Article Text

Abstract
Background: Continued or recurrent bleeding after endoscopic treatment for bleeding ulcer is a major adverse prognostic factor. Identification of such ulcers may allow for alternate treatments.
Aim: To determine factors predicting treatment failure with combined adrenaline injection and heater probe thermocoagulation.
Methods: Consecutive patients with bleeding peptic ulcers who received endoscopic therapy between January 1995 and March 1998 were studied. Data on clinical presentation, endoscopic findings, and treatment outcomes were collected prospectively. Multiple logistic regression analysis was used to identify independent risk factors for treatment failure.
Results: During the study period, 3386 patients were admitted with bleeding peptic ulcers: 1144 (796 men, 348 women) with a mean age of 62.5 (SD 17.6) years required endoscopic treatment. There were 666 duodenal ulcers (58.2%), 425 gastric ulcers (37.2%), and 53 anastomotic ulcers (4.6%). Initial haemostasis was successful in 1128 patients (98.6%). Among them, 94 (8.2%) rebled in a median time of 48 hours (range 3–480). Overall failure rate was 9.6%. Mortality rate was 5% (57/1144). Multiple logistic regression analysis revealed that hypotension (odds ratio (OR) 2.21, 95% confidence interval (CI) 1.40–3.48), haemoglobin level less that 10 g/dl (OR 1.87, 95% CI 1.18–2.96), fresh blood in the stomach (OR 2.15, 95% CI 1.40–3.31), ulcer with active bleeding (OR 1.65, 95% CI 1.07–2.56), and large ulcers (OR 1.80, 95% CI 1.15–2.83) were independent factors predicting rebleeding.
Conclusions: Larger ulcers with severe bleeding at presentation predict failure of endoscopic therapy.
- upper gastrointestinal bleeding
- endoscopic therapy
- rebleeding
- treatment failure
- ROC receiver operating characteristic
Statistics from Altmetric.com
Bleeding peptic ulcer is a common and life threatening medical emergency. Endoscopic haemostasis has significantly improved the outcome of patients with bleeding peptic ulcers.1–,3 While endoscopic therapy can stop bleeding in most bleeding ulcers, 10–20% of patients continue to bleed or rebleed after initial control. Recurrent bleeding remains the single most important adverse prognostic factor.4 Mortality in these patients increases substantially. Identification of such patients may allow for alternate treatment strategies to prevent recurrent bleeding.
In a randomised study, we demonstrated that adding heat probe thermocoagulation after adrenaline injection was more effective compared with adrenaline injection alone.5 In this prospective study, we sought to determine factors that may predict therapeutic failure after the combined treatment.
PATIENTS AND METHODS
The Prince of Wales Hospital is a teaching hospital that serves a catchment population of 1.2 million. All patients presenting with upper gastrointestinal bleeding are admitted under the joint care of medical and surgical gastroenterologists. All patients underwent endoscopy within 24 hours of admission. Patients who presented with fresh haematemesis or circulatory instability underwent emergency endoscopy after initial resuscitation. Twelve experienced endoscopists proficient at endoscopic treatment of bleeding peptic ulcers formed our gastrointestinal bleeding roster. Treatment procedures were performed by these endoscopists or training registrars under their supervision. Actively bleeding ulcers, ulcers with non-bleeding visible vessels (defined as protuberant discolourations) were treated. Clots were lifted by targeted irrigation with a heater probe or mechanically with the use of a mini-snare. Adrenaline (1:10 000 dilution) was injected in 0.5–1 ml aliquots into and around the bleeding point. Active bleeding usually ceases allowing a clear view of the bleeding vessel after which tamponade is firmly appied using a 3.2 mm heat probe (CD-10Z; Olympus, Tokyo, Japan) using a dual channel endoscope (2T-10 or 2T-200; Olympus). Coagulation at 30 J is then activated. A continuous set of three pulses are applied to any one site. Successful treatment was defined by cessation of bleeding and flattening or “cavitation” of the bleeding point. After treatment, patients were returned to the surgical gastroenterology ward for monitoring. Haemoglobin level was monitored daily and blood transfusion was given to maintain a haemoglobin concentration of approximately 10 g/dl. A policy of early feeding was adopted and oral omeprazole (Losec; Astra, Sweden) with or without Helicobacter pylori eradication therapy were prescribed.
