Article Text

Abstract
Objective Although serrated polyps may be precursors of colorectal cancer (CRC), prospective data on the long-term CRC risk in individuals with serrated polyps are lacking.
Design In a population-based randomised trial, 12 955 individuals aged 50–64 years were screened with flexible sigmoidoscopy, while 78 220 individuals comprised the control arm. We used Cox models to estimate HRs with 95% CIs for CRC among individuals with ≥1 large serrated polyp (≥10 mm in diameter), compared with individuals with adenomas at screening, and to population controls, and multivariate logistic regression to assess polyp risk factors for CRC.
Results A total of 103 individuals had large serrated polyps, of which 81 were included in the analyses. Non-advanced adenomas were found in 1488 individuals, advanced adenomas in 701. Median follow-up was 10.9 years. Compared with the control arm, the HR for CRC was 2.5 (95% CI 0.8 to 7.8) in individuals with large serrated polyps, 2.0 (95% CI 1.3 to 2.9) in individuals with advanced adenomas and 0.6 (95% CI 0.4 to 1.1) in individuals with non-advanced adenomas. A large serrated polyp was an independent risk factor for CRC, adjusted for histology, size and multiplicity of concomitant adenomas (OR 3.3; 95% CI 1.3 to 8.6). Twenty-three large serrated polyps found at screening were left in situ for a median of 11.0 years. None developed into a malignant tumour.
Conclusions Individuals with large serrated polyps have an increased risk of CRC, comparable with individuals with advanced adenomas. However, this risk may not be related to malignant growth of the serrated polyp.
Trial registration number The Norwegian Colorectal Cancer Screening trial is registered at clinicaltrials.gov (NCT00119912).
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Serrated polyps are thought to be precursors of colorectal cancer (CRC).
-
Prospective studies quantifying the risk of CRC in patients with serrated polyps are lacking.
-
The natural history of serrated polyps is unknown.
What are the new findings?
-
Patients with large (≥10 mm in diameter) serrated polyps have a 2.5-fold increased risk of developing CRC compared with the general population.
-
This risk is comparable with the risk of patients with advanced adenomas.
-
Large serrated polyps left in situ do not frequently progress to CRC.
-
The excess risk of CRC in patients with large serrated polyps may not be due to malignant growth of the serrated polyp, but to a ‘field’-effect in the patient with these polyps.
How might it impact on clinical practice in the foreseeable future?
-
Individuals with large serrated polyps have an increased risk for future CRC.
-
Meticulous inspection of the entire colorectum is warranted when a large serrated polyp is detected, as tumours may occur elsewhere in the colon.
Introduction
Until recently, colorectal cancer (CRC) has been thought to develop from adenomas through the adenoma–carcinoma pathway.1 Recent evidence has suggested, however, that up to 30% of CRC cases may not develop from adenomas, but from serrated polyps through an alternative path, the so-called serrated polyp pathway.2 These cancers have genetic and epigenetic features found more frequently in serrated polyps than adenomas, suggesting that serrated polyps may be the precursor of these tumours.3–6 Serrated polyps include hyperplastic polyps (HP), sessile serrated adenomas/polyps (SSA/P) and traditional serrated adenomas (TSA).7 Autopsy studies have estimated the prevalence of serrated polyps at 13%–52%.8–10
Because serrated polyps are proposed as precursors of CRC, removal of all these lesions is recommended in recent surveillance guidelines.11 ,12 However, the guidelines emphasise that their recommendations are based on weak scientific evidence, because little is known about the natural history of serrated polyps. It is currently debated whether serrated polyps have a fast or slow progression to cancer (up to 15 years), and the importance of serrated polyps as a marker for increased cancer risk in the patient, without malignant transformation within the serrated polyps themselves (so-called field effect).13–18
To improve the evidence for surveillance guidelines, we studied the natural history and risk of CRC among individuals with large serrated polyps identified in a population-based sigmoidoscopy screening trial. This screening trial was conducted when serrated polyps were still designated HP and no surveillance or polypectomy was routinely recommended.
Methods
The screening trial
The present study was conducted within the Norwegian Colorectal Cancer Prevention trial (NORCCAP).19–21 Altogether, 100 210 individuals aged 50–64 years, living in the city of Oslo or Telemark county, Norway, were randomly assigned to receive invitations to a flexible sigmoidoscopy screening (screening arm) with or without a single additional faecal occult blood test (FOBT), or to no screening (control arm) between 1999 and 2001. Of these, 1418 (1.4%) individuals were excluded from the analyses. Among 20 572 individuals randomised to screening, 12 955 (63%) attended the examination (figure 1).
