Article Text

Abstract
Aims: To determine whether an adequate histological diagnosis of gastric polyps can be attained on the basis of forceps biopsy.
Patients and methods: In a prospective multicentre study, 194 patients with 222 endoscopically removable gastric polyps (≥5 mm) underwent forceps biopsy and complete polypectomy. Patients with fundic gland polyps and polyposis syndrome were not included. Specimens were evaluated by primary and reference pathologists, and the complication rate of gastric polypectomy was also determined.
Results: Of the 222 polyps, histological examination of the polypectomy specimens revealed tumour-like lesions in 77% (10% focal foveolar hyperplasia, 59% hyperplastic polyps, 4% inflammatory fibroid polyps, 4% other polyps) and neoplasia in 19% (10% tubular adenoma, 2% tubulovillous adenoma, 1% high grade intraepithelial neoplasia, 6% adenocarcinoma). When biopsy results were compared, complete agreement was found in 124 cases (55.8%) and, in an additional 77 cases (34.7%), the clinically important differentiation between tumour-like lesions and neoplasia was possible. However, relevant differences were found by the reference pathologist in six cases (2.7%), the most common reason being failure of biopsy to reveal foci of carcinoma in hyperplastic polyps. Bleeding was observed after polypectomy in 16 patients (7.2%), in 15 of whom it was managed conservatively.
Conclusions: We recommend complete removal by an experienced endoscopist of all epithelial gastric polyps larger than 5 mm after thorough individualised risk-benefit analysis.
- gastric polyps
- stomach neoplasms
- gastroscopy
Statistics from Altmetric.com
Recommendations for diagnosis and treatment of epithelial gastric polyps remain controversial as there is no consensus regarding their malignant potential or the reliability of endoscopic forceps biopsy.1–4 According to the classification of gastric tumours and polyps established by the WHO,5 the frequency of malignant transformation depends on histological type. The risk has been reported to be 0–8.6% (mean 2.1%) for hyperplastic polyps,4,6–13 approximately 5% for tubular adenomas, and 28.5–40% for villous adenomas and pyloric gland adenomas.6,13–18 A precise histological classification therefore is essential for therapeutic action. Especially important is the reliability of the histological rating of forceps biopsy sampling with regard to the total polyp.
The present study represents the first multicentre investigation to examine prospectively the accuracy of the histological evaluation of forceps biopsy sampling from gastric polyps in comparison with endoscopic polypectomy. To estimate the risk-benefit ratio of the latter procedure, complications were also documented.
METHODS
We studied 194 patients with a total of 222 gastric polyps. Altogether 28 study centres (13 hospitals and 15 gastroenterologists in private practice) were involved, each yielding a median of six polyps (1–37). Histological assessment of the polyps was performed by pathologists in nine departments of pathology. Every gastric polyp considered amenable to polypectomy (≥5 mm) by the study participants was included. According to endoscopic criteria, those located submucosally were not included. Patients with polyposis syndrome and carcinoid tumours of the stomach were excluded. In addition, fundic gland polyps were also excluded as they are usually smaller than 5 mm and can readily be removed completely with biopsy forceps.18 The histopathological assessment of the biopsy material and polyps was performed by the pathologist chosen by each study centre (the primary pathologist). As both specimens were to be evaluated independently of each other, the total polyp was sent to the pathologist only after the biopsy result was received. In preparation for the histopathological examination, the biopsy samples and polyps were fixed in neutral 10% buffered formalin and embedded in paraffin. The 4 μm sections were stained with haematoxylin and eosin. Sections were assessed according to the WHO classification of gastrointestinal tumours published in 1990.5 After completion of the study, the WHO classification was revised19 and the term “dysplasia” was replaced with “intraepithelial neoplasia.” Accordingly, we updated the terminology in this paper. When the results of the primary pathologists showed relevant diagnostic differences between biopsy and polypectomy or focal carcinomas in hyperplastic polyps, these sections were blinded and reviewed by the reference pathologist (MS).
