Article Text

Abstract
Background: Duodenal cancer is one of the leading causes of death in familial adenomatous polyposis (FAP) patients. An endoscopic surveillance programme was therefore initiated in 1988, the outcome of which is described in this paper.
Methods: We report the 10 year follow up of 114 patients with FAP who were prospectively screened for the presence and severity of duodenal adenomas.
Results: Six of 114 patients (median age 67 years) developed duodenal adenocarcinoma. Four of these were from 11 patients who originally had Spigelman stage IV disease (advanced duodenal polyposis), which gives a 36% risk within this group of developing cancer. One case of duodenal cancer arose from 41 patients who originally had stage III disease (2%) and one cancer arose from 44 patients with original stage II disease (2%). All six patients have died: five were inoperable and one had recurrence three years after a pancreaticoduodenectomy. There was no association between duodenal cancer and site of germline mutation of the APC gene.
Conclusions: Surveillance for duodenal adenocarcinoma and subsequent early referral for curative surgery has not been effective. Selection of patients with advanced but benign (Spigelman stage IV) duodenal polyposis for prophylactic pancreaticoduodenectomy should therefore be considered and can now be justified on the basis of these results. More comprehensive endoscopic surveillance of high risk (stage III and IV) patients is needed in an attempt to avoid underestimating the severity of duodenal polyposis, and to evaluate the role of endoscopic therapy in preventing advanced disease.
- familial adenomatous polyposis
- duodenal cancer
- FAP, familial adenomatous polyposis
- FGP, fundic gland polyps
Statistics from Altmetric.com
Familial adenomatous polyposis (FAP) was previously known as familial polyposis coli, the change in name reflecting the recognition of extracolonic polyps and cancers. Prophylactic colectomy has decreased the incidence of colorectal cancer in FAP, and duodenal cancer and desmoid disease are now the leading causes of death.1 Management of the duodenal risk is complicated by the fact that despite over 95% of patients having identifiable adenomatous polyps in the duodenum, only 5% go on to develop cancer.2 Screening with upper gastrointestinal endoscopy is now commonplace but has not been shown to decrease the cancer rate,3,4 and clinicians are often confused as to what to do about the findings. One hundred and two FAP patients were prospectively screened using a defined protocol in 1988–9 and we report the 10 year follow up of these patients together with a further 12 patients screened shortly after submission of the original paper.5
PATIENTS AND METHODS
In the calendar year 1988, 114 consecutive patients with FAP (63 males, 51 females, median age 42 years (range 14–76)) underwent upper gastrointestinal endoscopy to a set protocol at a single centre using a side viewing duodenoscope: the position and size of gastric and duodenal polyps were documented using maps of the upper gastrointestinal tract with one map showing both the stomach and duodenum and one showing a detailed layout of the ampullary region (matching the view from a side viewing duodenoscope) with views to the third part of the duodenum. The number of polyps equalled the number of distinct areas (often flat lesions) of duodenal mucosal within the duodenum.
The sizes of the polyps were measured by comparison with open biopsy forceps. Two biopsies were taken from the largest duodenal polyp(s), two were taken from the papilla, and two were taken from the peripapillary region, even if the papilla and peripapilla appeared normal. Two antral biopsies and two biopsies of the fundus were taken in the initial period but this was not continued as part of the surveillance programme as there was no evidence of associated excess risk from gastric polyps.
Since 1992, the papilla itself has not been routinely biopsied because of a case of iatrogenic pancreatitis 24 hours after papillary biopsy. In the original study, both peripapillary biopsies and papillary biopsies were taken, but after this an immediately peripapillary biopsy was used to assess adenomatous change at the ampulla.
Patients were graded and a staging system described (Spigelman system, see table 1): 11, 41, 44, 15, and three patients were classified as stage IV to 0, respectively. The published data5 from this cohort led to the worldwide adoption of the Spigelman system. Patients were re-endoscoped at three yearly intervals unless they had advanced (stage IV) disease in which case the interval was reduced. Surgical intervention was recommended in the event of development of cancer or consistently severe dysplasia.
