Article Text

Abstract
Objective Hepatocellular carcinoma (HCC) is an infrequent yet critical event in primary biliary cirrhosis (PBC); however, predictive tools remain ill-defined. Our objective was to identify candidate risk factors for HCC development in patients with PBC.
Design Risk factor analysis was performed in over 15 centres from North America and Europe spanning >40 years observation period using Cox proportional hazards assumptions, logistic regression, and Kaplan-Meier estimates.
Results Of 4565 patients with PBC 123 developed HCC, yielding an incidence rate (IR) of 3.4 cases/1000 patient-years. HCC was significantly more common in men (p<0.0001), and on univariate analysis factors at PBC diagnosis associated with future HCC development were male sex (unadjusted HR 2.91, p<0.0001), elevated serum aspartate transaminase (HR 1.24, p<0.0001), advanced disease (HR 2.72, p=0.022), thrombocytopenia (HR 1.65, p<0.0001), and hepatic decompensation (HR 9.89, p<0.0001). As such, non-treatment with ursodeoxycholic acid itself was not associated with cancer development; however, 12-month stratification by biochemical non-response (Paris-I criteria) associated significantly with future risk of HCC (HR 4.52, p<0.0001; IR 6.6 vs 1.4, p<0.0001). Non-response predicted future risk in patients with early stage disease (IR 4.7 vs 1.2, p=0.005), advanced disease (HR 2.79, p=0.02; IR 11.2 vs 4.4, p=0.033), and when restricting the analysis to only male patients (HR 4.44, p<0.001; IR 18.2 vs 5.4, p<0.001). On multivariable analysis biochemical non-response remained the most significant factor predictive of future HCC risk (adjusted HR 3.44, p<0.0001).
Conclusions This uniquely powered, internationally representative cohort robustly demonstrates that 12-month biochemical non-response is associated with increased future risk of developing HCC in PBC. Such risk stratification is relevant to patient care and development of new therapies.
- AUTOIMMUNE LIVER DISEASE
- PRIMARY BILIARY CIRRHOSIS
- CHOLESTATIC LIVER DISEASES
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Hepatocellular carcinoma (HCC) is the fifth most common cause of cancer and the third most common cause of cancer-related death.
HCC usually arises in patients with underlying chronic liver disease, with an emphasis on surveillance of at risk individuals according to international consensus guidelines.
Primary biliary cirrhosis (PBC) is the most common of the autoimmune liver diseases, and patients are recognised to be at risk of HCC. Given its relative rarity, robust risk assessment has remained a challenge and is based often on single centre studies.
What are the new findings?
Using a uniquely powered international collaborative effort, we confirm that in PBC, men and those with advanced presenting disease develop HCC more frequently.
Although therapy with ursodeoxycholic acid does not affect HCC incidence, 12-month biochemical non-response represents the most significant risk factor for future development of HCC.
Biochemical non-response represents an independent and additive predictor across all risk groups in PBC.
How might it impact on clinical practice in the foreseeable future?
Identification of high risk patients according to patient gender, disease stage and biochemical response has the potential to facilitate more effective risk stratification.
The relatively low incidence among those who achieve adequate biochemical response, even in men and individuals with evidence of advanced presenting disease, questions routine HCC surveillance in well-treated patients.
In keeping with the current recommended use of biochemical surrogate endpoints in development of new therapies for PBC, our data lend support to a likely meaningful reduction in HCC risk for PBC patients who receive additional therapy that significantly improves their biochemical markers of disease activity.
Introduction
Primary biliary cirrhosis (PBC) is the most prevalent autoimmune liver disease, characterised by ductopenia, cholestasis and a risk of progressive liver fibrosis. Life expectancy is reduced in PBC and prognosis largely dictated by development of cirrhosis and portal hypertension,1–3 including for some the development of hepatocellular carcinoma (HCC). Given the relative infrequency of PBC compared to other chronic liver diseases, large scale, robust and representative analyses of HCC risk in PBC remain limited.
Presently, the majority of patients with PBC are treated with ursodeoxycholic acid (UDCA).1 ,4 Treatment benefit is best highlighted by applying biochemical stratification to therapy,3 ,5–9 and up to two-thirds of patients have an improved transplant-free/overall survival in this regard. However, there is a paucity of data with regard to biochemical response and modification of cancer risk in PBC.10 ,11 Consequently it remains unclear how much risk/benefit there is in performing HCC surveillance for patients with well-treated disease.12 Across the spectrum of liver disease generally, HCC incidence appears greatest among individuals with advanced fibrosis/cirrhosis, particularly men13; however, such observations in PBC frequently represent single centre studies, or are not immediately generalisable to Western practice.7 ,10 ,14–24 For example, a recent nationwide population survey from Japan identified a sex-specific contribution to HCC risk with respect to disease stage in Japanese patients with PBC.24
To address and overcome limitations to current knowledge and practice, we now describe the incidence of HCC across a global PBC cohort, with the specific aim of identifying predictive factors in a robust, statistically powered and internationally representative population. In so doing we document critical insight into challenges pertaining to long term patient follow-up, hepatocellular cancer susceptibility and disease outcome. Furthermore we identify a protective association in patients meeting specific biochemical endpoints that can be used to stratify HCC risk in the clinic setting.
