Article Text

Abstract
Background: Inflammatory bowel disease (IBD) is known to be associated with reduced bone density but the extent to which this results in an increased risk of fracture and the contribution of corticosteroid therapy are unclear. We have conducted a large cohort study to address these issues.
Methods: We selected subjects within the General Practice Research Database (GPRD) with a diagnosis of IBD and up to five matched controls for each patient. We derived dates of recorded hip fractures and also information on smoking, use of corticosteroids, and a number of other drugs. We calculated the absolute risk of fracture and the relative risk as a hazard ratio corrected for available confounders by Cox regression.
Results: Seventy two hip fractures were recorded in 16 550 IBD cases and 223 in 82 917 controls. Cox modelling gave an unadjusted relative risk of hip fracture of 1.62 (95% confidence interval (CI) 1.24–2.11) for all IBD, 1.49 (1.04–2.15) for ulcerative colitis (UC) and 2.08 (1.36–3.18) for Crohn’s disease (CD). Multivariate modelling showed that both current and cumulative use of corticosteroids and use of opioid analgesics confounded this relationship. After adjusting for confounding, the relative risk was 1.41 (0.94–2.11) for UC and 1.68 (1.01–2.78) for CD.
Conclusion: The risk of hip fracture is increased approximately 60% in IBD patients. Corticosteroid use is a contributor to this, both in the long term as previously recognised and also in an acute reversible manner. The majority of hip fracture risk in IBD patients however cannot be attributed to steroid use.
- corticosteroids
- fracture
- inflammatory bowel disease
- GPRD, General Practice Research Database
- UC, ulcerative colitis
- CD, Crohn’s disease
- IBD, inflammatory bowel disease
- HRT, hormone replacement therapy
- BMI, body mass index
Statistics from Altmetric.com
- GPRD, General Practice Research Database
- UC, ulcerative colitis
- CD, Crohn’s disease
- IBD, inflammatory bowel disease
- HRT, hormone replacement therapy
- BMI, body mass index
Although many studies have shown that patients with inflammatory bowel disease (IBD) are at increased risk of osteoporosis,1–5 there are relatively few data on the extent of the increased risk of fracture in these patients relative to the general population. A small number of case series have suggested high levels of osteoporotic fracture67 but data from the available controlled studies are inconsistent, with one study showing a rise in fracture risk both for ulcerative colitis (UC) and Crohn’s disease (CD),8 two an increase in risk in CD but not in UC,910 and one no increase in risk in either.11 As corticosteroids are a risk factor for osteoporosis,12 and are widely used in IBD, they may explain the associated osteoporosis. However, the size of the contribution from corticosteroids is unclear.113–16
Of the controlled studies of fractures to date, only one addressed the role of corticosteroid use,9 and in this study the use of corticosteroids was a risk factor for fracture in CD but not in UC. However, important limitations of this study included the use of retrospective data derived from questionnaires and examination of only cumulative duration of steroid use, which might underestimate the role of these drugs if, as has recently been suggested, their effect is reversible.17
To address these issues we carried out a cohort study examining both current and cumulative corticosteroid use and the risk of hip fracture in patients with IBD using prospectively gathered data.
METHODS
The General Practice Research Database (GPRD) is the world’s largest longitudinal primary care database and contains approximately 50 million patient years of data. The data reflect the observations, diagnoses made by, and therapies prescribed by, general practitioners, as well as information communicated to them by hospitals, collected in routine clinical practice by contributing computerised UK general practices since 1987. To ensure data quality, contributing practices received data quality training and are audited to ensure that at least 95% of prescribing and morbidity events are included.18 The validity of diagnoses of IBD within this dataset has been specifically assessed19 and 92% of diagnoses recorded were found to be accurate (the diagnoses of CD (94% accurate) and UC (93% accurate) were noted to be more reliable than those for indeterminate IBD (80% accurate)). Our IBD cohort was defined in the GPRD from the start of the database until December 2001, and comprised all patients within the GPRD with at least one prospectively recorded event coded as relating to IBD. A general population (control) cohort consisted of up to five (if available) age, sex, and practice matched controls who had no record of IBD themselves, and were alive and contributing data on the date of the case’s first prospective record of IBD.