Classification of the severity of duodenal polyposis (according to Spigelman et al)
The same cohort was followed throughout and we report the findings in 1998–9, 10 years later. Full endoscopic follow up, or follow up until death, was available for 99 patients over 10 years. Three patients were lost to follow up, six did not have endoscopic follow up, and in six patients the defined protocol was not followed (no biopsies were taken). There were seven different endoscopists and three histopathologists.
RESULTS
Six of 114 patients developed duodenal cancer at a median of six years (range 2–10) after entering the study (table 2). Median age at diagnosis was 68 years (60, 66, 67, 69, 70, and 71). Three of the duodenal cancers were ampullary cancers and three occurred in the second/third part of the duodenum (extra-ampullary). Two of the three patients with eventual ampullary cancer had, at initial endoscopy, adenomatous enlargement of the ampulla, and one had a normal ampulla. Similarly, two of the three patients with extra-ampullary duodenal cancers had an enlarged ampulla with mild dysplasia at the initial endoscopy and one had a normal ampulla.
Progression from duodenal adenoma to carcinoma in six patients
Patient No 1 had a persistent 25–30 mm flat lesion in the third part of the duodenum in which the histological findings were of mild to moderate dysplasia. Management was conservative and the patient developed cancer during the period of surveillance.
Patient No 2 progressed to cancer from initially mild (stage II) duodenal polyposis which consisted of 15–20 small (<2 mm) flat mildly dysplastic tubular adenomas only. He defaulted from surveillance examinations and within this extended period of five years developed ampullary cancer. His ampulla and periampullary area had previously been macroscopically and histologically normal. Pancreaticoduodenectomy was carried out for his ampullary cancer but he had disease recurrence three years later and died with distant metastases.
Patient No 3 underwent surgical transduodenal resection of a polyp in the second part of the duodenum that had been seen on the previous endoscopies. The polyp was found to contain adenocarcinoma and the resection margin was thought to be clear, but six months later recurrence occurred at the same site and further surgery was impossible.
Patient No 4 had previously undergone transduodenal resection of a tubulovillous adenoma in the second part of the duodenum but tubulovillous adenoma recurred in a carpet-like distribution around the ampulla. Documentation of the same lesion was made 18 months later but the biopsies suggested only mildly dysplastic adenoma. The patient then presented with malignant ascites and at the post mortem duodenal cancer was confirmed at the ampulla.
Patient No 5 underwent transduodenal resection of a moderately dysplastic duodenal polyp 15 years before with subsequent snare excisions of moderate and severely dysplastic polyps 12 years before. There was later development of a single flat 20–30 mm lesion in the second part of the duodenum in which the histological findings varied and it eventually became an adenocarcinoma with both local and distant metastases at diagnosis.
Patient No 6 was noted initially to have a 25 mm sessile polyp at the ampulla which was a villous adenoma with moderate dysplasia. Subsequent endoscopies did not reveal progression of this lesion, and biopsy of the lesion failed to reproduce the findings of villous adenoma. He later developed a cancer in the periampullary region and a pancreaticoduodenectomy was planned, but he died of pulmonary embolism prior to the procedure and no post mortem was carried out.
Four of the duodenal cancers were from 11 patients who had Spigelman stage IV disease 10 years previously and this gives a crude risk of 36% within this group (table 3). There were seven other original stage IV patients. The first developed probable gastric cancer originating in the fundus (indurated gastric polyp with ascites and liver metastases of adenocarcinoma). The second developed synchronous primary adenocarcinomas of the common bile duct, the junction of the right and left hepatic ducts, the head of the pancreas, and the gall bladder, and died as a result of this (previously reported by Spigelman and colleagues6). The third patient is well after an uncomplicated pancreaticoduodenectomy performed because of a severely dysplastic ampullary polyp. The fourth patient had persistent stage IV disease until 1996 but has not been examined more recently after development of metastatic ovarian carcinoma. The final three patients continue on the surveillance programme: this includes one patient in which the histological findings have varied from moderately dysplastic villous adenoma to mildly dysplastic tubular adenoma leading to confusion in the staging, and two patients who had moderately dysplastic adenoma on initial endoscopy which was not reproduced at later endoscopies.
