Article Text

Abstract
We report a very rare case of primary low grade mucosa associated lymphoid tissue (MALT) lymphoma of the oesophagus. An 83 year old woman was referred to our hospital in June 1999 for further examination and treatment of oesophageal tumour. Although a physical examination and laboratory data showed no significant abnormalities, endoscopic observation revealed two slightly elevated submucosal tumour-like lesions of the oesophagus. Tissue specimens were obtained by endoscopic mucosal resection of the oesophagus using a cap fitted panendoscope. The lesions were composed of diffuse small atypical lymphoid cells—that is, centrocyte-like cells—which were stained with CD20, L26, BCL-2, and κ, but not with CD3, CD5, CD10, or cyclin D1. Monoclonality was detected by polymerase chain reaction analysis using the primer for CDR-3 of immunoglobulin H and diagnosed as low grade MALT lymphoma of the oesophagus. The tumours were considered to be completely resected and therefore additional treatment was not administered. The patient is alive and well 22 months after treatment and diagnosis.
- mucosa associated lymphoid tissue
- lymphoma
- oesophagus
- primary oesophageal lymphoma
- endoscopic mucosal resection
- monoclonality
- MALT, mucosa associated lymphoid tissue
- PCR, polymerase chain reaction
- Ig, immunoglobulin
Statistics from Altmetric.com
- mucosa associated lymphoid tissue
- lymphoma
- oesophagus
- primary oesophageal lymphoma
- endoscopic mucosal resection
- monoclonality
The incidence of primary malignant lymphomas of the oesophagus is relatively rare compared with that of lymphomas occurring in other gastrointestinal organs, such as the stomach, small intestine, and colon.1 To our knowledge, there has only been one report describing a case of mucosa associated lymphoid tissue (MALT) lymphoma of the oesophagus.2 We report here a very rare case of primary low grade MALT lymphoma of the oesophagus.
CASE REPORT
An 83 year old woman was referred to Shinshu University Hospital in June 1999 for further examination and treatment of oesophageal neoplasm. Her practitioner first performed an upper gastrointestinal endoscopy because of her complaints of slight heartburn but aside from heartburn she presented no serious symptoms requiring prolonged hospitalisation. Immunophenotypic studies of the biopsy specimens of the oesophagus using monoclonal antibodies strongly suggested low grade MALT lymphoma of the oesophagus. She did not complain of fever, weight loss, or night sweating. On admission, physical examination revealed no marked features; the liver, spleen, and superficial lymph nodes were not palpable. The patient's main laboratory data showed no abnormalities. No hepatitis B surface antigen, hepatitis C virus antibody, Epstein-Barr virus capsid antigen, or human T cell leukaemia virus 3 antibody were detected. No elevation of tumour markers or autoimmune antibodies were observed. The level of anti-Helicobacter pylori antibody was not elevated. Although a physical examination and laboratory data showed no special abnormalities, endoscopic observation revealed two elevated submucosal tumour-like lesions at approximately 20 cm from the incisor teeth of the oesophagus (fig 1⇓). None of the tumorous elevations measuring 1 cm longitudinally was ulcerated but each was partially covered with grayish-white granular lesions. No lymphomatous involvement of the stomach or Barrett's changes at the oesophageal-gastric junction was found.

Endoscopic observation of the oesophagus shows two slightly elevated submucosal tumour-like lesions with grayish-white granular lesions (arrows).
To confirm a diagnosis of the lesions, tissue specimens were obtained by endoscopic mucosal resection of the oesophagus using a cap fitted panendoscope (GIF-Q240; Olympus, Tokyo, Japan).3 Specimens were fixed in 10% formalin, embedded in paraffin, and routinely stained with haematoxylin and eosin, and served as histopathological observation and as tissues for microdissection. The lesions of the oesophagus were composed of diffuse, small, atypical lymphoid cells—that is, centrocyte-like cells—which had invaded the epithelial mucosa (fig 3⇓). An immunohistochemical study was performed on paraffin embedded specimens using the streptavidin-biotin peroxidase complex method with the Vectatain Elite ABC kit (Vector Laboratories, Burlingame, California, USA). The atypical cells were diffusely positive for CD20, L26, BCL-2, and κ, but negative for CD3, CD5, CD10, and cyclin D1. Neoplastic B cells occupying the marginal zone are shown in fig 4⇓. Ultrasonography and computed tomography showed no hepatosplenomegaly or swelling of the para-aortic lymph nodes, and the removed tissues had clear resection margins, as shown in fig 2⇓.

