Article Text

Abstract
Background: Collagenous colitis is characterised by diarrhoea, lymphocytic inflammation, and a thickened subepithelial collagen layer in the colorectal mucosa. No standard treatment of the disease is established.
Aims: To investigate the clinical and histological effect of oral budesonide (Entocort, AstraZeneca) in the treatment of collagenous colitis.
Patients: Twenty patients with collagenous colitis (collagen layer >10 μm) and diarrhoea (>4 stools/day and/or stool weight >200 g/day).
Methods: A randomised, double blind, placebo controlled trial of budesonide treatment. Patients were randomised to placebo or budesonide for eight weeks. Stool frequency and stool weight were registered before and after treatment. Sigmoidoscopy was performed before and after treatment, and biopsies at fixed locations were obtained for morphometric analysis.
Results: Ten patients were randomised to budesonide and 10 to placebo. All 10 patients receiving budesonide had a clinical response compared with two in the placebo group (p<0.001). In the budesonide group, stool weight was reduced from 574 g/day to 200 g/day and stool frequency was reduced from 6.2/day to 1.9/day (p<0.01). The histological inflammation grade in the sigmoid mucosa and the thickness of the collagen layer were significantly reduced. A correlation between the grade of inflammation as well as collagen layer thickness and stool weight was found. No side effects were reported. Eight of 10 patients had relapse of symptoms within eight weeks after stopping treatment.
Conclusions: Budesonide is a highly effective and well tolerated treatment of collagenous colitis. There is a high risk of relapse after stopping eight weeks of treatment.
- collagenous colitis
- microscopic colitis
- diarrhoea
- inflammatory bowel disease
- morphometry
- randomised controlled trial
Statistics from Altmetric.com
- collagenous colitis
- microscopic colitis
- diarrhoea
- inflammatory bowel disease
- morphometry
- randomised controlled trial
The first case of collagenous colitis was described in 1976 by Lindström1 and now the disease is recognised as a distinct clinicopathological entity. It is characterised by chronic watery diarrhoea. Endoscopic examination reveals only minimal or absent mucosal changes. In biopsies from the colon mucosa, a characteristic abnormal thickening of the subepithelial collagen layer as well as lymphocytic infiltration of the epithelium and the lamina propria is found.2,3 The aetiology and pathogenesis of collagenous colitis are still unknown but it appears to be caused by mucosal injury from a luminal factor. Some observations indicate that the faecal stream contains the noxious agent but the nature of this luminal factor is unknown. Observations on patients with collagenous colitis after faecal stream diversion could indicate that this pathogenic agent is transmitted from the small bowel.4
Large studies of treatment of collagenous colitis have not been performed and no standard treatment has been established. Therapy is based on single case reports and several uncontrolled small series. In a retrospective study, treatment with non-specific antidiarrhoeals, 5-ASA, or prednisolone was recommended.5
Budesonide is a topical acting corticosteroid released in the small intestine and the ascending colon. It is characterised by a high receptor binding affinity and a high first pass metabolism in the liver. In controlled clinical trials budesonide was shown to be effective in the treatment of inflammatory bowel disease.6,7 In two uncontrolled studies8,9 and in one placebo controlled study10 budesonide also seemed to be of therapeutic benefit in collagenous colitis. The aim of this study was to investigate the clinical and histological effect of budesonide in the treatment of collagenous colitis.
METHODS
Patients
In this study, patients at least 18 years old with clinically active collagenous colitis were included. Diagnostic criteria for collagenous colitis were histological findings of a collagen layer more than 10 μm located beneath the surface epithelium in colonic mucosa. Clinical activity was defined as a daily stool frequency of >4 or stool weight >200 g/day. Patients treated with anti-inflammatory drugs (aminosalicylates, corticosteroids, azathioprine) within the last three months were excluded. Additional exclusion criteria were other chronic gastrointestinal diseases. Stool samples for pathogens, parasites, and ova should be negative. Patients with clinically significant renal or hepatic disease and pregnant or breast feeding women were ineligible. The protocol was approved by the local ethics committee and all participants provided written informed consent. Thirty two patients who attended our outpatient clinic for collagenous colitis were evaluated for the trial. Twenty patients (16 women and four men) fulfilled the study criteria and accepted participation. Median age was 54 years (40–80).
