Article Text

Abstract
Background and aims Bleeding from gastric varices is often severe and difficult to manage. Endoscopic injection of gastric varices with cyanoacrylate is effective in prevention of rebleeding. The efficacy of β-blockers in secondary prophylaxis of gastric variceal bleed has not been well studied. A comparison of the efficacy of β-blocker treatment and cyanoacrylate injection for the prevention of gastric variceal rebleeding was carried out.
Methods Patients with gastro-oesophageal varices type 2 (GOV2) with eradicated oesophageal varices or isolated gastric varices type 1 (IGV1) who had bled from gastric varices were randomised to cyanoacrylate injection (n=33) or β-blocker treatment (n=34). Baseline and follow-up upper gastrointestinal endoscopy and hepatic venous pressure gradient (HVPG) measurements were performed. Primary end points were gastric variceal rebleeding or death.
Results The probability of gastric variceal rebleeding rate in the cyanoacrylate group was significantly lower than in the β-blocker group (15% vs 55%, p=0.004) and the mortality rate was lower (3% vs 25%, p=0.026) during a median follow-up of 26 months. The median baseline and follow-up HVPG in the cyanoacrylate group were 15 (10–23) and 17 (11–24) mm Hg (p=0.001) and for the β-blocker group 14 (11–24) and 13 (8–25) mm Hg (p=0.003). While no patient showed reduction of HVPG in the cyanoacrylate group, in the β-blocker group 12 of 28 (42%) patients were responders, of which 5 (41% of responders) bled. On multivariate analysis, treatment method, portal hypertensive gastropathy and size of the gastric varix >20 mm independently correlated with gastric variceal rebleeding. Gastric variceal rebleeding independently correlated with mortality.
Conclusions Cyanoacrylate injection is more effective than β-blocker treatment for the prevention of gastric variceal rebleeding and improving survival.
Clinical trial number NCT00888784.
- Cirrhosis
- endoscopy
Statistics from Altmetric.com
Introduction
Gastric varices (GVs) are less common than oesophageal varices, occurring in ∼20% of patients with portal hypertension.1 GVs bleed less frequently than oesophageal varices1; however bleeding tends to be more severe, requires more transfusions and has a higher mortality rate than oesophageal variceal bleeding.1–3 After control of acute bleeding, GVs have a high rebleeding rate (34–89%) and treatment options to prevent rebleeding are not optimised.2 4 5 The frequency and severity of bleeding from GVs depends on their location (figure 1). GVs could be associated with oesophageal varices (gastro-oesophageal varices type 1 along the lesser curve, or type 2 (GOV2), along the fundus) or are present in isolation (isolated gastric varix type 1 (IGV1), in the fundus or at ectopic sites in the stomach or the first part of the duodenum (isolated gastric varix type 2)).1

Classification of gastric varices.
β-Blockers have been reported to reduce the risk of rebleeding of oesophageal varices by ∼40% and risk of death by 20%.6–11 A small open-label trial of β-blocker and nitrate treatment in patients with GVs reported no significant benefit for rebleeding or survival, but there was a trend towards lower rebleeding.12 Endoscopic injection of cyanoacrylate has been proven to be effective in the prevention of GV rebleeding.13–17 However, cyanoacrylate injection is associated with a risk of cerebral or pulmonary embolism and damage to the endoscope.18
Results on the long-term efficacy of gastric variceal obturation with cyanoacrylate injection are variable, with eradication rates between 50% and 100% and a rebleeding rate of 23–50%, with the majority occurring in the first year.13 16 19–21 Due to the high rate of primary haemostasis and lower rebleeding rate, GV obturation with cyanoacrylate injection is used as the first-line treatment for bleeding GVs and secondary prophylaxis of GV bleed.
For patients who have bled from IGV1 or GOV2, N-butyl-cyanoacrylate, transjugular intrahepatic portosystemic shunt (TIPS) or β-blockers have been recommended.22 Endoscopic injection of thrombin has also been tried for secondary prophylaxis of bleeding from GVs.23–26 β-Blockers have been recommended empirically for GVs since they have been found to be quite effective in patients who have bled from oesophageal varices. However, there is no randomised controlled trial available comparing β-blocker treatment with endoscopic cyanoacrylate injection for prevention of rebleeding from GVs. We conducted a randomised controlled trial to study the efficacy of endoscopic cyanoacrylate injection versus β-blockers in the prevention of gastric variceal (GOV2 or IGV1) rebleeding and improvement in survival. We also investigated the predictors of rebleeding and mortality in patients who had previously bled from GVs.