Before the endoscopic procedure, written informed consent for polypectomy and participation in the study was obtained. If the patient so requested, sedation with midazolam or pharyngeal anaesthesia with xylocaine, or both, were administered. The estimated size and location of the polyps were documented by the endoscopist. At least two forceps biopsy samples were taken from every polyp. Endoscopic snare polypectomy was performed with monopolar diathermy current. Submucosal injection of diluted adrenaline in saline was allowed facultatively to elevate sessile polyps. Complications arising during polypectomy or in the subsequent observation period were also documented. Bleeding was rated as a complication when the endoscopist believed that therapeutic intervention was required to halt it.
Diagnostic validity was assessed by classifying the polyps into three different subgroups: no epithelial polyp, tumour-like lesion, and neoplastic polyp. Owing to the very small number of specimens designated as “no polyp tissue”, adequate statistical comparison could not be made between these and the other subgroups. To determine sensitivity and predictive values of the histological results of biopsy and polypectomy specimens, these were compared with the ectomy result from the reference pathologist (MS) which was considered the gold standard. For the main results concerning diagnostic validity, confidence intervals are given. The dependency of the data from different polyps in the same patient was taken into account. For significance testing, only the first polyp from every patient was used. For determination of confidence intervals, all 222 polyps were used and included the correction of Rao and Scott20 for related standard errors. The size of the polyps within the different subgroups was compared by analysis of variance. To obtain equality of variances and normal data distribution, a logarithmic transformation of raw values was performed. Categorical data were compared using the χ2 test. For subgroup comparisons, Bonferroni's correction was applied. For comparison of complication rates, the sample was divided into two groups with non-experienced and experienced endoscopists. To achieve equality of variances for different complication rates, the arcsin transformation was applied. The level of significance was 0.05 (two sided) in all statistical tests. Statistical evaluation was performed with SPSSWIN.
The study protocol was approved by the ethics committee of the University of Erlangen-Nuremberg.
RESULTS
Of the 194 patients (114 women, 80 men; age 26–91 years (mean 70)), 24 had two polyps each and two patients had three (total 222 polyps). Mean polyp size was 10.5 mm (3–50), and tumour size did not differ among the subtypes of polyps (p>0.14). As noted, only polyps ≥5 mm were studied. The 3 mm polyps cited as the lower end of the range represent polypectomy specimens after reduction consequent to biopsy.
In 160 patients (82.5%), the polyp was found incidentally as there were no suggestive clinical symptoms. In 10 patients (5.2%) gastroscopy was performed for gastrointestinal bleeding; in 19 (9.8%) anaemia was present; and in five (2.6%) a delay in gastric emptying was suspected.
The polyps were most frequently located in the antrum (61.0%) and corpus (31.2%), and less frequently in the cardia (5.0%) and fundic region (2.8%). Of seven polyps in patients with a partially resected stomach, two were located in the anastomotic region. Location did not differ among the polyp subtypes (p>0.29).
In 135 polyps (60.8%) the epithelial surface was macroscopically intact, 77 (34.7%) showed erosions, and 10 (4.5%) appeared bloody. Surface appearance was significantly different between tumour-like lesions and neoplastic polyps (p<0.01) with the latter more often showing an intact epithelium.