Progression of duodenal disease according to original Spigelman (Sp) stage
One of 41 original stage III patients developed duodenal cancer, one gastric adenocarcinoma of the antrum, and one adenocarcinoma of the head of the pancreas. Four patients progressed to stage IV and one of these is awaiting pancreaticoduodenectomy. None of the other original stage III patients progressed, and this slow rate of progression can be seen to have also occurred in stage 0, I, and II patients (table 3). Five stage III patients progressed to stage IV and these were not older (median age 39 years (range 28–67)) than those who did not progress (median age 41 (confidence interval (CI) 30–52)). A similar pattern was seen for stage II patients: median age of the seven patients progressing to stage III was 39 years (25–62) and those not progressing, 39 years (CI 27–49).
Endoscopic therapy was attempted in just two patients. One of these was an original stage III patient with a 30 mm mildly dysplastic tubular adenoma in the third part of the duodenum removed by snare polypectomy without complications. Initially, 80–90% of the polyp was removed but at the six month follow up, a 1.5 cm tubular adenoma with mild dysplasia was seen at the same site. The polyp contained foci of moderate dysplasia. A further patient had snare polypectomy of a 25 mm mildly dysplastic tubulovillous adenoma at the junction of the first and second parts of the duodenum. He was admitted to his local hospital 24 hours later with malaena and needed endoscopic therapy to achieve haemostasis at the resection site. We thought that we totally removed the polyp but six months later a 6 mm lesion was seen at the same site, which grew to 12 mm the following year.
The prevalence of fundic gland polyps (FGP) was 63 of 114 (55%) patients. There were 55 patients with Spigelman stage III and IV duodenal polyposis and 59 patients with Spigelman stage 0, I, and II duodenal polyposis, and the prevalence of FGP in these two groups (38/55 (50%) and 35/59 (59%), respectively) was not significantly different (p>0.2). Two of the six patients progressing to duodenal cancer had FGP and four had no FGP. The patient with probable gastric fundal cancer had FGP and the patient with confirmed gastric antral cancer had no FGP.
Nineteen of the remaining 104 patients without upper gastrointestinal cancer were not available for the 10 year follow up: three died of rectal cancer (two with stage III duodenal disease and one with stage I), two died from complications of desmoid disease, two from myocardial infarction, and one from non-Hodgkin's lymphoma. Two patients refused further upper gastrointestinal endoscopy, six did not have further surveillance, and three did not have biopsies taken.
There was a lifetime history of rectal cancer in 1/11 (9.1%) stage IV patients, 8/41 (19.5%) stage III, 3/44 (6.8%) stage II, and 1/18 (5.6%) stage I/0 patients.
The average number of biopsies at the original endoscopy in 1988–89 was 5 (range 2–10) and at the second endoscopy this had decreased to 3 (range 1–7). We have now undertaken a similar analysis of the number of biopsies taken and have found that the trend towards lower numbers of biopsies persisted throughout the latter years, with the median number in 1998–99 also being 3 (range 2–8). We did not find a correlation between the number of biopsies taken and its relation to the degree of dysplasia and histological architecture (r=0.11, p>0.2). The median number of endoscopies for stage IV patients during the period 1988–99 was 7.5 (range 5–11) (although survival was less than 10 years), and the median number of endoscopies for the other 82 patients with a full 10 year endoscopic follow up was 4 (range 3–7). This is in accordance with local surveillance recommendations. The initial endoscopies were carried out by two endoscopists and there were a further five endoscopists over 10 years.