Permanent haemostasis was defined as successful initial haemostasis and absence of recurrent bleeding within the period of hospitalisation. Primary failure was defined as failure to stop bleeding during the index endoscopy and these patients underwent immediate surgery. Recurrent bleeding was defined by one of the following: fresh haematemesis, hypotension (systolic blood pressure <90 mm Hg) with tachycardia (pulse >110 beat/min) or with melena, or a total transfusion requirement of greater than 4 units to maintain a haemoglobin level of approximately 10 g/dl within 72 hours after endoscopic treatment. No comparative trial of endoscopic treatments was in progress during the study period. Patients who developed recurrent bleeding after initial endoscopic control were then recruited into a randomised study comparing emergency surgery and endoscopic retreatment.6 A uniform treatment protocol ensured that patients enrolled into this subsequent trial had been treated in an identical manner prior to their trial entry.
Patient baseline characteristics and details of endoscopic treatment were recorded by endoscopists at the end of each therapeutic procedure. Our fulltime research nurses entered data daily in our gastrointestinal bleeding registry and followed the patient's hospital course and outcome until discharge or death. This was cross checked against a computerised hospital record on patient discharges or deaths. Data were analysed using the S-Plus (MathSoft Inc, Seattle, Washington, USA). Factors predicting therapeutic failure were first identified using univariate analysis. Those with p values less than 0.25 were then entered into a stepwise multiple logistic regression. Significant independent factors were considered when p<0.05.