IBD type was classified based on Oxmis and Read coding. Subjects were classified as having indeterminate IBD if they had codes for both UC and CD, as having UC if codes both for non-specific IBD and UC were present, and as having CD if codes for both CD and non-specific IBD were found. Subjects with a diagnosis of IBD first coded at least one year after collection of their prospective data in the GPRD began were considered to be incident cases. For each subject we used a combination of Oxmis and Read coding to assess whether they had experienced a hip fracture and when this had occurred. For each individual, only the first recorded hip fracture was considered. We then extracted data on smoking habits, body mass index (BMI), age at entry to the study, sex, use of systemic corticosteroids and of a number of other drugs, and frequency of falls. Smoking status was classified based on the coding within the dataset as unknown, never a smoker, ex-smoker, or current smoker. Subjects who appeared in more than one of these categories at different times were coded in the category suggesting greatest smoking experience. Height and weight were coded as the median recorded level for each subject, and BMI was calculated only for adults.
All prescriptions for systemic corticosteroids (excluding topical and inhaled use) were extracted, and based on their dates, a subject’s time within the study was divided into that during which the subject was considered a current user (within 90 days of a corticosteroid prescription) and that when they were not. (This can be thought of as modelling a reversible component of the risk of corticosteroid use.) For each of these time periods, the incremental total corticosteroid use (as number of prescriptions to that point in time) was calculated. (This can be similarly thought of as modelling an irreversible risk due to corticosteroid use.) The use of other drugs was coded as prescriptions occurring never, less than once a year, or more than once a year: falls were coded in a similar manner, based on the frequency of diagnostic/symptom coding for falls.
Statistical analysis
Univariate analysis of hip fractures using the matched cohort design was conducted by the production of crude fracture rates. Multivariate analyses were conducted using a Cox regression model, and the validity of the assumption of proportional hazards was assessed using log log plots and Stata’s own diagnostic test. As age and sex are known to be associated with both the risk of IBD and the risk of hip fracture, they were included within our models on an a priori basis. Other potential confounding factors added to this base model were retained only if they resulted in a 10% or greater change in the hazard ratio for IBD. For blood pressure and smoking, the confounding variable was included in the analysis as a categorical variable with a category representing missing data. Although low BMI is known to be associated with fracture risk and is related to IBD, it was not considered as a confounder as it is likely to be on the causal pathway between IBD and fracture risk and hence to do so would be inappropriate. The multivariate analyses were repeated stratifying for disease. Tests for interaction between identified risk factors were carried out. In addition, restriction analyses were carried out to examine the risks among those who were incident cases of IBD.
All analyses were conducted using Stata version 7 (Stata Corporation, College Station, Texas, USA).
RESULTS
In total, our study included 16 550 patients with IBD and 82 917 appropriately matched controls. Within the IBD cohort, 5960 patients had CD, 8301 had UC, and 2289 had indeterminate IBD. Of these, 2336 CD cases, 3518 UC cases, and 1351 indeterminate cases were incident. The average age at entry to the study was 46 years for both IBD cases and controls, and 46% of each cohort were males. The IBD cohort were more likely to have a BMI <25 (36% v 29%). With respect to smoking, the relationship varied between IBD types, with smoking being more common among CD cases compared with the control cohort (28% smokers v 21% of their matched controls) and less common among UC cases (12% v 20%); indeterminate cases had intermediate levels of smoking (22% versus 21%). These results are summarised in table 1.
Age, sex, body mass index (BMI), and smoking in cases and controls by disease group
Table 2 shows the use of corticosteroids, opioid analgesics, hormone replacement therapy (HRT), bisphosphonates, and calcium and vitamin D supplements in IBD patients and controls, both overall and by disease type. Corticosteroid and opioid use was more common among all groups of IBD patients compared with controls. Few subjects received HRT, bisphosphonates, or calcium and vitamin D supplements, and this remained true among those experiencing a hip fracture. Of these, only 27 (9%) of 295 received one or more of these medications at any time.