There were 24 patients who took part in four different chemoprevention trials (none of the stage IV patients). The trials consisted of a six month aspirin study (n=6), six month sulindac study (n=9), six month celecoxib study (n=7), and six month ranitidine study (n=6). Four patients took part in the ranitidine trial and then the celecoxib trial. The trials consisted of six month treatments with either placebo or active drug. There was no difference in progression between patients taking active medication (2/15, 13% worsened) or placebo (2/9, 22% worsened; p=0.6).
Complications of surveillance included one patient who was admitted within 24 hours of biopsy of the papilla (previously reported7) and one patient who had a period of apnoea after sedation with pethidine 50 mg and midazolam 2.5 mg. There were no other complications from sedation. The median amount of sedation given was midazolam 2.5 mg and pethidine 50 mg. Two patients have refused to have further upper gastrointestinal endoscopy under sedation only because they found the procedure too unpleasant.
Germline mutation was tested for in 90/114 patients. The remaining patients were either lost to follow up (n=3), died before the advent of genetic testing with no relatives available to test (n=12), were not approached for testing (n=2), or are awaiting results or testing (n=7). Nineteen of the 90 patients had negative results on testing and five had a mutation confirmed on exon 15 which could not be further characterised by the standard methods of protein truncation test and polymerase chain reaction-single strand conformational polymorphism analysis. Precise germline mutation data were therefore available for 66/90 (73%) patients from 26/44 (60% families). The most common mutations were five base pair deletions at codons 1061 (14 patients from eight families) and 1309 (10 patients from five families), both on exon 15. The only other mutation affecting more than one family was a single base pair substitution (C to T) on exon 6 at position 694 affecting two families.
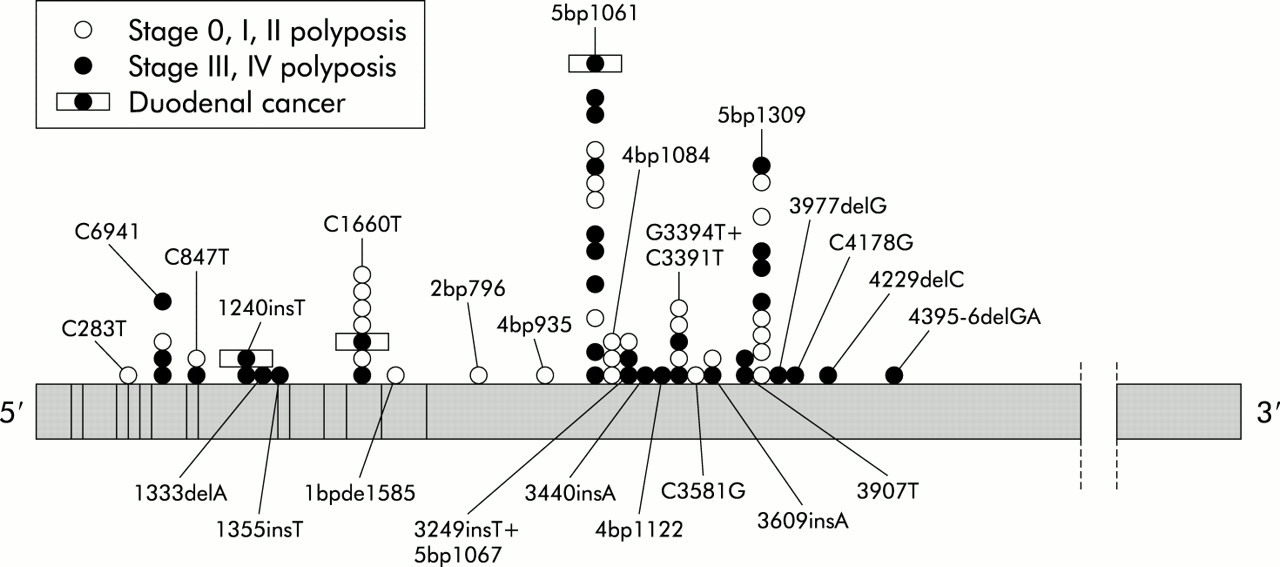
There were equal proportions of patients with more severe disease (stage III, IV, and duodenal cancer) in exons 1–14 (10/19=53%) and exon 15 (27/50=54%; p>0.2). There were also equal proportions of Spigelman stages III and IV and duodenal cancer patients with a negative gene test (7/18=39%) compared with a positive gene test (37/69=54%; p>0.2). It can be seen in fig 1 that there was exclusively stage III or IV duodenal polyposis in two families at codon 1061, one family at 1309, and one family with the C1660T insertion, and exclusively mild disease in one family with a four base pair deletion at codon 1084. Conversely, there was heterogeneity of disease severity in families with mutations at C694T, C847T, 3249insT, and G3394T. With regard to the relationship of germline mutation to FGP, there were equal proportions of patients with FGP in exons 1–14 (10/17=58.8%) and exon 15 (24/47=51.1%; p>0.2). There was also no more chance of a positive gene test in patients with FGP (34/39 tested=87%) than in those without FGP (30/42 tested=71%; p>0.2).
