered, then using H2RAs intermittently or on demand could be helpful.
Box 2: Recent treatment advances for persistent heartburn while on treatment with proton pump inhibitors
Baclofen, a γ-aminobutyric acid B receptor agonist, significantly reduced weakly acidic or duodenogastro-oesophageal reflux in patients with persistent heartburn on double-dose proton pump inhibitors (PPIs)
Botulinum toxin injection of the gastric pylorus improved refractory gastro-oesophageal reflux disease (GORD)-related symptoms in patients with gastroparesis
In patients with GORD who failed PPIs given once daily, adding acupuncture resulted in significantly better control of heartburn and regurgitation than doubling the PPI dose
Patients with GORD and documented positive association between weakly acidic reflux events and GORD symptoms, while on PPIs twice daily, reported marked improvement in symptoms for an average of 14 months after anti-reflux surgery
Proton pump inhibitors
In patients who failed PPIs once a day, there are two potential therapeutic strategies. These include switching to another PPI or doubling the PPI dose. In one study, patients who failed lansoprazole 30 mg once daily were randomised to either double-dose lansoprazole or 40 mg once daily esomeprazole.108 Single-dose esomeprazole was as effective as double-dose lansoprazole in percentage of heartburn-free days as well as symptom score for heartburn, acid regurgitation, and epigastric pain. There are no specific data regarding the other PPI brands, but switching to another PPI is an attractive therapeutic strategy that could be utilised in the management of patients with persistent heartburn despite PPI treatment. Doubling the PPI dose has become a commonly practised therapeutic strategy in patients with GORD who failed PPIs once daily. In patients with erosive oesophagitis, treating with double-dose PPIs over a period of 8 weeks will increase healing rate by 6% but will have no impact on symptom rate.68 In patients with symptomatic GORD who failed PPIs once a day, doubling the PPI dose can increase the rate of overall symptom improvement by 22–26%.109 There is also support for doubling the PPI dose in patients with functional heartburn using Rome II criteria.110 Patients with the sensitive oesophagus (normal endoscopy and pH test but positive symptom index) were more likely to respond to PPIs twice a day. There is no evidence to support further escalation of the PPI dose in those who failed PPIs twice daily. When doubling the PPI dose, one PPI should be given before breakfast and the other before dinner. The support for splitting the dose originates primarily from physiological studies demonstrating an improved control of intragastric pH when one PPI is given in the morning and the other in the evening as compared with both PPIs being given before breakfast.111
A recent study suggested that a minority of patients with GORD may lose PPI efficacy after 2 years of continuous and unmodified treatment with one or two PPIs per day.112 The sole parameter that was evaluated was the extent of oesophageal acid exposure as assessed by pH testing. The authors failed to provide clinical data to support their physiological findings. Further studies are needed to determine the loss of long-term efficacy of PPIs in patients with GORD. In another recent study, the authors demonstrated that infection with Helicobacter pylori in healthy subjects who are extensive metabolisers of CYP2C19 eliminated the differences in controlling intragastric pH between standard and double-dose PPIs.113 As with the previous study, the authors did not support their physiological findings with clinical data.
TLESR reducers
A variety of compounds have been shown to reduce the rate of transient lower oesophageal sphincter relaxation (TLESR) and thus the number of reflux events. However, only baclofen, a γ-aminobutyric acid B receptor agonist, has been introduced into the clinical arena as a potential add-on treatment for patients who failed PPI treatment (once or twice daily).114 115 The drug reduced TLESR rate by 40–60%, reflux episodes by 43%, increased lower oesophageal sphincter basal pressure, and accelerated gastric emptying.114–116 Baclofen has been shown to significantly reduce weakly acidic reflux and DGOR as well as duodenogastro-oesophageal reflux (DOER)-related symptoms.117 118 In subjects with persistent heartburn despite PPI treatment, doses up to 20 mg three times daily have been used.117 Because the drug crosses the blood–brain barrier, a variety of central nervous system (CNS)-related side effects may occur. They primarily include somnolence, confusion, dizziness, lightheadedness, drowsiness, weakness and trembling. The side effects are an important limiting factor in the routine usage of baclofen in clinical practice. However, several baclofen-like prototypes with better clinical and side-effect profiles are currently in development.
Baclofen should be considered in patients with clear evidence of persistent symptoms that are related to weakly acidic reflux as documented by intra-oesophageal impedance or in those with regurgitation, or sour or bitter taste in the mouth as the predominant symptom.