Patients and methods
Study setting and design
We collected and analysed data from well-characterised patients with an established diagnosis of PBC,1 ,4 who had previously attended or were under current clinical follow-up between 1959 and 2012. Our catchment population comprised over 15 centres across the UK, Europe, the USA and Canada, as detailed elsewhere.25 Both UDCA-treated and non-treated individuals with an established diagnosis of PBC in accordance with European and American guidelines were eligible for inclusion. Individual centre datasets (ICDs) contained mostly prospectively collected follow-up data on patients from diagnosis and/or start of UDCA therapy. Upon study initiation, ICDs were transferred onto a standardised case record form formulated by the Global PBC Study Group committee and amalgamated onto a common ‘master’ database for downstream analysis. Individual clinical and laboratory characteristics pertained to gender, clinician reported age and date of PBC diagnosis, liver histology, UDCA treatment (start date, dosage and duration of therapy), anti-mitochondrial antibody serology, laboratory values (serum alanine transaminase, aspartate transaminase (AST), alkaline phosphatase, bilirubin, albumin and platelets) at PBC diagnosis and annually thereafter, date of HCC diagnosis, and liver transplantation and mortality status.
Baseline was set as the point of starting therapy for patients in receipt of UDCA ≥12 months; and the date of first centre visit in non-treated individuals. Adopted biochemical response criteria for this study were as previously documented; specifically those from Barcelona,6 Paris,5 ,8 Rotterdam11 and Toronto.9 Liver biopsy performed within 1 year of study entry was classified as baseline histological assessment. Tissue material was assessed for liver disease severity according to the Ludwig and Scheuer classification, and staged histologically as early (I/II) or late (III/IV). Any individual with evidence of cirrhosis before confirmed PBC diagnosis was classified as cirrhotic at baseline. Given that liver biopsy is no longer standard practice in PBC, advanced baseline disease was also deemed present according to clinical features (eg, hepatic decompensation) and/or biochemical indices as per the criteria established by ter Borg et al.26
Individual patient follow-up was as per centre-specific practice, which although slightly variable included a clinic review at a minimum of every 12 months in the absence of cirrhosis, and at 6-monthly intervals for patients with evidence of advanced disease. Surveillance for HCC was conducted according to accepted international protocols—specifically 6-monthly ultrasound ± serum α-fetoprotein quantification. Confirmatory diagnosis was as per (timeline specific) internationally accepted protocols, either: (a) histopathological confirmation; (b) two coincident imaging techniques (CT, MRI, or contrast-enhanced ultrasonography) showing a focal lesion >2 cm with arterial phase enhancement; or (c) one imaging technique showing a focal lesion >2 cm with arterial phase enhancement in the presence of an α-fetoprotein serum titre >400 ng/mL.
Quality control
Individuals were excluded from analysis if follow-up data were insufficient or unavailable (<6 months’ follow-up or <2 clinic visits recorded), the start date of treatment or the exact date of major clinical events was unknown, and in the event of confirmed past/concomitant hepatitis B (HBV) or hepatitis C virus (HCV) infection, Wilson disease, α-1 antitrypsin deficiency, hereditary haemochromatosis, alcoholic liver disease, or overt overlapping features with autoimmune hepatitis.
Completeness, plausibility and validity of the data were carefully verified (by PJT, WJL and BEH). Extensive efforts, including individual site-centre visits (WJL) with personalised objective review of historical medical charts, were undertaken to retrieve missing data. Data pertaining to all cohorts were collected through to the end of December 2012.
Statistical analysis
The primary endpoint of this study was defined as development of HCC, and patients without a clinical event in this regard were censored at date of last follow-up, liver transplantation or death. Univariate and multivariable Cox proportional hazards models were fit in order to assess the impact of individual covariates on the instantaneous rate of events, with time-to-event analysis also being ascertained through Kaplan-Meier estimates. In order to account for possible heterogeneity across centre-specific populations, analyses were further stratified by centre.
Data are presented using the median and IQR for continuous variables and a value of p<0.05 considered statistically significant. Analyses were conducted using SPSS Statistics V.22.0 (SPSS Inc, Chicago, Illinois, USA), and repeated in a multiple imputed database to validate findings and study any potential bias. SAS V.9.0 (SAS Institute, Cary, North Carolina, USA) was used to generate 10 imputed datasets before combining results and retesting of multivariable analysis.
Results
Characteristics of the patient population
Our study cohort comprised 4845 patients (figure 1A and see online supplementary table S1); however, those without clear documentation of HCC status (presence or absence thereof) during follow-up were exempt from further analysis, as were individuals diagnosed with HCC simultaneously or within 12 months of PBC diagnosis. Therefore the final working group consisted of 4565 patients with PBC (90% female), of which 123 developed evidence of HCC during their clinical course, yielding an actuarial incidence rate of 3.4 cases/1000-patient years (figure 1B).