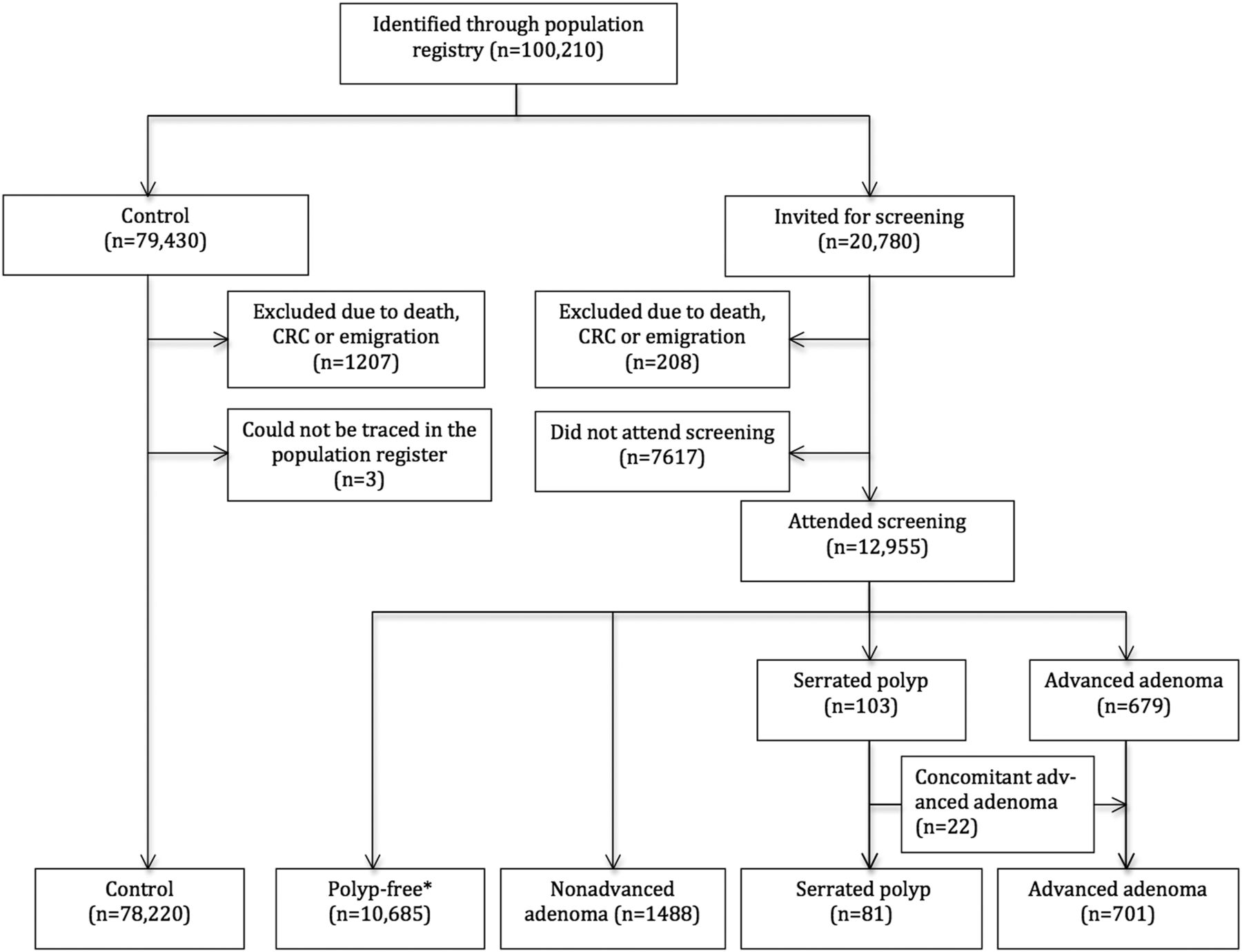
Flowchart. *No adenomas or serrated polyps ≥10 mm.