Low magnification of the mucosa associated lymphoid tissue lymphoma of the oesophagus obtained by endoscopic mucosal resection (haematoxylin and eosin stain). Lymphoma cells are not seen on the resected margin.
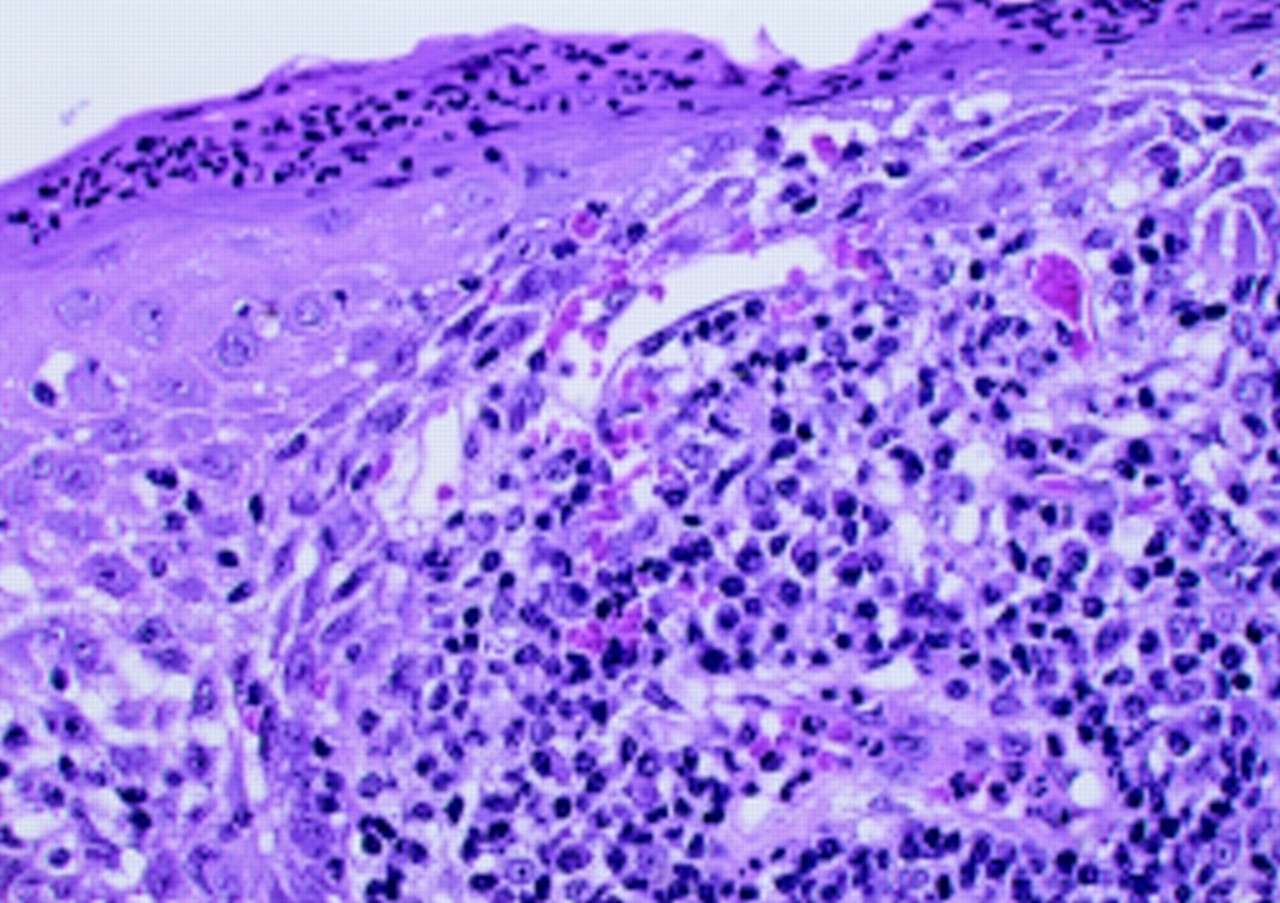