Methods
The study was a randomised, double blind, placebo controlled trial. Patients fulfilling the study criteria were randomised to receive placebo or active treatment with budesonide for eight weeks (9 mg for four weeks, 6 mg for two weeks, and 3 mg for two weeks). The budesonide formulation used was a gelatin capsule containing acid stable micro granules (Entocort 3 mg; AstraZeneca). The capsule dissolves at a pH of 5.5 or higher. This formulation releases budesonide in the distal part of the ileum and ascending colon. The placebo medication was identical in appearance. No anti-inflammatory medication other than the study drugs was allowed. Concomitant antidiarrhoeal drugs were allowed except during periods of stool weight determination.
At entry, patient demographic data and medical history were recorded. In all patients routine laboratory analyses and stool cultures were performed. Before and after treatment current clinical symptoms were recorded. Stool frequency and stool weight were assessed for three days. Sigmoidoscopy was performed before and after treatment with biopsies at fixed intervals in the distal 40 cm of the colon. The primary efficacy end point was clinical remission defined as a reduction in stool frequency or stool weight of >50%. After stopping treatment patients were followed for eight weeks for signs of relapse of clinical symptoms.
Histology
Biopsy specimens from all patients were reviewed independently by two experienced pathologists (VV, PST). Two biopsy specimens were taken from six fixed locations 40, 33, 26, 19, 12, and 5 cm above the anal verge, respectively. In order to obtain well oriented specimens, each biopsy specimen was stretched out on a millipore filter before fixation in 4% formaldehyde for 24–48 hours. Biopsies were divided into two parts and embedded in paraffin. Three sections cut perpendicular to the mucosal surface at different levels from each block were stained with haematoxylin and eosin and Masson’s trichrome. Histopathological evaluation was performed blindly by the two pathologists. One pathologist measured the thickness of the collagen layer at 10 points at a magnification of 600 on a monitor screen. The first measuring point was randomly chosen, the other nine were placed at intervals of 166.67 μm (10 cm on the screen) from the first point to avoid selection bias, so called “systematically random sampling”.11 This procedure was performed at every biopsy level. The other pathologist measured the grade of inflammation in the lamina propria semiquantitatively on a scale from 0 to 3: 0=no inflammation; 1=mild—that is, inflammatory infiltrate confined to the upper part of the lamina propria; 2=moderate—that is, inflammatory infiltrate extending beyond the base of the crypts; and 3=severe—that is, heavy inflammatory infiltrate occupying the lamina propria and infiltrating the lamina muscularis mucosa (fig 1). For each patient the average grade of inflammation and the average thickness of the collagen layer was calculated for the sigmoid colon (biopsies 1–4), rectum (biopsies 5–6), and all biopsies (1–6). To estimate the reproducibility of the morphometric methods, the thickness of the collagen layer of 24 biopsy specimens was measured blindly by both pathologists, as well as the grade of inflammation in 10 biopsy specimens.

Grades of inflammation in the colorectal mucosa: (A) 0=no inflammation; (B) 1=mild inflammation—that is, the inflammatory infiltrate is confined to the luminal part of the mucosa; (C) 2=moderate inflammation—that is, the inflammatory infiltrate extends beyond the base of the crypts; and (D) 3=severe inflammation—that is, the heavy inflammatory infiltrate occupies the entire lamina propria and infiltrates the lamina muscularis mucosa.
Statistical analysis
Fisher’s exact test, the Wilcoxon test for pair differences, and the Spearman rho test were used to compare data between and within groups where appropriate; p values <0.05 were considered statistically significant. In order to assess the variation between the results of the two pathologists concerning the thickness of the collagen layer and the grade of inflammation, the variation coefficient between the results of the two observers was calculated.
