Article Text

Abstract
Background and aims: Steatosis, a frequent histological finding in patients with chronic hepatitis C (CHC), has been suggested to influence liver fibrosis progression. The aim of the present study was to evaluate in patients with CHC and paired liver biopsies the relationship between the evolution of steatosis and that of fibrosis between the two biopsies.
Methods: Ninety six patients were selected according to the following criteria: absence of treatment; absence of cirrhosis at initial biopsy; and serum hepatitis B surface antigen and human immunodeficiency virus antibody negativity. Degrees of necroinflammatory activity, fibrosis, and steatosis grades were assessed in the two biopsies. In addition to histological lesions, parameters studied included the source of infection, duration of infection, body mass index, alcohol intake, alanine aminotransferase levels, hepatitis C virus genotype, and viral load.
Results: The mean interval between the two biopsies was 48 (32) months. Steatosis was found in 54% of patients at first biopsy, and was severe in 9%. Worsening of steatosis was observed in 34% of patients, stability in 50%, and improvement in 16%. Worsening of steatosis was significantly associated with hepatic fibrosis progression in patients with (p=0.03) or without (p<0.03) steatosis at diagnosis. Overall, fibrosis progression was observed in 31% of patients and stability in 69%. In a univariate analysis, fibrosis progression was associated with male sex (p=0.05), worsening of histological activity (p=0.04), and worsening of steatosis (p=0.0003). In a multivariate analysis, the only factor independently associated with fibrosis progression was worsening of steatosis (worsening v improvement/stability: odds ratio 4.7 (95% confidence interval 1.3–10.8); p=0.0001).
Conclusions: Our results suggest that in untreated patients with CHC and serial liver biopsies, fibrosis progression is strongly associated with worsening of steatosis.
- hepatitis C
- steatosis
- fibrosis
- liver biopsy
- HCV, hepatitis C virus
- CHC, chronic hepatitis C
- BMI, body mass index
Statistics from Altmetric.com
Chronic hepatitis C virus (HCV) infection is associated with a wide spectrum of liver histological lesions, ranging from mild chronic hepatitis to cirrhosis and hepatocelullar carcinoma.1 The course of HCV related hepatic disease varies markedly from one patient to another. Several factors, including age at exposure, duration of infection, alcohol intake, and male sex, have been shown to be independently associated with fibrosis progression.2–4 However, even in the absence of these factors, disease progression may be observed in some patients, suggesting a role for other factors that remain to be identified.
Hepatic steatosis is a frequent histological finding in patients with chronic hepatitis C (CHC) and, in addition to bile duct damage and lymphoid follicles, it has been shown to be a characteristic feature of chronic hepatitis C virus infection.5–9 Whether steatosis is mainly related to host factors or to the virus itself is uncertain. It must be stressed however that even when all causes such as obesity, diabetes, dyslipidaemia, and excessive alcohol intake are carefully excluded, a significant proportion of patients with CHC still have steatosis.10 In vitro and in vivo studies have demonstrated that HCV core protein could induce steatosis in transfected cells11 and transgenic mice.12 Recently, it has also been suggested that hepatic steatosis was the morphological expression of a viral cytopathic effect in patients infected with HCV genotype 3.13
The role of steatosis in the development of fibrosis in patients with CHC is still debated. Several studies10,14–18 have recently suggested a relationship between the degree of steatosis at histology and that of liver fibrosis, and in some14–18 this relationship remained significant after adjustment for potential confounding factors. In addition, two recent studies14,19 suggested that steatosis, when severe, was associated with a higher annual rate of fibrosis progression. It must be stressed however that in these two studies: (1) fibrosis progression was estimated indirectly on a single liver biopsy according to the model described by Poynard and colleagues2; and (2) steatosis evolution over time and its potential contribution to fibrosis progression were not assessed.
The aim of this study was to evaluate steatosis evolution and its relation to liver fibrosis progression in untreated patients with CHC and paired liver biopsies.
PATIENTS AND METHODS
Study population
Between March 1996 and September 1999, 558 consecutive patients with CHC infection (defined by positive serum antibodies to HCV by means of a second or third generation HCV enzyme linked immunosorbent assay (Ortho Diagnostic, Raritan New Jersey, USA) and detectable serum HCV RNA (Amplicor HCV; Roche Molecular Systems, Pleasanton, California, USA) had a liver biopsy performed in our department. Ninety six patients were selected for the study of steatosis evolution and fibrosis progression on the basis of: (1) at least two liver biopsies available; (2) absence of antiviral therapy before the first biopsy and between the two biopsies; (3) absence of cirrhosis at initial biopsy; and (4) serum hepatitis B surface antigen and human immunodeficiency virus antibody negative.
The following epidemiological data were obtained from all patients: age at diagnosis, sex, source of infection (transfusion, intravenous drug use, other source, unknown source), duration of infection in patients with a known risk factor (calculated as the interval between the presumed date of infection), age at exposure, and interval between the two biopsies. Body mass index (BMI kg/m2) was calculated and average alcohol intake during the six months preceding the first liver biopsy and during the interval between the two biopsies was obtained.
Virological tests
Serum antibodies to HCV were detected by means of a second or third generation HCV enzyme linked immunosorbent assay (Ortho Diagnostic), according to the manufacturer’s instructions. All tests were routinely performed at the time of the first visit to our unit.
HCV RNA was determined in all patients using a commercial assay (Amplicor HCV; Roche Molecular Systems) at the time of the first biopsy.
HCV genotype was determined in all patients using a line probe assay (Inno-LiPA HCV II; Innogenetics, Ghent, Belgium). Genotypes were classified according to Simmonds and colleagues.20
HCV viral load was determined by means of the second generation branched DNA assay (Quantiplex HCV RNA 2.0; Bayer Diagnostics, Emeryville, California, USA) on stored serum samples at the time of the first biopsy.
Histological studies and steatosis evaluation
Liver biospy specimens of more than 10 mm in length were fixed in formalin, paraffin embedded, and stained with haematoxylin-eosin-safran, or picroSirius red for collagen, and Perls’ technique for iron. For each liver biopsy specimen, histological fibrosis and activity were scored according to the METAVIR classification.21 Grading of histological activity that evaluates the intensity of necroinflammatory lesions was as follows: A0, no activity; A1, mild activity; A2, moderate activity; and A3, severe activity. Fibrosis was staged on a 0–4 scale: F0, no fibrosis; F1, portal fibrosis without septa; F2, few septa; F3, numerous septa without cirrhosis; and F4, cirrhosis. Paired biopsy samples were read by the same pathologist (ESZ) blinded to the demographic, clinical, and biological data of the patients.
Histological evolution was assessed by comparing the activity scores (A) and the fibrosis (F) scores between the two biopsies: improvement was defined as a decrease in A or F scores of at least one; worsening was defined as an increase in A or F scores of at least one; stability was defined as identical A or F scores.
Steatosis was graded on the two liver biopsies as follows21,22: none; mild (involving less than 10% of hepatocytes); moderate (involving 10–30% of hepatocytes); and severe (involving more than 30% of hepatocytes). Steatosis evolution was assessed by comparing the grades between the two biopsies: improvement was defined as a decrease of at least one grade; worsening was defined as an increase of at least one grade; stability was defined as identical steatosis grades.
Statistical analysis
Descriptive statistics are provided as means (SD). One way analysis of variance (ANOVA) or the Mann-Whitney test was used when necessary for statistical comparison of quantitative data, whereas the κ2 test or Fisher’s exact test was used when necessary for qualitative data. A p value <0.05 was considered significant.
To assess the independent value of each parameter related to histological evolution in the univariate analysis (p<0.1), a multivariate analysis was performed by means of a stepwise logistic regression analysis. All analyses were performed using the BMDP statistical software (BMDP statistical software Inc, Los Angeles, California, USA).
RESULTS
General characteristics of the patients at the time of the first liver biopsy
The characteristics of the 96 patients are given in table 1. They were 59 males and 37 females with a mean age of 41 (11) years. Infection was by blood transfusion in 41% of patients and by intravenous drug injection in 26%. Mean BMI was 24.6 (2.8) kg/m2, ranging from 19.3 to 31.2, with 13% of patients having a BMI >28 kg/m2. Ten per cent of patients had an alcohol intake >40 g/day. Patterns of alcohol intake during the interval between biopsies were as follows: in patients with an intake of ≤40 g/day, all patients continued to take small amounts of alcohol or discontinued alcohol intake; in the 10 patients with an intake >40 g/day, seven patients discontinued alcohol intake whereas the three others still had excessive alcohol intake. Sixty two per cent of patients were infected with HCV genotype 1 whereas 21% were infected with HCV genotype 3. The mean interval beetwen the two biopsies was 48 (32) months (range 10–176). Reasons for the absence of antiviral treatment in these patients were as follows: mild histological lesions (A=1 and F=1 according to the METAVIR scoring system) 50%; refusal 20%; repeatedly normal alanine aminotransferase (ALT) levels 12%; psychiatric contraindications 7%; heavy alcohol intake 6%; and miscallenous 5%.
Characteristics of the 96 patients according to the severity of steatosis at the time of the first biopsy
Steatosis at the time of the first liver biopsy and steatosis evolution
Steatosis was present in 51 of 96 patients on the first liver biopsy (53%). It was mild in 34% of patients, moderate in 10%, and severe in 9%. The characteristics of the 96 patients within each grade of steatosis are given in table 1. Patients with mild and moderate steatosis did not differ for most characteristics and thus were pooled for statistical analysis.
Severe steatosis was significantly associated with an increased BMI (p<0.05) and HCV genotype 3 (p=0.0004). Although an alcohol intake >40 g/day was more frequent in patients with severe steatosis (22% v 9%), the difference did not reach statistical significance. Worsening of steatosis was observed in 34% of patients, stabitity in 50%, and improvement in 16% (fig 1).

Evolution of hepatic histological activity, fibrosis (METAVIR score), and steatosis between the two biopsies in the 96 patients studied. Results are given as percentage of patients with improvement (defined as a decrease in histological activity, fibrosis, or steatosis grades of at least 1 between the two biopsies), stability (defined as identical histological activity, fibrosis, or steatosis grades between the two biopsies), and worsening (defined as an increase in histological activity, fibrosis, or steatosis grades of at least 1 between the two biopsies).
Characteristics of patients with worsening of steatosis
Characteristics of patients with worsening of steatosis according to the presence or absense of steatosis at diagnosis are shown in table 2. Steatosis appearence was significantly more frequent in patients without steatosis at diagnosis than worsening of steatosis in those with mild to moderate steatosis (53% v 24%, respectively; p<0.01). In patients without steatosis at diagnosis, steatosis appearence was significantly associated with fibrosis progression (p<0.03). In patients with mild to moderate steatosis at diagnosis, worsening of steatosis was significantly associated with fibrosis progression (p=0.03) and with infection with HCV genotype 3, with a relationship close to statistical significance (p=0.068).
Characteristics of patients with worsening of steatosis according to the presence or absense of steatosis at diagnosis*
Factors associated with fibrosis progression
During the study period, fibrosis progression was observed in 30% of patients, stability in 70%, and improvement in none, whereas worsening of activity was observed in 30% of patients, stability in 66%, and improvement in 4% (fig 1).
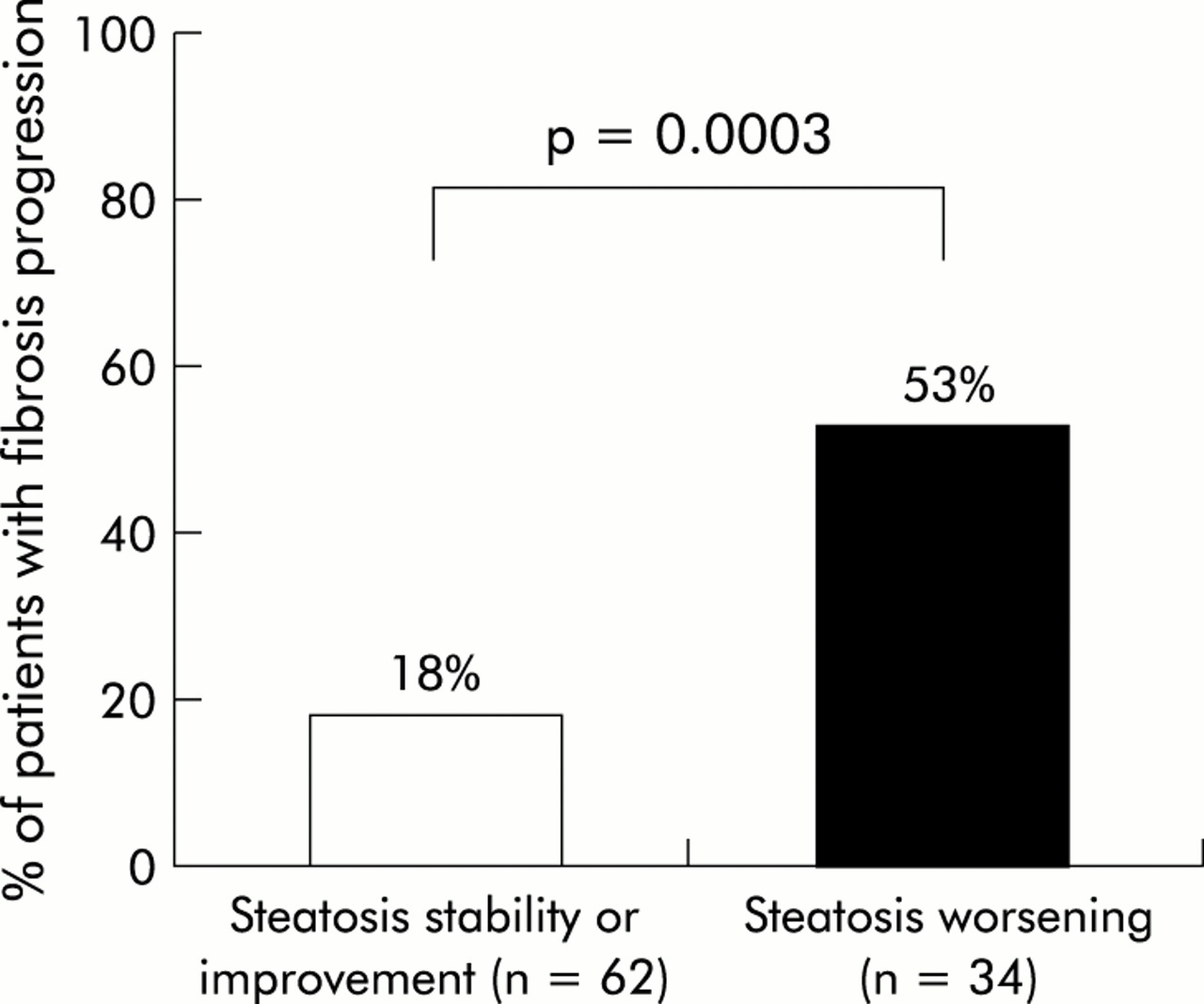
In a univariate analysis, factors associated with fibrosis progression were male sex (p=0.05), worsening of histological activity (p=0.04), and worsening of steatosis (p=0.0003). In a multivariate analysis, the only factor independently associated with fibrosis progression was worsening of steatosis between the two biopsies (worsening v improvement/stability: odds ratio 4.7 (95% confidence interval 1.3–10.8); p=0.0001). Overall, fibrosis progression was significantly more frequent in patients with worsening of steatosis than in those without worsening of steatosis (53% v 18%; p=0.0003) (fig 2).

{kind=link}
{kind=link}
Relationship between fibrosis progression and steatosis evolution between the two biopsies in the 96 patients studied. Worsening of steatosis was defined as an increase of at least one grade between the two biopsies; improvement or stability was defined as identical grades or a decrease of at least one grade between the two biopsies. Fibrosis progression was defined as an increase in fibrosis score of at least one between the two biopsies.
DISCUSSION
The spectrum of HCV related liver disease is broad and rates of fibrosis progression are extremely variable.1,2 Furthermore, the changing epidemiological pattern of HCV and the significant contribution of various cofactors to the outcome of HCV related liver disease also complicate the description of a general model for the natural history of hepatitis C.23 Studies on the natural outcome of hepatitis C have indeed shown conflicting results. On the one hand, studies based on 20–45 year follow up of large cohorts of transfusion or immunoglobulin infected patients suggested a globally slowly progressive disease, with low morbidity and mortality rates.24–26 On the other hand, studies of cohorts of patients with CHC seen in tertiary care and liver transplantation centres suggested more serious and often fatal outcomes.4,27–30 As recently suggested, estimates of disease progression are highly cohort dependent and influenced by specific risk factors and inherent selection bias.31 It is important to keep in mind that except in one study,30 the assessement of liver disease progression was not based on serial liver biopsies. Indeed, estimation of fibrosis progression is associated with pitfalls in the absence of repeated liver biopsies: firstly, the difficulty of finding valid controls in terms of spontaneous fibrosis progression rate; and secondly, the risk of variable fibrosis progression rates. In the present study, fibrosis progression was determined on paired liver biopsies in 96 untreated patients, carefully selected from a database of nearly 600 patients with CHC, by a single pathologist unaware of the demographic, clinical, or biological characteristics of the patients, using the METAVIR scoring system, a validated and reproducible score.21 To overcome the risk of variable fibrosis progression rates, we chose to study the percentage of patients with worsening, improvement, and no change in fibrosis stages between the two biopsies. In the present study, fibrosis progression was observed in approximately 30% of our patients over a mean period of four years, a rate consistent with previous reports.32,33 The availibity of paired liver biopsies gave us the opportunity to assess steatosis evolution over time, a parameter not studied to date.
The main finding of the present study was that worsening of steatosis was one of the factors associated with fibrosis progression (together with male sex and worsening of histological activity) in a univariate analysis and the only independent factor of fibrosis progression in a multivariate analysis. The mechanism of worsening of steatosis (which occurred in 34% of our patients) remains to be clarified. The role of HCV genotype 3 in the genesis of steatosis has been suggested recently.13,14,34 This was confirmed in the present study in which the proportion of patients infected with HCV genotype 3 was significantly higher in patients with severe steatosis at diagnosis (p=0.0004). Interestingly, in patients with steatosis at diagnosis, infection with HCV genotype 3 tended to be more frequent in those with worsening of steatosis than in those without (40% v 10%, respectively; p=0.068). These findings indicate a direct steatogenic effect of HCV, as supported recently by several lines of evidence: the development of progressive hepatic steatosis in transgenic mice expressing the HCV core gene12; the close relationship between intrahepatic HCV RNA and the development of steatosis35; and the correlation between hepatic steatosis and hepatic HCV replication in patients infected with HCV genotype 3.13
Worsening of steatosis was the only factor associated with fibrosis progression in our patients. Although we cannot exclude that worsening of steatosis occurs as a result of worsening of fibrosis, recent studies suggest, in contrast, that steatosis is a factor of fibrosis progression.14,19 The mechanism by which steatosis evolution could aggravate liver fibrosis remains hypothetical. It has been suggested that in the HCV infected liver, steatosis could contribute to fibrosis through a steatohepatitis-like pathway involving stellate cell activation and perisinusoidal fibrosis.15 Recent data indicate that in patients with non-alcoholic steatohepatitis, hepatic inflammation and fibrosis develop as a consequence of a two hit process, the first being steatosis and the second oxidative stress with subsequent lipid peroxidation.36 Indeed, it has been shown in the liver of patients with chronic HCV infection that steatosis correlates with lipid peroxidation37 and active fibrogenesis.38 An alternative explanation involves increased susceptibility of the fatty liver to the effects of the antiviral inflammatory response.15 Consistent with this hypothesis is the observation in the present study that worsening of histological activity tended to be more frequent in patients with worsening of steatosis.
Despite the association between worsening of steatosis and fibrosis progression, there was no significant association in our study between steatosis at diagnosis and fibrosis progression. These findings differ from those of Serfaty et al and Adinolfi and colleagues.14,19 Differences in patient selection and study design may explain these discrepancies. Indeed, it should be kept in mind that contrary to our study in which liver fibrosis progression was assessed using paired biopsies, fibrosis progression in the studies by Adinolfi et al and Serfaty et al was estimated indirectly on a single liver biopsy according to the model described by Poynard and colleagues.2
In conclusion, our results suggest that rather than steatosis at a given time, it is worsening of steatosis over time that is associated with progression of liver damage in patients with CHC. These findings may have important prognostic and therapeutic implications in the management of these patients. In this respect, particular efforts should be made to control factors associated with steatosis, namely excessive alcohol intake and excessive body weight, but also to favour indications of treatment in patients infected with HCV genotype 3, the newly identified steatogenic factor, which appears to be particularly sensitive to the present antiviral therapies.39,40