Article Text

Abstract
Background: Endoscopic ultrasound (EUS) is considered the best technique for local staging of primary gastric lymphomas. Its role in the follow up of patients with gastric lymphoma following organ conserving strategies has not been established.
Aim: To compare endosonographic response assessment with results of histological evaluation.
Patients and methods: Thirty three patients with primary gastric lymphomas underwent pretreatment EUS and were followed endosonographically every 3–6 months after administration of organ conserving treatment modalities. A wall thickness of ≤4 mm with preserved five layer structure and the absence of suspicious lymph nodes was defined as endosonographic remission. Decrease in wall thickness, increase in echogenicity, and regression of lymph nodes were tested for their value to predict histological remission.
Results: A total of 158 endosonographies were performed (median 4; range 2–12). Within a median follow up period of 15 months (range 3–48), 27 (82%) patients achieved complete histological remission while endosonographic remission was found in 21 (64%) patients. Eighteen patients achieved both forms of remission, with endosonographic remission occurring later (35.1 (11–212.9) weeks v 17.6 (11–97.9) weeks; median (range); p<0.02) than histological remission. A further three patients demonstrated a false negative remission on EUS. Histological relapse was paralleled by endosonographic relapse in only one of five patients. None of the tested endosonographic parameters was able to predict histological remission.
Conclusions: In view of the inferior accuracy of EUS when compared with histology, gastroscopy with biopsy seems sufficient for the routine follow up of patients with gastric lymphoma.
- endosonography
- mucosa associated lymphoid tissue
- gastric lymphoma
- MALT, mucosa associated lymphoid tissue
- EUS, endoscopic ultrasound
- DLBCL, diffuse large B cell lymphoma
Statistics from Altmetric.com
- MALT, mucosa associated lymphoid tissue
- EUS, endoscopic ultrasound
- DLBCL, diffuse large B cell lymphoma
The gastrointestinal tract, particularly the stomach, is the most common site of primary extranodal lymphomas, which account for 25–40% of all lymphomas according to geographic location. Mucosa associated lymphoid tissue (MALT) lymphoma of the stomach accounts for 4–8% of all gastric malignancies. The discovery of a causative link between Helicobacter pylori and the development of gastric MALT-type lymphoma has revolutionised treatment options as up to 80% of patients with early gastric MALT-type lymphoma achieve complete remission of the tumour following eradication of H pylori.1–4 This benefit however appears to be restricted to patients with lymphoma limited to the mucosa and submucosa3 while the MALT-type lymphoma specific chromosomal translocation t(11;18) has been discovered to be a negative predictive parameter for regression following H pylori eradication.5 Surgical intervention has been the preferred form of treatment in the past but currently organ conserving approaches are increasingly being applied as both irradiation and chemotherapy have given excellent results.6,7
In case of diffuse large B cell lymphoma (DLBCL) of the stomach, either arising de novo or following transformation from MALT-type lymphoma, conservative approaches have also given excellent results, as gastric DLBCL appears to be a highly chemosensitive disease.7
Endoscopic ultrasound (EUS) has been shown to be an accurate procedure for primary staging in MALT-type lymphoma of the stomach,8–10 and staging by endosonography may potentially predict the response to Helicobacter eradication in early stage disease.3,11 However, only limited data are available on the value of endosonography in the follow up of patients with MALT-type lymphoma of the stomach as only small series have described the endosonographic characteristics of the stomach wall after radiation and/or chemotherapy.8,12–15 To date, it is not known whether endosonographic follow up can monitor the response to treatment or is predictive for relapse of the disease, and histological assessment is currently considered the gold standard for assessment of treatment response in gastric lymphoma. In addition, the value of EUS in patients with gastric DLBCL following chemotherapy has not been established. The objective of this study was therefore to address the potential value of regular endosonographic follow up in patients undergoing stomach conserving therapy for gastric lymphoma.
PATIENTS AND METHODS
Between January 1996 and March 2001, 33 patients with primary gastric lymphoma undergoing organ conserving therapy were included in the study. Patients with gastric lymphoma of MALT-type according to the criteria established by Isaacson and included in the recently published WHO classification of lymphoid neoplasms for extranodal marginal zone B cell lymphoma of MALT-type, were studied, as were patients with gastric DLBCL with or without a MALT-type component.16 Histological assessment of biopsy samples from all patients included in the study was performed by a single reference pathologist (AC). In all patients, immunological phenotyping on paraffin sections was done for demonstration of light chain restriction and for the phenotype CD20+CD5-CD10-cyclinD1- which, in the context of microscopic appearance, is consistent with marginal zone B cell lymphoma of MALT-type. Primary gastric high grade B cell lymphoma was defined as high grade lymphoma arising in a background of extranodal marginal zone B cell lymphoma of the MALT-type. In patients without a MALT-type component, absence of disease dissemination beyond local nodes, as judged by clinical staging, served as an indication of a gastric origin of the lymphoma. In addition, samples were evaluated for the presence of H pylori or signs of changes associated with H pylori gastritis, and all patients underwent serological testing for antibodies against H pylori. Extension of disease was defined according to the Ann Arbor staging system, as modified by Musshoff17 and Radaszkiewicz and colleagues.18 In addition to the classic Ann Arbor classification, this modification accounts for depth of infiltration in stage I (confined to versus beyond submucosa) and extension of lymph node involvement in stage II (regional versus beyond regional).
