Article Text

Abstract
Objective Colorectal cancer (CRC) screening programmes based on the guaiac faecal occult blood test (gFOBT) reduce CRC-specific mortality. Several studies have shown higher sensitivity with the faecal immunochemical test (FIT) compared with gFOBT. We carried out an ecological study to evaluate the impact of FIT-based screening programmes on CRC mortality.
Design In the Veneto Region (Italy), biennial FIT-based screening programmes that invited 50–69-year-old residents were introduced in different areas between 2002 and 2009. We compared CRC mortality rates from 1995 to 2011 between the areas where screening started in 2002–2004 (early screening areas (ESA)) and areas that introduced the screening in 2008–2009 (late screening areas (LSA)) using Poisson regression models. We also compared available data on CRC incidence rates (1995–2007) and surgical resection rates (2001–2012).
Results Before the introduction of screening, CRC mortality and incidence rates in the two areas were similar. Compared with 1995–2000, 2006–2011 mortality rates were 22% lower in the ESA than in the LSA (rate ratio (RR)=0.78; 95% CI 0.68 to 0.89). The reduction was larger in women (RR=0.64; CI 0.51 to 0.80) than in men (RR=0.87; CI 0.73 to 1.04). In the ESA, incidence and surgery rates peaked during the introduction of the screening programme and then returned to the baseline (2006–2007 incidence) or dropped below initial values (surgery after 2007).
Conclusions FIT-based screening programmes were associated with a significant reduction in CRC mortality. This effect took place much earlier than reported by gFOBT-based trials and observational studies.
- COLORECTAL CANCER SCREENING
- CANCER PREVENTION
- CANCER EPIDEMIOLOGY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Colorectal cancer (CRC) screening programmes based on the guaiac faecal occult blood test (gFOBT) reduce CRC-specific mortality.
-
Several studies have shown higher clinical sensitivity of the faecal immunochemical test (FIT) compared with the gFOBT.
-
Data on the impact on mortality of FIT-based screening programmes are still lacking.
What the new findings?
-
Areas where FIT screening programmes were active showed a 22% reduction in CRC-specific mortality.
-
The impact of FIT programmes on mortality was greater and took place earlier compared with available evidence on gFOBT-based screening programmes.
How might it impact on clinical practice in the foreseeable future?
-
A screening schedule based on a single FIT with a positivity cut-off for a haemoglobin concentration of 20 µg Hb/g faeces (100 ng Hb/mL buffer) and an inter-screening interval of 2 years significantly reduces CRC mortality.
-
The reduction of incidence rates associated with the removal of precancerous lesions may convey an even higher impact on mortality in the medium–long-term.
Introduction
Colorectal cancer (CRC) is the third most common cancer in men and the second most common in women worldwide and represents a significant cause of cancer-related morbidity and mortality.1
Four randomised controlled trials evaluated the effect of a screening programme based on the guaiac faecal occult blood test (gFOBT) on CRC-specific mortality2–5 and found a 16% overall reduction in mortality compared with the non-screened controls.6
In the last 15 years, several screening programmes have been activated in many countries,7 ,8 mainly based on a periodic invitation to do a gFOBT. However, many studies have shown that the performance of the faecal immunochemical test (FIT) is higher than that of gFOBT9–14 and many programmes have adopted this kind of test as recommended by the European Guidelines on CRC screening.15
No trial has been carried out on CRC screening using FIT and therefore the impact of the use of these tests on mortality can only be derived from observational data of existing screening programmes.
The results of a few population screening programmes based entirely on the gFOBT have reported a reduction in mortality ranging from 10% to 16% in the screened populations.16–18 However, data about the impact of FIT-based screening programmes on mortality are lacking.
The main purpose of this study was to analyse the impact of FIT-based population screening programmes on CRC mortality by comparing the mortality rates of areas with early and delayed establishment of the screening programme. We also evaluated the effect of screening programmes on CRC incidence rates and on surgical resection rates.
Methods
CRC programmes in the Veneto Region
In the Veneto Region (Italy), which has about 4.9 million inhabitants, CRC is the second most common cancer (13% of all cancers)19 and the second most important cause of death from tumours (11%).20
The Regional Health System is subdivided into 21 local health units (LHUs) which are the public agencies that organise and administer the health services, including screening programmes, in 581 municipalities. According to Italian law21 and in line with the recommendations of the European Council,22 population-based CRC screening programmes started in 2002 in the Veneto Region and are still being implemented. The screening programmes involve residents from 50 to 69 years of age who are invited via mail every 2 years to perform a single FIT, without any dietary restriction. Non-compliers with the first invitation are mailed a reminder, usually within 6 months. Most programmes use the OC-Hemodia latex agglutination test, developed with the OC-Sensor Micro instrument (Eiken, Tokyo, Japan), excluding one LHU which used FOB Gold (Sentinel Diagnostics, Milan, Italy) for the first 3 years.