Promotility drugs
Presently, there are no available data about the value of adding a promotility drug in patients who failed either one or two PPIs per day. However, in patients with delayed gastric emptying and persistent GORD symptoms on PPIs, the use of a promotility drug is an attractive option. It is unclear though if patients with refractory GORD with normal gastric emptying would also benefit from adding a promotility drug.
Bile acid binders and sucralfate
The role of bile acid binders such as cholestyramine or sucralfate in GORD patients who failed PPI treatfment remains to be elucidated. Reducing DGOR in this patient population is desirable, but it is unclear if any of the currently available bile acid binders are sufficiently efficacious to improve symptoms.
Visceral pain modulators
Thus far, there are no studies that specifically evaluated the value of visceral pain modulators in GORD patients with persistent heartburn despite PPI treatment. However, given the fact that most of the patients who fail PPI treatment originate from the group with non-erosive reflux disease and that up to 40% of the patients who fail PPI treatment demonstrate lack of either weakly or acidic reflux during intra-oesophageal impedance assessment, the use of these agents is highly attractive.12 18 Additionally, it could be argued that even for weakly acidic reflux that has not been shown to be associated with oesophageal mucosal damage, visceral pain modulators could be helpful. Pain modulators such as tricyclic antidepressants, trazodone, and selective serotonin reuptake inhibitors have all been shown to improve oesophageal pain in patients with non-cardiac chest pain.18 119 120 It is believed that these agents confer their visceral analgesic effect by acting at the central nervous system and/or sensory afferents level. The pain modulators are used in non-mood-altering doses, and they presently provide a therapeutic alternative until more novel and oesophageal-specific compounds are available.
Endoscopic treatment for gastro-oesophageal reflux
Several studies using primarily the Stretta procedure (radio-frequency energy) evaluated the value of endoscopic treatment for GORD in patients who partially responded to PPI treatment. All studies reported marked improvement in patients’ heartburn score and quality of life assessment as well as significant reduction in the usage of anti-reflux medications that extended over a period of up to 4 years.121 Another study also demonstrated that the Stretta procedure was effective in treating patients with refractory GORD who underwent a Roux-en-Y gastric bypass.122 It is likely that the Stretta procedure improves symptoms in GORD patients by both reducing gastro-oesophageal reflux and oesophageal acid sensitivity. However, the Stretta procedure, as with other endoscopic treatments of GORD, lost its appeal as a viable therapeutic modality for GORD primarily due to potential adverse events, lack of reversibility, and lingering doubts about its clinical efficacy.
Botulinum toxin injection
In a recent study, the authors performed pyloric injection in 11 patients with refractory GORD and associated gastroparesis.46 Post-treatment, the authors were able to demonstrate marked improvement in GORD-related symptoms that correlated with improvement in symptoms related to gastroparesis and gastric-emptying scintigraphy. Unfortunately, a recently published study demonstrated that the effect of intrapyloric botulinum toxin injection on gastric emptying is likely to wear off within 1 month.123
Anti-reflux surgery
A recent surgical study reported that refractory GORD was the most common (88%) indication for anti-reflux surgery.124 Interestingly, the most common preoperative symptom under failure of medical anti-reflux treatment was regurgitation (54%). Overall, 82% of the patients reported that the preoperative reflux symptom completely resolved, and 94% were satisfied with the results of the surgery. In another study that included only 30 subjects with refractory GORD who were followed for a period of 12 months, the main preoperative symptoms were regurgitation (93%) and heartburn (60%).46 At the end of 1 year post-surgery, all patients were completely relieved of heartburn, but only 86% reported resolution of regurgitation. Patient satisfaction rate with the surgery was 87%.
Two recent studies suggest that a positive SI during impedance–pH monitoring in patients on PPIs can predict a favourable response to medical or surgical therapy. The first study by Mainie et al125 followed 19 patients who were refractory to a double-dose of PPI and successfully underwent laparoscopic Nissen fundoplication. Prior to surgery, 18 of the 19 patients were found to have a positive SI on oesophageal impedance–pH monitoring. After a mean follow-up of 14 months, 16 of the patients with a positive SI were asymptomatic. The second study by Becker et al126 assessed 56 patients with persistent symptoms on a single dose of PPI and abnormal impedance–pH monitoring. Most of these patients had a positive SI and later demonstrated significantly better response to doubling the PPI dose as compared to subjects with normal impedance pH monitoring. Both of the aforementioned studies were uncontrolled and did not clearly describe whether symptoms were due to remaining acid reflux, which could have been detected by a simple pH test and potentially treated with higher-dose PPI, or weakly acidic reflux.