Use of selected drugs in cases and controls by disease group. All counts are of numbers of unique prescriptions
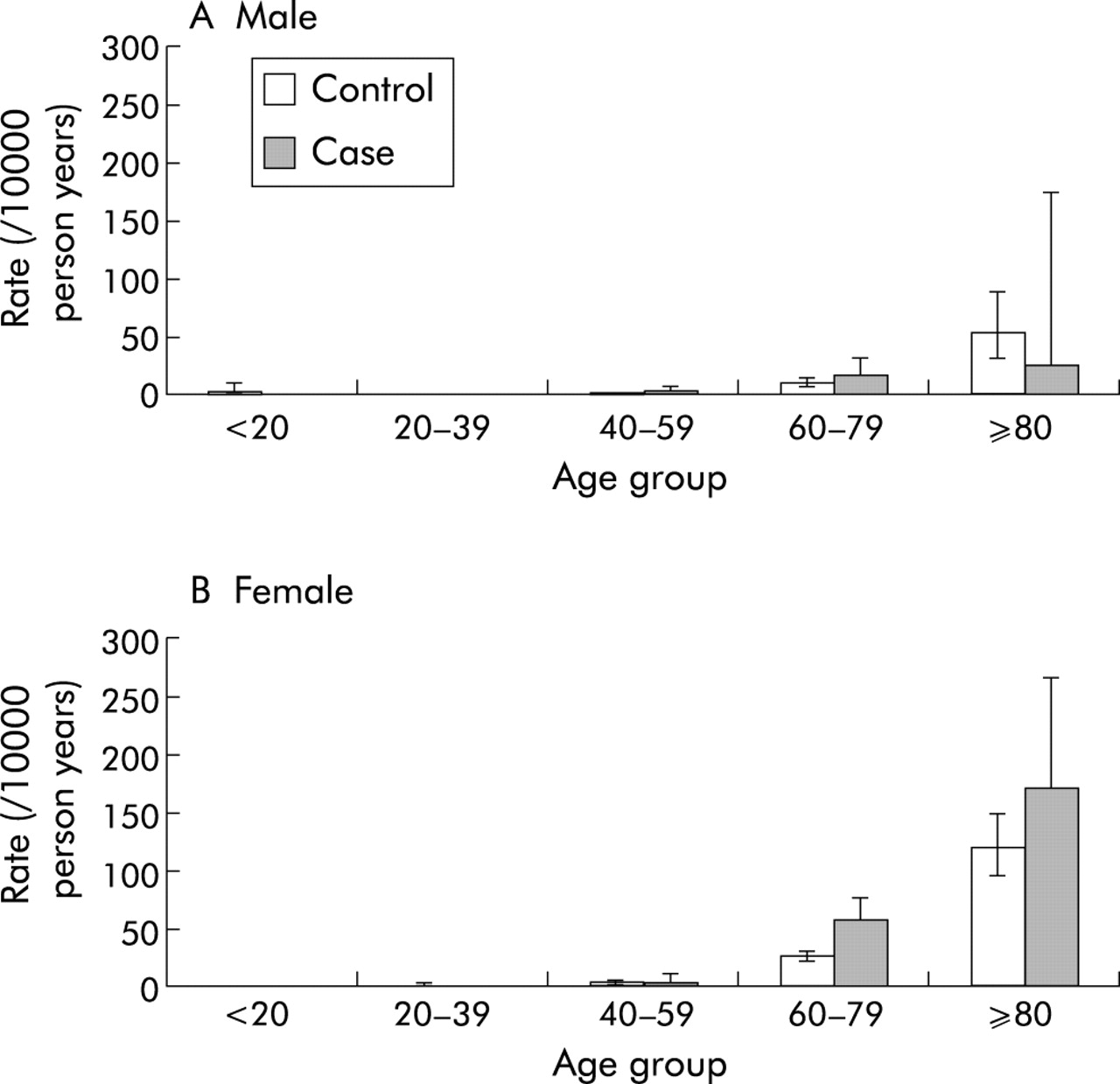
The IBD cohort contributed 61 130 years of follow up and 72 hip fractures, and controls 306 082 years of follow up and 223 hip fractures. These corresponded to crude hip fracture rates of 11.8 per 10 000 person years for cases and 7.3 per 10 000 patient years for controls. A breakdown of hip fractures, follow up available, and crude rates by disease type and sex are given in table 3 and by age and sex in fig 1. Expressing these results as hazard ratios via a univariate Cox regression model showed hazard ratios of 1.62 (95% confidence interval (CI) 1.24–2.11) for all IBD, 1.49 (95% CI 1.04–2.15) for UC, 2.08 (95% CI 1.36–3.18) for CD, and 0.85 (95% CI 0.30–2.47) for indeterminate IBD compared with their respective controls.