During the screening sigmoidoscopy, all visible lesions were biopsied, and individuals with a histologically verified cancer, adenoma, any polyp 10 mm or larger or a positive FOBT were offered follow-up colonoscopy (performed within 6 weeks of the positive sigmoidoscopy/FOBT). Of the 2639 individuals offered colonoscopy, 2520 (95%) attended, and all adenomas were removed. For the purpose of this study, screening flexible sigmoidoscopy and follow-up colonoscopy of screen-positive individuals are defined as ‘screening’. Due to the lack of guidelines and clinical awareness, treatment of non-adenomatous polyps (HP according to diagnostic guidelines at that time) was not standardised; by the discretion of the endoscopist, some polyps were resected, while others were only biopsied and left in situ if biopsy sampling revealed non-adenomatous histology.
A total of 1268 individuals were recommended colonoscopy surveillance according to Norwegian postpolypectomy guidelines22 because they had advanced adenomas (three or more adenomas, high-grade dysplasia, villous histology or size 10 mm or larger), small (1–4 mm) histologically verified tubular adenomas left in situ, CRC in first-degree relative or inadequate screening examination (poor bowel cleansing, missing histology or incomplete polyp resection). Of these, 1084 (85%) were recommended surveillance within 5 years.19
For the present study, we defined the following study groups in the screening arm:
Non-attender group: Individuals invited to screening who did not accept the invitation and were not screened.
Attender-group: According to the findings at screening (including screening flexible sigmoidoscopy and colonoscopy of screen-positive individuals), we classified screening attenders into four groups.
-
Non-advanced adenoma group: Individuals with one or two tubular adenomas <10 mm, without high-grade dysplasia.
-
Advanced adenoma group: Individuals with three or more adenomas or at least one adenoma with diameter ≥10 mm, villous features or high-grade dysplasia.
-
Serrated polyp group: Individuals with large serrated polyps (≥10 mm in diameter; including sessile serrated polyps, traditional serrated polyps, HP, and unclassified serrated polyps, no more than two non-advanced adenomas and no advanced adenoma.
-
Polyp-free group: Individuals without adenomas or large serrated polyps (≥10 mm in diameter).
Groups 1–3 were offered colonoscopy within 6 weeks after flexible sigmoidoscopy screening.
Serrated polyp group
We retrieved pathology specimens from the screening examinations performed between 1999 and 2001 in all individuals in the serrated polyp group. All polyps were reviewed, and those with serrated histology were reclassified by two experienced GI pathologists (EML and KG) into four groups according to the 2010 WHO criteria:23 (1) HP; (2) SSA/P with or without dysplasia; (3) TSA or (4) unclassified if the specimen did not allow precise subclassification (mainly due to small or superficial biopsy specimens or lack of proper orientation of tissue in the paraffin-blocks).
Serrated polyposis syndrome was defined according to current WHO criteria as: (1) at least five serrated polyps proximal to the sigmoid colon, with two or more >10 mm, and/or (2) >20 serrated polyps of any size distributed throughout the colon.23 All specimens were independently reviewed and results were compared. In case of disagreement, the specimen was re-examined by the two pathologists in companionship. If consensus could still not be reached, a third expert pathologist (TJE) established a final diagnosis. The pathologists were blinded for clinical information (polyp size, number of polyps, polyp shape, and localisation). We searched hospital records and reviewed reports from endoscopic examinations performed after screening (between 1999 and 2001) until 1 September 2012 in all individuals in the serrated polyp group. All pathology specimens from removed colorectal polyps during follow-up were retrieved and examined as described above.
All individuals in the serrated polyp group who were alive and not diagnosed with CRC by 31 December 2011 were invited for colonoscopy, performed between September 2012 and March 2013 by three experienced endoscopists (MB, ØK or ØH). All detected polyps were removed and subjected to histopathological evaluation. To ensure meticulous inspection of colonic segments with previous polyps, the endoscopists had access to previous endoscopy and pathology reports.
Outcomes and endpoint acquisition
Using the unique national identity number for all inhabitants in Norway, we identified CRC cases by linking all individuals to the nation-wide Cancer Registry which is virtually 100% complete.24 Additionally, we obtained information from the Population Registry and Cause of Death Registry. Thereby, we achieved complete follow-up and ascertained emigration, diagnosis of incident cancer as well as date and cause of death. Primary outcome was the comparison of the study groups with regards to CRC incidence. CRC was defined as adenocarcinoma with topography codes C18–C21 according to the third edition of the International Classification of Diseases of Oncology.25 Secondary outcomes were findings at colonoscopies performed after the screening examination in the serrated polyp group.