RESULTS
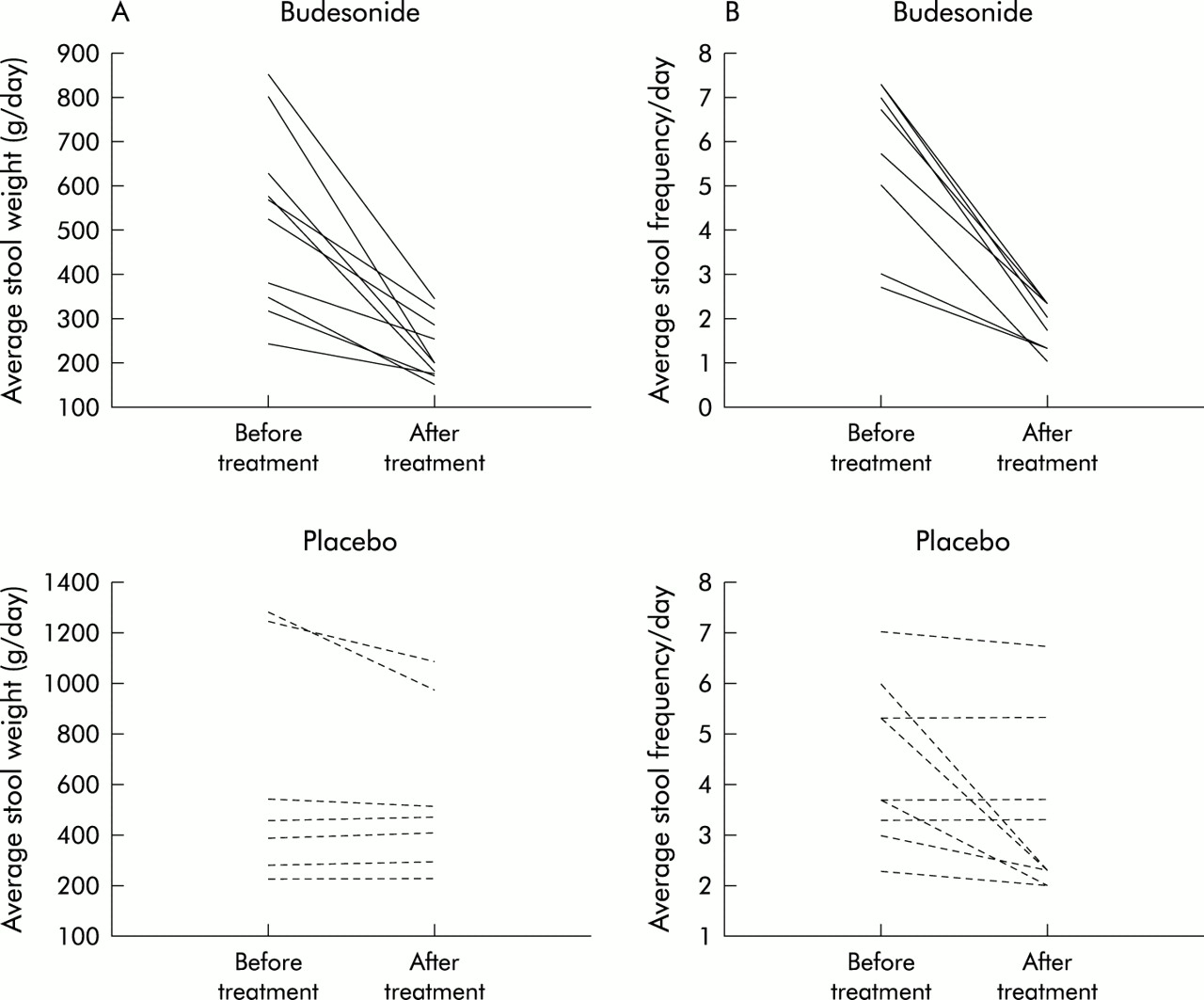
Ten patients were randomised to budesonide treatment and 10 patients to placebo treatment. Clinical and histological baseline characteristics were similar in both groups (table 1). All 10 patients who received budesonide had a reduction in stool frequency and/or stool weight of more than 50% whereas only two patients on placebo had a similar response (p<0.001). Median stool frequency was reduced from 6.2 (range 2.7–7.3) per day to 1.9 (range 1.0–3.3) per day in the budesonide group and from 4.5 (range 2.3–7.0) per day to 2.8 (range 2.0–9.0) per day in the placebo group. All patients had daily stool weights above 200 g before treatment. In the budesonide group stool weight was reduced in all 10 patients, in seven patients by more than 50%. Median stool weight was reduced from 574 g/day (range 241–853) to 200 g/day (range 151–346). In the placebo group, seven patients had their daily stool weight measured after treatment; none of these patients had a reduction of more than 50%. The change in median was from 463 g/day (range 229–1280) to 475 g/day (range 232–1084) (fig 2 ). Two patients refused to perform another faecal sampling after treatment, and the third patient had a volume more than 500 g/day but the exact volume was not measured.