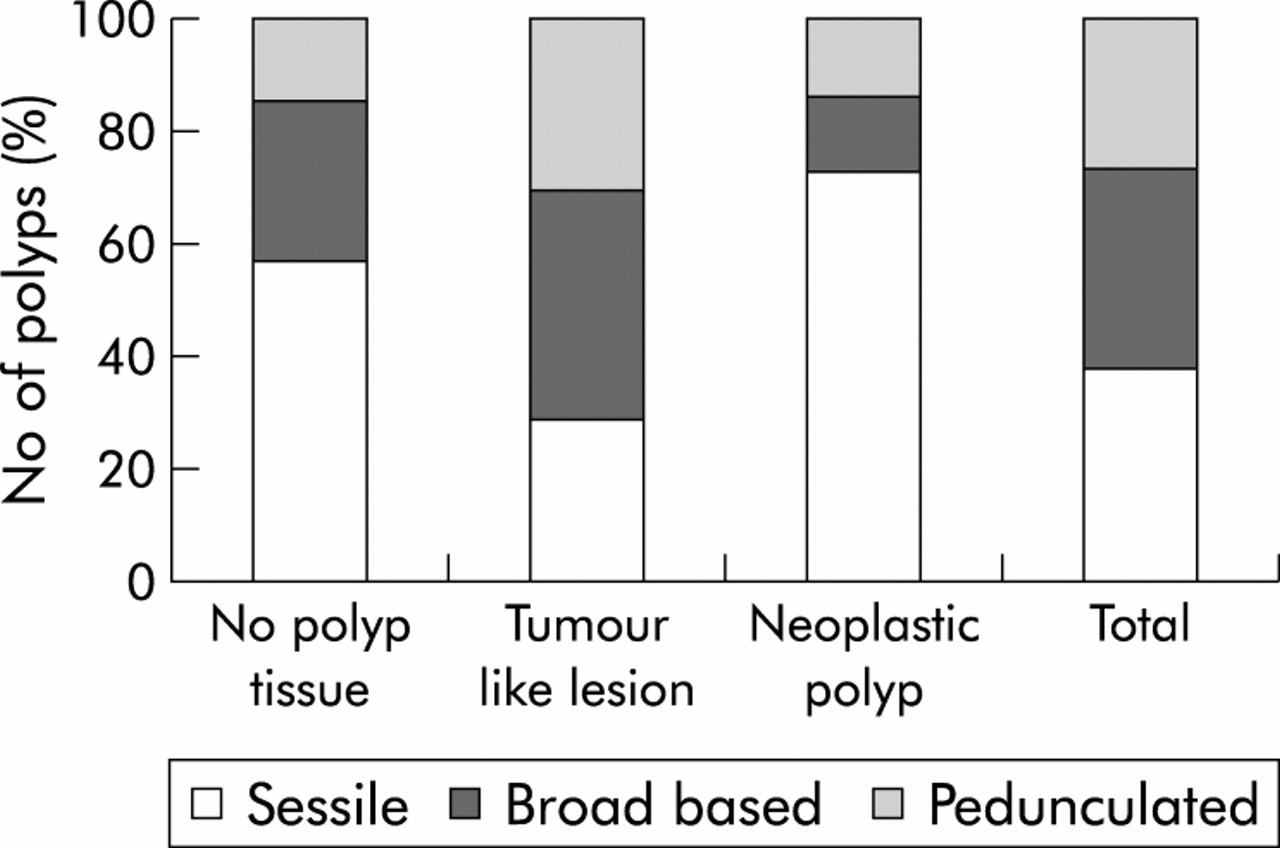
The growth pattern was sessile in 85 (38.3%) of the polyps, broad based in 78 (35.1%), and pedunculated in 59 (26.6%). Neoplastic polyps were significantly more frequently sessile (p<0.01 after Bonferroni's correction); no difference was found between the other two shapes (p>0.5 without Bonferroni's correction) (fig 1).

Polyp growth pattern (sessile, broad based, or pedunculated) according to histological subgroup.
The histological results of the polypectomy specimens after re-evaluation of discrepant results by the reference pathologist were as follows: 171 polyps (77.0%) were tumour-like lesions, 44 (19.8%) were neoplastic, and seven (3.2%) showed no polyp tissue (table 1).
Polypectomy specimens: histological results
In 56 polyps, focal foveolar hyperplasia was diagnosed by the primary pathologist on examination of the biopsy specimens only. This result was confirmed in only 18 cases (32.1%) after inspection of the polypectomy specimens. Of the remaining polyps, 31 (55.4%) were hyperplastic, five were inflammatory fibroid polyps, one was a tubular adenoma, and one was a Peutz-Jeghers polyp.
When the histological results of all biopsy and polypectomy specimens of the primary pathologist only were compared, complete agreement was seen in 124 polyps (55.8%). In an additional 77 polyps (34.7%), the clinically crucial distinction between tumour-like lesion and neoplastic polyp was made. However, in 21 cases (9.5%) there were important discrepancies: five polyps (2.3%) classified as neoplastic on biopsy were non-neoplastic or benign on polypectomy; seven (3.2%) polyps non-neoplastic or benign on biopsy were neoplastic or malignant on polypectomy; three (1.4%) hyperplastic polyps on biopsy were diagnosed as hamartoma; and six (2.7%) other hyperplastic polyps were found to have additional carcinoma or carcinoid tumour portions. These 21 preparations were sent to the reference pathologist who concurred with the primary pathologist's findings in 12 cases (57.1%). In nine cases (42.9%) however relevant disagreement occurred. Five specimens had been overestimated by the primary pathologist (that is, a tumour-like lesion had been diagnosed as neoplastic) and four specimens had been underestimated (see table 2).
