Article Text

Abstract
Introduction Probiotics may benefit irritable bowel syndrome (IBS) symptoms, but randomised controlled trials (RCTs) have been conflicting; therefore a systematic review was conducted.
Methods MEDLINE (1966 to May 2008), EMBASE (1988 to May 2008) and the Cochrane Controlled Trials Register (2008) electronic databases were searched, as were abstracts from DDW (Digestive Diseases Week) and UEGW (United European Gastroenterology Week), and authors were contacted for extra information. Only parallel group RCTs with at least 1 week of treatment comparing probiotics with placebo or no treatment in adults with IBS according to any acceptable definition were included. Studies had to provide improvement in abdominal pain or global IBS symptoms as an outcome. Eligibility assessment and data extraction were performed by two independent researchers. Data were synthesised using relative risk (RR) of symptoms not improving for dichotomous data and standardised mean difference (SMD) for continuous data using random effects models.
Results 19 RCTs (18 papers) in 1650 patients with IBS were identified. Trial quality was generally good, with nine reporting adequate methods of randomisation and six a method of concealment of allocation. There were 10 RCTs involving 918 patients providing outcomes as a dichotomous variable. Probiotics were statistically significantly better than placebo (RR of IBS not improving=0.71; 95% CI 0.57 to 0.88) with a number needed to treat (NNT)=4 (95% CI 3 to 12.5). There was significant heterogeneity (χ2=28.3, p=0.001, I2=68%) and possible funnel plot asymmetry. Fifteen trials assessing 1351 patients reported on improvement in IBS score as a continuous outcome (SMD=−0.34; 95% CI −0.60 to −0.07). There was statistically significant heterogeneity (χ2=67.04, p<0.001, I2=79%), but this was explained by one outlying trial.
Conclusion Probiotics appear to be efficacious in IBS, but the magnitude of benefit and the most effective species and strain are uncertain.
Statistics from Altmetric.com
Patients with irritable bowel syndrome (IBS) have a complex of symptoms1 which can be difficult to treat. Antispasmodics and bulking agents have modest efficacy,2 and even newer agents such as 5HT4 agonists3 and 5HT3 antagonists4 only have a 10% therapeutic gain over placebo. These newer drugs are now unavailable (5HT4) or have restrictions for general use (5HT3) because of concerns about possible cardiovascular risks5 and ischaemic colitis,6 respectively. Therapeutic options for IBS are therefore limited, which can be frustrating for patients and clinicians.
Attention has therefore focused on intestinal microflora, as these are important for intestinal function, and changes in gut microbiota are found in patients with IBS.7 8 Whether these changes are a cause or a consequence of IBS remains uncertain.9 The possibility that alterations in intestinal commensal bacteria have a causal role in some patients with IBS is supported by observations that IBS symptoms are more common following infectious gastroenteritis,10 and that this association may persist for several years.11 These findings could be due to bias or confounding, however, and altering intestinal flora in patients with IBS in a randomised controlled trial (RCT) would provide more compelling evidence for the role of gut microbiota in this disorder. Researchers have attempted this using probiotics in IBS but the results have been inconclusive. Studies have reported an improvement in global symptoms with probiotics,12 whilst others have failed to demonstrate any benefit.13 Other trials have not found a clear effect of probiotics on primary endpoints, but have found benefits for secondary endpoints such as bloating.14 However, the resolution of specific symptoms has not been consistent even in studies performed by the same group of investigators.15 Some of this variation may be attributable to the type of probiotic used, as well as methodological differences between trials. We have therefore conducted a systematic review of the literature to evaluate the impact of probiotics on IBS and to explore potential reasons for heterogeneity in study findings.