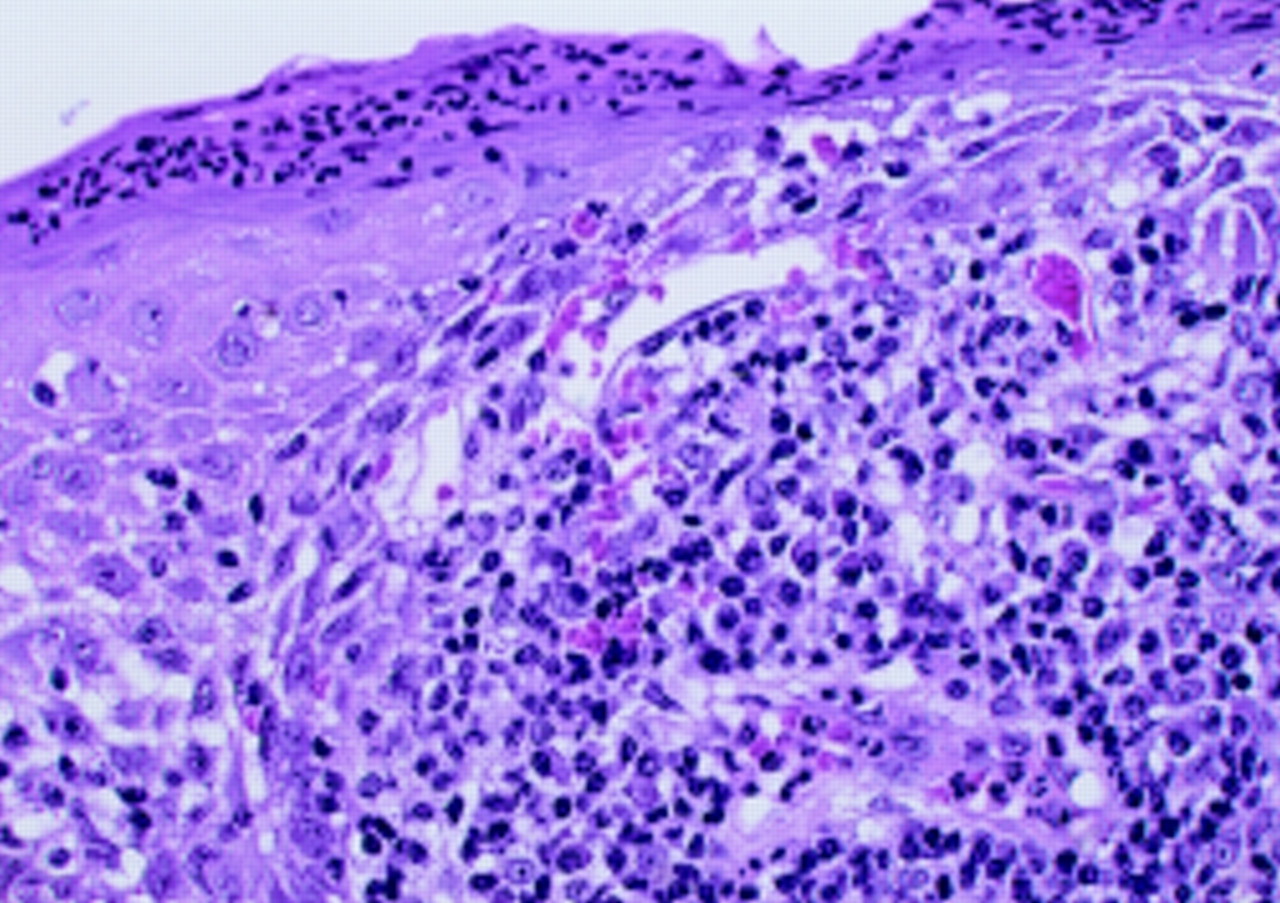
Microscopic image of atypical lymphoid cells that resemble centrocyte-like cells that invade the oesophageal epithelium (haematoxylin and eosin).

Neoplastic B cells occupying the marginal zone of the lymphoid follicles.