The role of anti-reflux surgery in patients with GORD who continued to be symptomatic on PPI treatment has been scarcely studied. Overall, if patients who fail PPI treatment are not carefully evaluated for the presence of symptoms associated with reflux events prior to surgical intervention, the outcome of surgery could be very poor.
Box 3: Future diagnostic techniques for refractory heartburn
Measurements of reflux
Improvements of impedance–pH monitoring
Prolonged recordings (48 h)
Wireless system
Better definition of proximal extent of reflux
Quantification of volume of gas and liquid reflux
Automatic analysis
Improvement of duodenogastro-oesophageal reflux monitoring
New sensor device without the need for dietary changes
Better definition of individual bile reflux events
Combination with impedance–pH
Endoscopic diagnosis
Detection of microscopic mucosal changes
High-definition endoscopy
Detection of dilated intercellular spaces with confocal endoscopy
Measurements of hypersensitivity to mechanical and chemical stimuli
New provocative tests, ie, proximal air insufflations
Stress tests
Brain imaging during provocative testing
Alternative medicine
The value of acupuncture has recently been evaluated in patients with GORD who failed PPIs once daily.55 When compared to doubling the PPI dose (standard of care), adding acupuncture was significantly better in controlling regurgitation and daytime and night-time heartburn. This is the first study to suggest that alternative approaches for treating visceral pain may have a role in GORD patients with persistent heartburn despite PPI treatment.
Psychological treatment
Currently, there are no studies evaluating the value of screening for psychological co-morbidity in patients who failed PPI treatment. Nojkov et al55 provided the first evidence that response to PPI treatment may be dependent on the level of psychological distress. This study suggests that future treatment of refractory GORD may require psychological evaluation and possibly intervention.
THE FUTURE
Box 3 provides a list of future diagnostic techniques for refractory heartburn. Persistent heartburn in patients receiving PPIs has been recognised by many pharmaceutical companies as an area of unmet need. Due to the relatively high prevalence of this clinical problem, the industry sees an opportunity for significant revenue in a market that is already saturated with PPIs. Thus, various therapeutic modalities are under investigation. Most focus on two main targets: decreasing TLESR rate and further improving suppression of gastric acid secretion.127–132 Another promising area is further development of more oesophageal-specific pain modulators. Even in the case of weakly acidic reflux, pain modulators could play an important role in relieving refractory symptoms. Other potential causes for symptoms in patients who failed PPI treatment include oesophageal distension and other components of the refluxate, such as bile, pepsin and others. Potentially, all could be symptomatically addressed with oesophageal pain modulators.
Future research will continue to focus on mechanisms for oesophageal pain, primarily the role of central and peripheral sensitisation in enhancing perception of intra-oesophageal stimuli.133 The serotonin-related drugs, such as 5-hydroxytryptamine (5HT) type 3 antagonist and 5HT type 4 agonist, appear to have a pain-modulatory effect, by altering the initiation, transmission or processing of extrinsic sensory information from the gastrointestinal tract.
Phosphorylation of N-methyl-d-aspartate (NMDA) receptors expressed by dorsal horn neurons leads to central sensitisation via an increase in their excitability and receptive field size.134 Potentially, this central sensitisation may be prevented or even reversed by antagonism of NMDA receptors within the spinal cord.
Potential targets that are currently under consideration include vanilloid receptor ion channels, acid-sensing ion channels, sensory neuron-specific Na+ channels, P2X purinoceptors, cholecystokinin (CCK) receptors, bradykinin and prostaglandin receptors, glutamate receptors, tachykinin, and calcitonin gene-related peptide receptors as well as peripheral opioid and cannabinoid receptors.135 136 The peripheral opioid receptor agonists are of great interest because they may offer visceral analgesic effects without crossing the blood–brain barrier and thus affecting the CNS.
Spinal afferents, which may play a role in visceral nociception, express tachykinins that include substance P, neurokinins A and B, and neuropeptide K. Tachykinin antagonists may confer a visceral analgesic effect that can be used in PPI-resistant patients. Neurokinin (NK)-1, NK-2 and NK-3 receptor antagonists were only evaluated in preclinical trials. Cholecystokinin receptor antagonists may alter visceral pain perception.
Another important area that is likely to attract future attention when treating patients with refractory GORD is complementary and alternative therapeutic modalities that can interfere with the mind and body axis.
REFERENCES
Footnotes
Competing interests: Declared. RF is the recipient of research grants from AstraZeneca, Wyeth and Takeda; is a speaker for AstraZeneca; and a consultant for AstraZeneca, Takeda, Eisai, Proctor & Gamble, Vecta, Addix, Xenoport and Pfizer. DS is the recipient of a research grant from Sandhill Scientific and AstraZeneca.