Absolute hip fracture rate by sex and disease group
{kind=link}
Hip fracture rated per 10 000 person years in males (A) and females (B), by age group.
In the multivariate Cox regression analysis, we included age at entry to the study and sex as confounders on an a priori basis. There was evidence of appreciable confounding in multivariate analyses by both current and cumulative corticosteroid use, and by opioid use, but not by smoking or by any other drug exposure we examined. The results of the multivariate analysis are presented in table 4. Overall, we found a hazard ratio for hip fracture among subjects with IBD of 1.42 (95% CI 1.05–1.91) when corrected for age, sex, corticosteroid use (both current and cumulative), and opioid use. Subdividing IBD cases by disease type showed that after correction for confounding, the hazard ratio remained greater for CD at 1.68 (95% CI 1.01–2.78) than for UC (1.41 (95% CI 0.94–2.11)). There was no statistically significant evidence of interaction between the effects of sex, age, corticosteroid, or opioid use and IBD.
Multivariate model of hip fracture risk corrected for age, sex, current steroid use, cumulative steroid use, and opioid use
When limited to incident cases, the hazard ratio for IBD in the multivariate model was reduced to 1.30 (95% CI 0.84–2.03). However, an analysis limited to those among the incident group with no record of systemic corticosteroid use but corrected for the other elements of the model showed a hazard ratio of 1.80 (95% CI 1.06–3.08).
DISCUSSION
We have shown in this general population based cohort study that the rate of hip fracture among patients with IBD was approximately 60% higher than that of their matched controls. This was greater in CD in which there was a twofold increase in risk compared with UC (1.5-fold). These findings are in contrast with the only previous European cohort study which reported only a non-significant excess of approximately 10% for both diseases,10 but are not dissimilar from those reported by a large North American study which found a 47% excess in CD patients and a 69% excess in UC patients.8 In multivariate analyses, these relative risks were reduced by correction for age, sex, current steroid use, cumulative steroid use, and opioid use. After correction for these factors, an increase in risk of 42% for IBD overall, 41% for UC, and 68% for CD remained. Within our multivariate model, current use of steroids was associated with a reversible 35% increase in the risk of hip fracture, and the receipt of, on average, one or more prescriptions for opioid analgesics each year with a 67% increase in risk. Irrespective of all of the other factors, hip fracture in our study remained very rare in those less than 60 years of age among both those with and without IBD, and even over the age of 60 years was far more common among females.
In this analysis, we looked only at the risk of hip fracture for two reasons. Firstly, this is a suitable outcome to study when attempting to assess the impact of osteoporosis on the health of IBD patients as hip fracture is clearly related to osteoporosis and is associated with significant morbidity and mortality. Secondly, as hip fractures generally results in hospitalisation and correspondence, the data are less susceptible to ascertainment bias which may occur with other fracture types if (as for both BMI and smoking behaviour) their recording were more complete for the IBD cohort than for healthy controls. It is possible that some fractures go unrecorded, and also that some diagnoses of fractures or of IBD may be in error. Such error would be likely to be random and hence lead to an underestimate in the risk we have shown, but is unlikely to be a major problem as both hip fracture recording20 and IBD diagnosis19 within the GPRD have been independently validated and found to be accurate in over 90% of cases. One disadvantage of the choice of hip fracture is that as this is a fracture predominantly of the elderly and IBD has its peak incidence in young adulthood, there is potential for the disease or its therapy to have a predisposing effect prior to the period observed.