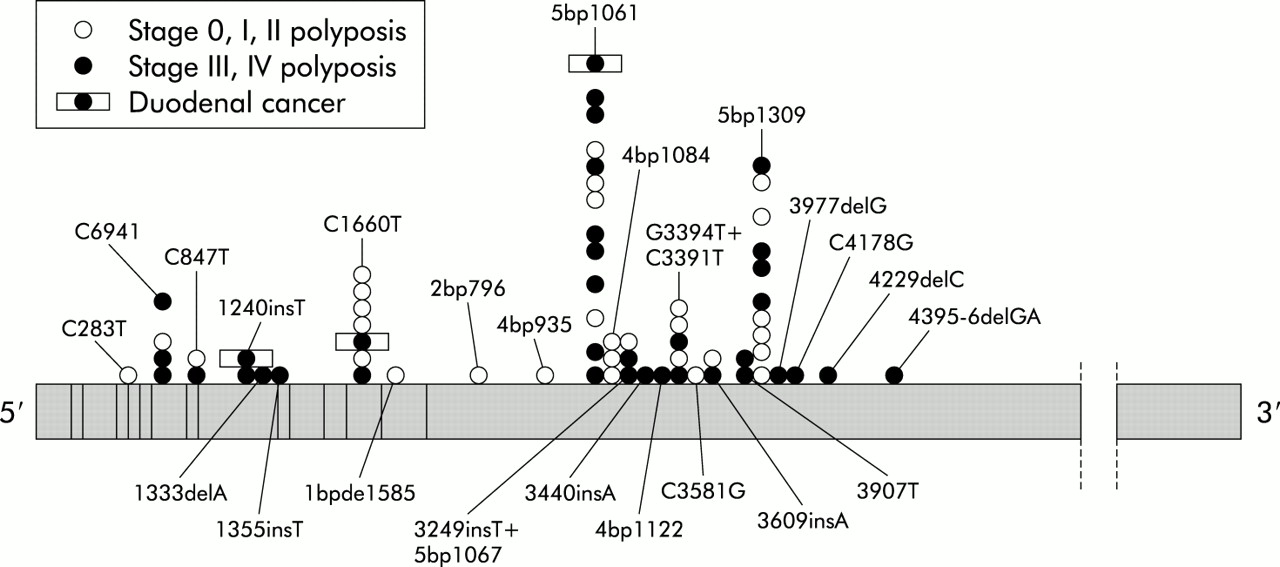
Position of germline mutation on the APC gene for patients with stage 0, I, or II duodenal polyposis versus stage III or IV polyposis or duodenal cancer. Where there was more than one family per mutation, individuals were grouped into families, seen at C694T and at codons 1061 and 1309.