All patients with evidence of H pylori infection received eradication therapy which was successful in all. Lymphomas not regressing after eradication therapy within one year or with disease advanced beyond the submucosa (that is, stage EI2) were treated additionally with chemotherapy and/or radiotherapy, while H pylori negative patients or patients with DLBCL were referred directly for chemotherapy or radiation. After pretreatment EUS staging, patients were followed every 3–6 months by means of endosonography and gastroscopy with multiple biopsies according to a standardised protocol. This required a minimum of 8–10 biopsies, including biopsies from macroscopically normal appearing mucosa. At each visit endosonography with a radial sector transducer (GF-UM3 or UMQ130; Olympus, Tokyo, Japan) of the upper gastrointestinal tract and gastroscopy (GIF-100, Olympus) with biopsy sampling were performed. Complete remission was defined on histological grounds as absence of lymphomatous involvement in at least two following biopsy specimens taken at an interval of at least four weeks or more.
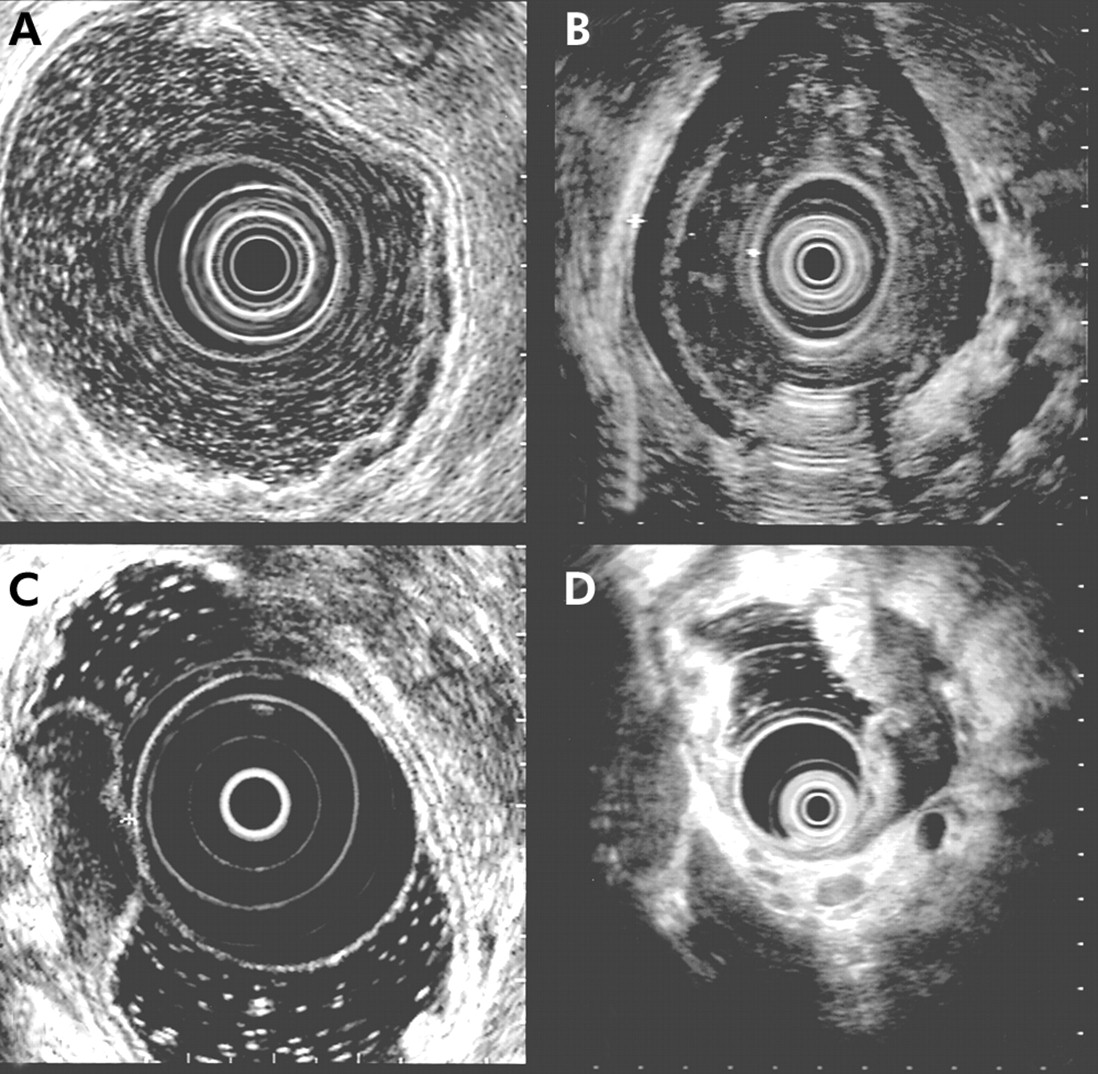
During the initial EUS, the gastric wall was assessed for different patterns of lymphoma infiltration with reference to Suekane and colleagues9 with some modifications—that is, superficial-type, diffuse infiltrating-type, mass forming-type, and mixed-type. A lesion was rated as superficial-type when thickening of the second and/or third layer with a preserved five layer pattern was seen. The diffuse infiltrating-type showed a diffuse transmural infiltrate of the gastric wall, with the five layer structure not always being distinguishable. In the mass forming-type, a localised hypoechoic mass with a clear margin was observed, with the mass being mainly located in the third or fourth layer. The mixed-type was defined as a combination of the diffuse infiltrating- and mass forming-type in cases were a mass forming-type without clear margins was detected. An example of each type is given in fig 1. At each examination the maximum thickness of the gastric wall (in mm) was measured. Furthermore, the five layer pattern of the gastric wall was classified as preserved, disturbed, or abolished. The echogenicity of the infiltrate was rated as echo poor, echo medium, or echo rich using the neighbouring normal appearing mucosa as reference. Finally, lymph node involvement based on previously established criteria—that is, hypoechoic, rounded, well demarcated, >1 cm—was recorded.19 A wall thickness of ≤4 mm with preserved five layer structure and the absence of suspicious lymph nodes was defined as endosonographic complete remission. Patients with normal EUS findings at the initial investigation were considered as endosonographic remission.

