Article Text

Abstract
Background: Many patients with primary biliary cirrhosis (PBC) are asymptomatic at the time of diagnosis. However, because most studies of asymptomatic PBC have been small and from tertiary centres, asymptomatic PBC remains poorly characterised.
Aims: To describe the features and progression of initially asymptomatic PBC patients.
Methods: Follow up by interview and note review of a large geographically and temporally defined cohort of patients with PBC, collected by multiple methods.
Results: Of a total of 770 patients, 469 (61%) were asymptomatic at diagnosis. These patients had biochemically and histologically less advanced disease than initially symptomatic patients. Median survival was similar in both groups (9.6 v 8.0 years, respectively) possibly due to excess of non-liver related deaths in asymptomatic patients (31% v 57% of deaths related to liver disease). Survival in initially asymptomatic patients was not affected by subsequent symptom development. By the end of follow up, 20% of initially asymptomatic patients had died of liver disease or required liver transplantation. The majority of initially asymptomatic patients developed symptoms of liver disease if they were followed up for long enough (Kaplan-Meier estimate of proportion developing symptoms: 50% after five years, 95% after 20 years). However, 45% of patients remained asymptomatic at the time of death.
Conclusions: Although asymptomatic PBC is less severe at diagnosis than symptomatic disease, it is not associated with a better prognosis, possibly due to an increase in non-hepatic deaths. The reasons for this are unclear but may reflect confounding by other risk factors or surveillance bias. These findings have important implications for future treatment strategies.
- primary biliary cirrhosis
- asymptomatic
- symptom progression
- prognosis
- PBC, primary biliary cirrhosis
- AMA, antimitochondrial antibodies
- UDCA, ursodeoxycholic acid
- SMR, standardised mortality ratio
Statistics from Altmetric.com
- PBC, primary biliary cirrhosis
- AMA, antimitochondrial antibodies
- UDCA, ursodeoxycholic acid
- SMR, standardised mortality ratio
Recent estimates suggest that there are 12 000–15 000 patients with primary biliary cirrhosis (PBC) in the UK 1 and 40 000 in the USA.2 PBC was initially described as a universally severe condition, presenting with pruritus and jaundice and usually progressing rapidly to liver failure in less than three years.3–5 The discovery of antimitochondrial antibodies (AMA),6 and their subsequent inclusion in “routine” autoantibody profiles, has led to PBC being diagnosed more frequently and often at an earlier stage in the disease process. Fox et al were the first to describe PBC presenting with no symptoms attributable to liver disease (“asymptomatic PBC”) in 1973.7 Subsequent studies redefined the spectrum of disease phenotypes to include a high proportion of such asymptomatic patients.8–10 However, the clinical course, particularly with respect to prognosis and symptom development, of asymptomatic PBC remains relatively poorly described with case series being small (less than 91 initially asymptomatic patients) and largely based in tertiary referral centres.7–20
By the early 1990s, the consensus of case series of initially asymptomatic patients was that: (i) after about six years, two thirds of initially asymptomatic patients would develop symptoms; (ii) once symptoms developed, prognosis was as for the generality of PBC patients; and (iii) overall mortality in initially asymptomatic patients was higher than age matched populations but only after 10 or more years, and lower than in initially symptomatic patients.
As up to 60% of PBC patients are now asymptomatic at diagnosis, it is timely to re-examine the outcome of asymptomatic PBC in a large unselected cohort of patients to gain a clearer idea of its true early natural history. This has become particularly important in helping to make treatment decisions and to inform the debate about the need to treat patients with, for example, ursodeoxycholic acid (UDCA) while they remain asymptomatic of their liver disease.21 We have recently examined the overall natural history of an established unselected cohort of 770 patients, defined between 1987 and 1994.22 However, we presented little specific data in respect of the 469 patients who were asymptomatic of liver disease at diagnosis. The present report examines the clinical features, symptom progression, and outcomes in these initially asymptomatic patients.