Preanalytical and analytical aspects of the programmes are reported in online supplementary appendix 1, according to the Standard for Faecal Immunochemical TesTs for Haemoglobin Evaluation Reporting (FITTER) guidelines that have been recently proposed by the World Endoscopy Organization.23 Quantitative haemoglobin analysis is performed by automated instruments; the cut-off for test positivity is 20 µg Hb/g faeces (100 ng Hb/mL buffer).24 Subjects are notified of their results by mail and people with a negative FIT are advised to repeat the screening in 2 years. Subjects with a positive screening test are contacted by telephone to undergo a total colonoscopy (TC) performed at an endoscopic referral centre during dedicated sessions. Patients with screening-detected cancer are referred to surgery or surgical endoscopy and then enrolled in a follow-up programme.
FIT screening programmes were established in different LHUs between 2002 and 2009. The LHUs where screening was set up in 2002–2004 were classified as ‘early screening areas’ (ESA) and those where screening started in 2008–2009 as ‘late screening areas’ (LSA). All the following analyses have been restricted to the ESA and the LSA, thus excluding LHUs that instituted screening programmes between 2005 and 2007.
Mortality
Death certificates are sent by each municipality to the LHU. Until 2005, causes of death were coded in each LHU according to International Classification of Disease (ICD)9. Since 2006, LHUs have transmitted a copy of the certificate to the Regional Epidemiological Department for coding of the underlying cause (using ICD10 since 2007) and entry into the electronic regional archive of causes of death.
The mortality records of residents in the Veneto Region in the period 1995–2011 were used to identify all deaths of subjects aged 50–74 years due to CRC (ICD9 153–154; ICD10 C18–C21). A sensitivity analysis was carried out adding codes for malignancy of the intestinal tract, part unspecified (ICD9 159.0, ICD10 C26.0).
The 70–74 age group was included in the analysis in order to account for the medium–long-term effect of screening on mortality (as well as incidence and surgery) rates, which is also expected to take place in older subjects who were screened in their 60s.
Incidence
The Veneto Tumour Registry (VTR) covers 49% of the regional population (about 2.3 million inhabitants) and has been active since 1989. A case-resolution programme resolves more than half the diagnoses by evaluating the concordance among the three main sources (hospital discharge records, pathology records and death certificates). The remaining cases are ascertained through the consultation of medical charts.
All malignant incident cases are recorded according to the third version of the International Classification of Diseases for Oncology (ICD-O 3).25 Multiple primaries are coded according to the 2004 classification proposed by the International Association of Cancer Registries, the International Agency for Research on Cancer and the European Network of Cancer Registries. Incidence rates are available up to 2007. This analysis includes invasive CRC (ICD-X C18–21) diagnosed from 1995 to 2007 among subjects aged 50–74 years in the areas covered by the VTR (ESA: LHUs 2-Feltre and 13-Mirano; LSA: LHUs 3-Bassano del Grappa, 12-Veneziana and 19-Adria; figure 1).

Map of local health units of the Veneto Region by period of activation of a colorectal screening programme.
Surgical resections
The regional archives of hospital discharge records include all hospitalisations in regional hospitals as well as discharges of residents hospitalised outside the region, thus ensuring complete coverage of all major surgical procedures performed in the population. Discharge diagnoses and procedures are recorded according to the ICD, 9th edition—Clinical Modification.
All discharges from 1 January 2001 to 31 December 2012 of patients aged 50–74 years with a diagnosis of CRC (ICD9-CM diagnostic codes 153–154, 230.3, 230.4) and intervention codes 45.7–45.8 (colon resection) and 48.35, 48.5, 48.61–48.69 (rectal resection) were extracted. In the case of repeated admissions of the same subject with the selected codes, only the first hospitalisation was considered. Subjects already hospitalised for CRC surgery in 2000 were excluded from the analyses.
Statistical analysis
Crude and age-specific mortality, incidence and surgery rates were computed as the number of events per 100 000 people, with population data derived from the National Institute for Statistics (http://demo.istat.it/). Age-standardised rates were obtained by the direct standardisation method, taking the European standard population as reference.
A difference in mortality due to an earlier adoption of the screening programme was assessed by two Poisson regression models of CRC mortality rates. A first model examined three approximately equal calendar periods: before introduction of the screening programmes in the Veneto Region (1995–2000), and around (2001–2005) and after (2006–2011) the establishment of the screening programmes in the ESA; an interaction term between the study area and the calendar period explored any differences in the time change in CRC mortality rates between the ESA and the LSA.