DISCUSSION
Although the benefit of surveillance has been questioned,3 and has not improved the outcome in this cohort, the staging system outlined by Spigelman and colleagues5 has facilitated both a better understanding of the natural history of duodenal polyposis and development of a method for stratification of duodenal cancer risk. In this long term cohort study it is clear that those with stage IV disease have by far the greatest risk of duodenal cancer. This trend was becoming apparent when the cohort was reported on in 19948 when one stage IV patient had confirmed duodenal cancer and two other stage IV patients were suspected of having this cancer. It was argued at that time that although three yearly endoscopy was safe for the majority of patients, those with stage IV disease need more regular surveillance. We have now shown that indeed these patients have a crude duodenal cancer risk as high as 36%, and given that none has been cured of their cancer this means that our policy of intermittent surveillance and referral of early cancer was not enough. We believe that all patients with Spigelman stage IV duodenal polyposis should have the opportunity to discuss duodenal resection with an appropriately skilled upper gastrointestinal surgeon. In FAP patients who have undergone duodenal resection for advanced benign duodenal polyposis, the mortality rate has been low: there has been one death among 42 patients (2.3%) reported from five centres.9–12 The operation of choice for premalignant duodenal polyposis is a pancreas (and pylorus) preserving duodenectomy which leads to good functional outcome and facilitates endoscopic follow up. We have previously shown, together with the group from the Hôpital St Antoine in Paris, that it is superior in the management of duodenal disease to duodenotomy and clearance, which was found to be universally followed by early advanced recurrence.13,14
In examining the results from the surveillance programme, it can be seen (table 2) that the managing clinicians were presented with quite variable histopathology results from the same patients on subsequent examinations. We have been worried that at times the endoscopist's assessment of the visible seriousness of the duodenal disease has not been followed through because biopsies have shown only mild dysplasia. This may be associated with the decrease in the number of biopsies taken over time, and perhaps sampling error in the biopsies occasioned by haste associated with patient distress. Clinicians who manage polyposis patients should be alert to the findings here that at times the biopsies serve to understage the disease. The opinion then, based on endoscopic appearance, of a clinician experienced in the spectrum of duodenal polyposis should not be disregarded lightly by the arrival of a more favourable histological report. This problem might be overcome if effective deep sedation/general anaesthesia were to be adopted for selected patients with known advanced polyposis which would allow better targeting of biopsies or allow polypectomy, both of which may provide more reliable histological specimens. As well as making surveillance kinder for the patients it would allow an opportunity, as yet prospectively untested, for assessment of endoscopic therapeutic intervention.
Snare polypectomy in the FAP duodenum can be difficult because of the flat morphology of most duodenal polyps. New techniques however utilising prior submucosal saline/adrenaline injection, and endoscopic mucosal resection with endoscopic clipping to close any defect, may greatly reduce the risks of haemorrhage and perforation.15,16 Submucosal saline injection techniques have already been used safely and successfully in the duodenum in non-FAP patients with smaller adenomas (median size 10.5 mm).17 Regardless of the technique, removal of ampullary polyps can be perilous, as demonstrated by the report of a death from severe pancreatitis of a patient undergoing endoscopic ampullary polypectomy.18 Thermal ablation techniques using electrocautery for duodenal polyposis in FAP has also been used. At one centre, and after prophylactic sphincterotomy, 17 of 19 patients had disease clearance or improvement using the Nd:YAG laser,19 although we do not know whether these polyps were large or histologically advanced. Complications included one perforation. Photodynamic therapy using 5 amino-laevulinic acid or photofrin as the sensitiser has also been used in six patients20: 5 amino-laevulinic acid caused only superficial tumour destruction whereas photofrin caused good adenoma reduction but with unacceptable photosensitivity. The argon plasma coagulator has been used in some centres although there are as yet no published data.
The recent finding in a randomised controlled trial21 that the cyclooxygenase 2 inhibitor celecoxib significantly improves the endoscopic duodenal stage gives an alternative therapeutic option for those with mild to moderate duodenal polyposis. Further chemoprevention trials are planned with new agents and the effect on duodenal polyposis is particularly important given its status as the major cause of mortality in FAP. Stage III patients with larger polyps, and stage IV patients in whom open surgery is inappropriate, may be considered for endoscopic polypectomy as an additional measure if the position and morphology of a polyp is suitable, with prospective evaluation of this treatment. Patients with particular problems are the stage IV patients in whom surgery is inappropriate because of desmoid disease or their medical condition, and in whom endoscopic intervention is impossible because of carpeting of the duodenum by adenoma or extensive involvement of the ampulla.