METHODS
The methods used to identify the Northeast England cohort of patients with PBC have previously been described.1 This cohort included all incident and prevalent cases of definite or probable PBC alive between 1 January 1987 and 31 December 1994 within a geographically defined area of Northeast England. Multiple case finding methods were employed to ensure completeness of the cohort.
Definite PBC was defined as all three of: abnormal liver function tests, positive AMA, and compatible liver histology. Probable PBC was defined as any two of these. Data here includes both probable and definite disease. Date of diagnosis was defined as the first date when two of these diagnostic criteria were found to be present.
Patients were defined as initially asymptomatic if they did not have symptoms attributable to their liver disease at the date of diagnosis. The presence of symptoms at diagnosis was determined from medical records and by initial interview of patients by the investigators. Symptoms of PBC were defined as pruritus, persistent fatigue (lasting greater than three months in the absence of other identifiable causes such as anaemia or hypothyroidism), persistent right hypochondrial pain in the absence of another cause such as cholelithiasis, overt jaundice, bleeding oesophageal varices, ascites, or hepatic encephalopathy. Liver failure was defined as any of the last three symptoms.
Patients were followed up by regular interview and by examination of their medical records until 1 January 2000 or death. Deaths were defined as being “liver related” after review of the notes if they were related to a complication of liver disease (including hepatocellular carcinoma). Patient deaths were noted by examination of all clinical records and by logging all patient details with the Office of National Statistics.
Results were analysed using χ2 and Mann-Whitney U tests. Survival data were analysed by the Kaplan-Meier method and Cox proportional hazards regression. Survival times were adjusted in the Cox proportional hazards regression to take account of the presence of cases that were prevalent at the outset of the study using the methods described by Kieding.23 The presence of these cases could otherwise introduce bias into survival estimates as the survival times of prevalent cases are positively biased compared with those in the underlying population. The database complied with data protection legislation and local ethics committees approved this study.
Liver function tests were reported as the ratio of the test result to the upper limit of normal for the laboratory performing the test to account for tests being undertaken in multiple hospitals with differing normal ranges and units of measurement. For survival data, patient information was censored at 1 January 2000 for living patients. For symptom data, patient information was censored at the last clinic visit where symptoms may have been recorded, or death if the patient remained asymptomatic from their liver disease at this point. The records of patients who underwent liver transplantation were censored at the time of surgery. Indirect standardised mortality ratios (SMRs) were calculated at 1 January 1999 (the last date for which regional population data were available). SMRs were calculated using five year age-sex bands. General population data were obtained from mortality statistics for the Northern Regional Health Authority (which very largely corresponds to the study area). Indirect standardisation (as compared with direct) avoids large error in estimates due to very small numbers of deaths observed in individual bands, but means that individual SMRs cannot be compared with each other.
RESULTS
Of 770 patients with PBC (472 definite, 298 probable) in the Northeast England cohort, 469 were asymptomatic from PBC at the time of diagnosis (60.9% (95% confidence interval 57.4–64.4%)).
Data to allow calculation of survival corrected for the effect of prevalent cases were available for 765 patients (99%). Initial interview to determine symptoms at the time of diagnosis was possible for 354 of 469 (75%) initially asymptomatic patients. Initial medical record review was possible for all patients. Full clinical symptom follow up data by interview and regular case note review were possible for 422 (90%) initially asymptomatic patients.
Median follow up for mortality data was 7.4 years (range 0–28). Median follow up for symptom data was 7.3 years (range 0–28).
The clinical features of initially asymptomatic patients are shown in table 1. Median age at diagnosis was similar in initially asymptomatic and symptomatic patients (63.1 v 61.8 years). A total of 260 (55.4%) asymptomatic patients were aged less than 65 years at the time of diagnosis. The severity of PBC, whether assessed through serum liver function tests or liver histology, was milder in patients with initially asymptomatic disease than initially symptomatic patients. However, relatively few patients in either group had markedly abnormal liver function tests at diagnosis (proportion of patients with bilirubin greater than twice the upper limit of normal, 8% asymptomatic v 17% symptomatic).