(A–D) Endosonographic patterns of lymphoma infiltration. (A) Superficial-type with thickening of the second and third layer with preserved five layer pattern. (B) Diffuse infiltrating-type with a transmural echo poor infiltrate involving the entire gastric wall. (C) Mass forming-type with an echo poor clearly demarcated mass. (D) Mixed-type as a combination of the infiltrating and mass forming-type. Additionally, an echo poor lymph node can be seen in the centre below the scope.
In order to find a parameter to predict complete histological remission by endosonography, we tested the difference in wall thickness, increase in echogenicity, and regression of lymph nodes for their predictive value.
Statistics
Statistical evaluation was performed using the SPSS software (SPSS Inc., Chicago, Illinois, USA). Results are expressed as median (range). Comparison between groups was made using the Fisher’s exact test or Wilcoxon’s test as appropriate. Statistical significance was defined as p<0.05.
RESULTS
A total of 158 endosonographies (median 4 (range 2–12)) were performed in 33 patients, with a median follow up of 15 months (range 3–48). Patient characteristics, disease stage, H pylori status, localisation of lymphoma, sonographic pattern at the initial examination, and histological findings are given in table 1. Twenty seven patients (82%) achieved complete remission during follow up, as assessed by histology. Endosonographic complete remission was found in only 21 (64%) patients, including three patients with normal endosonographic findings at the initial investigation. One of these patients did not reach histological remission. Neither H pylori status nor histological grading influenced endosonographic response. Two patients received eradication therapy as sole therapy while all other patients were treated with chemo- and/or radiotherapy. Concordant findings of histology and endosonography were found in 21 patients (64%) (table 2). Eighteen patients achieved both histological and endosonographic remission during the follow up period. After exclusion of two patients with normal findings at their initial endosonography, endosonographic remission in these patients occurred later (35.1 (11–212.9) weeks v 17.6 (1–97.9) weeks; median (range); p<0.02) than histological remission. In only one patient with abnormal endosonographic findings at the initial investigation did endosonographic remission precede histological remission. The time course to achieve histological and endosonographic remission is shown in fig 2. Patients who achieved histological and endosonographic remission had a longer follow up compared with patients who achieved histological remission only (25.6 (12.7) months v 9.1 (6.7) months; mean (SD); p<0.01).
Patient and tumour characteristics
Cross tabulated relation of histological and sonographic remission at the end of follow up

{kind=link}
{kind=link}
Time course of histological and endosonographic remission (n=16). Only patients who achieved both forms of remission were included. Patients with normal findings at initial endosonography were excluded (n=2). The filled circle (•) indicates the case with endosonographic remission preceding histological remission.