Thereafter, a model of segmented Poisson regression was built assuming that a different trend in mortality could be observed immediately after the start of the screening programme in the ESA:
where the trend is a continuous variable equal to the years since the start of the study period. Change is a continuous variable that is the number of years since the intervention in 2002. The difference in change is equal to the change for the ESA and to 0 for the LSA; X is the set of other covariates in the model (age class and gender). According to this parameterisation, β1 corresponds to the difference in log-rates between the ESA and the LSA before the intervention, β2 corresponds to the common time trend in both areas before the intervention, β3 to the change in trend after 2002 in the LSA and β4 to the different change in trend in the ESA with respect to the LSA after 2002.
The above models were run in the total population aged 50–74 years adjusting for gender and 5-year age classes, and in men and women separately.
Results
Five LHUs set up screening programmes during 2002–2004 (2-Feltre, 4-Alto Vicentino, 7-Pieve di Soligo, 13-Mirano and 22-Bussolengo; ESA) while another five were started in 2008–2009 (3-Bassano del Grappa, 10-Veneto Orientale, 12-Veneziana, 16-Padova and 19-Adria; LSA) (figure 1). The other 11 LHUs established screening programmes between 2005 and 2007 and are not included in the study population. At the mid-period (2001–2005), the 50–74-year-old resident populations of the ESA and the LSA were 274 266 and 348 674 subjects, respectively (table 1), accounting for 20.7% and 26.3% of the regional population of the same age band (n=1 325 993).
Mean population and age-standardised mortality, incidence and surgery rates for colorectal cancer (European standard population) with 95% CIs by gender and calendar period in areas of early/late establishment of the screening programme
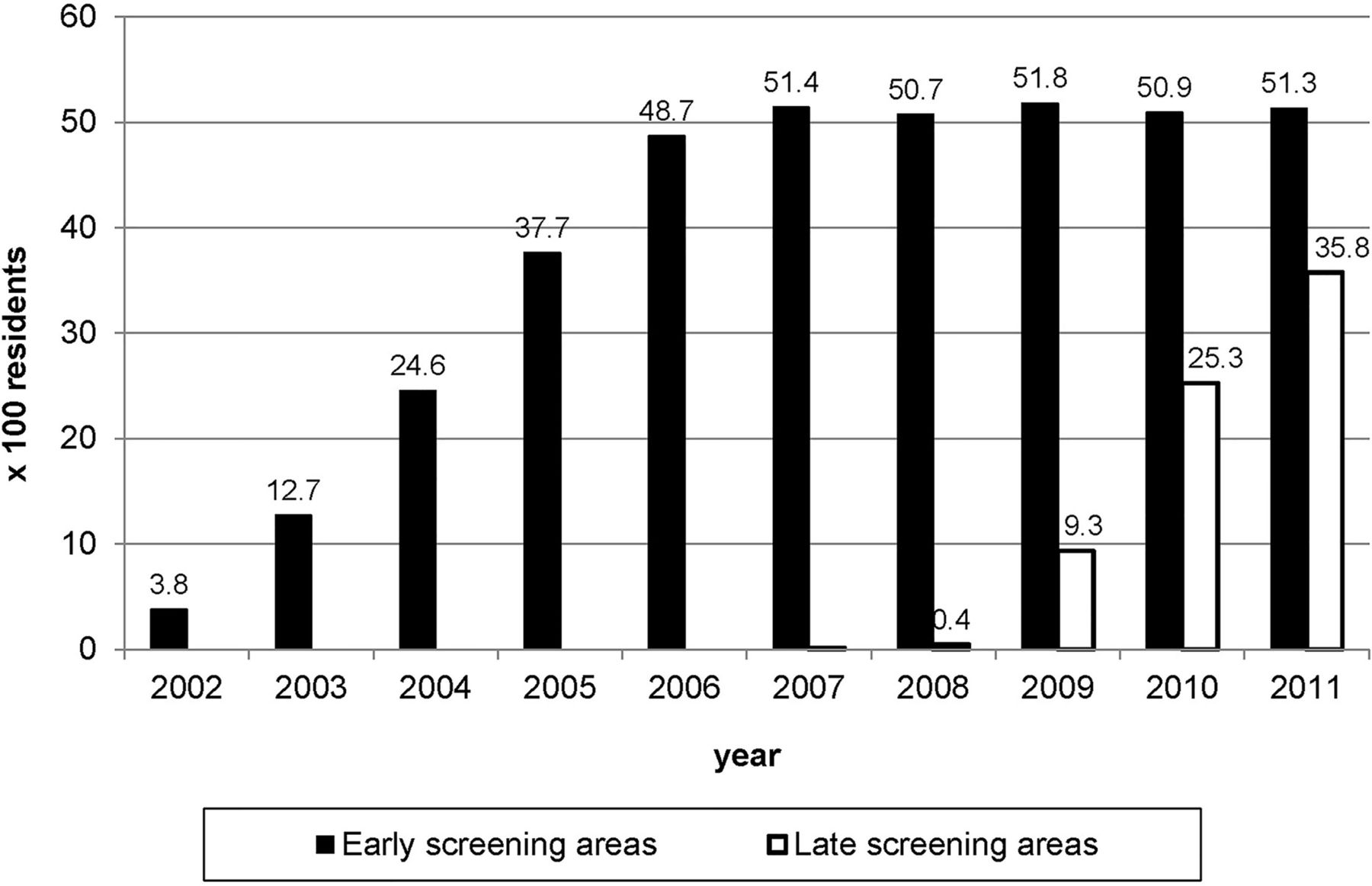
The population coverage with FIT in the ESA increased progressively from 2002 to 2006, when it reached a steady state with about half of the residents aged 50–69-year-old being tested with FIT (figure 2). In the LSA, coverage increased from 9% in 2009 to 36% in 2011.
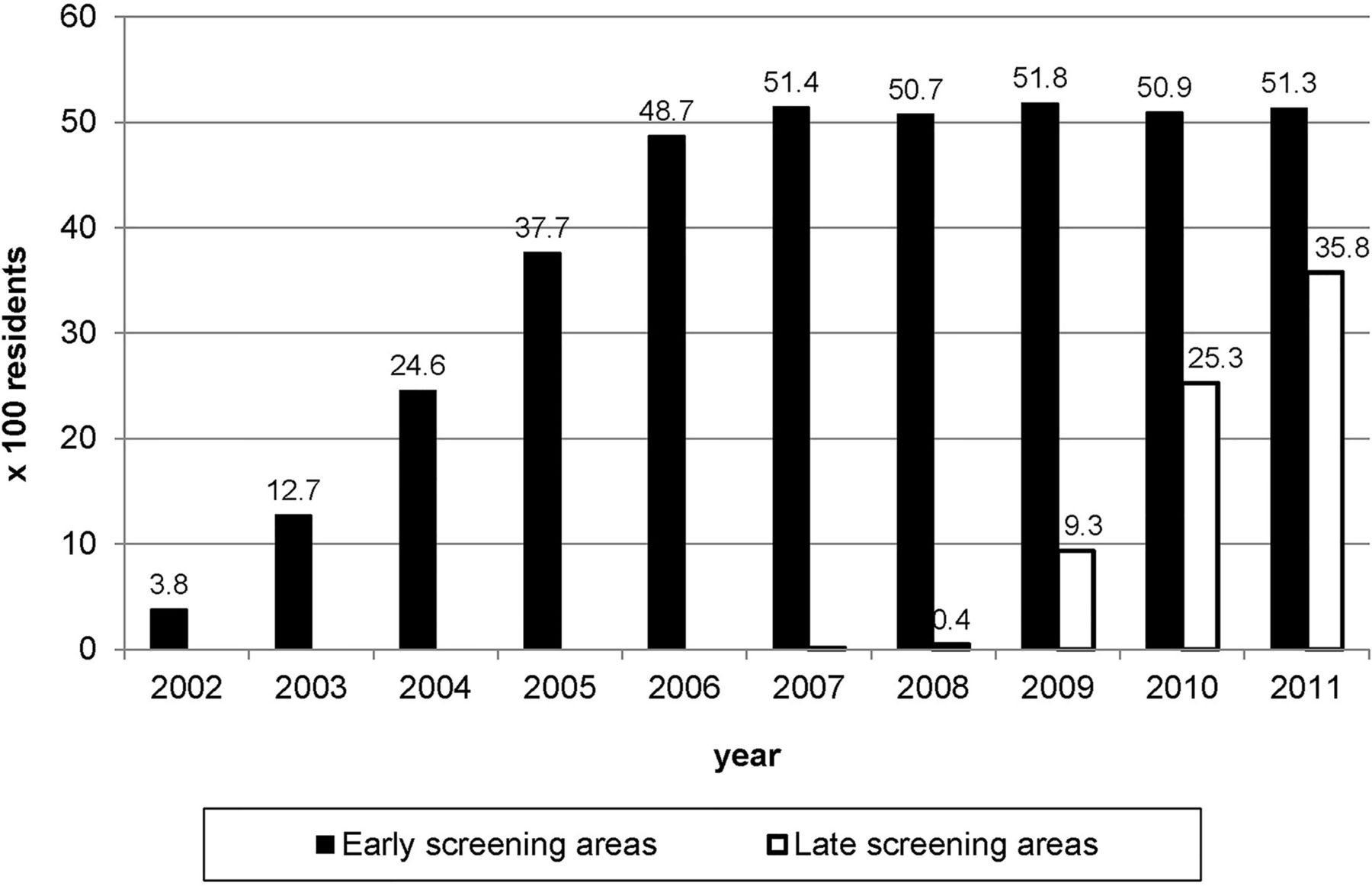
Coverage of the resident population with the screening test (proportion of 50–69-year-old residents who complied with invitation in the previous 2 years) by period of activation of colorectal screening programme.
Table 1 reports CRC mortality, incidence and surgery rates in the ESA and the LSA during 1995–2000, 2001–2005 and 2006–2011, overall and by gender. The population aged 50–74 years increased throughout the study period, especially in the ESA.
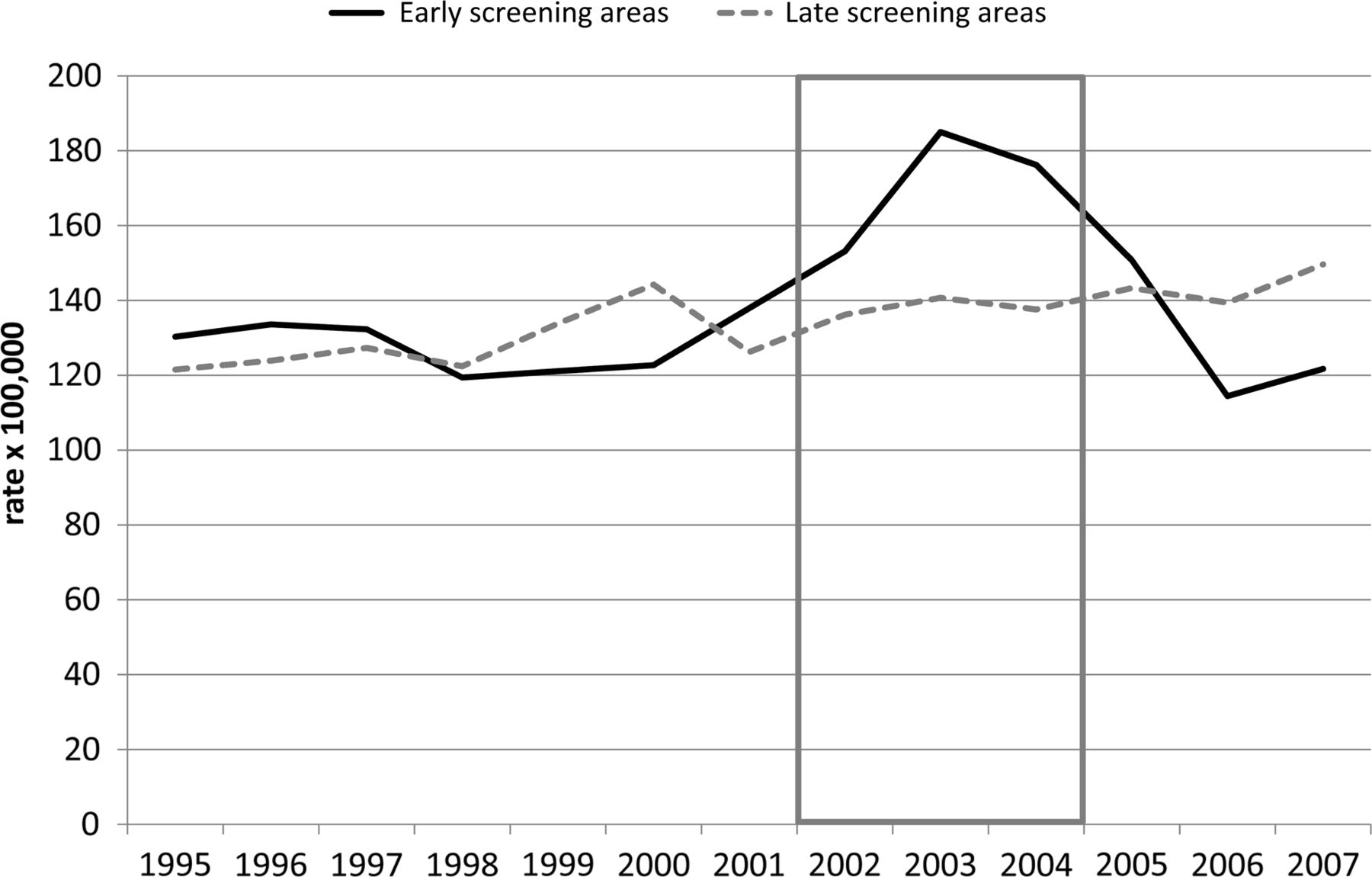
In the ESA, mortality rates in 2006–2011 were compared with those observed in 1995–2000 and showed an overall decline of 24% (22% in men and 32% in women). In the LSA, a smaller decrease was observed among men, whereas mortality among women remained almost unchanged. Figure 3 shows that mortality (both genders combined) was similar at the beginning of the study period, whereas after the introduction of the screening programmes, the rates observed in the ESA fell below the values registered in the LSA.

Age-standardised (European standard population) colorectal cancer mortality rates, by year and period of activation of the screening programme; 50–74-year-old subjects, 1995–2011. Grey and dotted boxes: period of activation of colorectal screening programme in early and late screening areas, respectively.
The Poisson regression models confirmed that the time trend in mortality rates changed after the introduction of screening programmes in the ESA compared with the LSA (table 2). The mortality rate difference in 2006–2011 vs. 1995–2000 between the areas was statistically significant in both genders combined (rate ratio (RR)=0.78; 95% CI 0.68 to 0.89) and among women (RR=0.64; CI 0.51 to 0.80), but not among men (RR=0.87; CI 0.73 to 1.04). The findings did not change if codes for malignancy of the intestinal tract were added to the analysis of mortality rates (data not shown).
Rate ratios (RRs) with 95% CIs for colorectal cancer mortality estimated by two Poisson regression models, early screening areas (ESA) vs. late screening areas (LSA)
Incidence rates were available for only part of the LHUs included in the ESA and the LSA. They showed a major peak during the introduction of screening programmes in the ESA, and then returned to the baseline in 2006–2007, which are the last years with incidence figures. The incidence rates in the LSA increased progressively between 1995 and 2007 (figure 4).
Age-standardised (European standard population) rates of colorectal cancer incidence by year and period of activation of the screening programme; 50–74-year-old subjects, 1995–2007. The grey box shows the period of activation of colorectal screening programme in early screening areas.
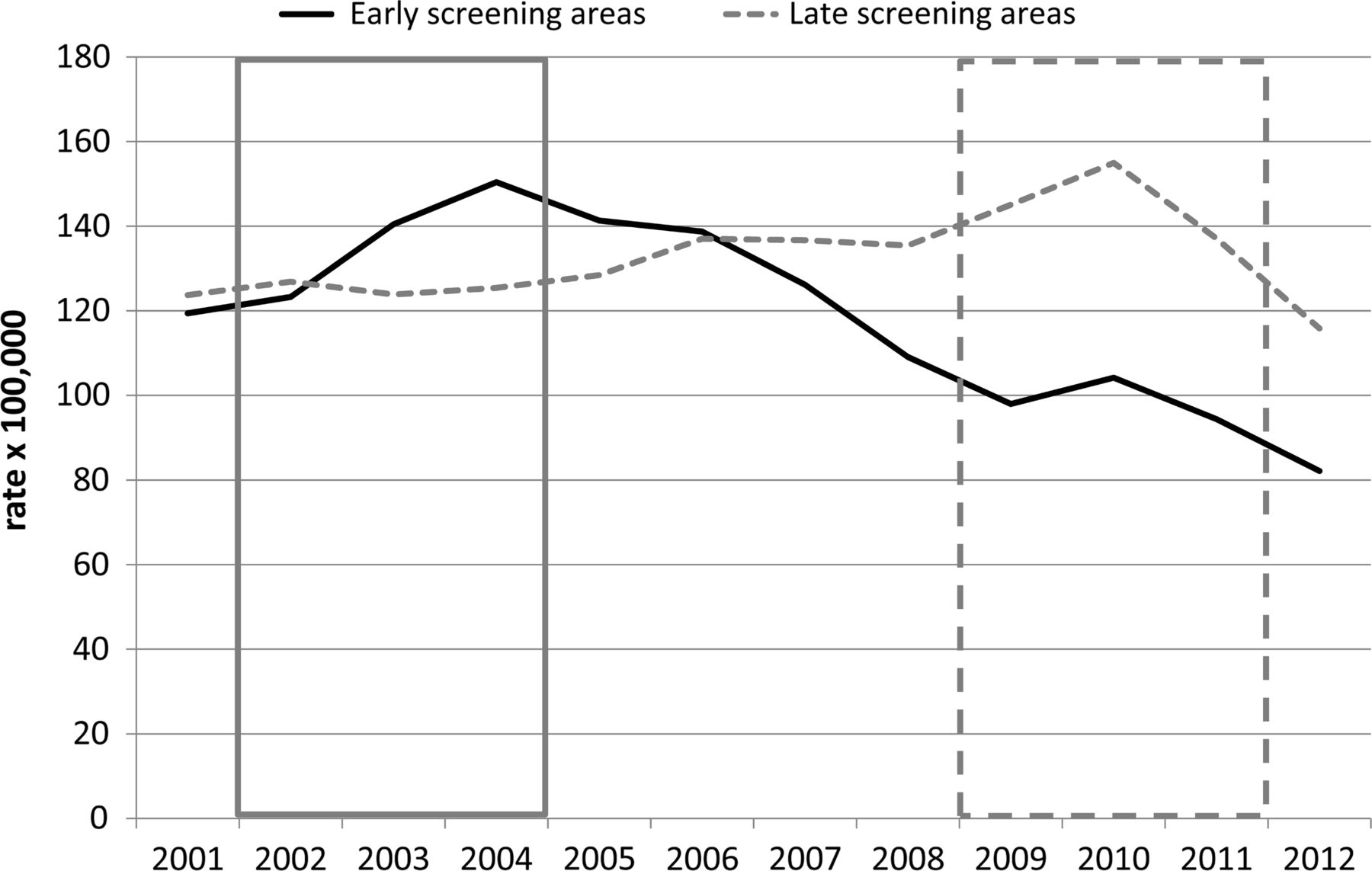
Surgical resection rates in 2001 were similar in the ESA and LSA (119.4 and 123.7 per 100 000, respectively), peaked according to the spread of the screening programmes in 2004 in the ESA (150.4 per 100 000) and in 2010 in the LSA (155.0×100 000), and then dropped to lower values (82.1×100 000 in 2012 in the ESA) (figure 5). Compared with 2001, the 2012 RR of surgical rates in the ESA was 0.69 (95% CI 0.58 to 0.81).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-standardised (European standard population) rates of colorectal cancer resection by year and period of activation of the screening programme; 50–74-year-old subjects, 2001–2012. Grey and dotted boxes: period of activation of colorectal screening programme in early and late screening areas, respectively.
Discussion
This ecological study provides the first evidence regarding the impact of FIT-based CRC screening programmes on CRC mortality. We observed an early reduction of CRC mortality in those areas where screening programmes had been set up, which took place about 4 years after the screening started and amounted to 22% until the 10th year of screening activity.
The reduction of mortality that we observed is greater and took place earlier compared both with other ecological evidence16 and to a per-protocol analysis of the trials.6 However, this result is not surprising. Our programmes used FIT, which has shown a higher sensitivity for cancer and precancerous lesions than gFOBT.9–14 It is also associated with a higher compliance with invitation to screening.26 In fact, FIT compliance in the ESA was high—69.1% overall during the whole study period—and the actual extension (i.e., the proportion of the target population invited during the period of interest) was 81.4%.27 ,28 On the other hand, Costantini and colleagues reported that the impact of screening on mortality was evident after 10 years of screening and reached a 13% overall reduction over 20 years. However, the compliance with the gFOBT invitation was low—less than 40%—especially during the programme's first years.16 Screening uptake for gFOBT in data published on France17 and Scotland18 ,29 ,30 ranged from 52.8% to 55.0%.
Furthermore, some trials may have underestimated the potential reduction of mortality since the estimated effect of screening was probably diluted by a low compliance with the protocol. In some studies, at least a third of the enrolled subjects did not undergo even one screening test.3 ,4
The impact of screening on mortality rates is likely to take place mainly through two different mechanisms: the reduction of incidence rates, which is expected to have an impact on mortality in the medium–long-term, and the improvement of the prognosis of screen-detected cases. Data from the Italian national survey on colorectal screening programmes showed a better distribution by stage of screen-detected cases vs. cases diagnosed outside the screening setting.31 More than half of the 281 CRCs that were detected by screening in Veneto in 2006 were stage I, compared with 12% of the 609 cases diagnosed in 2000–2001 in the absence of a screening programme.27 This is likely to be the reason for the early reduction of mortality rates observed in the ESA.
The reduction of CRC mortality that we observed in the ESA was statistically significant among women, but not in men. Previous studies on the impact of screening on CRC mortality did not report this effect, while the results by gender of the main process- and early impact-indicators are contrasting. A higher compliance among women invited to screenings has been reported in the literature31–34 as well as in the Veneto Region,27 ,28 whereas, in our experience, compliance with TC of FIT+ subjects was higher among men. A higher sensitivity for advanced neoplasia35 and CRC in men has been also described.36 According to the evaluation of the proportional incidence of interval cancers, CRC sensitivity in our programmes was higher for men than women (80.1% vs. 74.8%), although the difference was not statistically significant.37
The biological mechanisms that were hypothesised to explain gender differences (lower haemoglobin concentrations in blood, slower colonic transit time)38 ,39 account for a lower sensitivity of screening among women, but not the opposite. Thus, the most plausible explanation of our result is that the impact of screening on mortality could be masked by the reduction of CRC-specific mortality rates in men that took place during the study period both in the ESA and the LSA (table 2).
The reduction of mortality that we estimated is relevant for the population's health and in terms of economic savings for the Regional Health System. Figure 5 shows that 10 years after the introduction of the programme in the ESA, surgical resection rates declined by about 30%. In a relevant proportion of screen-detected cases, the treatment is limited to endoscopic resection (19.8% out of over 2500 screen-detected CRCs in Italy in 2008),32 resulting in an improved quality of life for patients and reduced costs. The effect of screening on surgical hospitalisation rates is relevant because more than half of the CRCs are diagnosed in subjects who are 50–74-years-old.40 Moreover, a further 40% of CRCs affect older ages. In the medium-term and long-term, we can also expect the screening to have an impact on this age group through a reduction in incidence following the removal of precancerous lesions that occurred when the subjects were of screening age.
The impact of screening programmes on incidence rates has already been described in the literature.41 ,42 It is suggestive of a two-step effect. Screening is initially associated with an immediate increase of newly diagnosed CRCs deriving from the diagnostic anticipation of cases that otherwise would be detected later. Screening also allows the detection and removal of a large number of precancerous lesions (i.e., advanced adenomas) with an outcome on primary prevention of CRCs that is expected to translate into a reduction of future incidence rates.
Unlike the four randomised controlled trials that evaluated the effect of a screening programme based on the gFOBT2–5 in which the impact on incidence rates could only be seen after a long time lag,43 our experience has shown that the impact began in the third year after the start of screening.
As in all ecological studies, the present findings could be affected by several possible sources of bias.44 First, there can be differences in the underlying CRC risk between areas. We are confident that this is not the case in our study because, first of all, the two LHU groups have not been aggregated into specific areas within the region but are a geographic mix. Second, CRC incidence and mortality rates in the ESA and the LSA before the start of screening were similar.
A second major bias could be contamination, i.e., the spread of opportunistic screening before the introduction of organised programmes in the LSA. This bias could have led to an underestimation of the effect of CRC screening. During the study period, a proportion of subjects underwent faecal occult blood tests (FOBT, thus including both gFOBT and FIT) and TCs independently of prevention screening programmes and/or because of clinical symptoms. The spread of this practice in the target population (50–69-years-old) was monitored by Progressi delle Aziende Sanitarie per la Salute in Italia,45 an ongoing surveillance system that monitors the prevalence of major behavioural risk factors for non-communicable chronic diseases and the adherence to some important preventive measures. According to the 2007 survey, FOBT coverage in the entire Veneto Region for the previous 2 years was 41.1% with 93% having free-of-charge access to the test (i.e., through a screening programme).46 Therefore, the extra-screening FOBT coverage was negligible; similar findings were reported for TC. Moreover, a significant ‘halo effect’ of the screening programmes on the coverage with FOBT or TC in nearby areas is unlikely, given that there has been no increase in incidence in the areas adjoining those with screening programmes until 2007.
Third, the mortality reduction in the ESA could depend on differential changes in treatment efficacy between the areas during the study period. Advances in CRC treatment over the last decade include the introduction of laparoscopic surgery47 and the introduction of new therapeutic agents for metastatic cancer.48 However, there are no cutting-edge universities or healthcare facilities located within the ESA that could be used for innovative early therapeutic approaches.
Ultimately, the only evident difference in CRC diagnosis and management across the public regional health system during the study period was the staggered establishment of screening programmes.
In conclusion, huge changes in terms of CRC mortality, incidence and hospitalisations were observed in those areas where FIT-based screening programmes were introduced. Moreover, the impact of screening took place much earlier than observed in gFOBT-based trials and observational studies. These findings are particularly relevant to increasing the evidence regarding the efficacy of FIT as a screening test but further research on this topic is necessary.
Acknowledgments
We thank Dr. Lorena Zardo and Dr. Daniela Rubin for their work in compiling the FITTER checklist.
References
Footnotes
-
Contributors MZ, UF: study concept and design; interpretation of data; drafting of the manuscript. ES, EB, SG, SB, CF: data collection and statistical analysis. MZ, UF, MS, APDT: interpretation of data. All the authors: critical revision of the article for important intellectual content and final approval of the article.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.