Features at diagnosis of asymptomatic and asymptomatic patients
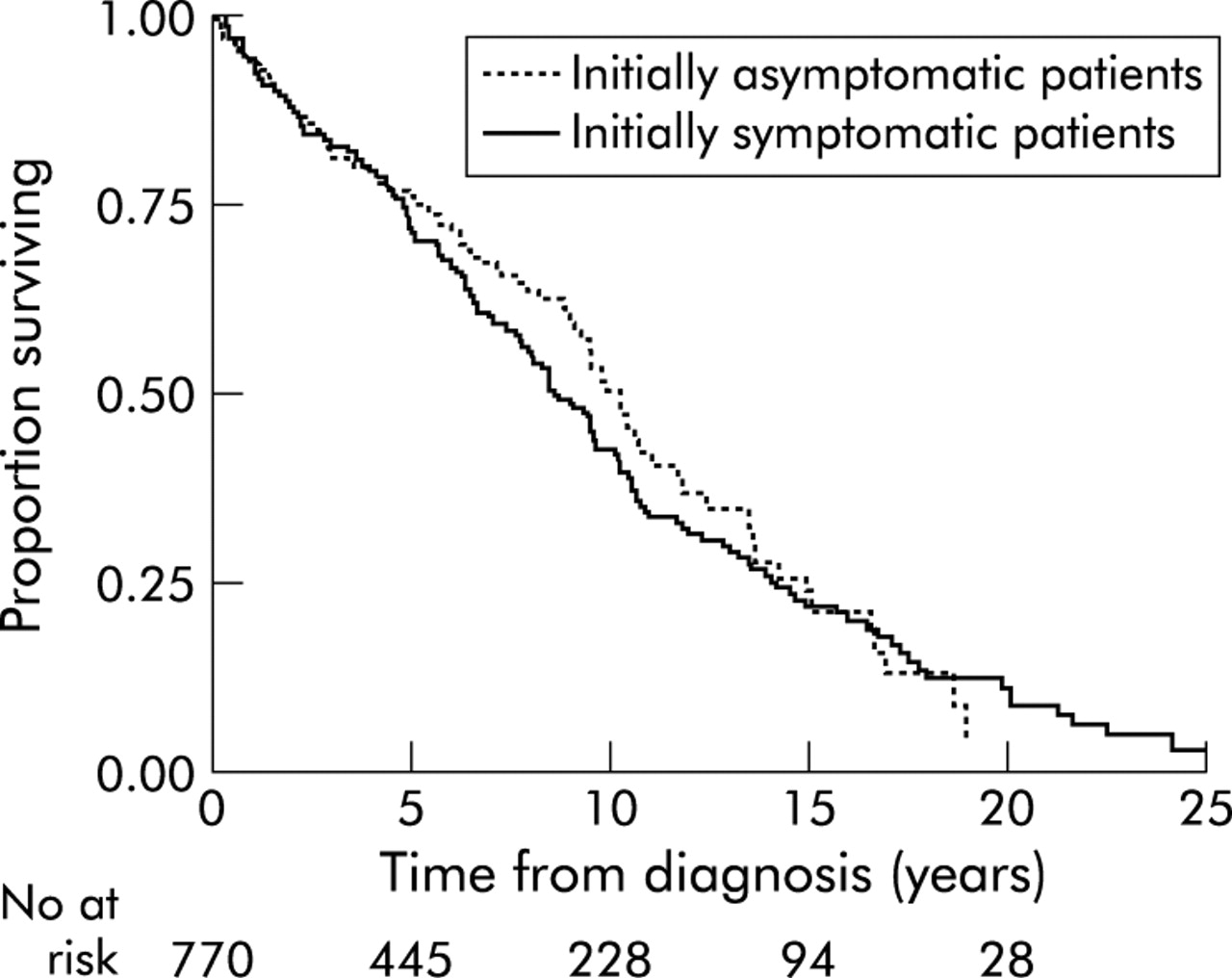
A total of 248 (52.8%) initially asymptomatic patients died during follow up. As shown in fig 1, although median survival time from diagnosis was slightly longer in asymptomatic than in symptomatic patients (9.6 years (95% confidence limits 8.6–10.5) v 8.0 years (6.6–10.0)), this difference was not statistically significant (p = 0.212). This result was unchanged in multivariate survival analysis, including prognostic variables such as age, sex, and initial liver function tests. Censoring patients at the point of transplantation had a small effect on overall survival estimates (approximately one year in all estimates) and did not alter the relative survival of symptomatic and asymptomatic patients.