Methods
Search strategy and study selection
A search of the medical literature was conducted using MEDLINE (1950 to June 2008), EMBASE (1980 to June 2008) and the Cochrane Controlled Trials Register (2007). RCTs comparing the effect of probiotics with placebo or no treatment in adult patients with IBS (over the age of 16 years) were eligible for inclusion. Trials that permitted other concomitant therapies were eligible, as long as these were administered to both the intervention and control arms. The first period of crossover RCTs were also eligible for inclusion. Minimum duration of treatment and follow-up was 7 days. The diagnosis of IBS could be based on either a doctor's opinion or symptom-based diagnostic criteria, supplemented by the results of investigations to exclude organic disease, where studies deemed this necessary. The primary outcome of this systematic review was change in global IBS symptoms reported as a dichotomous or continuous variable. Abdominal pain data were included in the review if data for global symptoms were not available. Where studies did not report extractable data, but were otherwise eligible for inclusion in the systematic review, we attempted to contact the original investigators in order to obtain further information.
Studies on IBS were identified with the terms irritable bowel syndrome and functional diseases, colon (both as medical subject heading (MeSH) and free text terms), and IBS, spastic colon, irritable colon, and functional adj5 bowel (as free text terms). These were combined using the set operator AND, with studies identified with the terms: Saccharomyces, Lactobacillus, Bifidobacterium, Escherichia coli or probiotics (MeSH and free text terms).
There were no language restrictions, and abstracts of the papers identified by the initial search were evaluated by the lead reviewer for appropriateness to the study question, and all potentially relevant papers were obtained and evaluated in detail. Foreign language papers were translated where necessary. Abstract books of conference proceedings between 2001 and 2007 were hand-searched to identify potentially eligible studies published only in abstract form. The bibliographies of all identified relevant studies were used to perform a recursive search of the literature. Articles were independently assessed by two reviewers using predesigned eligibility forms, according to the prospectively defined eligibility criteria. Any disagreement between investigators was resolved by consensus between the two researchers, adjudicated with the support of a third investigator.
Outcome assessment
The primary outcome assessed was the effect of probiotics compared with placebo on global IBS symptoms (or abdominal pain if global symptoms were not reported) at the end of treatment. Dichotomous data included either symptom cure or improvement, and if multiple strata were given to define improvement then the cut-off point with the greatest improvement was utilised (eg, if the scale was 1, no improvement; 2, a little improvement; 3, a moderate amount of improvement; 4, symptoms very much improved; the latter descriptor was used). Patient-reported outcomes were included where possible in the review, but investigator-reported outcomes were included if these were the only data available. Continuous data were defined as ean total IBS symptom scores or abdominal pain scores from questionnaire data. Secondary outcomes included effect of treatment on bloating, urgency and flatus, and adverse events as a result of treatment.
Data extraction
All data were extracted independently by two reviewers on to a Microsoft Excel spreadsheet (XP professional edition; Microsoft Corp, Redmond, Washington, USA). All data extraction was then checked by a third reviewer. In addition, the following clinical data were extracted for each trial: setting (primary, secondary or tertiary care-based); number of centres; country of origin; dose and duration of treatment; total number of adverse events reported; criteria used to define IBS; primary outcome measure used to define symptom improvement or cure following treatment; duration of treatment; duration of follow-up; proportion of female patients; and proportion of patients according to predominant stool pattern. Data were extracted as intention-to-treat analyses, where all drop-outs are assumed to be treatment failures, wherever trial reporting allowed this.
Study quality
Assessment of study quality was performed independently by two reviewers according to the Jadad scale,16 which records whether a study is described as randomised and double-blind, the method of generation of the allocation schedule and method of double-blinding, and whether there is a description of drop-outs during the trial.
Data synthesis and statistical analysis
Data were pooled using a random effects model.17 The impacts of probiotics on dichotomous outcomes were expressed as a relative risk (RR) of global IBS symptoms or abdominal pain persisting with intervention compared with control with 95% CIs. The number needed to treat (NNT) and 95% CIs were calculated from the reciprocal of the risk difference from the meta-analysis. The effect of probiotics on total IBS symptom scores and abdominal pain scores after completion of treatment was examined using a standardised mean difference (SMD) with a 95% CI.