Patients and methods
Patients with portal hypertension with upper gastrointestinal bleed were assessed. All consecutive patients with cirrhosis with GVs (GOV2 with eradicated oesophageal varices or IGV1) admitted to our hospital from August 2006 to March 2009 were enrolled. The study was approved by our institutional review board, and written informed consent was obtained from all patients. Parents gave the written consent for children. Patients who had bled from GOV2 or IGV1 were included. The exclusion criteria were non-cirrhotic portal hypertension, presence of oesophageal varices, contraindications to β-blockers and cyanoacrylate injection, patients already on β-blockers, past history of cyanoacrylate injection or sclerotherapy for GVs or GV ligation, TIPS, balloon-occluded retrograde transvenous obliteration (BRTO), balloon-occluded endoscopic injection sclerotherapy, shunt operation, undetermined origin of bleeding, hepatic encephalopathy grade III/IV, hepatorenal syndrome, hepatocellular carcinoma, presence of deep jaundice (serum bilirubin >10 mg/dl), cardiorespiratory failure, age >75 years, pregnancy or patients who did not give informed consent.
After assessing eligibility with initial endoscopy and subsequently obtaining informed consent patients were randomised, using a sealed envelope technique, to receive cyanoacrylate injection (Nectacryl, Nectar Laboratories, Medak, India) or β-blocker (propranolol). The allocation sequence remained with the statistician and the sequence remained concealed from the investigators until the intervention was assigned. The doctors who evaluated the outcomes were blinded to group assignment. According to the Baveno IV consensus on portal hypertension,22 secondary prophylaxis starts from the sixth day of acute variceal bleed. For patients presenting with acute GV bleeding, an emergency endoscopy was done and, if the bleeding was found to be from GOV2 or IGV1, one cyanoacrylate injection was given to control acute GV haemorrhage (not with the intention of obliterating the GV). The patients were randomised and the follow-up started from day 6 after occurrence of acute bleeding. None of the patients presenting with acute GV bleeding received β-blocker or endoscopic treatment for secondary prophylaxis from day 0 till day 6. Patients with a previous bleed were randomised after control endoscopy. For patients randomised to the propranolol group, control endoscopy was completed and propranolol was started on the same day. For patients randomised to the cyanoacrylate group, a second endoscopy with cyanoacrylate injection was performed on the same day. In patients with a history of past bleeding, the follow-up started immediately after randomisation. The follow-up period was terminated at 3 months after enrolment of the last patient.
Upper gastrointestinal endoscopy was done to determine the variceal status at baseline and repeated at 3 month intervals or during rebleeding. The size of the GV, recurrence of oesophageal varices and portal hypertensive gastropathy (PHG) were recorded. An attempt was made to localise the source of bleeding at the time of emergency endoscopy. The size of the GV was calculated by a zebra guide wire with markings made at 5 mm intervals, and we classified the fundal varix as small (<10 mm), medium (10–20 mm) or large (>20 mm). The colour of the GV was observed as red or blue. The recent signs of haemorrhage over the GV were the presence of a clot or blackish spot localised over the GV.1 The presence or absence of oesophageal varices and PHG were also evaluated. Concurrence of two independent observers was required before characterising the type of GV and its size. Rebleeding from GVs was managed with a cyanoacrylate injection in the β-blocker group and TIPS or surgery in the cyanoacrylate group.
The primary end points of the study were rebleeding from GVs or death. The actuarial probability of rebleeding from GVs and mortality were calculated. Secondary end points were increase or decrease in the size of GVs, appearance of new oesophageal varices and appearance or worsening of PHG and complications.
The diagnosis of cirrhosis was based on clinical, biochemical, radiological and histological findings. Ultrasonography of the abdomen with Doppler of splenoportal axis, CT angiography or magnetic resonance (MR) angiography was done to diagnose cirrhosis and assess spontaneous shunts. Model for end-stage liver disease (MELD) and Child–Turcotte–Pugh (CTP) scores were calculated at baseline and serial intervals.