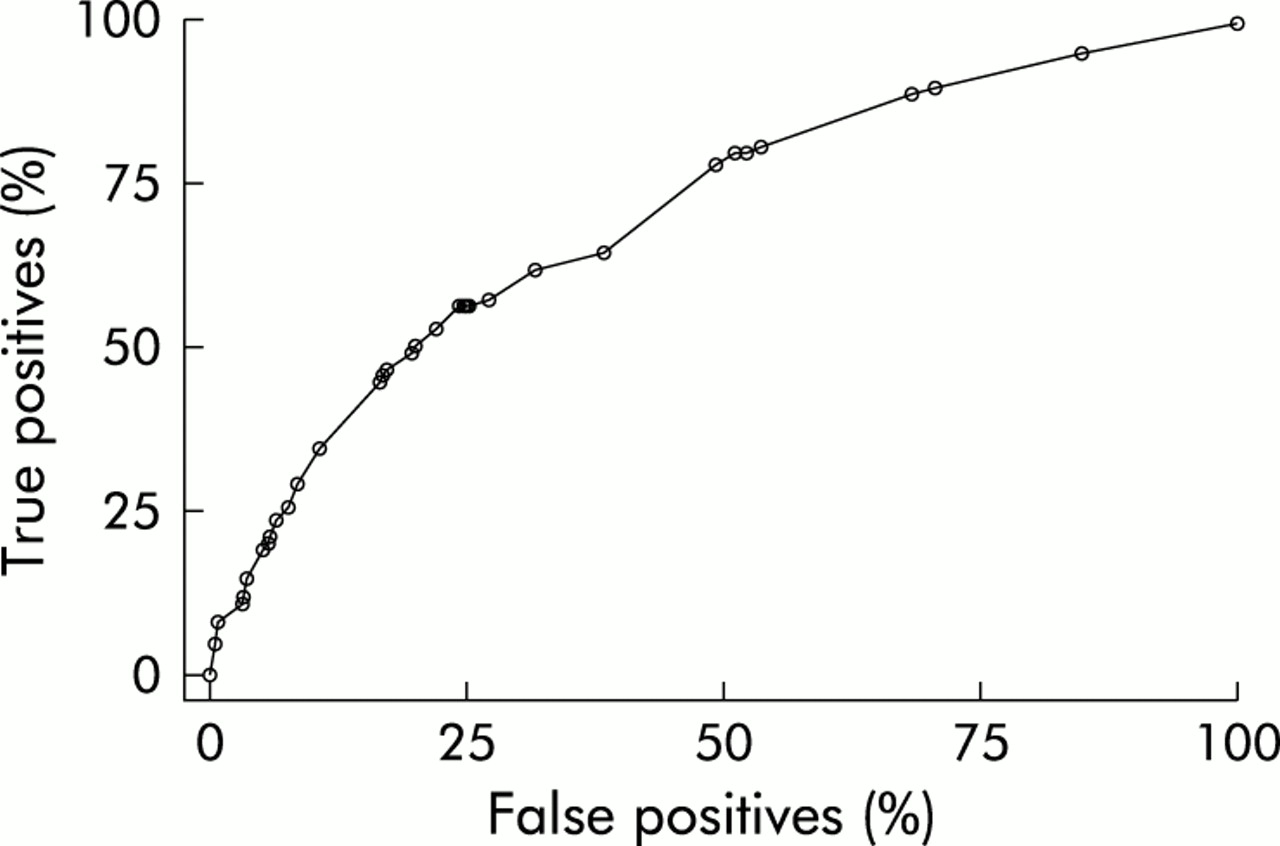
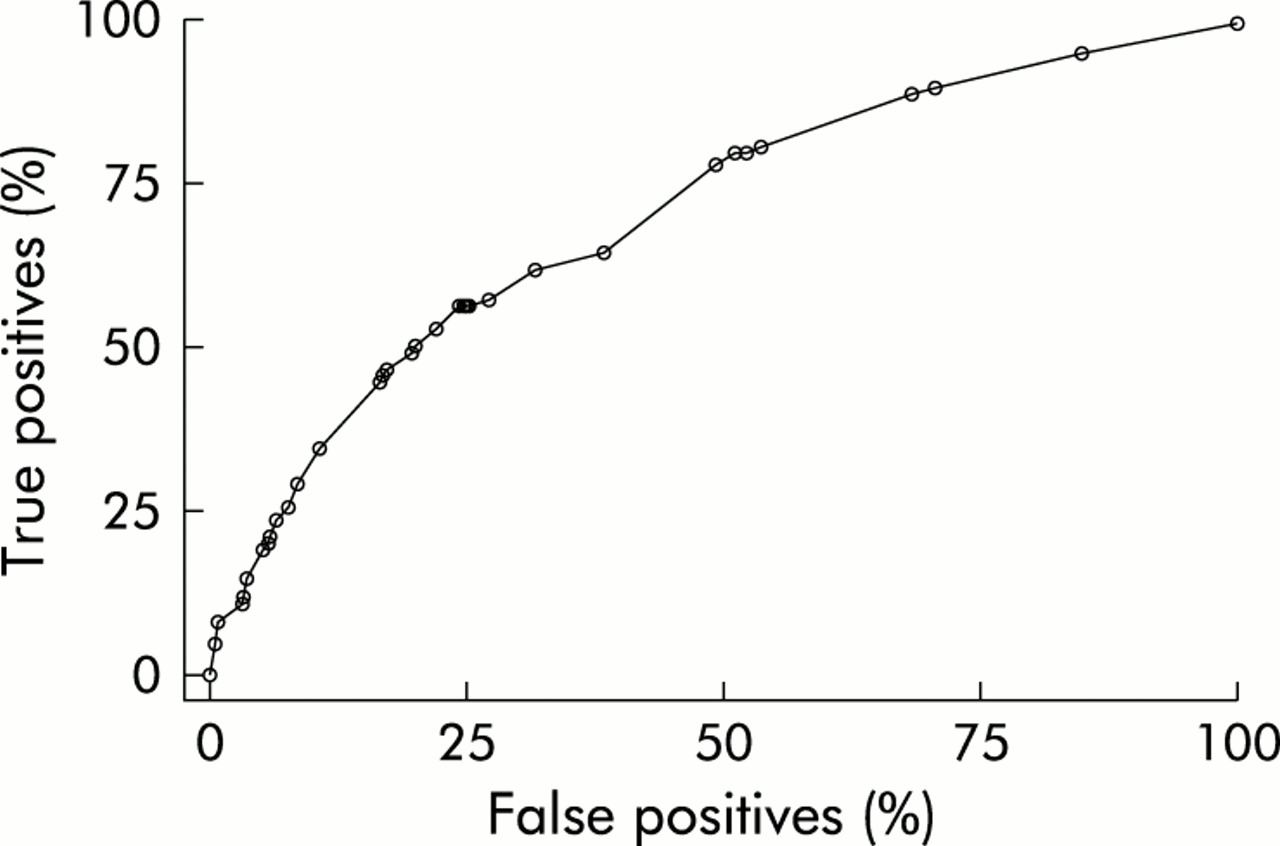
The predictive ability of the final prognostic model was assessed by means of the area under the receiver operating characteristic (ROC) curve7 and was validated using the bootstrapping technique to correct for possible bias due to overestimation of the predictive performance of the final model.8 An area under the ROC curve value of 0.5 indicates no predictive power whereas a value of 1.0 indicates excellent prediction.
In recent years there has been concern regarding how well a prognostic model works in practice and it is widely recommended that they need to be validated. The bootstrapping technique is a method being used increasingly in the context of internal validation of a prognostic model. The method involves selecting a random sample, the bootstrap sample, of 1144 observations from the original dataset with replacement into the final model. A stepwise logistic regression model is then derived from this bootstrap sample, and the predictive performance is evaluated on the bootstrap sample, ROCboot, and on the original dataset, ROCorg. The difference between the two predictive performances (that is, ROCboot−ROCorg) yields a bias statistic. This process was repeated 500 times and an average bias was calculated over the 500 bootstrap samples, ROCbias. The bootstrap corrected performance of the prognostic model was calculated by subtracting ROCbias from the area under the ROC derived from the original stepwise logistic regression model.