The results of individual studies can be diverse, and this inconsistency within a single meta-analysis can be quantified with a statistical test of heterogeneity, to assess whether the variation across trials is due to true heterogeneity, or chance. This quantity is termed I2, and its value ranges from 0 to 100%, with 0% representing no observed heterogeneity, and larger values indicating increasing heterogeneity. A value below 25% is arbitrarily chosen to represent low levels of heterogeneity.18 Where the degree of statistical heterogeneity was greater than this among trial results in this meta-analysis, possible explanations were investigated using sensitivity analyses according to trial setting, criteria used to define IBS, whether the methods of randomisation or concealment of allocation were reported, level of blinding, and study quality according to the Jadad scale. These are exploratory only, and may explain some of the observed variability, but the results should be interpreted with caution.
Review Manager version 4.2.8 (RevMan for Windows 2003, the Nordic Cochrane Center, Copenhagen, Denmark) and StatsDirect version 2.4.4 (StatsDirect, Sale, Cheshire, UK) were used to generate Forest plots of pooled RRs and risk differences for primary and secondary outcomes with 95% CIs, as well as funnel plots. The latter were assessed for evidence of asymmetry, and therefore possible publication bias, using the Egger test.19
Results
A total of 185 citations were identified, of which 18 papers12–15 20–33 were eligible (figure 1) evaluating 1650 participants. Extra information was obtained from the authors of five papers.14 15 22 25 31 The quality of the studies was generally good, with 11 (58%)12–15 20–33 scoring at least 4 out of 5 on the Jadad scale (table 1). Nine trials14 15 22 24 25 27 31–33 reported an adequate method of randomisation, and six studies14 15 25 27 31 33 described appropriate methods of concealment of allocation (table 1). The majority of trials recruited patients with Rome II IBS,12–15 22 23 25–27 29–31 but two20 28 used an author-defined definition of IBS, two used Rome I,21 24 and one each employed the Manning32 and Rome III33 criteria (table 1).

Flow diagram of trials evaluated in the systematic review.
Characteristics of included studies
Efficacy of probiotics on overall IBS symptoms
Ten studies14 21 22 24–26 30–33 with 918 participants reported IBS symptoms as a dichotomous outcome. Probiotics had a statistically significant effect in reducing IBS symptoms (RR of symptoms persisting in probiotic group=0.71; 95% CI 0.57 to 0.88) (figure 2) with an NNT of 4 (95% CI 3 to 12.5). There was significant heterogeneity among studies (χ2 =28.3, degrees of freedom (d.f.)=9, p=0.001, I2=68%). There was no difference between the different types of probiotics used, with Lactobacillus (three trials, 140 patients),20 21 33 Bifidobacterium (two trials, 422 patients),30 31 Streptococcus (one trial, 54 patients)32 and combinations of probiotics (four trials, 302 patients)14 24 25 26 all showing a trend towards benefit (figure 2). There was, however, some asymmetry in the funnel plot (figure 3) (Egger test=−2.97; 95% CI −5.54 to −0.41, p=0.028), suggesting publication bias or other small study effects. Trials with a Jadad score ≥414 21 26 31–33 had significantly less of a treatment effect (RR=0.86; 95% CI 0.72 to 1.03) than those with a Jadad score <420 24 25 30 (RR=0.52; 95% CI 0.35 to 0.77) (Cochrane Q=5.2, p=0.02).

Forest plot of trials comparing probiotics with placebo reporting a dichotomous outcome. IBS, irritable bowel syndrome.

Funnel plot of studies reporting a dichotomous outcome.