The tissues obtained by microdissection, in which they were manually dissected from each slide using a sterile fine needle under an inverted microscope, were treated with ethanol and xylene for dehydration and deparaffinisation, and suspended in 30 μl of proteinase K solution to digest the tissue protein for 20 hours at 37°C. After heating at 95°C for 10 minutes and cooling, the proteinase K solutions were used as DNA extracts, which were applied to polymerase chain reaction (PCR) studies for determining the clonal rearrangement of B cells. The specimens were subjected to amplification of the CDR-3 of the immunoglobulin (Ig) heavy chain gene. The PCR products for the Ig heavy chain appeared as discrete, sharp, single bands, as shown in fig 5⇓, indicating the monoclonal rearrangement of the cells. However, API2-MALT1 chimeric transcripts were not detected by reverse transcription-PCR assay. On the basis of these findings, the present tumour was diagnosed as a stage 1 extranodal marginal zone B cell lymphoma of MALT, which has been proposed by the revised European American lymphoma classification.4

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Polymerase chain reaction (PCR) products. The PCR product for CDR-3 of immunoglobulin H in this case appears as a sharp single band.
No additional therapy, such as chemotherapy or radiation was performed. Twenty two months after diagnosis and treatment, the patient is still alive and free of disease.
DISCUSSION
Although it is well known that the primary extranodal malignant B cell lymphomas of MALT, which were first described by Isaacson and Wright,5 develop from the mucosal organs, mainly from those of the gastrointestinal tract, including the stomach and colon,6–,8 they may also arise from the lung.5,9 To our knowledge there has been only one report concerning MALT lymphoma arising in the oesophagus and therefore the case reported here is a very rare case of this condition.
The reported cases diagnosed as primary oesophageal lymphoma to date are summarised in table 1⇓.10–,25 The most frequent complaint was dysphagia due to narrowing of the oesophagus. The median age of the patients was 57.9 years (range 30–86). The ratio of male to female patients was 15:9. As the immunophenotype and genetic features of MALT-type lymphoma were described according to the REAL classification which was proposed in 1994, retrospective analyses of the lymphomas reported before 1994 are possible. A lymphoma diagnosed as a centrocyte-type according to the Kiel classification, which was reported by Doki and colleagues,14 had the morphological features consistent with a MALT lymphoma. However, immunohistochemical and genetic analyses were not carried out in that case and hence it is difficult to diagnose it conclusively as a MALT lymphoma. Matsuura and colleagues15 reported a lymphoma characterised as a B cell type non-Hodgkin's lymphoma, which was diagnosed as a diffuse-lymphocytic poorly differentiated lymphoma using Rappaport's classification, and Mengoli and colleagues17 described a small lymphocytic-plasmacytoid lymphoma of the oesophagus according to the working formulation of non-Hodgkin's lymphoma. Moreover, Kurihara and colleagues21 reported a diffuse B cell oesophageal lymphoma of the small cell type with lymphoplasmacytic subtype, according to the criteria of the Japan Lymphoma Study Group. These cases were possibly MALT lymphomas as they expressed some features of this type of lymphoma.
Clinical and pathological findings of the reported primary oesophageal lymphomas
Recently, endoscopic mucosal resection, which obtains a greater amount of tissue than the conventional biopsy method, was confirmed as a useful therapeutic procedure for early gastric and oesophageal cancers. This procedure also results in an improved differential diagnosis of malignant lymphoma occurring in digestive organs.26,27 In the case reported here, endoscopic mucosal resection of the oesophagus completely removed the two tumorous lesions and therefore no additional treatment was needed. We feel that this method should be made available to treat incipient low grade MALT lymphomas.
It is well known that H pylori infection of the gastric epithelium contributes towards the occurrence of MALT lymphomas of the stomach and gastric lymphoma without chromosomal aberration of t(11;18) and regresses completely after H pylori eradication therapy.28,29 In this case, no H pylori infection of the oesophagus was found and hence other factors such as the mechanical stimuli of food, hot water, and chemicals in meals may play an important role in the development of oesophageal MALT lymphomas. The mechanisms of the occurrence of oesophageal MALT lymphoma remained to be clarified.
Because the biological and clinical characteristics of MALT lymphoma of the oesophagus are currently unknown, further study is needed. It is important to accumulate information on, and to further investigate patients with, primary oesophageal MALT lymphoma.
REFERENCES
Linked Articles
- Commentaries