Technique of cyanoacrylate injection
Endoscopic injection was performed intravariceally using a therapeutic endoscope and a transparent Teflon injector, with a 6–8 mm long, 21-gauge needle, with N-butyl-2-cyanoacrylate. The cyanoacrylate was injected without dilution with lipiodol. The maximum amount of cyanoacrylate injected per site was 2 ml, and the total amount of cyanoacrylate required to obliterate the GVs completely was recorded. An attempt was made to obturate the GVs completely at one session by injecting cyanoacrylate at multiple sites. If a second session was required, it was done within a week of the initial session. The injected GV was palpated using the hub of the injector with the needle retracted to look for solidification and obliteration of the GV. If the GV was not completely obturated, cyanoacrylate was reinjected till the whole GV became solidified.
β-Blocker treatment
Propranolol was started at a dose of 20 mg twice daily. The dose was increased every alternate day by 20 mg to achieve target a heart rate of 55/min or to the maximal dose of 360 mg/day if the medication was well tolerated and the systolic blood pressure was >90 mm Hg. On the occurrence of intolerable adverse effects, systolic blood pressure <90 mm Hg or pulse rate <55/min, the dose of the medication was decreased step-wise, and eventually stopped if these adverse events were disabling and persisted. Reintroduction of the medication was attempted if cessation of the drug resulted in improvement of the reported side effect. Compliance was assessed by pill count, and monitoring the heart rate and blood pressure. Patients were monitored every day until adequate β-blockade was achieved, then every month for the first 3 months and subsequently every 3 months. Patients were advised to refrain from consuming alcohol and from taking non-steroidal anti-inflammatory drugs.
HVPG measurement
After an overnight fast, HVPG measurement was performed as previously described.27 HVPG was measured and repeated after 1 year in both groups. In patients who presented with GV bleeding, HVPG was measured within 24 h. Patients were categorised into responders (≥20% reduction in HVPG or HVPG <12 mm Hg) and non-responders (<20% reduction in HVPG), and the primary end points were calculated.
Statistical analyses
The rebleeding rates following cyanoacrylate injection have been reported to be in the range of 15–25%.13–18 We hypothesised that the rate of GV rebleeding would be more in the β-blocker group (50%) in comparison with the cyanoacrylate group (15%). Thus, to achieve a statistical power of 80% with an error of 5% and drop-out rate of 20%, a sample size of 32 patients in each group was calculated.
Fisher exact test was used to compare categorical groups. Student t test and Mann–Whitney U test were used for the parametric and non-parametric data, respectively. For comparison of pretreatment and post-treatment parameters, paired Student t test was used. The Kaplan–Meier analyses and log-rank test were applied to compare the cumulative probability of rebleeding from the GV, and death. Each patient was analysed in an intention to treat manner. A p value of <0.05 was considered significant. Statistical analysis was done using SPSS, version 15.0 (SPSS, Chicago, Illinois, USA).
Results
A total of 1005 consecutive patients with portal hypertension and upper gastrointestinal bleeding presented to our hospital between August 2006 and March 2009 (figure 2). Inclusion criteria were not fulfilled in 938 patients. Sixty-seven (6.6%) patients with cirrhosis who were enrolled in the study had GVs (GOV2/IGV1) without oesophageal varices with a history of GV bleed, and were randomised to receive either cyanoacrylate injection (n=33) or β-blocker (n=34). One patient in the cyanoacrylate group and two patients in the β-blocker group refused the allocated intervention, so 32 patients with cirrhosis received the allocated treatment in each group. One patient who was lost to follow-up in the β-blocker group was included in the final analysis.

Trial profile.