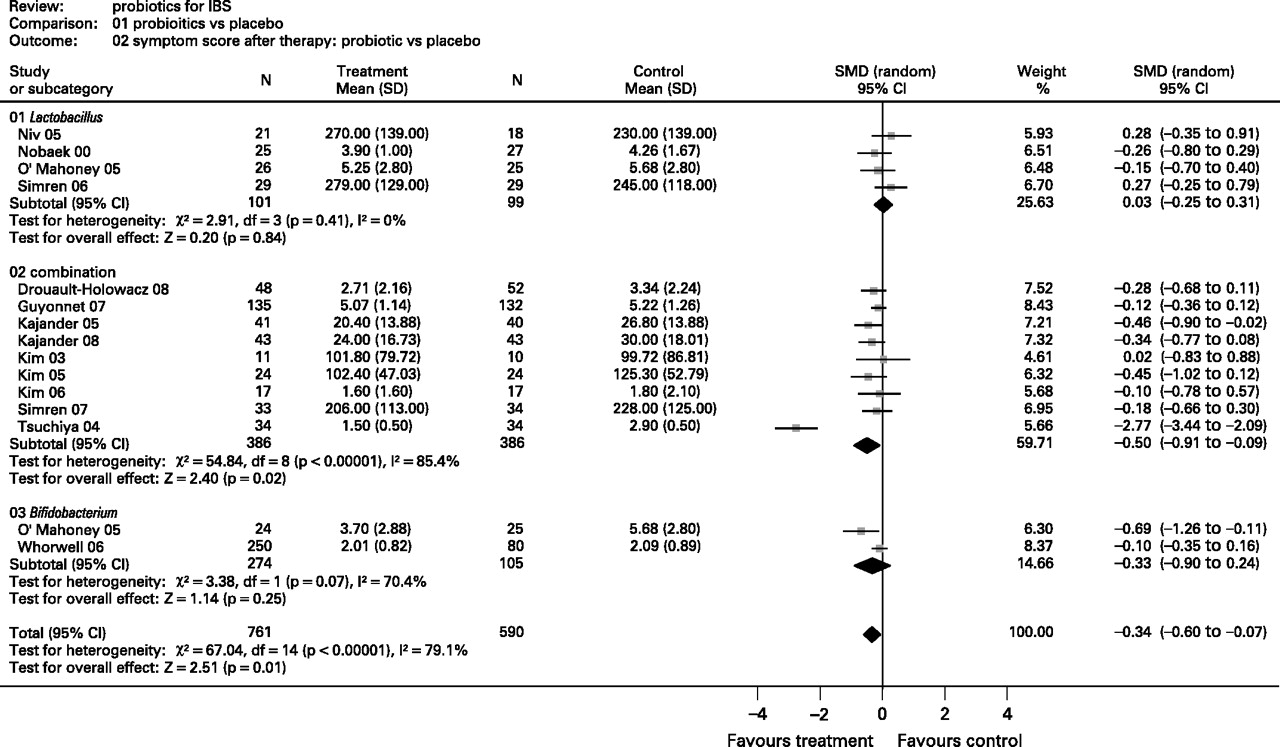
Fifteen trials described in 14 papers12–15 21–29 31 with 1351 participants reported IBS symptoms as a continuous variable. Probiotics had a statistically significant effect in improving IBS symptoms compared with placebo (SMD=−0.34; 95% CI −0.60 to −0.07) (figure 4). There was statistically significant heterogeneity (χ2=67.04, d.f.=14, p<0.001, I2=79%), but this was explained by one outlying trial.25 When this trial was excluded, the statistically significant effect of probiotics in improving IBS symptoms remained (SMD=−0.18; 95% CI −0.29 to −0.06) but heterogeneity was no longer apparent (χ2=12.1, d.f.=13, p=0.52, I2=0%). There was no significant funnel plot asymmetry (Egger test=−1.75; 95% CI −5.15 to 1.64, p=0.29). There was a trend for higher quality studies to report less of a treatment effect than lower quality studies, but this was driven by one outlier.25 When this study was removed, the treatment effect was similar in trials with a Jadad score ≥412–15 21 22 26 27 31 (SMD=−0.19; 95% CI −0.31 to −0.03) and those with a Jadad score <423–25 28 29 (SMD=−0.13; 95% CI −0.45 to 0.17). Four trials13 20–22 evaluated Lactobacillus in 200 patients and found no effect on IBS symptoms, nine trials12–15 24–29 evaluated combinations of probiotics in 772 patients with a significant effect in improving IBS symptoms, whilst two trials22 31 evaluated Bifidobacterium in 379 patients with a trend towards improving IBS symptoms that did not reach statistical significance (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of trials comparing probiotics with placebo reporting a continuous outcome. IBS, irritable bowel syndrome; SMD, standardised mean difference.