RESULTS
During the study period there were 3386 patients with bleeding peptic ulcers. Of these, 1144 (796 men, 348 women) required endoscopic treatment. Mean age was 62.5 (SD 17.6) years. A total of 466 patients had a previous history of peptic ulcer disease (40.7%) and 349 (30.5%) were receiving non-steroidal anti-inflammatory drugs or aspirin. There were 425 gastric ulcers (37.2%), 666 (58.2%) duodenal ulcers, and 53 (4.6%) anastomotic ulcers.
Therapy could not be completed in 16 patients (1.4%) due to torrential bleeding that prevented adequate visualisation of the ulcers and all were treated by emergency surgical haemostasis. Successful initial haemostasis was achieved in 1128 patients (98.6%) and permanent haemostasis was achieved in 1034 (90.4%). Ninety four patients (8.2%) developed inhospital rebleeding at a mean time of 60 hours (SD 68) after the index endoscopy.
Heater probe related perforations occurred in 14 patients (1.4%) (three after repeat endoscopic therapy) and all underwent emergency surgery. In those in whom permanent haemostasis was achieved, 3.8% (39/1034) died from their comorbid illnesses. Of 110 patients in whom endoscopic haemostasis failed, mortality was 16.4% (18 deaths). Overall mortality was 5.0% (57/1144 patients).
In a univariate analysis, the clinical variables age (p=0.036), haemoglobin concentration at presentation (p<0.001), hypotension (p<0.001), and fresh haematemesis (p=0.042), and four endoscopic variables (presence of fresh blood or clots in the stomach (p<0.001), ulcers with active bleeding (Forrest's grade I; p<0.001), ulcer size greater than 2 cm (p=0.002), and anastomotic ulcers (p=0.029)) were significantly related to therapeutic failure (tables 1, 2⇓⇓). Further analysis using a multiple stepwise logistic regression model showed that hypotension (p<0.001; odds ratio (OR) 2.21, 95% confidence interval (CI) 1.40–3.48), haemoglobin level less that 10 g/dl (p=0.007; OR 1.87, 95% CI 1.18–2.96), fresh blood in the stomach (p<0.001; OR 2.15, 95% CI 1.40–3.31), ulcer with active bleeding (p=0.025; OR 1.65, 95% CI 1.07–2.56), and large ulcers ≥2 cm (p=0.010; OR 1.80, 95% CI 1.15–2.83) were found to be independent variables predicting therapeutic failure (table 3⇓). The risk of failure increased twofold with each additional risk factor. The area under the ROC curve of the logistic regression model was 70.6% (fig 1⇓) and the corrected area of the ROC curve from 500 bootstrap samples was 67.5%, which suggested that the original predictive performance was overestimated by approximately 3%.
Univariate analysis: clinical and endoscopic factors related to failure of dual endoscopic therapy
Univariate analysis: ulcer size and location in gastric and duodenal ulcers
Risk factors predicting therapeutic failure of endoscopic haemostasis from stepwise logistic regression
{kind=link}
Receiver operating characteristic (ROC) curve for prediction of therapeutic failure.
DISCUSSION
In about 80% of patients with bleeding peptic ulcers, bleeding stops spontaneously. Endoscopic intervention is targeted at those bleeding at endoscopy or at risk of developing further bleeding. The National Institutes of Health consensus conference recommended that only ulcers with active bleeding or visible vessels should be treated endoscopically.1 Recent evidence indicates that patients with ulcer of an adherent clot may also constitute a high risk group.9 Various modalities of endoscopic therapies have been proved to reduce recurrent bleeding, the need for surgery, and mortality (on meta-analyses). In our institution, we combine the use of adrenaline injection and thermocoagulation by heater probe. Preinjection with diluted adrenaline in the vicinity of the bleeding stops the bleeding, allowing a clear view, and accurate and firm tamponade. In our series, endoscopic adrenaline injection with heater probe treatment achieved permanent haemostasis in 90.4% of patients with a mortality rate of 5%.