Kaplan-Meier estimates of patient survival from the time of diagnosis in initially asymptomatic and symptomatic patients.
The primary cause of death, as recorded on patients’ death certificates, is shown in table 2. Twenty four deaths (20 in initially asymptomatic patients) were due to lung cancer. Patient death was due to atheromatous vascular disease in 57 (24% of deaths) initially asymptomatic patients. Twenty two deaths were classified as being due to liver disease following case note review but did not have liver disease listed as the primary cause of death on their death certificate. These deaths have therefore been ascribed to liver disease.
Primary cause of death according to death certificate data
The proportion of deaths that were related to liver disease was lower in initially asymptomatic than symptomatic patients (77 deaths (31% of deaths) v 97 deaths (57%) were related to liver disease respectively; p = 0.004). As shown in fig 2, mortality due to liver disease was lower in initially asymptomatic than symptomatic patients (median survival with non-liver deaths excluded 14.6 years (12.6–20.1) v 24.1 years (17.7 to infinity)). As shown in fig 3, the proportion of deaths in asymptomatic patients due to non-liver related causes decreased with over time between diagnosis and death (χ2 for linear trend = 7.53 (1 df), p = 0.006; χ2 for residual = 10.2 (6 df); p>0.05).

Kaplan-Meier estimates of patient mortality due to liver disease from the time of diagnosis in initially asymptomatic and symptomatic patients.

Proportion of deaths (with 95% confidence interval) attributable to liver disease in initially asymptomatic patients at increasing time from diagnosis.
The indirect SMR for asymptomatic patients was 2.64 (95% confidence limits 2.30–3.02) and was 1.86 (1.57–2.18) excluding liver related deaths. Similar SMRs in initially symptomatic patients were 3.22 (2.74–3.77) and 1.49 (1.16–1.87), respectively.
A total of 255 (60.5%) of 422 initially asymptomatic patients for whom follow up data were available developed symptoms of liver disease during follow up. Table 3 gives the Kaplan-Meier estimate of the proportion of initially asymptomatic patients developing each symptom of liver disease 1, 5, and 10 years after the date of possible diagnosis. Approximately half (51%) of initially asymptomatic patients had developed symptoms of PBC within five years of diagnosis and 95% after 20 years. However, 112 (45%) of 248 initially asymptomatic patients who died during follow up, died prior to the development of liver related symptoms and of causes unrelated to their liver disease.
Kaplan-Meier estimates of the proportion of initially asymptomatic patients developing symptoms of liver disease during the first 10 years of follow up
The effect on survival of symptom development in initially asymptomatic patients was analysed using a time dependent Cox proportional hazards model. Data were available to perform this calculation for 413 (98%) patients. All clinical features, except liver histology at diagnosis, of these 413 initially asymptomatic patients were used in a time independent model of hazard rate. The development of a first symptom of PBC was added into this model in a time dependent fashion. In the adjusted model, symptom development was associated with a small increase in hazard rate which was not statistically significant (p = 0.34), as shown in fig 4. Repeat modelling, including liver histology, did not change this finding.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier estimates comparing patient survival in initially asymptomatic patients before and after symptom development.