Statistical methods
We calculated age-standardised incidence rates as absolute measures of CRC incidence using the screening arm as the standard, and estimated HRs with 95% CIs as a measure of relative risk by fitting Cox regression models adjusted for age and sex. We calculated the HRs with two different control groups as the reference. First, we compared the different polyp groups to the NORCCAP control arm to assess CRC risk relative to the general population. Second, we used the polyp-free group as the reference to assess CRC risk relative to a low-risk population. The proportionality assumption in the comparison with the NORCCAP control arm was violated due to screen-detected CRC in the screening arm (visual inspection of the plotted scaled Schoenfeld's residuals). To further test whether the HRs were valid, we calculated the age-standardised CRC incidence rate ratios for the different polyp groups relative to the NORCCAP control arm with the same results as from the Cox model. Follow-up time was calculated from entry date until a diagnosis of CRC, death, emigration or 31 December 2011, whichever occurred first. For those invited to screening, the study entry date was the date of the scheduled screening examination. In the controls, each individual was assigned a study entry date evenly distributed throughout the screening period.21
All CRC cases (included screen-detected CRC) diagnosed from study entry date until 31 December 2011 were included in the primary analysis of CRC incidence. CRC cases detected at screening were excluded from the analysis in estimates of relative risk of CRC after screening in the serrated polyp group compared with the advanced and non-advanced adenoma groups.
To assess different polyp characteristics as risk factors for CRC, we fitted a multivariate logistic regression model with CRC as the outcome and serrated polyp ≥10 mm (present vs absent) and adenoma characteristics as binary covariates: size (<10 mm vs ≥10 mm), low-grade versus high-grade dysplasia, tubulous versus tubulovillous or villous histology and multiplicity (<3 adenomas vs ≥3 adenomas). The model was also adjusted for age and sex. Goodness of fit was tested with the Hosmer–Lemeshow test.26 We calculated the κ statistics to assess interobserver agreement in histopathological classification.27 We compared categorical variables using χ2 statistics and continuous variables using Mann–Whitney U test. All tests were two-sided, and p<0.05 was considered statistically significant. We used STATA V.13.1 (StataCorp LP, Texas, USA) for statistical analyses.
The NORCCAP trial is approved by the Norwegian Data Inspectorate and the Regional Ethics Committee of South-East Norway, and is registered at clinicaltrials.gov (NCT00119912). All screening participants provided written informed consent at screening. The present study was waived any additional approval from the Regional Ethics Committee.
Results
Descriptive characteristics
In NORCCAP, 20 572 individuals were invited to screening and 78 220 were assigned to the control arm (figure 1). Among 12 955 screening attenders, we identified 103 (0.8%) with at least one large serrated polyp. Of these, 22 had concomitant advanced adenomas (including two patients diagnosed with CRC at screening or during follow-up) and were categorised in the advanced adenoma group. Thus, the serrated polyp group comprised 81 individuals of whom four (4.9%) fulfilled WHO criteria for serrated polyposis syndrome.23 The non-advanced adenoma group comprised 1488 individuals, the advanced adenoma group 701 individuals and the polyp-free group 10 685 individuals (figure 1).
Descriptive characteristics are presented in table 1.
Screening characteristics of the study groups
Among the 81 individuals in the serrated polyp group, we detected 450 polyps at screening: 51 non-advanced adenomas and 399 serrated polyps. The serrated polyps were further classified as HP in 139 (35%), SSA/P in 169 (42%), TSA in 1 (0.3%) and unclassified in 90 (23%) cases. The pathologist interobserver agreement for serrated polyps was 62.3% (κ: 0.35) when all four subgroups were included and 66.6% (κ: 0.34), both ‘fair’ agreement, when we excluded TSA and unclassified serrated polyps. The interobserver agreement was 97.8% (κ: 0.93, almost perfect agreement) in separating adenomas from serrated polyps. Forty-nine individuals (60.5%) had synchronous HP and SSA/P at screening, 18 individuals (22.2%) had SSA/P only and 10 individuals (12.3%) had only HP. A detailed description of polyps detected at screening is displayed in tables 2 and 3.
