Article Text

Abstract
Background and aims: The γ-aminobutyric acid (GABAB) agonist baclofen has been shown to reduce reflux episodes during the first three postprandial hours in patients with gastro-oesophageal reflux disease (GORD) and in normal controls. The aim of the study was to assess the effect of acute (one day) and chronic (four weeks) administration of baclofen on 24 hour pH metry and symptoms in GORD patients and normal controls.
Patients and methods: Acute study: 28 patients with GORD with none or mild oesophagitis at endoscopy and 15 controls underwent oesophageal and gastric 48 hour pH metry in which baclofen or placebo was given for 24 hours in a double blinded manner. Chronic study: 16 GORD patients received baclofen (10 mg four times daily) or placebo for four weeks. Twenty four hour oesophageal pH metry and reflux symptom scores were evaluated before and at the end of treatment.
Results: Acute study: the number of reflux episodes and per cent time with pH <4 was significantly lower after baclofen in GORD patients and controls (p<0.003; p<0.0007). Gastric pH increased significantly in GORD patients and controls (p<0.001; p<0.05). Chronic study: four weeks after initial administration of baclofen, the number of reflux episodes and percentage of time with pH <4 significantly decreased in all GORD patients (p<0.003; p<0.02). Symptom scores significantly improved after treatment with baclofen (p<0.0007).
Conclusions: The GABAB agonist baclofen reduces 24 hour gastro-oesophageal reflux and increases gastric pH in GORD patients and controls. When given for one month to GORD patients, baclofen reduces oesophageal acid refluxes and significantly improves symptoms. Baclofen may be useful in the therapy of GORD.
- baclofen
- GABA
- gastro-oesophageal reflux
- GORD, gastro-oesophageal reflux disease
- GABA, γ-aminobutyric acid
- LOS, lower oesophageal sphincter
- TLOSR, transient lower oesophageal sphincter relaxations
Statistics from Altmetric.com
- GORD, gastro-oesophageal reflux disease
- GABA, γ-aminobutyric acid
- LOS, lower oesophageal sphincter
- TLOSR, transient lower oesophageal sphincter relaxations
GABA (γ-aminobutyric acid) is a potent inhibitory neurotransmitter in the central nervous system and antagonises the release of neurotransmitters from vagal nerve afferents through its GABAB receptor.1 GABAB receptors are present in the nucleus tractus solitarius and in the dorsal motor nucleus of the vagus, which are known as centres that integrate the afferent preganglionic signal arising from gastric tension mechanoreceptors2 and the lower oesophageal sphincter (LOS).3 Physiology and pharmacology studies in animals have shown that activation of GABA receptors with the GABAB agonist baclofen inhibits transient LOS relaxation, gastro-oesophageal reflux,4,5 and gastric secretion.6 In normal human subjects and in patients with gastro-oesophageal reflux disease (GORD), recent studies have shown that baclofen reduces the rate of transient lower oesophageal sphincter relaxations (TLOSR), the rate of gastro-oesophageal acid reflux episodes, and increases basal LOS pressure.7,8 Baclofen therefore has been proposed as potentially useful in the treatment of GORD. Studies with baclofen however have been limited to evaluation of a single oral dose on gastro- oesophageal acid reflux for a two hour postprandial period and more recently for 12 hours.9 Furthermore, as peak plasma levels of baclofen given orally occur two hours after administration, with disappearance from blood 4–6 hours thereafter,10 a study with multiple oral dosing is essential to obtain coverage of a 24 hour period that should be necessary to set up a therapeutic programme in patients with GORD. To date, there is no information on the effect of baclofen when administered in multiple doses over a 24 hour period either in normal subjects or GORD patients, or data on the effect of chronic administration of baclofen on 24 hour gastro-oesophageal acid reflux and symptoms in patients affected by GORD.
The aim of this study therefore was to assess the effects of the GABAB agonist baclofen on 24 hour oesophageal and gastric pH patterns in normal subjects and in patients with GORD. Moreover, we evaluated the effects of one month of treatment with baclofen versus placebo on the oesophageal pH pattern and symptoms in patients with GORD.