Previous work has found a correlation between mutations in codons 1250–1464 and rectal cancer22 and between mutations in codons 1250–1500 and risk of secondary proctectomy.23 In one recent report, the common 5 base pair deletion at codon 1309 was found to lead to the onset of rectal cancer 10 years earlier than either mutations outside this region or unknown mutations24; this follows previous reports of patients with a 1309 mutation having significantly more colonic polyps at the time of colectomy.25 These studies did not report an association between germline mutation and severity of duodenal polyposis although this issue was not addressed either in these or other studies, possibly because of the rarity of complete clinical data on duodenal polyposis. The recent publication from Bonn looked for and failed to show an association between germline mutation and the presence of duodenal polyps although the authors recognise that this may reflect the almost universal (95%5, 97%26) prevalence of duodenal adenomas in FAP. Dobbie reported severe extracolonic manifestations, including three patients with small intestinal polyps, in patients from their cohort with mutations beyond codon 1403, but curiously there were said to be no extracolonic manifestations in the 25 families with mutations 5′ to this despite the recognised high prevalence of duodenal polyps.27
Our data did not reveal a correlation between site of germline mutation and duodenal polyposis severity, or ability to detect germline mutation and duodenal polyposis severity. We also noted three patients with severe duodenal polyposis and no patients with mild disease 3′ of codon 1403, but the small number of patients with mutations in this region makes it difficult to draw any firm conclusions. There remains little evidence of a genotype-phenotype correlation for duodenal polyposis.
The situation with regard to duodenal disease management is now becoming clearer (fig 2). Those with stage IV disease should be offered surgery because of the high risk of progression to cancer, and surgery should be a pylorus preserving pancreaticoduodenectomy. Those who do not wish to have surgery, or those for whom it is inappropriate for other reasons, should have the opportunity to undergo alternative treatments as previously mentioned. At the opposite end of the disease spectrum however patients with stage 0 or I disease can be left safely for five years between surveillance examinations without therapeutic intervention, as none of these patients progressed beyond stage II over 10 years.

{kind=link}
{kind=link}
Algorithm for the management of duodenal polyposis in familial adenomatous polyposis. CP, chemoprevention; ET, endoscopic therapy; GA, general anaesthetic; PPPD, pancreas (and pylorus) preserving pancreaticoduodenectomy.
This leaves stage II to III patients who present more of a challenge: only 2% developed cancer and our results (table 3) show that progression only occurred in 12 of 85 (14%) patients. Kaplan-Meier estimates from elsewhere26 suggest a progression of adenomatous disease with age with 30% predicted to reach stage IV by age 65 years, but this has not yet occurred in the majority of our cohort. In our stage II and III patients, only five (12.2%) and seven (15.9%) patients progressed in stage and age did not predict progression.
Therefore, we currently recommend a universal policy of three yearly endoscopy for all stage II patients, and two yearly endoscopy for all stage III patients with a low threshold for examination under general anaesthetic, which allows passage of both side viewing and forward viewing endoscopes giving a maximum view of the ampulla, stomach, duodenal bulb, and the third and fourth parts of the duodenum, and an opportunity for therapeutic manoeuvres. Stage II and III patients may also be entered into prospective evaluation of chemoprevention, with or without endoscopic therapy. The aim of treatment is an attempt to prevent progression to stage IV disease with the resulting one in three risk of duodenal cancer.
Acknowledgments
We thank Kay Neale and the staff of St Mark's Polyposis Registry, and the following present or past members of staff who contributed: Iain Beveridge, Marina Wallace, Henry Debinski, Karen Nugent, Christopher Williams, and Alistair Forbes.