Lymph node involvement was found in 16 (48.5%) patients at the initial endosonography. Only one of 10 patients (10%) with a superficial-type had suspicious lymph nodes. In contrast, lymph node involvement was found in nine (56.3%) patients with the diffuse infiltrating-type, two (66.6%) with the mixed-type, and in all four patients (100%) with the mass forming-type.
In five patients a histological relapse occurred during follow up. Median time until the occurrence of relapse was 46.8 weeks (range 7.3–55.5). However, this was accompanied by endosonographic relapse in only one patient (with a mass forming endosonographic pattern), demonstrating a new echo poor infiltrate in the area of the previous mass on EUS. Three other patients had a superficial-type of infiltrate on the initial investigation, without any endosonographic abnormality in one patient. The remaining patient had a diffuse infiltrating endosonographic pattern.
None of the tested endosonographic parameters predicted complete histological remission. Neither the decrease in gastric wall thickness nor the increase in echogenicity correlated with complete histological remission. Likewise, regression of lymph nodes was not correlated with histological remission or residual disease, respectively.
DISCUSSION
In the present study, we specifically addressed the value of endosonography in the follow up of patients with primary gastric lymphoma. To date, several series have been published describing endosonographic features in patients with gastric lymphoma after stomach conserving therapy.13 In a recent study including 24 patients15 the authors suggested that histological remission is usually accompanied by specific endosonographic changes—that is, a decrease in wall thickness and an increase in echogenicity of the involved gastric wall—and eventually results in normalisation of endosonographic findings. However, strict validation of these parameters during a prolonged follow up period has not been performed so far. In our study, similar changes, as reported by others,13,15 were seen in patients achieving histological remission. These endosonographic changes nevertheless took place significantly later than histological remission. This was reflected by a mean interval of 29.1 weeks to reach histological remission compared with 41.7 weeks to achieve endosonographic remission. In addition, follow up in patients with both definitions of remission was longer than in those with histological remission alone. Therefore, it seems likely that a longer follow up would eventually result in endosonographic remission in a higher percentage of patients. This hypothesis is supported by the findings of Lügering et al who described normalisation of the gastric wall in all patients with histological proven remission after a longer period of follow up.15 From this observed time lag between histological and endosonographic remission, it is not surprising that neither of the tested endosonographic parameters was able to predict histological remission in our series. However, it would have been expected that endosonography is able to correctly assess recurrence of disease, as has been suggested by Lévy and colleagues.13 Unfortunately, this was not uniformly the case in the present study. In only one of five patients who experienced relapse of their disease during follow up did accompanying specific endosonographic changes develop (that is, echo poor infiltration). This patient had a mass forming-type of lymphoma mainly located in the submucosa and proper muscle layer of the stomach wall. It has to be noted however that three of the remaining four patients had only minor or even no endosonographic changes at their initial investigation and were classified as superficial-type lymphoma. Furthermore, all had MALT-type lymphoma without signs of transformation. A relapse of this relatively indolent disease might therefore take longer to result in detectable endosonographic changes compared with histological changes. This is especially true in a setting where regular follow up examinations are carried out. In addition, one cannot completely rule out the presence of a sampling error—that is, focal persistence of the lymphoma in spite of negative histology.
An interesting finding of our study was that even in patients with complete endosonographic normalisation of the gastric wall, residual disease could be detected on histological evaluation of biopsy samples in three cases. Even though one of these patients eventually achieved complete histological remission, we have no clear cut explanation for why in this patient endosonographic remission preceded histological remission as opposed to the majority of the rest of our patients. However, it has been shown that endosonography underestimates the surface extension of the lymphomatous infiltrate in the stomach wall.10 It therefore seems likely that in cases of a prompt response to therapy, minute residual disease can only be detected by histology. Another possibility could be a higher degree of acute inflammation at the initial examination. Acute gastritis with an accompanying oedema may result in an endosonographically detectable thickening of the mucosa.20 However, no difference in disease specific parameters or treatment modalities were identified that could explain this finding.
The problem of endosonographic follow up and restaging after chemo- and/or radiotherapy has been addressed in a few studies in solid tumours of the oesophagus, stomach, or rectum.21–24 In these studies, in common with ours, endosonography proved less specific in the assessment of the primary tumour (T staging) following chemo- and/or radiotherapy. This was due to the fact that endosonography tended to overstage residual disease as it was not able to differentiate between tumorous infiltration and inflammatory response to therapy.
Taken together, our findings have potential implications for the use of endosonography in patients with gastric lymphoma of the MALT-type and/or diffuse large cell histology. Apart from a well documented value in the initial staging and the potential ability to predict the response to H pylori eradication, endosonography appears to provide little additional information to endoscopy and histology during follow up.
In view of its inferior accuracy compared with histology and the limited availability of endosonography, gastroscopy with biopsy seems sufficient for routine follow up of patients with primary gastric lymphoma undergoing organ conserving treatment.