Biopsy and polypectomy specimens: histological results of the primary and reference pathologists
At the re-evaluation of these 21 cases by the reference pathologist, the clinically relevant differentiation between tumour-like lesion and neoplastic polyp was possible in 15 cases by inspection of the biopsy sections alone whereas in the remaining six cases comparison with the polypectomy sections uncovered relevant differences (table 3). Of these, biopsy failed to reveal foci of carcinoma in three hyperplastic polyps. In two specimens it is suspected that no polyp tissue was removed during biopsy in one and polypectomy in the other. In a further polyp, biopsy did not contain the relevant carcinoid tumour portion.
Biopsy and polypectomy specimens: clinically relevant differences on histological examination by the reference pathologist
In table 4, sensitivities and predictive values and their respective confidence intervals are given for the histological biopsy and polypectomy results of the primary pathologist as well as for the biopsy results of the reference pathologist. Values for tumour-like lesions and neoplastic polyps are tabulated separately. For both examiners, the validity of the histological biopsy results was lower than that of the polypectomy results of the primary pathologist.
Biopsy and polypectomy specimens: sensitivity, predictive value, and confidence limits*
No lethal complications of polypectomy arose. Bleeding occurred in 16 patients (7.2%). It ceased spontaneously in three but required therapeutic intervention in 13 (injection in six, additional coagulation in one, additional clipping in three, clipping solely in two, laparotomy in one). Two of the patients required transfusion. In one patient an inflammatory reaction of the peritoneum owing to a closed perforation without free gas on x ray or signs of generalised peritonitis was suspected. The patient was managed conservatively.
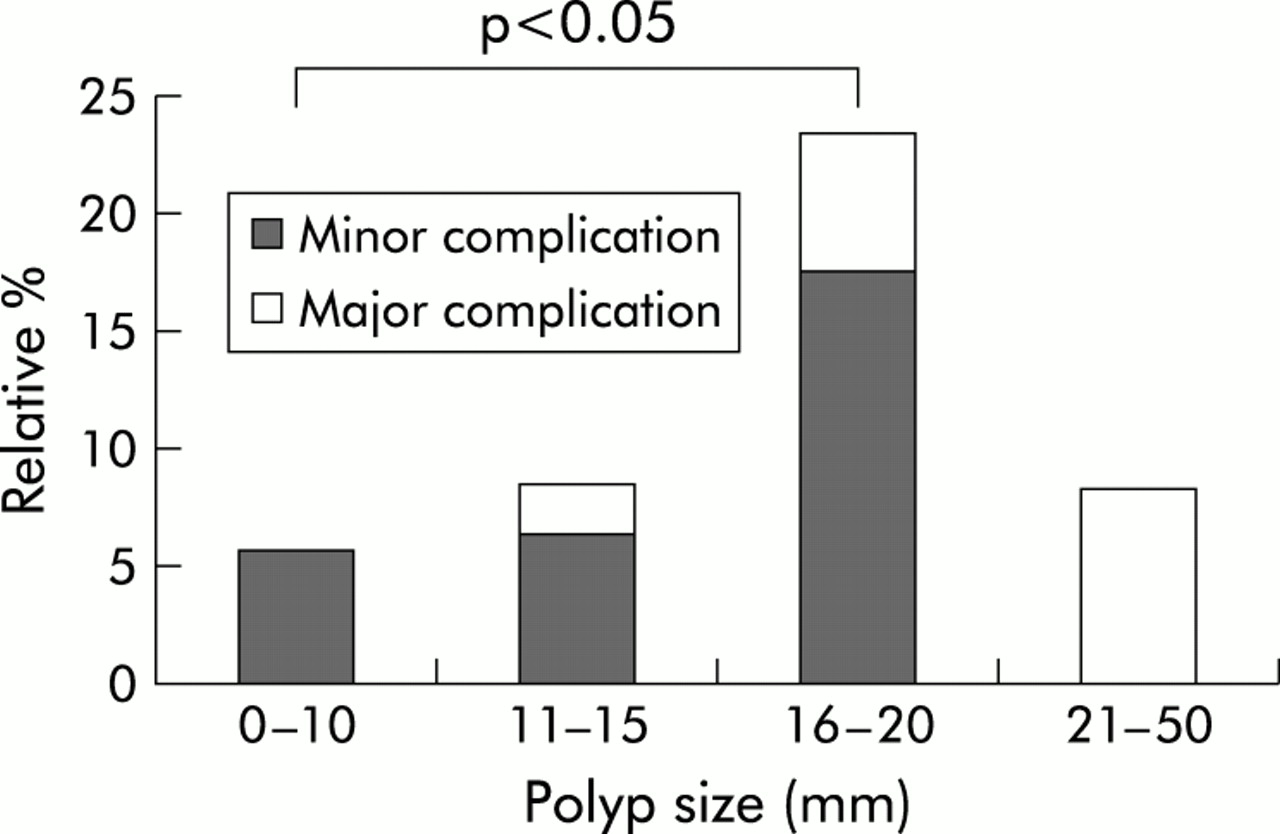
Although the complication rate was not consistently proportionate to increasing tumour size (p>0.4), it was significantly higher in mid size (16–20 mm) than in small (<10 mm) tumours (p<0.05 after Bonferroni's correction with factor 6 according to the six possible paired comparisons). There was also a tendency for major complications to occur in larger polyps although this impression was not statistically significant owing to the small number of polyps in this group (fig 2).

{kind=link}
{kind=link}
Complication frequency of polypectomy according to polyp size.
The complication rate for endoscopists with less experience with polypectomy (<7 polyps) was higher than for more experienced endoscopists (11.4% v 6.8%) although this difference was not statistically significant.
DISCUSSION