Efficacy of probiotics on individual IBS symptoms
Individual IBS symptoms were almost exclusively given as a continuous outcome. Ten trials (from nine papers)14 15 21 22 24–26 28 31 with 834 participants reported on abdominal pain. There was a statistically significant effect in favour of probiotics improving pain scores (SMD=−0.51; 95% CI −0.91 to −0.09, p=0.016) with significant heterogeneity among studies (χ2=61,08, d.f.=9, p<0.0001, I2=85%). This was due to one outlying study,25 and when this was removed the statistically significant effect on improving IBS symptoms remained (SMD=−0.22; 95% CI −0.37 to −0.06, p=0.002) but heterogeneity was no longer apparent (χ2=7.29, d.f.=8, p=0.51, I2=0%).
Eight trials (from seven papers)14 15 22 24 25 28 31 with 682 patients reported on bloating. There was a trend towards probiotics improving bloating (SMD=−0.54; 95% CI −1.10 to 0.02, p=0.058), but this did not reach statistical significance. There was significant heterogeneity among studies (χ2=66.12, d.f.=7, p<0.001, I2=89%), but again this was due to one outlying study,25 and when it was excluded this disappeared (χ2=3.35, d.f.=7, p=0.76, I2=0%).
Six trials14 15 21 27 28 31 evaluating 566 patients reported on flatulence. Probiotics statistically significantly improved flatulence (SMD=−0.22; 95% CI −0.42 to −0.01, p=0.04) with no significant heterogeneity among studies (χ2=5.74, d.f.=7, p=0.33, I2=13%).
Three trials14 15 31 evaluating 394 patients reported on urgency. There was no statistically significant change in the scoring of urgency as a symptom compared with placebo (SMD=−0.08; 95% CI −0.3 to 0.14, p=0.49).
Adverse events associated with probiotics in IBS patients
Six trials14 15 20 21 32 33 reported that there were no adverse events in either the control or active treatment arm. Three trials12 13 27 reported on overall adverse events in 407 patients. There was no significant difference in adverse events between probiotics and placebo (RR of adverse event on probiotic=0.93; 95% CI 0.64 to 1.36). All other studies did not report on adverse events or did not provide extractable data.
Discussion
The intestine has between 1012 and 1014 organisms per millilitre, which is ∼100-fold greater than the number of eukaryotic cells in the human body.34 We provide a stable environment for our commensal bacteria and these organisms in turn are important for the host metabolism as well as intestinal and immune function.34 It is biologically plausible that gut microflora have an aetiological role in IBS and that modulating this environment may improve symptoms. This systematic review indicates that probiotics have a therapeutic benefit in improving IBS symptoms. The dichotomous data would suggest probiotics are very effective, with an NNT of 4. This is probably an overestimate, however, as there is heterogeneity in these data and possible evidence of funnel plot asymmetry, suggesting there may be publication bias, with an over-representation of small positive studies in the published literature. Furthermore, the higher quality studies reported a more modest treatment effect compared with lower quality trials. In addition, IBS is a condition that is well recognised to have a high placebo response rate to treatment in RCTs, and this may also have contributed to the small number of patients needed to treat to prevent one patient's symptoms persisting. While the NNT is likely to be >4, studies reporting continuous data still suggest that probiotics are likely to have some impact in reducing IBS symptoms. This is coherent with the effect of probiotics in other gastrointestinal disorders. Probiotics have been shown to reduce the risk of antibiotic-induced gastrointestinal symptoms,35 36 traveller's diarrhoea,37 and a systematic review and meta-analysis has demonstrated their efficacy in shortening the duration of illness in infectious diarrhoea compared with placebo or no treatment.38
The prevailing paradigms of IBS highlight the role of dysmotility and hypersensitivity.39 Lactobacillus paracasei NCC2461 was reported to attenuate postinfectious intestinal dysmotility in a mouse model.40 A number of animal models have also shown that probiotics improve visceral hypersensitivity.41–43 Lactobacillus acidophilus NCFM administration induces the expression of cannabinoid and opioid receptors on intestinal cells,44 and this may explain the effect of probiotics on visceral hypersensitivity. Subtle intestinal inflammation and subsequent neuromodulation have been hypothesised as the underlying pathology driving the pathophysiology of IBS.45 Probiotics can have potent anti-inflammatory properties,46 and Bifidobacterium infantis 35624 normalised circulating interleukin 12 (IL10) and IL12 levels in IBS patients in an RCT included in this review.22
This systematic review has several strengths. A large number of RCTs were identified, and in general the study quality was reasonable. We were also rigorous in obtaining information from the trials. The presentation of the data was not ideal in five papers14 15 22 25 31 so we obtained additional information from the authors for these. Probiotics have been evaluated in North American, European and Asian patients with IBS in both primary and secondary care. However, there are also a number of limitations of this review. The size of the therapeutic effect in the studies reporting dichotomous outcomes is uncertain due to possible publication bias. The heterogeneity in the continuous data is due to one strongly positive study,25 though it is not clear why this trial, an Italian study evaluating 68 Rome II patients with IBS using a prebiotic and probiotic cocktail, gave different results. There was ambiguity in the paper as to whether this was an RCT, but we determined that there were adequate methods of randomisation and concealment of allocation by contacting the senior author (Dr Marotta, personal communication). The main limitation of this review is that there were a variety of species, strains and doses of probiotics used, and therefore it was difficult to come to any conclusion about the optimum probiotic strategy to use in IBS.47 Individual probiotics may differ greatly in their effects on host immune function, and the reason for their potential therapeutic efficacy remains unclear. Therefore, combining the effects of probiotics in a meta-analysis may not be an appropriate method of estimating their effect on IBS symptoms. These underlying differences between probiotics may explain some of the heterogeneity we observed when data from individual RCTs were pooled. On the other hand, evaluating all RCTs of probiotics in a systematic review allows the identification of patterns that would not be apparent if trials were considered individually. The dichotomous data suggest that all probiotics have a trend for being efficacious in IBS. The continuous data suggest that Lactobacilli have no impact on symptoms, whilst probiotic combinations improve symptoms in patients with IBS. There was a trend for Bifidobacteria to improve IBS symptoms, but this effect did not reach statistical significance. The review was conservative as we decided a priori to include all doses of probiotics. One trial31 of B infantis 35624 was a dose-ranging study in which the authors found that the preparation methods had resulted in organisms being clumped together in the higher dose and inactivated in a post hoc evaluation. We still included this dose in the analysis and, had we excluded these patients, the Bifidobacteria data would have reached statistical significance. Almost all probiotic combinations contained both Bifidobacteria and Lactobacilli, and the latter did not have an effect in the continuous data meta-analysis. It is therefore possible that Bifidobacteria constitute the active treatment in probiotic combinations. Alternatively it is possible that different species of probiotics are synergistic in promoting a therapeutic effect on IBS.
Future studies need to establish which species, strain and dose of probiotics are most efficacious in IBS. Factorial designed RCTs that compare individual bacterial species with combinations are also required to establish whether probiotics can have a synergistic effect. While we need more information, this systematic review suggests that probiotic treatment is a promising strategy to treat patients with IBS.
Acknowledgments
This study was supported by funding from the American College of Gastroenterology. We thank Dr Marotta and Dr Zinsmeister for providing extra data for studies in which they were involved.
References
Footnotes
Competing interests Declared (the declaration can be viewed on the Gut website at http://www.gut.bmj.com/supplemental).