Of the 64 patients, 15 presented with active bleeding from GVs and were treated with a combination of vasoactive drugs along with an emergency single injection of cyanoacrylate after endoscopic confirmation of the source of bleed from GVs as revealed by active ooze of blood (n=6), spurt (n=5) or presence of a clot (n=4). Of 15 patients presenting with acute gastric variceal bleed, eight patients were randomised to the cyanoacrylate group and seven to the β-blocker group. Of the 64 patients, 49 had a history of bleed from GVs within a 15 day period from the time of enrolment. These patients had undergone diagnostic endoscopy at the time of acute bleeding at peripheral hospitals which confirmed bleeding from GVs as shown by evidence of spurt (n=7), ooze (n=17) or presence of a clot (n=14) on GVs, and only large GVs (n=11) without any other obvious source of bleeding, such as oesophageal varices, portal hypertensive gastropathy, gastric antral vascular ectasia, gastric ulcer, gastric erosions and duodenal ulcer. However, these patients did not receive endoscopic injection of cyanoacrylate. They were managed with blood transfusions or infusion of fresh frozen plasma, and some patients received vasoactive drugs. Bleeding stopped in all the patients without endoscopic treatment. Upper gastrointestinal endoscopy performed after a median period of 7 (4–15) days showed maroon-black spots (n=26), a nipple (n=9) on GVs and only large GVs (n=14) without other obvious source of bleeding.
Baseline characteristics of both groups of patients were comparable (table 1). The median follow-up period was 26 (range 3–34) months in both the groups. The most common aetiology of cirrhosis was alcohol or cryptogenic (table 1). Four patients in the β-blocker and six patients in the cyanoacrylate group had IGV1; the rest of the patients had GOV2. The size, colour of GVs and PHG between the two groups were similar (table 1). MR portovenography and Doppler ultrasound demonstrated spontaneous lienorenal shunt in the cyanoacrylate group (n=8) and in the β-blocker group (n=11).
Baseline characteristics of study group patients
Gastric variceal obturation
Endoscopic intervention could be performed with 100% technical success. Complete obturation of GVs was achieved in all. The mean number of sessions required to achieve obliteration was 1.7±0.4 (range 1–2). The mean volume of cyanoacrylate required was 6.0±1.7 (range 3–9) ml. Mean time to obturation was 2.0±0.6 (range 1–3) days.