Baseline characteristics of patients

Stool weight (A) and stool frequency (B) before and after eight weeks of therapy with budesonide or placebo.
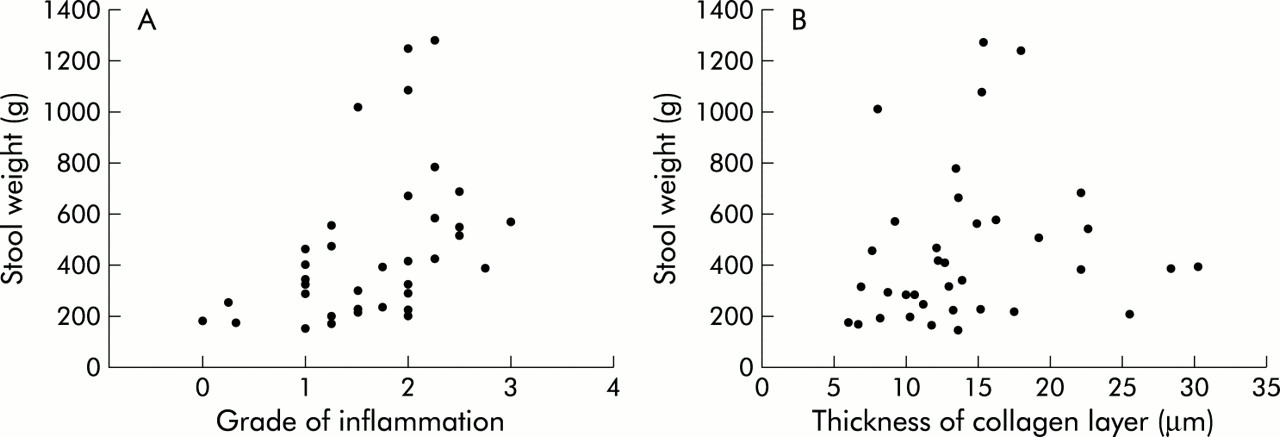
The grade of inflammation at entry was less pronounced in the rectum (median 1.3 (range 0.5–3.0)) than in the sigmoid colon (median 2.3 (range1.3–3.0)) and the median collagen layer was thinner (rectum 9.7 μm (range 4.7–15.4), sigmoid colon 15.6 μm (range 8.0–25.5)). In 11 patients the subepithelial collagen layer in the rectum was less than 10 μm. In the sigmoid colon the median inflammation grade was reduced from 2.3 (range 1.5–2.75) to 1.0 (range 0.0–1.25) (p<0.01) in the budesonide group whereas no significant change was detected in the placebo group (1.9 (range 1.0–2.5) to 1.5 (range 1.0–2.5); NS) (fig 3). The collagen layer in the sigmoid colon was reduced after treatment in the budesonide group (median 15.6 μm (range 8.0–25.5) to 10.2 μm (range 6.1–13.3); p<0.02) but not in the placebo group (median 15.3 μm (range 7.6–30.3) to 12.7 μm (range 8.8–19.7); NS). The grade of inflammation in the sigmoid colon and stool weight correlated significantly (rho=0.53; p<0.001), and a positive correlation between the thickness of the collagen layer and stool weight (rho=0.34; p<0.05) was also found (fig 4). In the rectum, the effect of budesonide was less pronounced and no significant effect on grade of inflammation or collagen layer thickness was detected. However, a positive correlation between rectal collagen layer thickness and stool weight (rho=0.37; p<0.05) but not between grade of inflammation and stool weight (rho=0.27; NS) was found in the rectum.

Morphology of the sigmoid mucosa before (A) and after (B) treatment with oral budesonide.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Correlation between grade of inflammation in the sigmoid colon and stool weight. Rho <0.531, p<0.001, n=36. (B) Correlation between thickness of the collagen layer in the sigmoid colon and stool weight. Rho <0.337, p<0.05, n=36.