Our cohort of patients was younger than those of contemporary series. The National UK Audit conducted in 1993 was a population based study consisting of 4185 patients collected over a four month period.10 Their mean age was 66 years compared with 63 years in our series. It is well documented that old age is associated with increased mortality. Elderly patients often succumb to their concomitant illnesses rather than the bleeding itself. While old age predicts mortality, it does not predict failure of endoscopic therapy in most series. In a large series of unselected patients, Choudari and colleagues11 found no differences in the outcome of patients in different age groups (<60, 61–74, or >75 years) treated endoscopically. The authors suggested that age did not influence the response to or death after endoscopic treatment.
Several studies have defined factors that predict failure before endoscopic therapy12, 13 or after different treatment regimens.14–,18 These factors were related to high risk ulcers (ulcer size/bleeding stigmata/position) with signs of massive bleeding (hypotension/ haematemesis/low haemoglobin level) or to patient characteristics (age/comorbidities/non-steroidal anti-inflammatory drug user). Similar factors were reported as significant in predicting rebleeding.12–,18 Of the factors evaluated in these studies, one of the most consistent predictors of rebleeding was the position of the ulcer at the posterior duodenal bulb. This would seem logical as larger ulcers in this location would erode into branches of the gastroduodenal artery complex. This factor however was not significant in our analysis. This may be attributed to the unreliability of reporting ulcer location at the duodenal bulb at endoscopy.19 From our analysis, the principal determinants for recurrent bleeding appeared to be ulcer related while mortality was more related to rebleeding and patient age.10 Endoscopic therapy was most likely to fail for larger ulcers with rapid bleeding manifested by hypotension and low haemoglobin level.
Our prognostic model should ideally be validated prospectively in another cohort of patients. We choose to use the bootstrapping technique for internal validation of the final model. The corrected area of the ROC was 67.5%, indicating fair predictive performance.
Heater probe related perforation occurred in 1.4% of our patients. This value is in keeping with those from other series. Zuccaro20 summarised series using thermocoagulation and found a similar perforation rate of 1%. In our experience, perforation often occurs at the thinner anterior duodenal wall. In the clinical setting, it is often difficult to distinguish a perforation from transmural thermal injury related to heater probe treatment from a sealed perforation reopened by gas insufflation during endoscopy. Larger chronic ulcers often involve the full thickness of the bowel wall. Their ulcer craters are technically outside the bowel wall. Our heater probe setting and technique have been reported by Johnston and colleagues21 based on experimental findings.
There is little controversy concerning the management course of patients with actively bleeding ulcers that fail to stop at the index endoscopy. Most would agree that these patients should undergo surgical treatment. The preferred line of management of ulcer haemorrhage after endoscopic haemostasis is not yet defined. Variables identified in this and other reports enable us to define high risk patients. Early elective surgery in these patients seems logical as mortality from elective surgery is likely to be substantially lower than that from emergency surgery. There are however few data in the literature to support such an approach. The role of second look endoscopy is unclear. Published studies on the use of routine second look endoscopy consist of inadequate patient numbers.22–,24 The difference is likely to be marginal. With more effective index therapy, the gain from routine second look endoscopy would be evener smaller, and significant proportions of patients are likely to undergo unnecessary endoscopies.
In our series, heat probe related perforation during initial endoscopic haemostasis was approximately 1% but in our randomised study comparing endoscopic retreatment with surgery in rebleeding patients6 perforations from repeated heater probe use occurred in 2/44 patients (4.5%) and both were duodenal ulcers in the anterior wall. Contact thermal devices should be used with great caution. For this reason and because of its unproved benefit, we do not advocate routine second look endoscopy. It would seem more logical to be selective in offering repeat endoscopy. In a randomised study consisting of a smaller number of patients, Saeed and colleagues25 adopted an approach of scheduled retreatment to high risk patients based on a composite clinical and endoscopic score and demonstrated a significant benefit in the prevention of rebleeding. In a randomised study comparing endoscopic retreatment with surgery in rebleeding patients from this same cohort, second look and retreatment at the time of recurrent bleeding caused haemostasis in approximately 75% of patients. Outcomes in both groups of patients were similar. A regression analysis indicated that ulcers greater than 2 cm and hypotension at recurrent bleeding were independent factors predicting retreatment failure.5 One could argue that these patients could be better served if they had undergone elective surgery to forestall rebleeding. Recently, we demonstrated that after initial endoscopy to control bleeding ulcers, high dose infusion of proton pump inhibitors substantially reduced recurrent bleeding and improved patient outcome.26 With a low rebleeding rate of about 5% and only approximately 10% in ulcers greater than 2 cm in size in patients on maximal acid reduction, we feel that this may represent the best treatment strategy after initial endoscopic control.
Acknowledgments
We thank Bing-Yee Suen, BSc, RN, Man-yee Yung , RN, and Suki Yu for technical and secretarial assistance.