With the introduction of endoscopic polypectomy in the stomach in the early 1970s, an alternative to surgical ablation became available.21 As forceps biopsies had been considered unreliable, the procedure enjoyed widespread use.1,22,23 However, complications soon led to reconsideration of clearing the stomach of all polyps and to the use of forceps biopsy for decision making.
To evaluate whether forceps biopsy is representative of the entire polyp, only three series, smaller than the present, have as yet been reported.1–3 With a faulty differentiation between tumour-like lesions and neoplastic polyps rated as a clinically relevant difference, the discrepancy rate between biopsy and polypectomy results ranged from 0 to 29%.
In our prospective multicentre study the clinically relevant discrimination between tumour-like lesions and neoplastic polyps with forceps biopsy after the initial examination by the primary pathologist was possible in 201 of 222 polyps (90.5%). After review of the specimens by the reference pathologist, only six cases (2.7%) with relevant differences from polypectomy results remained. The most important reason for the differing appraisal by the reference pathologist between these specimens was the presence of foci of carcinoma in hyperplastic polyps that were not gathered by forceps biopsy. In nine cases (4.1%) the reference pathologist found clinically relevant biopsy or polypectomy results that were different from those of the primary pathologist.
On the one hand these results show that with a meticulous examination of the forceps biopsy samples by an experienced pathologist, a correct histological diagnosis can be obtained without a complete polypectomy in nearly all cases (97.3%). On the other hand, foci of carcinoma are present in a small percentage of hyperplastic polyps and may be missed with biopsy sampling. In our survey we found four such polyps (3.1%) in a total of 131 hyperplastic polyps, ranging from 10 to 50 mm (median 15 mm). In only one of these was the malignant focus detected by forceps biopsy. Since the first description in 1978 by Remmele and Kolb of a hyperplastic polyp containing a carcinoma,24 several case reports have been published. Although at first it was thought that only hyperplastic polyps larger than 20 mm could contain malignant foci,7,25–27 this finding has more recently been observed in polyps of 5 mm.4,8,10,11,28 The reported frequency differs considerably. One reason may be that in the older literature adenomas were misinterpreted as hyperplastic polyps containing intraepithelial neoplasia. On the other hand, regenerative alterations, which always occur in the erosive area in hyperplastic polyps, were in part overestimated as intraepithelial neoplasia. Stolte demonstrated malignant foci in only 0.3% of 2036 hyperplastic polyps.6 In contrast, a meta-analysis of three other studies found malignant foci in 2.2% of 1072 polyps8,10,11 which compares well with our result of four carcinomas (3.1%) in a total of 131 hyperplastic polyps.