β-Blocker treatment
All patients were compliant to β-blocker treatment. The mean daily dose was 160 (range 80–320) mg. The median time interval to achieve the desired heart rate was 15 (range 5–20) days, and during this period no patient bled from GVs.
Gastric variceal rebleeding
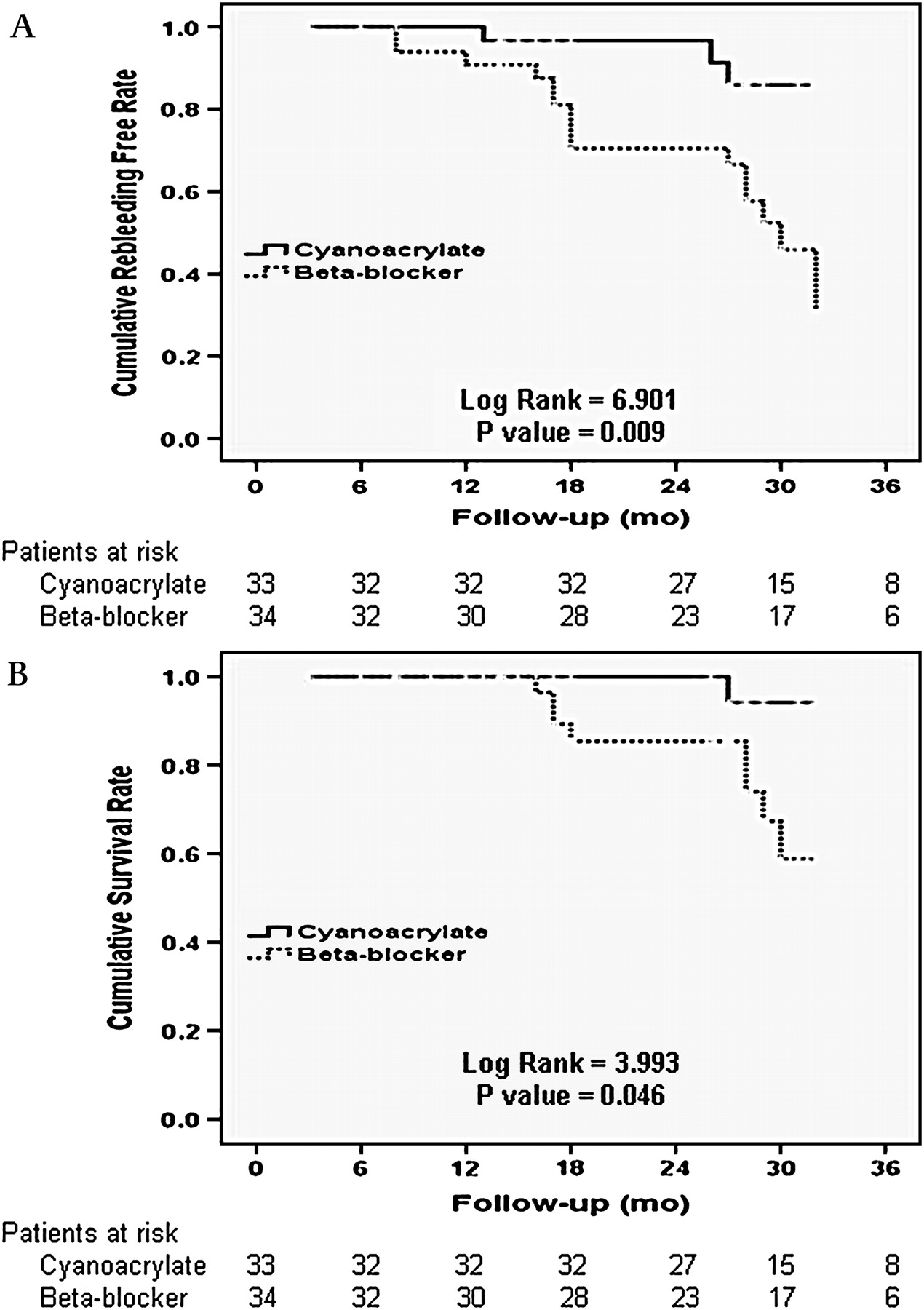
Over a median follow-up period of 26 (3–34) months, in the cyanoacrylate group 3 (9%) (GOV2 (n=2), IGV1 (n=1)) patients bled, in contrast to 15 (44%) (GOV2 (n=12), IGV1 (n=3)) in the β-blocker group. The probability of GV rebleeding was significantly lower in the cyanoacrylate group (15%) compared with the β-blocker group (55%) (p=0.004, log rank 8.466, figure 3A). The difference was also significant in the frequency of bleeding over a median follow-up period of 26 months from GOV2 between the two groups (p=0.005) (table 2). Of 34 patients in the β-blocker group 15 had rebleed, and cyanoacrylate injection was used to control rebleeding in 13 patients. In two patients, bleeding from GVs was torrential and cyanoacrylate injection could not be performed, and they were subjected to surgery. Of 33 patients in the cyanoacrylate group, two patients had a rebleed and were managed by surgery.
{kind=link}
{kind=link}
{kind=link}
Probability of freedom from gastric variceal rebleeding (A) and survival (B) in the cyanoacrylate and β-blocker group.
Results of treatment in the cyanoacrylate and β-blocker groups
Size of gastric varix
Over a median follow-up period of 26 (3–34) months in the cyanoacrylate group all patients had a decrease in GV size (table 2) and the median size of GVs decreased from ∼25 (10–35) to ∼5 (0–10) mm (p<0.01). In the β-blocker group, 15 of 34 (44%) patients had an increase in size of GVs and the size of GVs increased from a median of 25 (10–35) to 30 (15–40) mm (p<0.01). All patients bleeding from GVs in the β-blocker group had an increase in size of at least 5 mm.
Appearance of oesophageal varices and PHG
Over a median follow-up period of 26 (3–34) months in the cyanoacrylate group, 7 of 33 (21%) and in β-blocker group 4 of 34 (11%) patients developed oesophageal varices on follow-up (p=0.302). All patients had small oesophageal varices and did not bleed. No significant difference was noted between the cyanoacrylate group (24%) and the β-blocker (21%) group regarding appearance or worsening of PHG (table 2).