Nineteen (7.3% of patients aged less than 65 years at diagnosis) initially asymptomatic patients underwent liver transplantation during the period of follow up. A total of 133 (31.5%) initially asymptomatic patients received UDCA, of whom 99 (74.4%) had developed symptoms prior to starting therapy. Thus only 34 patients had received UDCA before symptom development. The median dose of UDCA was 450 mg/day.
DISCUSSION
As discussed above, with wider diagnosis the recognised phenotype of PBC has changed from a universally severe disorder3,5 to a heterogeneous condition that is often asymptomatic when initially diagnosed. Six groups have subsequently reported their experience of asymptomatic PBC.9,11,13–19 These comprised between 13%16 and 70%15 of PBC patients in their case series.
Direct comparison between these series is difficult due to differences in patient populations (largely derived from tertiary referral centres and therefore possibly subject to Berkson’s bias)9,11,13–15 and varying definitions of the symptoms of PBC (and hence asymptomatic PBC). For example, Springer et al included 18 patients with persistent fatigue among 91 “asymptomatic” patients19 and Roll et al five patients with overt jaundice among 37 “asymptomatic” patients.16 Finally, these series were relatively small, ranging in size from 179 to 9119 asymptomatic patients.
This is the first report of strictly defined asymptomatic PBC in a cohort that was relatively free of selection and referral biases, and with a strict definition of the date of diagnosis. In this large group, slightly more than half (61%) of all patients were asymptomatic at the time that diagnosis was possible.
Three previous studies have compared the laboratory features at diagnosis of asymptomatic and symptomatic patients. Roll et al found that patients with asymptomatic PBC were more likely to have a lower AMA titre and less advanced histological fibrosis than symptomatic patients.16 Nyberg and Loof confirmed that asymptomatic PBC was associated with histologically less advanced disease.15 Uddenfeldt and Danielsson reported that asymptomatic patients had lower alkaline phosphatase, bilirubin, and transaminase levels.20 Our series confirmed all of these except the autoantibody differences.
Five surveys have previously reported on the survival of initially asymptomatic PBC but none of these studies accounted for the effect of prevalent cases on estimates of survival. Nyberg and Loof followed up 56 initially asymptomatic patients for a mean of 9.5 years.15 Median survival (12.7 years) was better than in symptomatic patients (8.0 years) but worse than expected for the general population, although it took 12 years for this to become statistically significant. The Yale liver unit reported the survival of 37 initially asymptomatic patients. These patients had better median survival than initially symptomatic patients (16 years v 7.5 years) but worse than the general population, which became apparent after 11 years of follow up.14,17 Balasubramaniam et al and Springer and colleagues11,19 reported that patients with asymptomatic PBC had decreased survival compared with the general population (median survival 9.5 and 14 years, respectively) although they did not compare this with survival in initially symptomatic PBC patients. In contrast, Uddenfeldt and Danielsson20 found that patients with asymptomatic PBC had similar survival to the normal population, which again was better than in symptomatic patients. However, all five studies were based on very few (all less than 18) patient deaths. (The total number of deaths in all five studies combined was just 47 compared with 248 in the present study.)
Thus until now the consensus has been that survival is better in initially asymptomatic than symptomatic patients. Our study reports survival over a longer period and with a very much larger number of patient deaths than previous series, and did not confirm this finding. We confirmed that asymptomatic PBC has a reduced survival compared with the general population (with an SMR over two and a half times as high as expected).11,13–15 We did not however find that initial symptom status affected subsequent survival, despite asymptomatic patients having lower median bilirubin and less cirrhosis on biopsy than symptomatic patients at diagnosis. Two possible reasons for this are firstly, that although the median bilirubin level was higher in symptomatic patients, relatively few patients had markedly elevated bilirubin levels. Secondly, any improvement in liver related survival in initially asymptomatic patients might have been outweighed by an excess of non-hepatic deaths, particularly in the asymptomatic group.