Focal foveolar hyperplasia is considered a potential precursor of hyperplastic polyps by the WHO. However, Stolte et al showed that focal foveolar hyperplasia and hyperplastic polyps can readily be differentiated on the basis of architectural and cytological criteria, even in forceps biopsy material.29 This estimation cannot be supported by the results of our study as more than 55% of the biopsy specimens initially judged to be focal foveolar hyperplasia were diagnosed as hyperplastic polyps after evaluation of the corresponding polypectomy specimens. In two cases, clinically crucial differentiations (a neoplastic polyp in one and a Peutz-Jeghers polyp in another) were not possible by the primary pathologist.
A recommendation based on these data to remove all polyps classified as focal foveolar or hyperplastic on biopsy completely with the snare must be weighed against the possible risks of polypectomy. In our study, bleeding occurred in 16 patients (7.2%). With the exception of one case, managed by laparotomy, all others ceased spontaneously or could be controlled endoscopically. Transfusion was necessary in only two patients. This underscores the importance of proficiency in endoscopic haemostatic techniques by the endoscopic team as a prerequisite for performing polypectomy in the stomach. Additionally, in one patient a closed perforation was suspected. In summary, in a total of three patients (1.4%) major but not lethal complications occurred. As expected, we observed an increase in the frequency of complications with increasing polyp size. However, the largest polyps (21–50 mm) were associated with a lower complication rate than the mid sized polyps although the number in the former subgroup was small (12 polyps—5.4%). In view of the risk-benefit profile (2.3% undetected foci of carcinoma in hyperplastic polyps on biopsy; 1.4% major complications of polypectomy), complete endoscopic removal of even smaller polyps rated as hyperplastic on biopsy must be considered. Regarding focal foveolar hyperplasia, this recommendation should be adapted to the endoscopic appearance of the polyp. For polyps with characteristic macroscopic features (size <5 mm, multiple occurrence, location in the antrum6), no further action seems to be justified. For all other polyps rated as focal foveolar hyperplasia on biopsy, endoscopic polypectomy should be considered also as in the clinical setting no unequivocal differentiation from other histological polyp types based on forceps biopsy specimens seems to be possible at present. Of course, the patient's general condition (especially age and concomitant illnesses that might be exacerbated by possible complications) should also be a factor.
There is no controversy regarding indications for removal of adenomatous polyps as the adenoma-carcinoma sequence holds true in gastric as well as colorectal polyps.6,30 In our series, the concomitant presence of adenomatous and carcinomatous portions in a single polyp was observed in two specimens. Here—in contrast with carcinomatous foci in hyperplastic polyps—underestimation on biopsy is not clinically relevant as all adenomas must be removed completely. Owing to the characteristically sessile growth pattern of adenomas and carcinomas, submucosal injection is recommended to facilitate complete endoscopic removal. In many cases, an endoscopic classification can be attempted as most adenomas reveal an intact mucosal surface whereas hyperplastic polyps and carcinomas frequently show erosions and bleeding.31 As the sensitivity and specificity of endoscopic diagnosis are unknown, histological examination remains mandatory.
In all other polyp types (22 (9.9%) in our study), polypectomy would only be necessary when the polyps are symptomatic or produce complications (bleeding, obstruction). As the remaining number of poly types is limited, a general recommendation to remove all epithelial gastric polyps larger than 5 mm primarily without prior histological clarification by forceps biopsy may be justified.
In conclusion, the results of our study show that in a clinical setting focal foveolar hyperplasia larger than 5 mm cannot be unequivocally differentiated from other histological polyp types based on forceps biopsy specimens alone and hyperplastic gastric polyps can contain neoplastic foci that might not be diagnosed by forceps biopsy alone. Even if the bleeding rate after snare polypectomy appears to be higher in the stomach than in the colon, the majority of cases can be managed endoscopically. Therefore, we recommend removal by an experienced endoscopist of all epithelial gastric polyps larger than 5 mm after thorough individualised risk-benefit analysis.
APPENDIX
The participants in the study group are shown in Table A1.
Participants in the study group