Polyp location, median size and median number at screening among 81 individuals with serrated polyps
Diagnosis and localisation of the large serrated polyps (≥10 mm) at screening
CRC incidence
During a median follow-up of 10.9 years, three individuals (3.7%) in the serrated polyp group were diagnosed with CRC. The CRC incidence rate was highest in the serrated polyp group and lowest in the polyp-free group (table 4). Compared with the control arm, the HR for CRC was 2.5 (95% CI 0.8 to 7.7) in the serrated polyp group and 2.0 (95% CI 1.3 to 2.8) in the advanced adenoma group (table 4). The difference in HR in the serrated polyp group and the advanced adenoma group was not statistically significant, p=0.7. Compared with the polyp-free group, the HR for CRC in the serrated polyp group was 4.2 (95% CI 1.3 to 13.3). In the multivariate logistic regression model, having a serrated polyp ≥10 mm was an independent risk factor for CRC (OR 3.3; 95% CI 1.3 to 8.6) (table 5).
Number of individuals, colorectal cancer cases and person-years, age-standardised rates, time to diagnosis after screening and HRs, with 95% CI for colorectal cancer after median 10.9 years of follow-up in the different study groups.
Polyp characteristics as risk factors for colorectal cancer
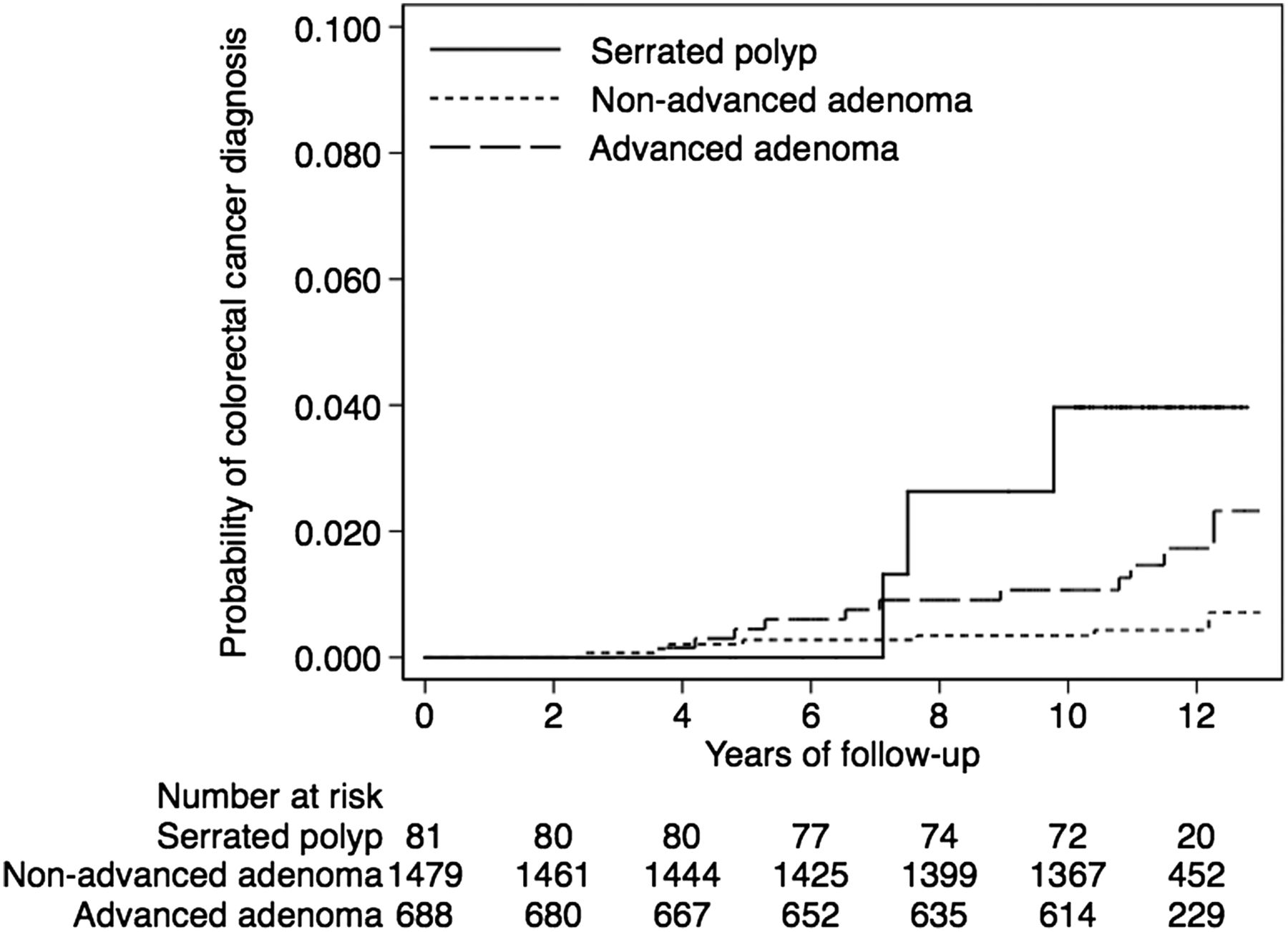
Median time to CRC diagnosis after screening in the serrated polyp group was 7.5 (range 7.1–9.8) years, and 7.1 (range 3.7–12.3) years in the advanced adenoma group. The HR for CRC after screening (excluding screen-detected CRC) was 3.2 (95% CI 0.9 to 11.4) in the serrated polyp group compared with the advanced adenoma group and 9.6 (95% CI 2.5 to 37.7) compared with the non-advanced adenoma group (figure 2). The results were comparable when we adjusted for differences in surveillance recommendations between the groups.