This is first study to examine non-liver related mortality in asymptomatic PBC. After excluding liver deaths, the mortality rate remained nearly twice that expected. There are several possible reasons for this excess. Firstly, asymptomatic PBC may have been diagnosed during investigation of unrelated conditions and the excess mortality was due to this comorbidity (surveillance bias). The excess of non-liver deaths early after diagnosis supports this possibility. Secondly, two case control studies have previously found an excess of smoking in patients with PBC24,25 and the excess mortality observed here may reflect non-hepatic smoking related adverse events. However, the rates of atheromatous disease and lung cancer, as recorded on death certificates, were broadly similar to those in the local population, suggesting that, if present, this effect is relatively small. Three previous studies have failed to find an excess of mortality due to coronary artery disease in patients with PBC.26–28 Thirdly, the excess mortality may reflect an association between PBC and other diseases. Patel et al found an excess of autoimmune disease in patients with PBC compared with their siblings and friends.25 PBC has been reported to be associated with an excess of non-hepatic malignancy.29–31 A previous study of this cohort followed for a median of 5.4 years found a small but statistically significant excess of non-hepatic cancers when the effect of increased surveillance was accounted for (standardised incidence ratio 1.7 (95% confidence limits 1.3–2.2)).32
Our study is the first to examine the effect of symptom development on patient survival in a time dependent manner. Symptom development did not significantly (p = 0.34) affect patient survival. The lack of a marked effect of symptom development on survival is perhaps to be expected as, in contrast with the above studies, we did not find that survival was different in initially symptomatic and asymptomatic patients. Two previous studies suggested that initially asymptomatic disease had a better prognosis than symptomatic disease only until the development of symptoms.13,14 However, these studies reported on very small numbers of deaths in patients who developed symptoms (15 deaths and two deaths, respectively). Furthermore, they used analysis methods that did not account for the time delay between date of diagnosis and onset of symptoms.
This new perspective may also change attitudes as to when to introduce treatment for patients with asymptomatic PBC. As prognosis is broadly similar to symptomatic patients, it may be argued that, as in the case of asymptomatic systemic hypertension for example, treatment of patients with asymptomatic PBC should be started where possible at the date of diagnosis.
This is the first study to examine the time course of symptom development in initially asymptomatic patients. Previous studies have reported symptom development in 21 (60%) of 35,15 24 (67%) of 36,14 33 (36%) of 91, and 33 (89%) of 3711 initially asymptomatic patients followed for varying periods. However, none of these studies reported the time course of symptom progression. Kaplan-Meier analysis in our cohort clearly shows that the asymptomatic phase of PBC can be regarded as a temporary phenomenon. If patients survive for a long enough period, virtually all will develop one or more symptoms of PBC (95% after 20 years). However, we also found that many patients died before developing symptoms of PBC (45% of deaths occurred in patients who were still asymptomatic), reflecting the age of patients at diagnosis and variation in the progress of disease. The median age at diagnosis in this study (62 years) was 5–10 years higher than in most previous studies—perhaps reflecting referral patterns to tertiary referral centres. This greater age may also explain our higher proportion of non-liver deaths.
Only a small proportion of asymptomatic patients received therapy with UDCA prior to symptom development. The median UDCA dose (450 mg) used is now thought to be subtherapeutic,33 although it is controversial as to whether UDCA affects the prognosis of PBC.34,35 The pattern of UDCA usage may reflect the time period from which patients were drawn and varying prescribing habits among gastroenterologists in the study region.
In conclusion, 20% of initially asymptomatic patients died of liver disease or required transplantation. Furthermore, overall prognosis did not differ from patients presenting with symptoms. These findings contrast with the previous assumption that asymptomatic PBC represents a largely mild form of disease and may have profound implications in future considerations of treatment of disease.
Acknowledgments
The study was supported by the Wellcome Trust (JVM) and the Northern and Yorkshire Regional Health Authority and Medical Research Council (MP).
We are grateful to all of the gastroenterologists and other physicians in Northeast England for their continued support and assistance throughout this study.
REFERENCES
Linked Articles
- Digest
- CORRECTION