Our finding that corticosteroid use was a confounder of the increased hip fracture risk is consistent with previous studies. Corticosteroids are commonly used to treat IBD, and are known to be associated with an increased risk of fracture.21 Furthermore, corticosteroids have previously been shown repeatedly to be confounders of the association with osteoporosis in IBD3–522 and, in the only previous study to examine their role in it, of fracture risk in IBD.9 This study however was reliant on a self administered questionnaire for data relating to steroid use, which introduced the potential for recall bias. Our study, by using prospectively gathered prescription data, avoided this problem. We were also able to examine not only the effect of cumulative use as was previously attempted but also the effect of current use, which has recently been suggested as an important risk factor for fracture17 and previously been shown to predict reduced bone density in CD.22 That there was significant risk associated with IBD after correction for available confounders, including corticosteroids, suggests however that they do not account entirely for the risk. Our findings suggest that steroid use accounts for less than half of the excess fracture risk in CD and less than 20% of that in UC.
It is important to recognise the limitations to precise estimation of steroid exposure in our subjects. For the nearly 60% who were prevalent cases, the GPRD will not have captured exposure prior to entry into the database. In addition, some exposure to steroids will be prescribed by hospitals and therefore not captured. It is for this reason that our estimates of cumulative exposure are in broad categories, allocation to which should remain valid despite these limitations. The imprecision of our estimates of cumulative steroid use however implies that it is possible that there was residual confounding from them, and that hence we may have underestimated the role of corticosteroids. Subgroup analyses of all incident cases, and of incident cases with no record of steroid use, allowed us to some extent to assess the importance of these limitations. Although these analyses are inevitably of very limited power, that they showed increased risk in groups free from these problems suggests that their impact may not be great. These findings are consistent with the previous observation that CD patients have reduced bone mineral density at diagnosis.13
Although we found that hip fracture was associated with both current and cumulative corticosteroid use in IBD, this does not prove that corticosteroids cause the increased risk. It is equally possible that corticosteroid use is a marker of increased inflammatory activity (as they will be given when such activity occurs) and that this directly affects bone metabolism.23 A further possibility is that the risk, at least in CD, is related to bowel malfunction, and the recent finding of a similar excess of hip fracture risk in patients with coeliac disease24 may support this.
Our other important findings were an increased risk of hip fracture in IBD patients using opioids regularly, which confounds the risk associated with IBD, and a low rate of use of bone protecting medications. As an excess risk of fracture in opioid users has previously been shown,25 and there is evidence to suggest that dependence on them is not rare in IBD,26 it is not surprising that they should be confounders in this context. It is perhaps no more surprising since the prevention of osteoporosis has only relatively recently gained prominence in the literature that we found little use of medications aimed at doing so in this dataset collected between 1987 and 2001. This finding does however highlight the opportunity for prevention that may be present.
In conclusion, we found that IBD was associated with an approximate 60% increase in the risk of hip fracture. We also found that although corticosteroids may explain some of this risk, they cannot explain all of it, and probably explain rather less than half of it, even in CD where they have their greatest effect. The finding that corticosteroids have an effect not only through prolonged consumption but also a rapid and reversible effect supports the suggestion that prophylactic therapy should be initiated acutely with corticosteroids.2728 Finally, our findings suggest that although the majority of the excess hip fracture risk in IBD may not be due to drug use, there is an opportunity to reduce this risk by reducing the use of opiates and increasing the use of prophylactic medication.
Acknowledgments
Dr Card is supported by a Wellcome Research Training Fellowship in Clinical Epidemiology (No 060529). This work was also supported by a project grant from the National Association for Colitis and Crohn’s Disease (NACC).