{kind=link}
{kind=link}
Cumulative risk of colorectal cancer (CRC) in individuals without CRC at screening in the serrated polyp group, the non-advanced adenoma group and the advanced adenoma group. The table denotes the number of individuals at risk.
One of the three cancers in the serrated polyp group was located proximal to the descending colon and two in the rectum. Location of the large serrated polyps detected at screening were related to location of the CRC in one patient with rectal CRC (unclassified serrated polyp), but not in the other two CRCs (both SSA/P). All three cancers were detected due to symptoms. None of these patients fulfilled the criteria for serrated polyposis syndrome. The median number of serrated polyps at screening was five (range 5–13) in those who developed CRC, compared with four (range 1–19) in those without CRC (p=0.1). Two cases of CRC were found among 67 individuals (3.0%) with SSA/P at screening and one among 14 individuals (7.1%) with serrated polyps other than SSA/P (p=0.4).
Colonoscopy after screening
By September 2012, three individuals in the serrated polyp group had been diagnosed with CRC, and six individuals had died. The remaining 72 individuals were invited for colonoscopy and 52 of them (72%) attended (see online supplementary figure S1). No additional CRC was detected. Of the 29 individuals who did not attend colonoscopy in 2012, 11 had at least one colonoscopy after screening. Thus, 63 individuals (78%) had at least one (range 1–4) postscreening colonoscopy. The median time to first colonoscopy after screening was 10.9 years (range 2.6–13.5). Caecum intubation rate was 95%. Apart from the three CRCs, SSA/P was found in 29 (46.0%) individuals, of whom five had low-grade dysplasia, and seven (11.1%) individuals had advanced adenomas.
Natural history of large serrated polyps
In 24 individuals, serrated polyps ≥10 mm found at screening were only biopsied and left in situ. One of these individuals developed CRC during follow-up, but in another colon segment than that of the polyp left in situ. Twenty-one individuals with 23 large serrated polyps (5 HP, 11 SSA/P without dysplasia, 2 SSA/P with low-grade dysplasia and 5 unclassified serrated polyps) had at least one colonoscopy after screening (table 6). Median time to first colonoscopy after screening was 11.0 years (range 6.1–12.7). In eight individuals, no remnants or other polyps were found in the same bowel segment as the large serrated polyp biopsied at screening. In six individuals, the polyp at follow-up was smaller than the screen-detected polyp; in three cases, the polyp was of equal size, and five polyps had increased in size. In one individual, there was no information of polyp size at follow-up. Two SSA/P with low-grade dysplasia at screening were found and removed at follow-up after 12.0 and 12.4 years; the size had increased (14 and 20 mm at screening; 20 and 25 mm at follow-up, respectively), but dysplasia was still classified as low grade. Only one individual developed new dysplastic features (low-grade dysplasia) in the polyp left in situ. Detailed information is available in the online supplementary table S1.
Findings at follow-up colonoscopy after median 11 years in 21 individuals with 23 large serrated polyps left in situ: n denotes the number of large serrated polyps
Discussion
This large, prospective study provided several salient findings. First, individuals with large serrated polyps have an increased risk for CRC during long-term follow-up: 3.7% developed CRC within 10.9 years, a risk 2.5 times higher than the general population and four times as high as for individuals with no polyps at screening. Second, the excess risk for CRC is at least as high as for individuals with advanced adenomas. And third, most large serrated polyps seem to have an indolent course, and cancer may not develop through progression of the large serrated polyp, but arise elsewhere in the colon of patients with such lesions.
This study is the largest follow-up study of CRC risk in individuals with large serrated polyps. Previously, one study reported on 40 individuals with non-dysplastic SSA/P. After 1–15 years, five (12.5%) developed CRC.28 In another retrospective study, 33 individuals with SSA/P or mixed SSA were followed for 5 years, and one patient (5%) developed CRC.29 In a third retrospective study, two of 38 (5%) individuals with dysplastic SSA/P developed CRC, but follow-up time in this study was not reported.30 Our estimate of absolute CRC risk is lower, but direct comparison is difficult due to different length of follow-up and inclusion criteria.
Strengths of our study include its population-based prospective design, high compliance, complete follow-up, and access to valid comparison groups to estimate relative cancer risk. Access to previous colonoscopy reports enabled meticulous endoscopic examination at follow-up, and validated histopathological classification of all potential precursor lesions are additional strengths. A main limitation of our study is its low statistical power due to few individuals with large serrated polyps, resulting in rather wide CIs around the HR point estimates for patients with serrated polyps. A power calculation based on the observed CRC risk in the polyp-free group and the serrated polyp group, gives an actual power of 0.63. Another limitation is that the polyps in this study were detected in a flexible sigmoidoscopy screening trial, and even if about 20% of screenees had colonoscopy at screening,19 some patients with proximal lesions may have been missed and, thus, misclassified as polyp-free. Hence, even use of polyp-free individuals as the reference group might generate a conservative estimate of the excess CRC risk associated with large serrated polyps, although an opposite mechanism is theoretically possible as described by the Will–Rogers phenomenon.31 However, a preliminary report from a large retrospective study from Denmark comparing CRC risk in individuals with SSA/P with individuals with adenomas identified at colonoscopy support our findings.32 As in any study including participants based on active search for a lesion, our observation may be prone to length-time bias: screening-detected polyps may be slow-growing with low malignant potential and have a higher chance of being detected endoscopically than aggressive lesions which grow faster. This would underestimate the risk of malignant transformation of polyps. Finally, our study cannot answer if the natural history of unresected large proximal serrated polyps without a distal serrated polyp or adenoma differ from proximal large serrated polyp with a distal serrated polyp or adenoma. Thus, whether the natural history of proximal, large serrated polyps is different from distal, large serrated polyps remains unknown.
While HP is the most frequent of the serrated polyps, SSA/P is considered to have a higher malignant potential. However, the distinction between HP and SSA/P may be difficult since criteria of the two lesions are often difficult to ascertain in small biopsies and in specimens with suboptimal orientation. Thus, an expected modest interobserver agreement between the two participating pathologists diagnosing subgroups of serrated polyps was observed in this study as well as in others.23 ,33–36 Guidelines from the European Society of Gastrointestinal Endoscopy, therefore, recommend that all patients with serrated polyps 10 mm or larger (irrespective of HP or SSA/P histology) should be regarded at high risk for CRC and receive surveillance.11 Our results support this recommendation. We suggest that individuals with large serrated polyps (including HP, SSA/P with or without dysplasie and TSA should be referred to as advanced serrated polyps indicating an increased risk for CRC, but acknowledge that low statistical power and concomitant presence of different serrated polyps preclude us from drawing firm conclusions about risk in subgroups of serrated polyps.
The time for progression from serrated polyp to CRC is not established. Case reports have suggested that it may be short,14 ,37 ,38 while larger studies suggest longer intervals. Three studies have indicated that the time from an individual is diagnosed with SSA/P to a diagnosis of CRC may be 7–15 years.15 ,16 ,28 In our study, the first CRC in the serrated polyp group was diagnosed 7.1 years after the last screening examination, and the median time from screening to diagnosis of CRC was 7.5 years. Additionally, our observation that large serrated polyps may be left in situ for more than 10 years without malignant transformation with only minimal growth, may support longer surveillance intervals than the currently recommended 3 years. This conclusion is, however, limited by the small number of polyps left in situ (n=23). In a study from the Mayo clinic, the 10-year risk of CRC at the site of an unresected polyp was 8%.39
The observed indolent course of the large serrated polyps left in situ raises the important question whether the future risk of CRC is related to the polyp per se or if large serrated polyps are just markers of excess CRC risk (field effect). We found that 63% of individuals with a large serrated polyp had a concurrent adenoma and 21% a concurrent advanced adenoma, a considerably higher prevalence than the 30.2% and 5.7% found in a recent systematic review.40 Additionally, 56% of our individuals had three or more serrated polyps at screening, indicating that serrated polyps may be associated with multiplicity, a finding in line with previous reports.41 ,42 High level of methylation of Cytosin-rich promoter regions (CpG island methylator phenotype, CIMP) is associated with increasing size of serrated polyps4 and with size and villousness of adenomas.3 ,43 Thus, individuals with large serrated polyps appear prone to develop other serrated and adenomatous polyps, suggesting a ‘serrated environment’ in the colorectum which may be a driving force in both the adenoma–carcinoma pathway and the serrated pathway. Indeed, individuals with both serrated polyps and adenomas have been found to have larger serrated polyps, and larger and more advanced adenomas compared with individuals with only one kind of polyp.18 However, when we adjusted for characteristics of concomitant adenomas, a large serrated polyp was an independent risk factor for CRC. Finally, large serrated polyps may be a surrogate marker for fast-growing de novo CRC.
The question whether the CRC risk is related to the large serrated polyp per se or is merely a marker of future risk of CRC is more relevant than ever, as serrated polyps are detected at an increasing rate, probably due to awareness,44 and guidelines recommending that all serrated polyps should be removed. This raises concerns about polypectomy complication rates, as most serrated polyps are located in the proximal colon where the bowel wall is thin and the risk of serious complications like bleeding and perforation are higher.45–48 According to our results, most large serrated polyps have an indolent course. Resection of all these lesions may thus be unnecessary, only exposing individuals to increased risk of complications without adding any benefit.49 Complications may indeed outweigh the benefit in a CRC screening programme. Biopsy sampling of lesions with a high risk for polypectomy complications may be an alternative. At removal of the serrated lesion left in situ, we found no indication of long-lasting post-biopsy fibrosis. All polyps were successfully removed by endoscopic mucosal resection. However, the validity of this approach has not been investigated, and the rate of sampling error by biopsy of serrated polyps is unknown.
In conclusion, we show that individuals with large serrated polyps have an excess risk of CRC. The risk is comparable with individuals with advanced adenomas. Having a large serrated polyp is an independent risk factor for CRC. However, even large serrated polyps may have an indolent course and may regress or disappear. Most large serrated polyps may not be precursor lesions per se, but merely a biomarker for increased risk of CRC.
Acknowledgments
The authors wish to thank the staff at the pathology departments at Telemark Hospital, Oslo University Hospital Rikshospitalet and Oslo University Hospital Ullevål. We are also indebted to the staff at the endoscopy departments at Telemark Hospital and Oslo University Hospital Rikshospitalet.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Flowchart
- Data supplement 2 - Online table
Footnotes
-
Contributors ØH: Study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. MB: Study concept and design; acquisition of data; interpretation of data; critical revision of the manuscript for important intellectual content. ØK: acquisition of data, interpretation of data; critical revision of the manuscript for important intellectual content. MK: Study concept and design; interpretation of data; critical revision of the manuscript for important intellectual content. ML: interpretation of data; critical revision of the manuscript for important intellectual content. TJE: Study concept and design; acquisition of data; interpretation of data; critical revision of the manuscript for important intellectual content. EML, KG: Acquisition of data; interpretation of data; critical revision of the manuscript for important intellectual content. GH: Study concept and design; acquisition of data; interpretation of data; critical revision of the manuscript for important intellectual content. H-OA, Interpretation of data; critical revision of the manuscript for important intellectual content.
-
Funding The NORCCAP trial was funded by research grants from the Norwegian Government and the Norwegian Cancer Society. The work with the present study was funded by Sørlandet Hospital Kristiansand and by grants from South-East Regional Health Authorities of Norway, The Norwegian Fulbright Foundation, The Research Council of Norway (Grant no 224845/F11) and The Norwegian Cancer Society (Grant no HS02-2009-0082).
-
Competing interests MB is member of the European scientific advisory board of Exact Sciences and has received equipment for testing in scientific studies from Olympus, Fujinon, Falk Pharma and CCS Healthcare. ØH, ML, H-OA, MK, ØK, TJE, EML, KG and GH report no conflicts of interest.
-
Ethics approval Regional Ethics Committee of South-East Norway.
-
Provenance and peer review Not commissioned; externally peer reviewed.