Hepatic venous pressure gradient
Baseline HVPG was measured in 27 patients in the cyanoacrylate group (three patients refused and, in another two patients, the hepatic vein could not be cannulated) and in 28 patients in the β-blocker group (three patients refused and in another one patient the hepatic vein could not be cannulated). Follow-up HVPG was measured in 23 patients in the cyanoacrylate group (three patients refused HVPG measurement and in one patient the hepatic vein could not be cannulated) and in 28 patients in the β-blocker group. Median baseline HVPG was 15 (10–23) mm Hg and follow-up HVPG was 17 (11–24) mm Hg in the cyanoacrylate group. The increase in HVPG on follow-up in the cyanoacrylate group was significant (p=0.001). The median baseline HVPG was 14 (11–24) mm Hg and follow-up HVPG was 13 (8–25) mm Hg in the β-blocker group. The decrease in HVPG on follow-up in the β-blocker group was significant (p=0.003). In the cyanoacrylate group, 22 of 27 (81%) patients had HVPG >12 mm Hg at baseline and 22 of 23 (91%) patients had HVPG >12 mm Hg on follow-up. In the β-blocker group, 24 of 28 (85%) patients had HVPG >12 mm Hg at baseline and 18 of 28 (64%) patients had HVPG >12 mm Hg on follow-up.
Response to treatment and rebleeding
In the cyanoacrylate group, none of the patients responded to treatment in the form of reduction in HVPG. In the β-blocker group, 12 of the 28 (42%) patients were responders. However, 5 (41%) responders bled during follow-up. Of the non-responders, 2 of 23 (8%) patients in the cyanoacrylate group and 8 of 16 (50%) patients in the β-blocker group bled. In responders, the median baseline HVPG was 16 (12–22) mm Hg and the follow-up HVPG was 12 (8–16) mm Hg. A >20% reduction in HVPG was achieved in 12 of 28 (42%) patients in the β-blocker group. In non-responders in the β-blocker group, the median baseline HVPG was 14 (11–24) mm Hg and the follow-up HVPG was 13.5 (10–25) mm Hg. Of the responders who bled, one had IGV1 and the other four had GOV2. Those responders who did not bleed had a mean decrease in HVPG from baseline of 30% in comparison with a 22% decrease in those who bled. In patients with IGV1, the baseline median HVPG was 13 (11–17) mm Hg and in patients with GOV2 the baseline median HVPG was 14 (10–24) mm Hg.
Since all the patients were bleeders, it was interesting to note that patients with spontaneous shunt (n=21) at baseline had a lower median HVPG (13 (10–15) mm Hg) than patients without spontaneous shunt (n=43) (18 (13–24) mm Hg (p=0.001)). Thus, the HVPG levels which predict the likelihood of rebleeding in patients with or without shunt are 13 and 18 mm Hg, respectively. In patients with spontaneous shunt, 6 of 21 (28%) patients had a HVPG value of <12 mm Hg. In patients without spontaneous shunt, all had HVPG >12 mm Hg. Overall, 20% of patients who bled had a HVPG <12 mm Hg. Patients with cirrhosis who bled had a median HVPG of 15 (11–24) mm Hg at baseline and 14 (9–25) mm Hg (p=0.715) at follow-up. In non-bleeders, the median HVPG at baseline was 14 (10–23) mm Hg and follow-up HVPG was 13.5 (8–22) mm Hg (p=0.031). HVPG decreased in 5 of 10 (50%) patients in the β-blocker group with spontaneous shunt.
Complications
No significant difference in the frequency of complications was observed between the two groups. One (3%) patient in the cyanoacrylate and 2 (6%) patients in the β-blocker group developed spontaneous bacterial peritonitis, and improved on treatment (table 2). Four patients in the β-blocker group developed headache and generalised weakness which was controlled with dose reduction, and after 2–3 weeks the desired dose was achieved. No serious adverse effects were noticed which required stoppage of β-blocker.
Mortality
Over a median follow-up period of 26 (3–34) months, a significant difference in the overall mortality was observed between the cyanoacrylate (n=1, 3%) and the β-blocker (n=8, 25%) group (p=0.016, log rank=5.808, figure 3B). Of 15 patients with rebleeding in the β-blocker group, treated with cyanoacrylate injection, 6 (19%) patients died in comparison with none in three of 33 patients in the cyanoacrylate group (p=0.024) who were managed with surgery at the time of rebleeding. In the β-blocker group, one patient died of hepatic encephalopathy and one patient died of spontaneous bacterial peritonitis and hepatorenal syndrome. In the cyanoacrylate group, one patient died of hepatic encephalopathy. The cumulative 2-year survival rate was 90% in the cyanoacrylate group and 52% in the β-blocker group. In the β-blocker group, only one patient died among responders compared with seven patients among non-responders (p=0.077).