No systematic difference between the measurements of the two pathologists was observed. The variation coefficient was 0.19 concerning measurement of the thickness of the collagen layer and 0.17 for determination of the grade of inflammation.
DISCUSSION
This study demonstrates that budesonide has an excellent effect on the clinical symptoms of collagenous colitis. This is in accordance with previous open studies8,9 and a recently published placebo controlled trial.10 Collagenous colitis is characterised by watery diarrhoea and in the present study up to 10 bowel movements a day were found. In most cases the disease has a chronic course with continuous or relapsing symptoms, and the average symptom duration in our study was 9.3 years. We found a reduction in stool frequency and stool weight. Patients with collagenous colitis generally suffer little morbidity but diarrhoea affects daily living. Improvement in clinical symptoms therefore is of great importance and in our study all patients treated with budesonide reported subjective improvement. Quality of life parameters were not assessed in this study but we would recommend this in the future.
In a previous uncontrolled study12 the effect of prednisolone treatment was evaluated, and treatment was associated with a decrease in stool frequency. However, the effect was transitory and diarrhoea recurred when treatment was discontinued or the dose reduced. Treatment with prednisolone for prolonged periods of time has been recommended but the risk of serious side effects must be recognised.
Budesonide has a topical effect and low systemic activity because of a high first pass metabolism in the liver. Therefore, the risk of corticosteroid associated side effects should be reduced. In a previous study of patients with Crohn’s disease, budesonide was compared with prednisolone. Budesonide had fewer corticosteroid related side effects and less effect on adrenal function.6 Corticosteroid related side effects were not reported in our study and the 9 mg dose of budesonide has been found to be safe in previous studies. Cases of prednisolone refractory collagenous colitis successfully treated with budesonide have been described.13 Budesonide has a high receptor binding affinity and an enhanced retention time in the mucosa compared with prednisolone and this could be the explanation for a better anti-inflammatory effect of budesonide in collagenous colitis.
Symptoms rapidly return when medication is stopped. In our study, 8/10 patients had relapse of clinical symptoms within eight weeks after withdrawal of budesonide treatment. Most patients may need sustained treatment to remain symptom free and the effect of maintenance treatment with budesonide in patients with collagenous colitis should be studied further. Duration of treatment has to be determined and the long term effects of continuous budesonide treatment should also be studied.
In the normal colonic mucosa the subepithelial collagen band varies from 3 to 6 μm whereas collagenous colitis is characterised by a thickened subepithelial layer and inflammatory infiltrate. The collagen band varies in thickness and should focally exceed at least 10 μm to be diagnostic of collagenous colitis.14,15 Previously it has been shown that the histological findings of collagenous colitis are unevenly distributed16 and in addition tangential sectioning of the tissue can create false thickening of the basement membrane. Multiple biopsy specimens and careful measurement is important. In this study multiple random measurements in well oriented biopsies were done by two pathologists and a good concordance rate was found. It has been suggested that rectal biopsies underestimate the diagnosis.14 In other studies however is was found that collagenous colitis can be diagnosed from rectal or sigmoid colon biopsies in more than 90% of cases.17,18 The present study demonstrates that it is important to obtain proximal biopsies in patients with chronic diarrhoea as the collagen layer is less pronounced in the rectum. In more than half of the patients in our study, the diagnosis of collagenous colitis could not have been established from only rectal biopsies. We found a reduction in the inflammatory infiltrate in budesonide treated patients and the reduction was more prominent in the proximal part of the sigmoid colon than in the rectum. In the present study we found a positive correlation between symptoms and the thickness of the collagen layer. Lee and colleagues19 analysed a mixed material of collagenous colitis and lymphocytic colitis and found that the intensity of clinical symptoms was unrelated to the thickness of the collagen band but a correlation between daily stool weight and inflammation in the lamina propria was found. In our study the correlation between symptoms and grade of inflammation was higher, and these findings suggest that clinical symptoms may be more closely related to colonic inflammation than to subepithelial collagen deposition.
In conclusion, we found that budesonide is highly effective and well tolerated in the treatment of collagenous colitis. Effects on both clinical symptoms and inflammatory infiltrate were seen. However, there is a high risk of relapse after stopping eight weeks of treatment.