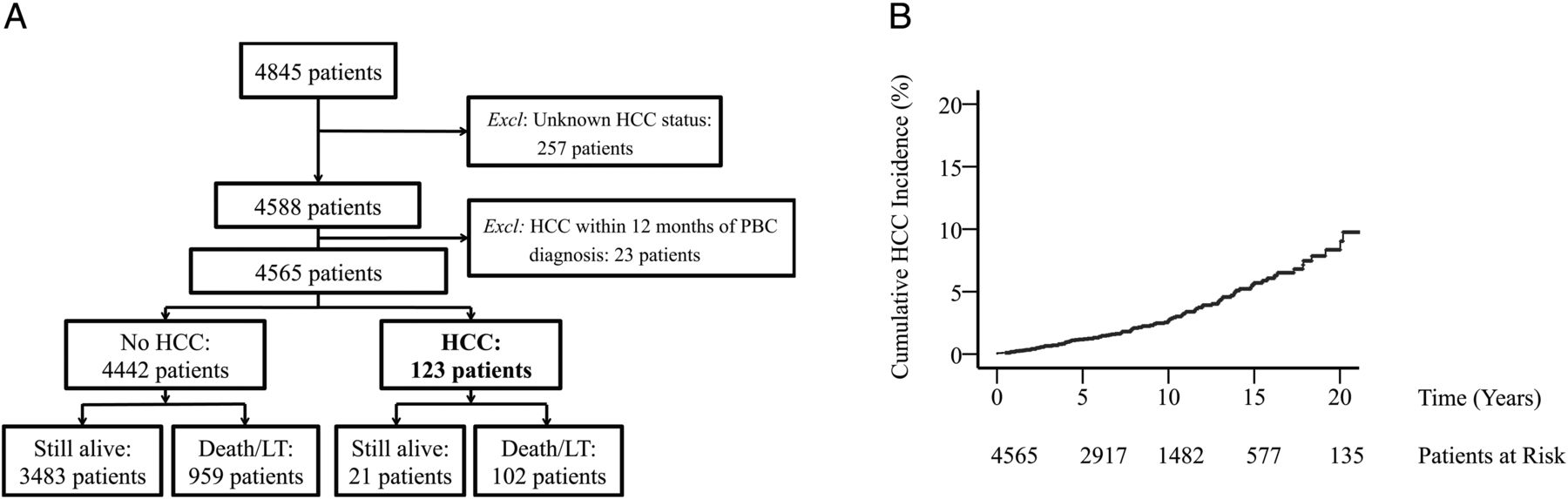
Study cohort. At time of analysis (A) data were available from 4845 patients; however, 257 patients were excluded because documentation of hepatocellular carcinoma (HCC) status (presence or absence thereof) was not present in medical records. A further 23 patients were excluded because they were diagnosed at the same time (within the first year) of primary biliary cirrhosis diagnosis, and identification of risk factors pertaining to HCC risk would have been inaccurate. The final study group therefore consisted of 4565 patients (B) of which 123 developed HCC over 36 577 patient-years.
In PBC, HCC incidence is increased in men and patients with advanced disease at baseline
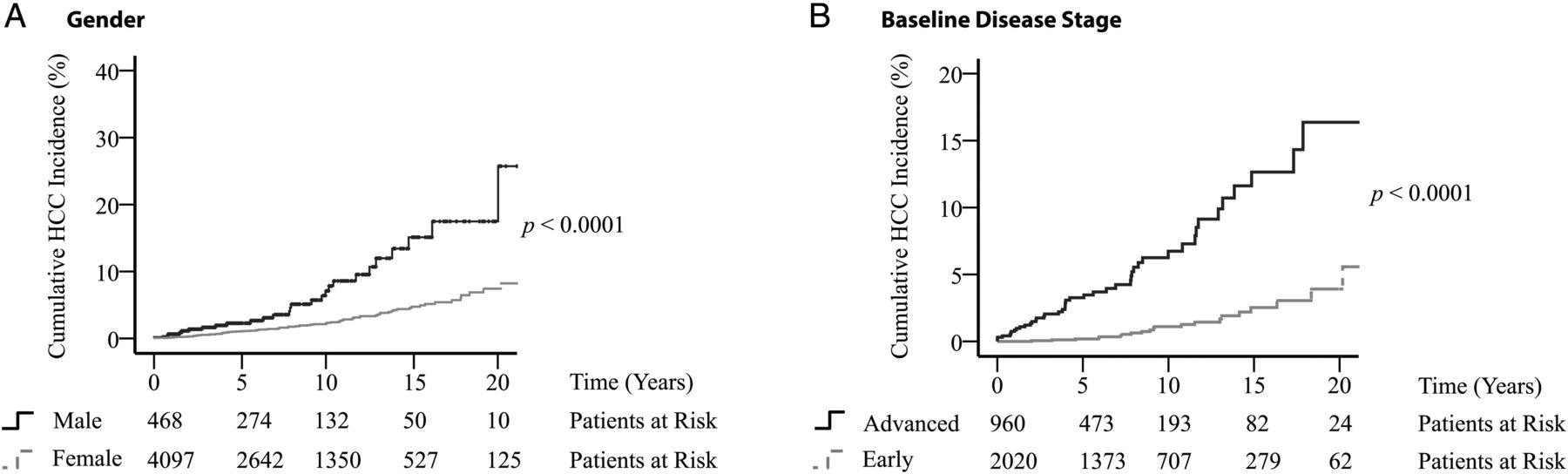
Development of HCC was associated with significantly poorer transplant-free and overall survival (HR 22.61, 95% CI 18.34 to 27.87; p<0.0001), and at baseline future risk of HCC was increased particularly in patients of male gender (figure 2A and online supplementary table S2) and those having moderate/late (advanced) biochemical disease (figure 2B). Men were observed to have a significantly greater incidence of HCC when analysis was restricted to patients with advanced disease (see online supplementary figure S1), and gender remained a significant risk factor following multivariable adjustment of baseline covariates (see online supplementary table S2). Subsequent transplant-free survival following development of cancer was not, however, different between men and women (see online supplementary figure S2).

Cumulative hepatocellular carcinoma (HCC) incidence according to gender and baseline primary biliary cirrhosis disease severity. Kaplan-Meier estimates of HCC incidence in: (A) men versus women, 6.7 vs 2.6 cases per 1000 patient-years; and (B) patients with moderate/late* (advanced) versus early disease, 7.6 vs 1.3 cases per 1000 patient-years. *According to criteria by ter Borg et al.26
Overall, the proportion of patients with histological evidence of advanced fibrosis at PBC diagnosis was also significantly greater in patients who developed HCC (p<0.0001); but the absence of baseline liver biopsy in many of our study group (n=2685) precluded further, more explicit analysis pertaining to histological characteristics.