Predictors of GV rebleed and mortality
On univariate analysis, the variables which influenced GV rebleeding were size of the GV >20 mm, a red or black spot over the GV, blue colour of the GV, presence of PHG, international normalised ratio (INR) ≥1.6, serum creatinine >1 mg/dl, CTP score ≥9, MELD score ≥17 and the treatment method. On multivariate analysis, the treatment method (p=0.006), PHG (p=0.029) and size of the GV >20 mm (p=0.002) independently correlated with GV rebleeding. Variables which influence survival on univariate analysis included GV rebleeding, presence of PHG, CTP ≥9, MELD score ≥17 and the treatment method. On multivariate analysis, GV rebleeding (p=0.003) independently correlated with mortality.
Discussion
The results of this large prospective randomised controlled clinical trial comparing the efficacy of cyanoacrylate and β-blocker treatmjent clearly demonstrate that endoscopic injection of cyanoacrylate is significantly more effective than β-blocker treatment for the prevention of rebleeding from GVs.
Small studies have reported that drug treatment is effective in the prevention of GV rebleeding after successful endoscopic injection of the bleeding varix with tissue adhesives.12 28 A small open-label trial of β-blocker and nitrate treatment reported no significant benefit in terms of risk of rebleeding or survival.12 This study had several limitations such as a small sample size, retrospective analysis, fixed and low doses of drug and lack of haemodynamic monitoring. In another study, Evrard et al randomised patients to receive 160 mg/day of propranolol (n=20) or histoacryl injection (n=21) for secondary prophylaxis of gastro-oesophageal variceal bleed.28 The rebleeding and mortality rates were similar in the β-blocker and endoscopic treatment groups, with a higher complication rate in the latter (10% vs 47%). This study had limitations of early termination due to increased complications in the histoacryl arm, no haemodynamic monitoring and inclusion of patients with co-existing oesophageal varices. In fact, all patients had oesophageal varices, and 17 had GVs (12 with GOV1 and 5 with GOV2).
The median baseline HVPG was 14.5 (10–24) mm Hg. Of 55 patients with bleeding from gastric varices, 16% had baseline HVPG <12 mm Hg. Patients with gastric variceal bleed have been shown to have lower HVPG than patients with bleeding from oesophageal varices.29 In addition, ∼35% of patients with gastric variceal bleed have portal pressure <12 mm Hg.29 Spontaneous splenorenal or gastrorenal shunts commonly develop between the splenic vein (splenorenal shunt) and gastric varices, respectively, and connect via the inferior phrenic or suprarenal vein to the left renal vein.30 These shunts are seen in up to 60% of patients with GVs.30 31 We found spontaneous shunts in 33% of our patients. Median HVPG in patients with spontaneous shunts was lower in comparison with those without shunts (13 vs 18 mm Hg). In fact, HVPG was high in patients with both GOV2 and IGV1 types of varices. Of the 15 patients who bled, 20% had HVPG of <12 mm Hg.
There are limited data on the efficacy of β-blockers in reduction of portal pressure in patients with GVs. Keeping this in view, HVPG was measured to assess the response to β-blocker treatment in all our patients with GVs. The median HVPG was significantly reduced on follow-up; however, this could not prevent GV rebleeding or mortality. Of the 12 responders to β-blocker, five patients who rebled had a median decrease in HVPG of 22% compared with 30% in seven patients who did not rebleed. This raises the question of whether a 20% reduction in HVPG is adequate to define a response to β-blocker in patients with GVs, or whether it should be a >25% reduction. In the cyanoacrylate group, HVPG increased on follow-up, however without an increase in the frequency of rebleeding. This increase in HVPG could be attributed to redistribution of blood flow in the portal system and indirectly suggests adequacy of GV obturation. Whether addition of a β-blocker to prevent the rise in HVPG by cyanoacrylate injection will be helpful needs further studies.