METHODS
The study was divided into two parts. The first was a placebo controlled randomised comparison of baclofen or placebo in patients with GORD and normal controls. The second was a placebo controlled randomized parallel group comparison of baclofen or placebo administered for four weeks in GORD patients.
Patient selection
Patients were aged 18 years or older, both males and females, and were chosen on the basis of clinical symptoms indicating GORD (heartburn, belching, and regurgitation) for at least three months before enrolment. In the week preceding the study, each patient underwent endoscopy to assess the presence and degree of oesophagitis and other gastroduodenal pathology. Patients with no signs of oesophagitis or only mild oesophagitis with erythema, hyperaemia, and/or friability with no visible macroscopic erosions were selected. Patients with oesophagitis grade 2–5, according to Hetzel and colleagues,11 oesophageal varices, active or previous history of gastric or duodenal ulcer or gastrointestinal bleeding, erosive gastritis, duodenitis, inflammatory bowel disease, or recent history of gastrointestinal cancer treatment were excluded. Patients were also ineligible if they had received therapeutic doses of proton pump inhibitors, aspirin, or non-steroidal anti-inflammatory drugs in the 30 days preceding the study. The number of antacid tablets consumed per week in the month preceding the study was also recorded.
A group of healthy subjects matched for age and sex to the GORD patients was studied as a control group.
Each subject gave written informed consent to participate and the protocol was approved by the ethics committee of G D’Annunzio University.
Data analysis
Oesophageal pH recording was analysed for the total number of acid reflux episodes and per cent time with pH <4 in the 24 hour observation period. The number of reflux episodes and per cent time pH <4 were also analysed every two hours. A reflux episode was considered as a drop in oesophageal pH below 4 until its return to a value of 4.2, lasting 10 seconds. GORD was diagnosed when the total number of reflux episodes in a 24 hour period was greater than 50, and/or per cent time with pH <4 was more than 5% in 24 hours.
Gastric pH was analysed as mean pH value every hour and as a total value in the 24 hour period.
Study protocol
First part
Each subject or patient admitted to the study underwent 48 hour oesophageal and gastric pH metry starting after an overnight fast at about 8 am. Patients and subjects were divided into two groups: in the first group, baclofen 10 mg was given orally at 10 am, 2 pm, 6 pm, and 10 pm in the first or second 24 hour period in a random manner. In the second group, placebo was administered instead of baclofen using the same schedule. This first or second 24 hour recording without baclofen or placebo was considered the basal period.
pH metric probes were kept anchored to the patient’s nose throughout the whole recording period to reduce to a minimum artefacts due to probe displacement. At the end of the recording, the probes were removed and data were transferred to a personal computer and analysed using a dedicated program (Scan, System; SME, Solothurn, Switzerland). pH metry was performed using two glass pH flexible probes with distal incorporated electrode (SME). The pH electrodes were calibrated in buffers of pH 7 and 4. Catheters were introduced nasally under fluoroscopy: one probe was positioned in the gastric body which has been shown to be an optimum position in conjunction with the fundus to record ambulatory gastric acidity,12 and the other one was placed 5 cm above the LOS which was manometrically identified two days prior to the study. The probes were taped firmly to the nose and connected to a portable data logger (Gastroscan II; SME). The data logger was carried in a shoulder bag, allowing continuous recording with a freely moving subject.
In each 24 hour period, starting 30 minutes after pH probe positioning, all subjects and patients ate similar meals with equivalent caloric content: breakfast (8 am) consisted of one croissant or two slices of toasted white bread and 200 ml whole milk at room temperature (360 kcal); lunch (12 am) consisted of 150 g pasta with tomato sauce, 100 g boiled chicken or veal, salad, one apple or peach, and 150 ml water (720 kcal); and supper (8 pm) consisted of 150 g fresh mozzarella cheese and boiled potatoes, beans, or carrots (490 kcal).
No drug that could modify gastric pH was allowed during the whole recording period.
Second part
GORD patients diagnosed following the clinical and oesophageal pH metry described above who did not participate in the first part of the study were assigned to receive four weeks of treatment with placebo or baclofen at a dose of 10 mg orally three times daily (10 am, 2 pm, and 6 pm) for the first week, and then 10 mg orally four times daily (10 am, 2 pm, 6 pm, and 10 pm) for the remaining three weeks in a random manner. Baclofen was given in increasing doses to avoid possible side effects. At the end of treatment, every patient underwent oesophageal 24 hour pH metry, as described in the first part of the study. pH metry was performed using a recorder different from that used in the first part of the study (pH-day2; MENFIS BioMedica srl, Bologna, Italy). With this recorder and its related software, reflux lasting longer than five minutes was also computed.
During the one month treatment period, patients were asked to report any side effects to the medical personnel who were available 24 hours a day.
The number of antacid tablets used per week was also monitored. Patients were requested to use antacid tablets only for the treatment of heartburn recurrence and were free to use any antacid tablet commonly available on the market, except during the period of pH recording.
Symptom assessment
Before and at the end of the treatment period, each patient completed a questionnaire related to the severity and frequency of symptoms in the four weeks preceding and during the study. Symptoms evaluated were: bitter taste, belching, fasting epigastric pain, postprandial epigastric pain, night-time heartburn, daytime heartburn, and acid regurgitation. The severity of each symptom was classified as none, mild (symptom easily tolerated and lasting a short time), moderate (symptom caused some discomfort and interfered with usual activities), severe (symptom caused much discomfort and interfered with usual activities), and disabling (symptoms unbearable and interfered considerably with usual activities), and was scored: 0=absent, 1=mild, 2=moderate, 3=severe, 4=disabling. The frequency of each symptom was evaluated on a 0–4 scale (0=absent, 1=once/month, 2=once/week, 3=3 times/week, 4=daily).
Statistics
Data from 24 hour pH metry were analysed using the Wilcoxon signed rank test for paired data and are presented as percentage decrease and exact values (median and interquartile range). All other data are presented as mean (SEM). The GORD symptom score was compared between the randomised groups at the beginning and after one month of treatment with baclofen or placebo using the Mann-Whitney U test. A p value of <0.05 was accepted as indicating statistical significance.
RESULTS
First part
Twenty eight GORD patients (15 men and 13 women, mean age 40 (8) years) and 15 control subjects (nine men and six women, mean age 43 (5) years) were evaluated using oesophageal and gastric pH measurement. These patients were included into the final evaluation. Fifteen GORD patients and nine controls received baclofen. Eight patients with GORD and four controls received baclofen in the first 24 hours of pH recording, and seven GORD and five controls received baclofen in the second 24 hour recording period. Thirteen GORD patients and six controls received placebo. Seven GORD patients and three controls received placebo in the first 24 hour period and six GORD patients and three controls received placebo in the second 24 hour period of recording. A summary of the protocol is described in fig 1.

Summary of the first part of the study. GORD, gastro-oesophageal reflux disease.
Analysis of the total number of acid reflux episodes and per cent time pH <4 in the oesophagus during the 24 hour period
In all patients with GORD and in controls during treatment with baclofen, there was a decrease in the number of reflux episodes (GORD: basal 149 (110–235), baclofen 73 (22–118) (−51.01%); controls: basal 42 (27–54), baclofen 18 (4–41) (−57.14%)) and in per cent time with pH <4, which was highly statistically significant (GORD: basal 6.4% (2.7–12.2), baclofen 2.7% (1.2–7.0) (−57.81%); controls: basal 1.5 (0.4–2.0), baclofen 0.6 (0.2–1.0) (−60%)) (fig 2). During placebo, no significant change was noted for number of reflux episodes (GORD: basal 271 (114–325), placebo 258 (124–346); controls: basal 41 (6–54), placebo 40 (16–54)) or per cent time pH <4 (GORD: basal 7.5% (3.7–12.4), placebo 6.6% (3.8–13.8); controls: basal 1.25% (0.2–2.9), placebo 1.75% (0.2–4.7)) (fig 2). It should be noted that in the placebo group, GORD patients showed a statistically significant greater average number of reflux episodes in comparison with GORD patients treated with baclofen (p<0.003).

Number of reflux episodes (A, C, E, G) and mean per cent of time with pH <4 (B, D, F, H) in the 24 hour basal period and during baclofen administration (10 mg four times daily) in 15 patients with gastro-oesophageal reflux disease (GORD) (A, B) and nine controls (C, D), and in the basal period and during placebo administration in 13 GORD patients (E, F) and six controls (G, H). Individual data for each patient and median and interquartile range are shown for the basal period and during baclofen or placebo treatment. ***p<0.001 versus basal.
Analysis of the number of reflux episodes and per cent time with pH <4 in the oesophagus every two hours
A general decrease in the number of reflux episodes and per cent time pH <4 was found with baclofen during daytime fasting and after eating. Specifically, with baclofen there was a significant reduction in the number of acid reflux episodes during the day between 12 and 2 pm, 2 and 4 pm, 4 and 6 pm, and 8 and 10 pm in controls and between 10 am and 12 pm, 2 and 4 pm, 6 and 8 pm, and 8 and 10 pm in GORD patients (fig 3).

Number of acid reflux episodes (A, C) and per cent time pH <4 (B, D) every two hours for a total of 24 hours during the basal period and after baclofen administration (10 mg four times daily) in 15 patients with gastro-oesophageal reflux disease (GORD) (A, B) and nine controls (C, D). Values are median and interquartile range. Arrows indicate the time of baclofen administration and M=meal. *p<0.05 versus basal.
Per cent time pH <4 in every two hour period was found to be significantly lower in controls between 12 and 2 pm, 2 and 4 pm, 6 and 8 pm, 8 and 10 pm, and 10 and 12 am, and in GORD patients between 10 am and 12.00 pm, 12 and 2 pm, 2 and 4 pm, 6 and 8 pm, and 10 pm and 12 am (fig 3). A statistically significant decrease in the number of reflux episodes and in per cent time with pH <4 was found with baclofen in the two hours after meals both in GORD and controls (fig 3). No changes were found with placebo (data not shown).
Analysis of mean pH in the stomach during the 24 hour period
GORD patients showed a statistically significant higher median gastric pH compared with control (controls: 2.02 (1.25–2.92); GORD: 3.15 (1.50–4.50); p<0.0001). A statistically significant increase in mean gastric pH value in the 24 hour period was noted with baclofen in nine control subjects and in 15 GORD patients (controls: basal 2.02 (1.25–2.92), baclofen 2.34 (1.31–3.72), p<0.002; GORD patients: basal 3.15 (1.50–4.50), baclofen 4.04 (2.31–5.52), p<0.0004). No change was noted with placebo (controls (six subjects): basal 2.59 (1.71–4.93), placebo 2.46 (1.91–4.78), NS; GORD (13 patients): basal 3.62 (1.62–5.07), placebo 3.34 (1.86–4.91), NS).
Analysis of the gastric pH curves every hour after baclofen and placebo showed similar behaviours, including the postprandial neutralisation reacidification phase, with greater values for baclofen that reached statistical significance one or two hours after meals (fig 4).

Gastric pH evaluated every hour (mean (SEM)) during the basal, placebo, and baclofen periods in patients with gastro-oesophageal reflux disease (GORD) (A) and in controls (B). Arrows indicate the time of baclofen administration and M=meal. *p<0.02 versus basal.
Second part
Analysis of the total number of acid reflux episodes and per cent time pH <4 in the oesophagus after one month of treatment with baclofen or placebo.
Eighteen GORD patients (eight males, 10 females, mean age 45 (5) years) were evaluated. Twelve received baclofen and six placebo. Two patients (one male and one female) in the baclofen group withdrew from the study because of side effects. In the remaining 10 GORD patients treated with baclofen, the number of reflux episodes and per cent time pH <4 was significantly decreased at the end of treatment in comparison with values reported at the beginning of treatment with baclofen (number of reflux episodes: basal 220 (160–266), baclofen 52 (33–77) (−76.36%); percentage of time pH <4: basal 5.8% (4.0–10.4), baclofen 2.7% (1.2–3.9) (−53.45%)). The median number of reflux episodes and per cent time with pH <4 in patients with GORD treated with placebo was not changed (number of reflux episodes: basal 118 (89–134), placebo 124 (90–180); per cent time pH <4: basal 6.5% (4.2–9.8), placebo 6.0% (4.0–10.9)) (fig 5).
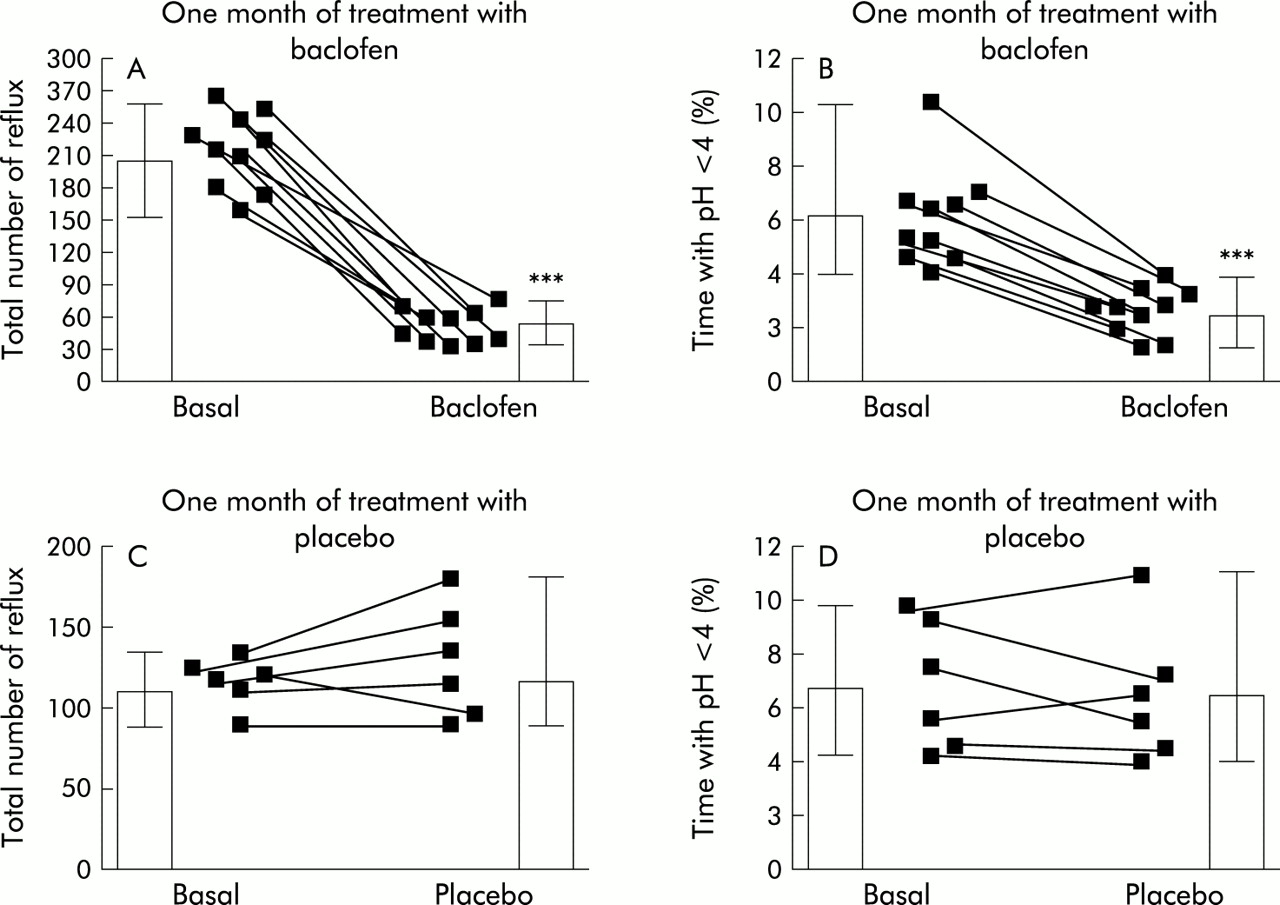
Number of reflux episodes (A, C) and per cent time pH <4 (B, D) before and after four weeks of treatment with baclofen (10 gastro-oesophageal reflux disease (GORD) patients) (A, B) or placebo (six GORD patients) (C, D). Individual data for each patient and median and interquartile range are shown for the periods before and after four weeks of treatment with baclofen or placebo. ***p<0.001 versus basal.
The number of reflux episodes longer than five minutes was assessed in five cases treated with baclofen and in three cases treated with placebo. With baclofen, a significant reduction was found (basal: 7 (4–11), baclofen 2 (1–4); p<0.002) while no change was noted with placebo (basal: 7 (3–8), placebo 8 (2–9); NS).
Symptoms and side effects
The intensity and frequency of symptoms were found to be significantly improved after treatment with baclofen in all patients, while with placebo the total symptom scores did not change (fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intensity (A, C) and frequency (B, D) of reflux symptoms (median and interquartile range) before and after four weeks of treatment with baclofen (10 mg four times daily) (A, B) in 10 gastro-oesophageal reflux disease (GORD) patients and with placebo (C, D) in six GORD patients. *p<0.05.
The number of antacid tablets consumed was 7 (2) per week before placebo, 8 (2) per week during placebo (NS), 8 (1) per week before baclofen, and 2 (1) per week during baclofen (p<0.01).
Two patients withdrew from the study after 10 days of treatment with baclofen, one because of low blood pressure (90/80 mm Hg) with dizziness, and the other due to nocturnal anxiety with sleepiness. The drug was well tolerated in all other patients.
DISCUSSION
We have shown that the oral GABAB agonist baclofen, in comparison with placebo, reduced the total number of acid reflux episodes and per cent time pH was <4 in the oesophagus during a 24 hour period when given in multiple doses over 24 hours, and caused an increase in mean gastric pH value in patients with GORD and in normal controls. In patients with GORD, baclofen given for four weeks reduced oesophageal acid reflux and significantly improved reflux symptoms.
Current pharmacological treatment of GORD is based on acid suppression with anti-H2 receptor antagonists or proton pump inhibitors, or both.13 Drugs that have less activity on acid secretion have also been evaluated with various results. Prokinetic agents such as cisapride have been shown to reduce meal induced reflux symptoms14 but use has been limited due to serious side effects.15 Dicyclomine, a peripheral anticholinergic agent, induces a decrease in the number of reflux episodes only in the first postprandial hour,16 hyoscine N- butylbromide, a peripheral anticholinergic agent, in contrast increases the number of reflux episodes,17 while pirenzepine, a muscarinic subtype 1 receptor antagonist, appears to be no better than placebo.18 Atropine seems to produce a favourable effect on reflux when administered before a meal, with a significant reduction in the postprandial number of refluxes.19,20 Atropine however is available only for intravenous or intramuscular use, and cannot be used for prolonged periods due to various side effects.
Baclofen, a GABAB receptor agonist, is already available for therapeutic purposes in gastroenterology and other branches of internal medicine. Lidums and colleagues7 have demonstrated that baclofen 40 mg in a single dose caused a reduction in the total number of gastro-oesophageal acid reflux episodes in normal subjects and related this effect to the ability of the drug to inhibit TLOSR and to induce a slight increase in basal LOS pressure. More recently, Zhang and colleagues8 and Cange and colleagues9 in a similar study in patients with GORD reported inhibition of postprandial gastro-oesophageal acid reflux with a maximum effect within a period of four hours after a single dose of baclofen 40 mg, while data presented in our study showed that inhibition of gastro-oesophageal acid reflux may be extended to 24 hours providing that the same dose of baclofen is given in four separate administrations of 10 mg each at four hour intervals. It must be noted however that while in the acute studies baclofen was equally effective in patients with oesophagitis or hiatal hernia, so far a beneficial effect after prolonged administration has been shown only in a selected population of GORD patients with mild or no signs of oesophagitis.
The reduction in gastro-oesophageal acid reflux after baclofen in patients and normal subjects suggests that the drug modifies a physiological mechanism responsible for gastro- oesophageal acid reflux. This probably involves TLOSR more than other mechanisms as TLOSR are present both in normal subjects and in GORD patients, with the difference that in GORD patients the number of TLOSR may be increased compared with normal controls21 or that, when TLOSR occur in GORD, they are more likely to be associated with reflux.22
Baclofen may also decrease gastro-oesophageal acid reflux through an inhibitory effect on gastric pH. In the present study, baclofen induced an increase in gastric pH before and after a meal compared with placebo, with peak values greater than 5.0 recorded in GORD patients one to two hours postprandially. The postprandial neutralisation-reacidification curve also showed a similar slope for placebo and baclofen, with higher values of pH for the latter, suggesting a direct effect on gastric hydrochloric acid production for baclofen rather than an indirect effect on gastric motility. To date, there are no studies in humans in this area and animal studies do not help to clarify this hypothesis as they describe a generic dual inhibitory and stimulatory effect of baclofen on gastric secretion6,23,24 and an increase in gastric tone and amplitude of contractions.25
The reduction in the number of gastro-oesophageal acid reflux episodes was approximately 51% in GORD patients and 57% in controls after the first 24 hours of treatment with baclofen. This value increased to approximately 76% after four weeks of treatment in GORD patients, suggesting there is no tachyphylaxia but most importantly that there is a strengthening of the effect. This may be due to an increase in plasma levels of the drug during treatment. Pharmacokinetic studies in patients with multiple sclerosis and spinal cord injury treated with a stable dosing regimen of baclofen at a higher dosage (80–300 mg/day for up to 16 weeks) than that used in the present study showed that baclofen caused blood levels to rise gradually over time, probably as a result of impaired renal clearance.26 These data may explain why the effect noted after four weeks of therapy was greater than that shown after the one day treatment and indicate that more studies are necessary on renal function and on plasma levels of the drug when chronically administered to GORD patients.
All GORD symptoms significantly improved after one month of treatment with baclofen in all patient treated. The number of antacid tablets taken for heartburn recurrence was also significantly reduced during baclofen therapy from 8 to 2 per week. Although we did not report a daily or weekly score of symptoms, patients reported a beneficial effect a few days after the start of treatment. This rapid improvement may be explained by the fact that baclofen is effective in reducing gastro-oesophageal acid reflux immediately after its first administration, as shown in the first part of this study.
Side effects were not reported in our patients, except for two who interrupted their participation because of low blood pressure and nocturnal anxiety that were assumed to be due to baclofen. Baclofen has been reported to be a well tolerated drug and severe side effects have been reported at higher dosages in patients treated for periods much longer than those used in the present study.27
In summary, in the present study the GABAB agonist baclofen in multiple doses reduced gastro-oesophageal acid reflux for a 24 hour period in terms of the number and period of acid exposure in the oesophagus in both normal subjects and in patients with GORD without or with only mild oesophagitis. The improvement in reflux parameters and of symptoms related to gastro-oesophageal reflux in patients with GORD treated for four weeks with baclofen suggest a potential therapeutic role for this drug in the treatment of gastro-oesophageal reflux disease.
Acknowledgments
The authors thank Dr Samuela Bartolacci for help in collecting data and Catherine Di Placido for reviewing the English style of the manuscript. Preliminary data from this study were presented as an oral presentation at the 102nd Annual Meeting of the American Gastroenterological Association, May 20–23, 2001, Atlanta, and were published in abstract form in Gastroenterology 2001;120:A34.