Biochemical non-response predicts future risk of HCC in PBC patients
Overall, 96% (n=4361) of individuals remained under follow-up for a minimum of 12 months. Analysing this cohort in its entirety, 85% (n=3724) of patients were in receipt of UDCA therapy for ≥1 year—in keeping with the demographic of PBC treatment reported elsewhere.27 No significant difference between HCC appearance rates was observed, however, between treated versus untreated patients (p=0.972; online supplementary figure S3).
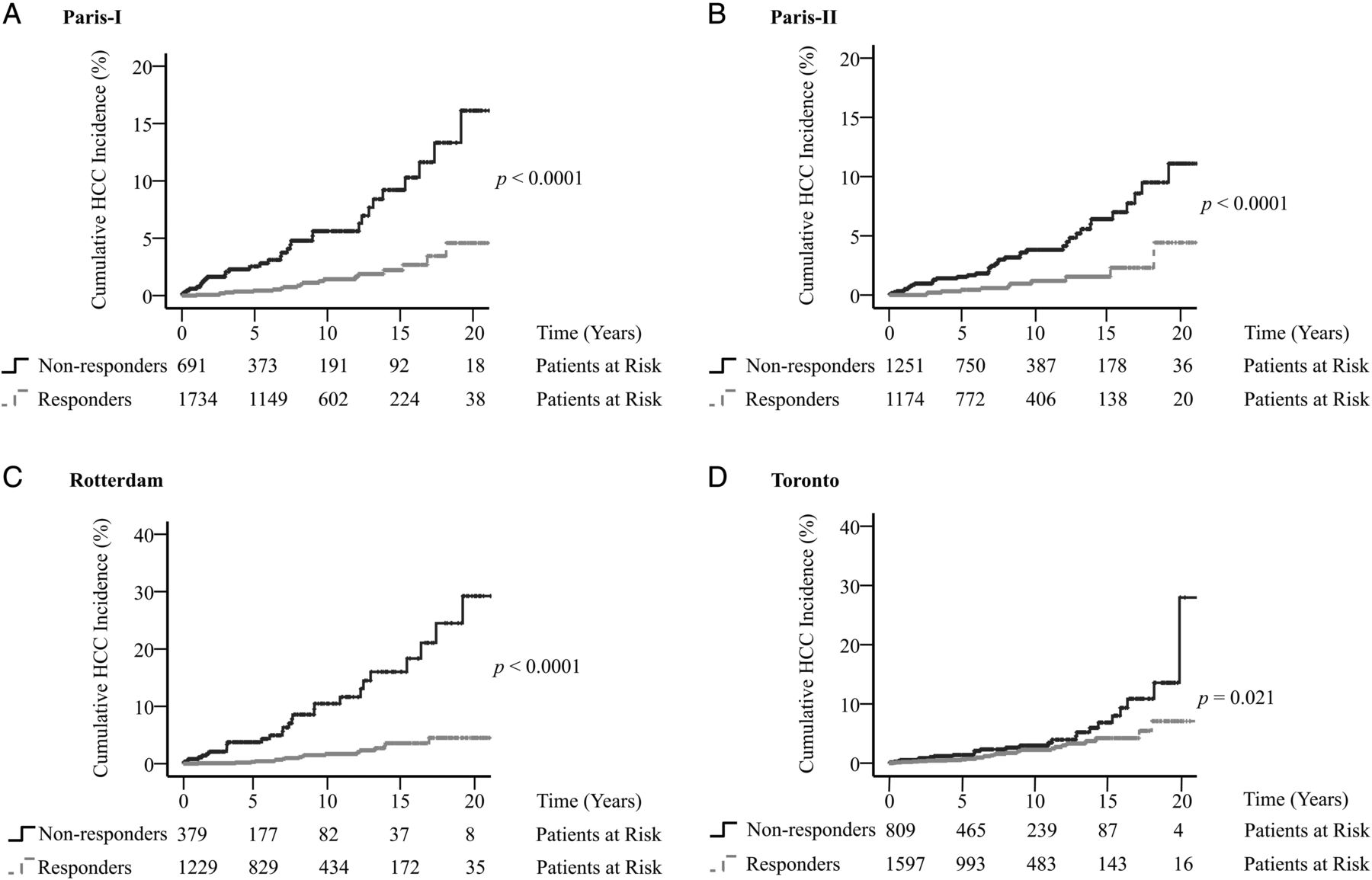
Twelve-month biochemical response (Paris-I) was calculable in 65% (n=2425) of all treated individuals and met by an inclusive 72% (n=1734). On univariate analysis HCC risk was observed to be significantly greater in biochemical non-responders according to Paris-I, Paris-II, Rotterdam and Toronto (table 1 and figure 3) but not Barcelona criteria (HR 1.48, 95% CI 0.93 to 2.36; p=0.099). Furthermore, biochemical non-response retained its predictive value when analysis was inclusive of patients not receiving UDCA (see online supplementary figure S4), and when extending the period over which response was assessed from 1 to 2 years (calculable in n=2725 (73%) of all UDCA-treated patients—HR 4.41, 95% CI 2.60 to 7.47; p<0.0001; online supplementary figure S5). Given that the most widely adopted criterion in clinical practice is Paris-I,3 ,27 ,28 this model is used to classify biochemical response in subsequent discussion unless otherwise specified.
Covariates associated with future hepatocellular carcinoma risk following 12 months of ursodeoxycholic acid (UDCA) treatment

Cumulative hepatocellular carcinoma (HCC) appearance rates according to biochemical response. Kaplan-Meier estimates of HCC incidence in biochemical non-responders versus responders as per the following criteria: (A) Paris-I, 6.6 vs 1.4 cases per 1000 patient-years; (B) Paris-II, 4.3 vs 1.2 cases per 1000 patient-years; (C) Rotterdam, 11.9 vs 1.8 cases per 1000 patient-years; and (D) Toronto, 4.5 vs 2.4 cases per 1000 patient-years. No significant differences were observed when biochemical response was stratified using Barcelona criteria (data not presented). Analysis restricted to ursodeoxycholic acid-treated patients only in whom 12-month biochemical data were available to calculate response (24 months in the case of Toronto criteria 9). Time measured in years following calculation of biochemical response.
Biochemical non-response predicts added HCC risk in men with PBC
Having identified that HCC developed more frequently in male patients compared to females, we next analysed the performance of biochemical response criteria specifically in men with PBC. Indeed, HCC incidence was greater in male non-responders versus responders (HR 4.44, 95% CI 1.29 to 10.20; p<0.001) (figure 4), and the former represented the group at highest future risk.
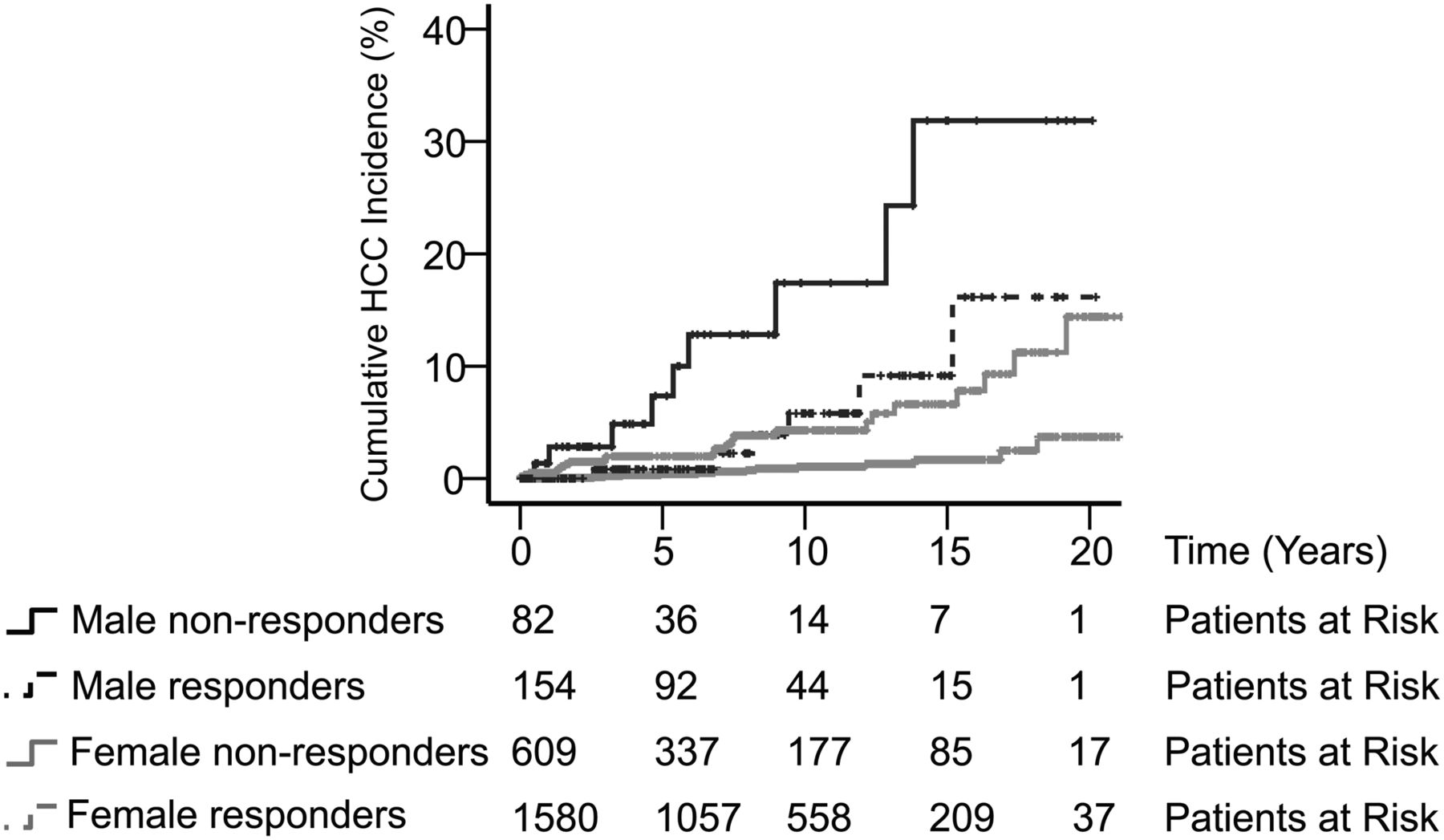
Hepatocellular carcinoma (HCC) incidence stratified according to gender and biochemical response. Kaplan-Meier plot comparing cumulative HCC incidence in male non-responders versus female non-responders (HR 3.70, 95% CI 1.71 to 8.00, p<0.001; 18.2 vs 5.2 cases per 1000 patient-years, log-rank p<0.001); male non-responders versus male responders (HR 4.44, 95% CI 1.29 to 10.20, p<0.001; 18.2 vs 5.4 cases per 1000 patient-years, log-rank p<0.001); male responders versus female non-responders (HR 0.90, 95% CI 0.36 to 2.21, p=0.811; 5.4 vs 5.2 cases per 1000 patient-years, log-rank p=0.766); female non-responders versus female responders (HR 4.74, 95% CI 2.44 to 9.22, p<0.0001; 5.2 vs 1.1 cases per 1000 patient-years, log-rank p<0.0001); and male responders versus female responders (HR 5.29, 95% CI 2.03 to 13.78, p<0.001; 5.4 vs 1.1 cases per 1000 patient-years, log-rank p=0.0001). Analysis conducted in ursodeoxycholic acid-treated patients only, for whom 12-month biochemical data were available to calculate response. Time measured in years following calculation of biochemical response.
Given that gender and advanced disease may adversely influence attainment of satisfactory biochemical response,27 ,29 an assessment of interaction terms was conducted. Although a greater proportion of men relative to women were observed to have advanced baseline disease (see online supplementary figure S1), no significant interactions between gender and disease stage (p=0.346), gender and biochemical response (p=0.285) or biochemical response and disease stage (p=0.690) were identified; thus strengthening the independent value of biochemical non-response in predicting future HCC risk.
Biochemical non-response predicts HCC risk irrespective of baseline PBC disease stage
As HCC most often develops on a background of severe fibrosis/cirrhosis—a factor associated with reduced biochemical response to treatment29—subsequent analysis focused exclusively on patients with evidence of advanced hepatic disease at time of PBC diagnosis. Within this inherently high risk population, stratification through biochemical response identified that the subgroup at greatest hazard of HCC fell into the non-response category (HR 2.79, 95% CI 1.18 to 6.94; p=0.02), whereas in biochemical responders of matched disease stage, development of HCC was much less apparent (figure 5A). Although fewer patients with advanced disease at baseline were exposed to UDCA therapy (see online supplementary table S3), when the cohort was extended to include non-UDCA-treated patients, biochemical non-response was still able to identify those at increased future HCC risk (see online supplementary figure S6A).

Hepatocellular carcinoma incidence in patients with varying disease stage stratified according to biochemical response. Kaplan-Meier estimate restricted to those with: (A) advanced presenting disease and biochemical non-response versus response, 11.2 vs 4.4 cases per 1000 patient-years; and (B) early presenting disease and biochemical non-response versus response, 4.7 vs 1.2 cases per 1000 patient-years. Analysis conducted in ursodeoxycholic acid-treated patients only in whom 12-month biochemical data were available to calculate response. Time measured in years following calculation of biochemical response.
Given reports of HCC developing in the absence of advanced fibrosis,15 ,24 thereafter we conducted an evaluation of risk factors exclusively in patients presenting with early-stage PBC at baseline. Across this subgroup, HCC developed infrequently and as a relatively late event (figure 5B and see online supplementary figure S6B); however, future HCC risk was observed to be significantly greater in patients who failed to achieve 12-month biochemical response (p=0.005).
Biochemical non-response remains the most significant predictor of future HCC risk in PBC
When performing a multivariable analysis of all hitherto identified risk factors—both those present at time of PBC diagnosis as well as over time—only thrombocytopenia and biochemical response retained statistical significance (table 1). This observation held true when extending the analysis to include patients not receiving UDCA as well as when the model was adjusted for centre-specific heterogeneity.
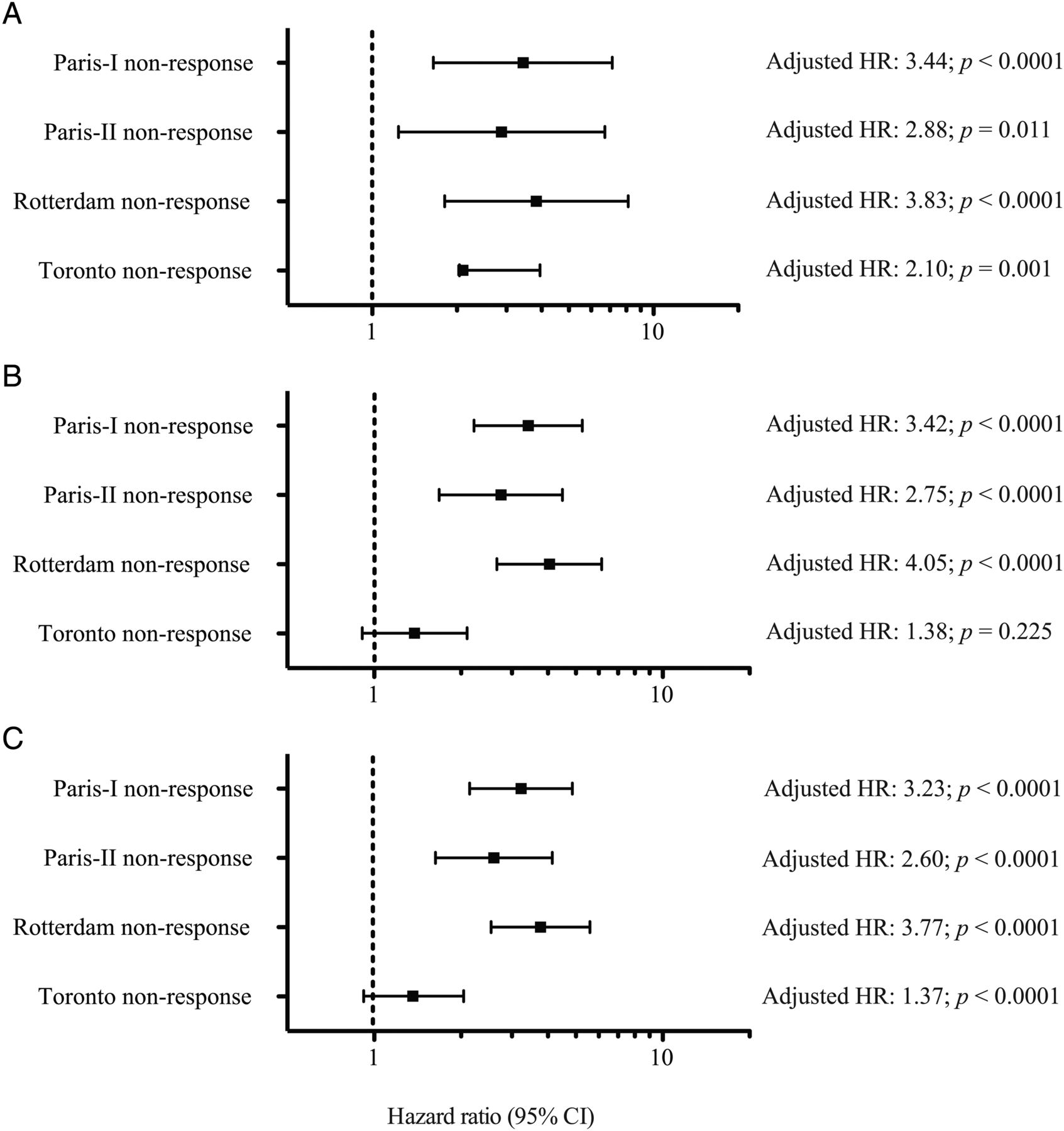
In order to confirm an absence of bias from missing data we next performed multiple imputation analysis (see online supplementary figure S7).30 In doing so, biochemical non-response was validated as an independent and significant predictor of future HCC risk (table 1 and figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparative (multivariable) evaluation of biochemical response in predicting hepatocellular carcinoma (HCC) risk. Performance of biochemical response criteria in predicting future HCC risk following: (A) individual multivariable analysis (stepwise backward model) adjusted for age at primary biliary cirrhosis diagnosis, sex, disease stage, hepatic decompensation, remaining laboratory parameters (not included in respective biochemical response criteria) and centre-specific heterogeneity; (B) analysis as in (A) following multiple imputation to correct for missing data values—ursodeoxycholic acid (UDCA) treated patients only; and (C) analysis as in (B) following inclusion of non-UDCA untreated patients in whom 12-month biochemical response criteria were calculable.
Discussion
We report a robust and uniquely powered evaluation of the largest internationally representative PBC cohort assembled to date, with the specific aim of identifying risk factors for HCC. In doing so we demonstrate that HCC is a critical event in the clinical course of PBC and associated with significantly poorer transplant-free survival. Although the incidence is significantly greater in male patients and those with advanced disease, 12-month biochemical non-response represents an independent and additive predictor for HCC, and on performing a comparative assessment of all identified covariates remained the most significant risk factor.
Historically, development of HCC in PBC was considered to be predominantly restricted to men, with a more variable correlation reported for disease stage.10 ,11 ,14 ,17 ,21 ,22 Initially perceived as a relatively rare complication, some report that the incidence is in fact comparable to chronic HCV infection,20 ,31 and indeed we found a similar frequency of HCC in PBC as previously documented.16 Larger, more contemporary reports also describe an association with male gender,24 as well as older age and advanced histological disease. However, the relatively low number of patients included in several earlier studies, as well as restricted geographical influence across others, have yielded many inconsistent results.
In agreement with preceding investigators we now robustly validate male sex as a risk factor,21 ,24 ,32 although on further analysis statistically significant differences between genders appear restricted to patients with advanced disease at presentation. Although suggestive that as a subgroup men are more likely to be diagnosed with PBC at a later stage,27 advanced disease was not found to be an interaction moderator in this regard. Prior studies have also documented relatively higher rates of past HBV infection and alcohol consumption in men.24 Despite being considered as exclusion criteria in our study, the complete distribution of past viral infection by gender across our global cohort could not be obtained, and viral serology would not have been routinely tested in patients diagnosed with PBC pre-1980. The reason for increased hepatocarcinogenesis in male patients across a disease with such overwhelming female predisposition remains unknown, although may be due to a lack of protective effect from oestrogen-mediated inhibition on specific cytokines such as interleukin-6.33 This however remains speculative.
In addition to male gender, advanced biochemical disease and thrombocytopenia were factors identifiable at PBC diagnosis associated with future risk of HCC—in keeping with many early reports wherein tumours developed exclusively on a background of late-stage disease.14 ,17 ,21 ,22 ,34 The majority of patients in our cohort received UDCA, and the effect of PBC-specific therapy with regard to HCC risk represented an understudied topic.10 ,11 UDCA therapy per se had no apparent effect on risk of HCC development across our cohort; but when stratifying according to several biochemical response criteria, patients classified as non-responders developed significantly more HCC during their clinical course. Indeed, risk was significantly greater in biochemical non-responders and this observation retained significance when inclusive of patients who never received UDCA but for whom categorisation of response was possible. It is likely therefore that achievement of biochemical response according to specific criteria—irrespective of whether this occurs in the context of therapy—infers a surrogate associated with improved HCC-free survival rather than a chemo-preventative effect of UDCA. The present evaluation not only validated findings of a previous much smaller study,11 but on performing a sub-analysis in patients identified as inherently high risk (men and those with advanced disease), biochemical non-response was associated with additional future risk of HCC. Indeed, on multivariable analysis only thrombocytopenia and biochemical non-response retained statistical significance and superseded the effect of gender and other tested parameters of disease stage. Of interest, platelet count is commonly employed as a surrogate of portal hypertension,35 and as part of the AST/platelet ratio has recently been validated as an independent and additive biomarker of transplant-free survival in biochemical responders.3 However, given the relatively small number of HCC observed in responding patients, sub-stratification of cancer risk in such regard would prove difficult.
The lower incidence in patients achieving biochemical response has practical implications for HCC surveillance (see online supplementary table S4), which at present is advocated for all chronic liver disease patients in which the annual incidence approaches or exceeds 1.5%.12 ,36 Specific to PBC, surveillance recommendations apply to all with advanced histological disease; however, in the present day clinical setting liver biopsy is rarely performed, and the advent of progressive imaging techniques makes tissue analysis rarely necessary in the ‘diagnostic work-up’ of suspected HCC.13 ,36 The use of transient elastography as an alternative risk marker of disease stage is also evolving,37 although due to limited availability still requires aetiology-specific validation. The prevalence of a globally aging population represents a further impending burden on healthcare services. In this regard, older age is increasingly recognised to confer additional HCC risk;38 ,39 the average age at time of HCC diagnosis being 67 years across our study population.
The emergence of well-substantiated treatment response criteria has allowed accurate prediction of transplant-free survival in patients with PBC,3 ,5–9 ,27 and herein we illustrate that failure to achieve the same biochemical endpoints confers increased HCC risk. Moreover, the relatively low incidence among those who achieve adequate biochemical response, even in men and individuals with evidence of advanced presenting disease, questions routine HCC surveillance in well-treated patients irrespective of gender and disease stage. Therefore, we recommend particular attention to: (1) male patients who either fail to achieve biochemical response (irrespective of disease stage), or in whom cirrhosis is already established (irrespective of biochemical response status); and (2) all female non-responders with evidence of advanced disease.
As with any longitudinal study evaluating long term outcomes, some patient data were inevitably not available during follow-up, whereas censoring at time of liver transplantation or death (free of HCC) may have led to pre-selection bias by restricting inclusion of patients who survive without transplant. However, such patients are no longer at risk of native liver HCC over time, and this approach is commonly adopted in studies where transplant-free mortality is not the primary endpoint. Moreover, all explanted livers were rigorously examined for the presence of HCC irrespective of transplant indication. In addition, our overall large sample size as well as validation of results through multiple imputation (table 1; figure 6 and online supplementary figure S7) demonstrate that any missing data have not introduced meaningful bias. Nevertheless, it is plausible that a proportion of patients who died during follow-up may have had undiagnosed HCC, and complete postmortem data in this regard are not possible to obtain. Another limitation to our study is that disease stage was assessed non-invasively for the most part—a reflection of the current standard of care in PBC. Further external validation of our results in this regard is important, albeit accepting the considerable challenges to long term prospective studies in PBC: slowly progressive and uncommon, with currently only one established treatment, and an absence of routine histological evaluation as part of standard clinical practice. We were also unable to obtain data pertaining to smoking status and comorbidities/coexisting extrahepatic autoimmune diseases40; however, many previous studies have failed to confirm an association with HCC in this regard.16 ,24 While the demography of our cohort is consistent with prior reports, we recognise that studies such as ours are heterogeneous with respect to referral practice between centres and countries. Opportunities therefore continue for large scale population studies in PBC to confirm our findings and better define strategies for clinical practice.
In conclusion, based on our results from the largest multicentre international study to date, we report that HCC is a rare yet critical event in the clinical course of PBC, and one associated with significantly poorer outcome. While the frequency of HCC was increased in men and those with advanced disease, biochemical non-response remained the most important risk factor, retaining predictive value independently and additively of disease stage and patient gender. Our globally representative data therefore add new knowledge to HCC risk in PBC and informs ongoing discussions about stratified treatment and surveillance. Additionally, given the potential use of surrogate endpoints in development of new therapies beyond UDCA, our data lend support to a meaningful reduction in HCC risk for PBC patients meeting specific biochemical response criteria.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
PJT and WJL are joint first authors.
BEH and GMH are joint senior authors.
↵† AKB deceased
Collaborators Tony Bruns, Ka-Kit Li, Teru Kumagi, Angela C Cheung, Nora Cazzagon, Ilaria Bianchi, Irene Franceschet, Kirsten Boonstra, Mohamad Imam, Giulia Pieri.
Contributors PJT,WJL, HRvB, BEH and GMH conceptualised the study. PJT and WJL performed data collection and analysis, wrote the first manuscript draft, revised text and figures to completion, and approved the final submission. HRvB, BEH and GMH supervised the study and contributed to data analysis, interpretation, presentation and approval of the final submission. AP, AF contributed to data capture, interpretation, presentation and approval of the final submission. HLAJ, PI, PMB, CYP, CC, RP, MJM, AKB, FN, ALM, TB, KL, KVK, TK, AC, AL, NC, IB, IF, LC, KB, MI, GP, PK, KDL contributed to data capture and approval of the final submission.
Funding PJT is a Wellcome Trust funded Clinical Research Fellow (099907/Z/12/Z). GMH is a co-investigator for UK-PBC (http://www.uk-pbc.com) supported by a Stratified Medicine Award from the UK Medical Research Council. This investigator-initiated study was supported by unrestricted grants from Intercept Pharmaceuticals and Zambon Nederland BV and was funded by the Foundation for Liver and Gastrointestinal Research in Rotterdam, the Netherlands. The supporting parties had no influence on the study design, data collection and analyses, writing of the manuscript, or on the decision to submit for publication.
Competing interests None.
Ethics approval This study was conducted in accordance with the Declaration of Helsinki and protocol reviewed and approved by the Institutional Research Board of the initiating centre (Rotterdam, the Netherlands), before circulation to individual participating hospitals for approval in accordance with local regulations.
Provenance and peer review Not commissioned; externally peer reviewed.