BRTO and balloon-occluded endoscopic injection sclerotherapy have shown good results for prophylaxis of high risk fundal variceal bleed.31 32 In a prospective trial, Hong et al showed that the therapeutic efficacies of glue and BRTO for the treatment of active gastric variceal haemorrhage and/or high-risk GV appeared to be similar. However, glue might be associated with a higher rebleeding rate than BRTO, and BRTO could be an effective rescue treatment for patients with gastric variceal haemorrhage after initial treatment with glue.32 TIPS has been found to be quite effective in the prevention of GV rebleeding, not only by reducing the portal pressure, but also by allowing the possibility of obliterating gastric variceal channels. In a randomised controlled trial (patients with both oesophageal varices and GVs), Lo et al showed that TIPS was more effective than glue injection in preventing rebleeding from GVs, with similar survival and frequency of complications.33 However, all these procedures are quite expensive, need expertise and are associated with complications over time.18 29 32–35 Cyanoacrylate injection, on the other hand, is easily available, rapid, cost-effective, requires less expertise, is less invasive and has been shown to be very effective in preventing GV rebleeding.13 16 19–21 34
Endoscopic variceal sclerotherapy is inappropriate for patients with fundal varices.5 19 The randomised trials by Tan et al and Lo et al compared histoacryl injection and variceal band ligation and reported a rebleeding rate almost twice higher with ligation for secondary prevention of bleeding from GVs.13 36
Generally not more than 2 ml of cyanoacrylate should be injected at a single site to prevent embolic and thrombotic complications.37 38 Precautions to prevent damage to the endoscope must be taken during cyanoacrylate injection. By avoiding lipiodol use, limiting the total volume per injection and by proper monitoring, no embolic complication was observed in our study population. Dilution of cyanoacrylate with lipiodol delays solidification by 15–20 s, thus increasing the chances of distal embolisation. In the undiluted form, it solidifies within 5–7 s, and thus the chances of distal embolisation become almost negligible. However, with undiluted cyanoacrylate injection, there is a risk of needle impaction in GVs at the time of injection.39
β-Blocker treatment was well tolerated and none of our patients required withdrawal of treatment. In the cyanoacrylate group, 21% of patients had appearance of new oesophageal varices in comparison with 11% in the β-blocker group, although none of the patients bled from oesophageal varices. The frequency of PHG in both the groups was similar (24% vs 21%).
Survival in the cyanoacrylate group was better because of a low frequency of rebleeding compared with the β-blocker group. In both the groups, differences in mortality were due to rebleed-related deaths. However, mortality due to other causes (not rebleed related) was similar in both the groups. More favourable survival in our patients could be due to close follow-up during the study period and the fact that ∼50% of the patients with cirrhosis in both the groups were Child A and B.
The stronger aspects of our trial are that it was a randomised controlled study and had a large sample size, a longer follow-up period and a minimal drop-out rate. The weaker aspect of this study is inclusion of only a selective patient group with IGV1 and GOV2 types of GVs. The applicability of the present study is related only to patients with bleeding GVs of GOV2 and IGV1 types. GVs of GOV2 and IGV1 types are more common, and associated with more frequent and more severe bleeds with higher mortality rates as compared with other types of gastric varices.1
In conclusion, the results of our study clearly demonstrate that cyanoacrylate injection is more effective in the prevention of rebleeding from GVs and improving patient survival as compared with β-blocker treatment. Propranolol is not effective in preventing gastric variceal rebleeding despite reduction in HVPG.
Significance of this study
What is already known about this subject?
The efficacy of β-blockers in secondary prophylaxis of gastric variceal bleeding has not been well studied.
Endoscopic injection of cyanoacrylate has been proven to be effective in the prevention of gastric variceal rebleeding.
β-Blockers have been recommended empirically for prophylaxis of gastric variceal bleeding without proof.
What are the new findings?
The probability of rebleeding from large gastro-oesophageal varices type 2 (GOV2) or isolated gastric varices type 1 (IGV1) was significantly lower in the cyanoacrylate group (15%) compared with the β-blocker group (55%).
The majority of patients with such gastric varices have baseline HVPG >12 mm Hg.
Cyanoacrylate injection increases the hepatic venous pressure gradient (HVPG), and β-blocker decreases HVPG significantly on follow-up.
Mortality in patients treated with a β-blocker is higher than with cyanoacrylate injection.
How might it impact on clinical practice in the foreseeable future?
Endoscopic injection of cyanoacrylate should be used to prevent rebleeding from large GOV2 and IGV1 and improve survival.
β-Blockers are not effective in prevention of rebleeding from such gastric varices, although they decrease HVPG in these patients.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the MAMC Ethical Committee, New Delhi.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest