Article Text

Abstract
The risk of endoscopy in patients on antithrombotics depends on the risks of procedural haemorrhage versus thrombosis due to discontinuation of therapy.
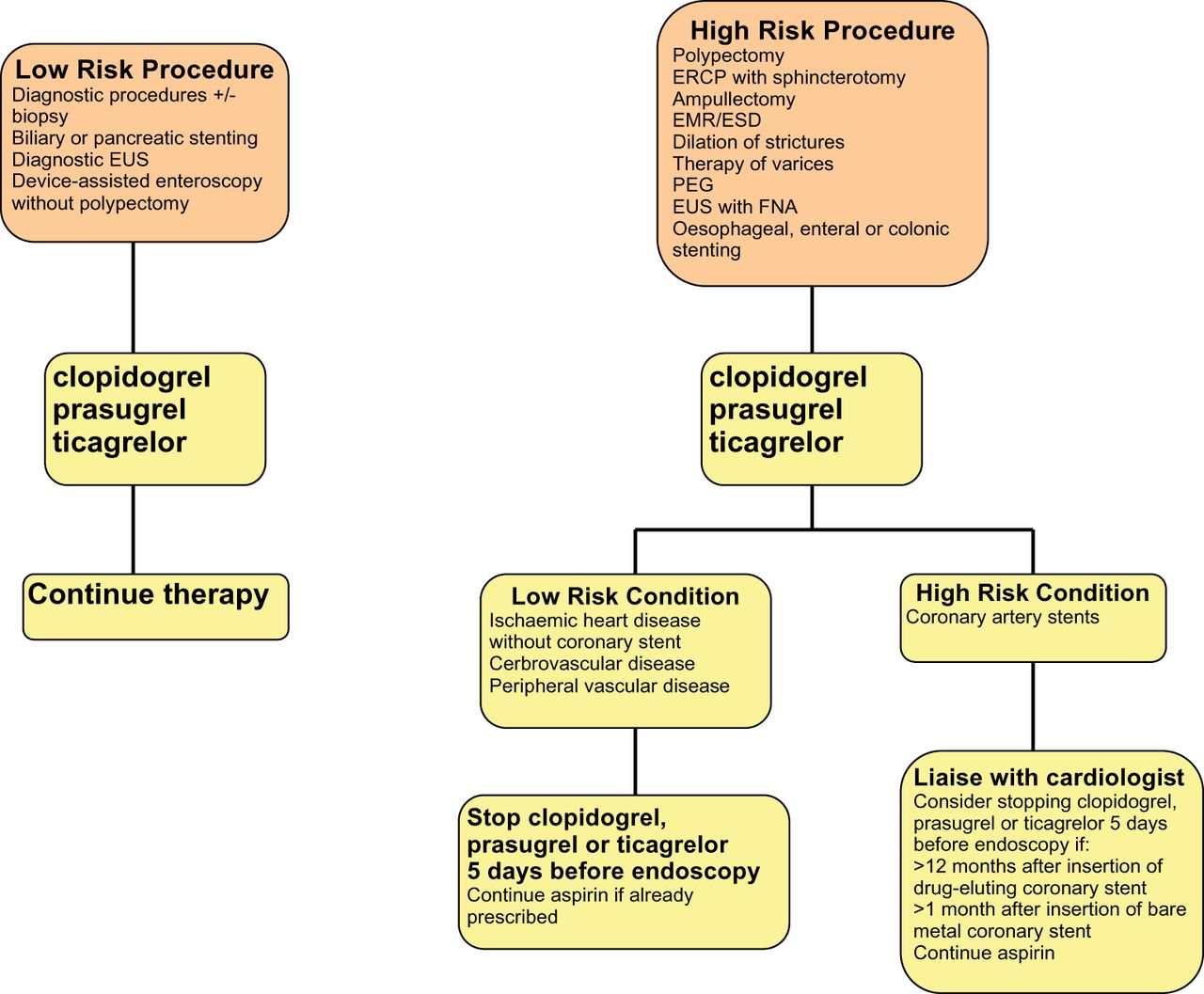
P2Y12 receptor antagonists (clopidogrel, prasugrel, ticagrelor) For low-risk endoscopic procedures we recommend continuing P2Y12 receptor antagonists as single or dual antiplatelet therapy (low quality evidence, strong recommendation); For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing P2Y12 receptor antagonists five days before the procedure (moderate quality evidence, strong recommendation). In patients on dual antiplatelet therapy, we suggest continuing aspirin (low quality evidence, weak recommendation). For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend continuing aspirin and liaising with a cardiologist about the risk/benefit of discontinuation of P2Y12 receptor antagonists (high quality evidence, strong recommendation).
Warfarin The advice for warfarin is fundamentally unchanged from British Society of Gastroenterology (BSG) 2008 guidance.
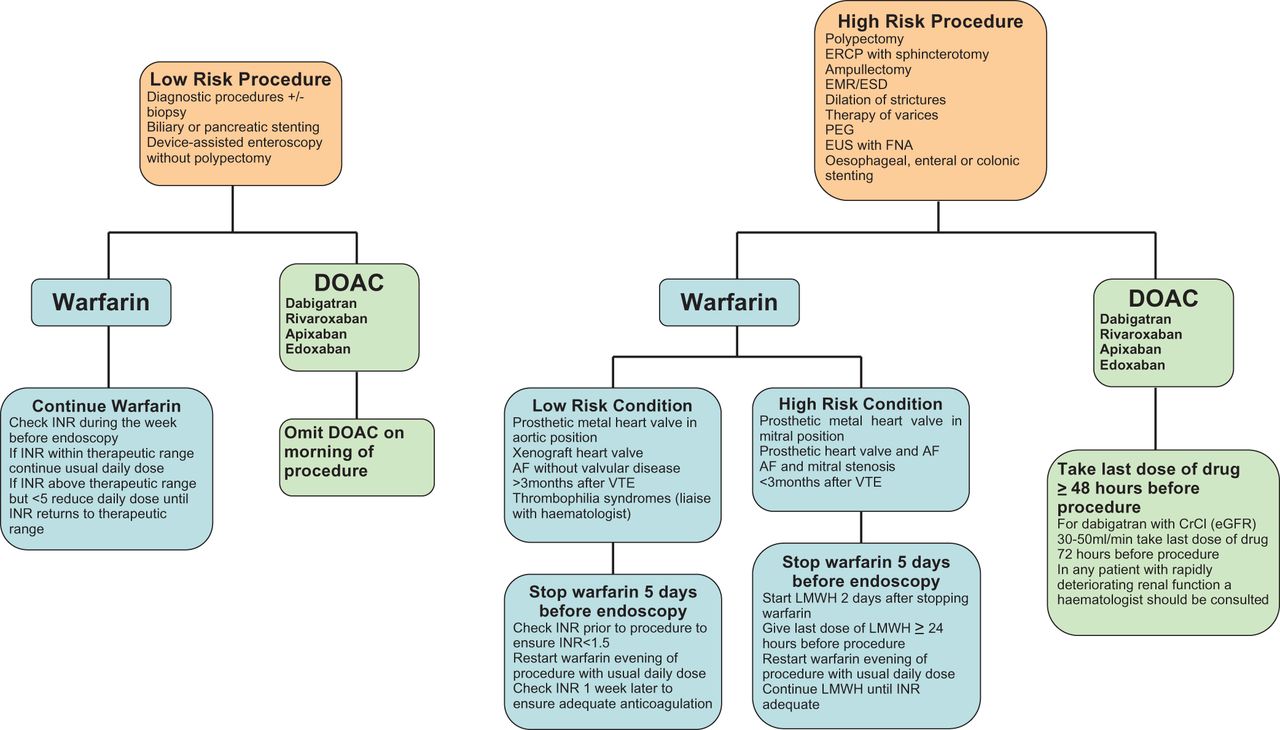
Direct Oral Anticoagulants (DOAC) For low-risk endoscopic procedures we suggest omitting the morning dose of DOAC on the day of the procedure (very low quality evidence, weak recommendation); For high-risk endoscopic procedures, we recommend that the last dose of DOAC be taken ≥48 h before the procedure (very low quality evidence, strong recommendation). For patients on dabigatran with CrCl (or estimated glomerular filtration rate, eGFR) of 30–50 mL/min we recommend that the last dose of DOAC be taken 72 h before the procedure (very low quality evidence, strong recommendation). In any patient with rapidly deteriorating renal function a haematologist should be consulted (low quality evidence, strong recommendation).
- ENDOSCOPY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
1.0 Summary of recommendations
These guidelines refer to patients undergoing elective endoscopic gastrointestinal procedures. Management of antiplatelet therapy and direct oral anticoagulants (DOACs) in acute gastrointestinal haemorrhage is discussed in detail in European Society of Gastrointestinal Endoscopy (ESGE) guidelines on the management of acute non-variceal upper gastrointestinal bleeding.1
Recommendations for the management of patients on antiplatelet therapy or anticoagulants undergoing elective endoscopic procedures are outlined in the algorithms in figures 1 and 2. Risk stratification for endoscopic procedures and antiplatelet agents (APAs) are detailed in tables 1 and 2. There is no high-risk category of thrombosis for DOACs as they are not indicated for prosthetic metal heart valves. Warfarin risk stratification is detailed in table 3. Our recommendations are based on best estimates of risk:benefit analysis for thrombosis versus haemorrhage. When discontinuing antithrombotic therapy, patient preference should be considered as well as clinical opinion: the risk of a potentially catastrophic thrombotic event such as a stroke may not be acceptable to a patient even if that risk is very low.
Risk stratification of endoscopic procedures based on the risk of haemorrhage
Risk stratification for discontinuation of clopidogrel, prasugrel or ticagrelor based on the risk of thrombosis
Risk stratification for discontinuation of warfarin therapy with respect to the requirement for heparin bridging

Guidelines for the management of patients on P2Y12 receptor antagonist antiplatelet agents undergoing endoscopic procedures.

{kind=link}
{kind=link}
Guidelines for the management of patients on warfarin or direct oral anticoagulants (DOAC) undergoing endoscopic procedures.
For all endoscopic procedures we recommend continuing aspirin (moderate evidence, strong recommendation), with the exception of endoscopic submucosal dissection (ESD), large colonic endoscopic mucosal resection (EMR) (>2 cm), upper gastrointestinal EMR and ampullectomy. In the latter cases, aspirin discontinuation should be considered on an individual patient basis depending on the risks of thrombosis versus haemorrhage (low quality evidence, weak recommendation).
1.1 Low-risk procedures
For low-risk endoscopic procedures we recommend continuing P2Y12 receptor antagonists (eg, clopidogrel), as single or dual antiplatelet therapy (low quality evidence, strong recommendation).
For low-risk endoscopic procedures we suggest that warfarin therapy should be continued (low quality evidence, weak recommendation). It should be ensured that the International normalised ratio (INR) does not exceed the therapeutic range in the week prior to the procedure (low quality evidence, strong recommendation).
For low-risk endoscopic procedures we suggest omitting the morning dose of DOACs on the day of the procedure (very low quality evidence, weak recommendation)
1.2 High-risk procedures
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing P2Y12 receptor antagonists (eg, clopidogrel) five days before the procedure (moderate quality evidence, strong recommendation). In patients on dual antiplatelet therapy, we suggest continuing aspirin (low quality evidence, weak recommendation).
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing warfarin 5 days before the procedure (high quality evidence, strong recommendation). Check INR prior to the procedure to ensure <1.5 (low quality evidence, strong recommendation).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend continuing aspirin and liaising with a cardiologist about the risk/benefit of discontinuing P2Y12 receptor antagonists (eg, clopidogrel) (high quality evidence, strong recommendation).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend that warfarin should be temporarily discontinued and substituted with low molecular weight heparin (LMWH) (low quality evidence, strong recommendation).
For all patients on warfarin we recommend advising that there is an increased risk of post-procedure bleeding compared to non-anticoagulated patients (low quality evidence, strong recommendation).
For high-risk endoscopic procedures in patients on DOACs, we recommend that the last dose of DOACs be taken at least 48 h before the procedure (very low quality evidence, strong recommendation). For patients on dabigatran with a CrCl (or estimated glomerular filtration rate (eGFR)) of 30–50 mL/min we recommend that the last dose be taken 72 h prior to the procedure (very low quality evidence, strong recommendation). In any patient with rapidly deteriorating renal function a haematologist should be consulted (low quality evidence, strong recommendation).
1.3 Post endoscopic procedure
If antiplatelet or anticoagulant therapy is discontinued, then we recommend this should be resumed up to 48 h after the procedure depending on the perceived bleeding and thrombotic risks (moderate quality evidence, strong recommendation).
2.0 Origin and purpose of these guidelines
Anticoagulants and APAs are widely prescribed for a number of cardiovascular and thromboembolic conditions with established benefit to patients. These drugs confer an increased risk of haemorrhage when undertaking therapeutic endoscopic procedures, but also pose risks of thromboembolic sequelae if discontinued. The British Society of Gastroenterology (BSG) published guidelines on the management of anticoagulants and APAs in patients undergoing endoscopy in 20082 and the ESGE published guidelines on endoscopy and APAs in 2011.3 Both guidelines are due for revision, and the BSG and ESGE have cooperated to produce a joint guideline. Since the publication of the previous guidelines there has been an expansion in the use of the newer antiplatelet drugs, and new oral anticoagulant drugs have been introduced. The latter have been widely prescribed and pose particular problems for endoscopists with regard to haemorrhage; their effects are difficult to reverse in an emergency situation, and moreover some of these drugs are associated with a higher incidence of spontaneous gastrointestinal haemorrhage compared to warfarin.
3.0 Preparation of the guidelines
These guidelines were drafted by a working party comprising members of the BSG and ESGE, a haematologist, interventional cardiologist, and a patient representative from the charity AntiCoagulation Europe. Guidelines were prepared according to AGREE II principles4 and comply with the requirements of the National Institute for Health and Care Excellence (NICE). Clinical questions were formulated using the PICO (Patients, Interventions, Controls, Outcomes) system. Search strategies were delegated to authors with responsibilities for specific sections. Literature searches were conducted using PubMed and OVID Medline, Embase and Cochrane Library. Additional searches were conducted using Google. Literature searches were re-run in February 2015, and any additional relevant studies considered up to August 2015. Quality of evidence and strength of recommendations were determined by the authors and consensus achieved according to the GRADE system.5 After agreement on a final version, the manuscript was subjected to internal peer review and revision by the BSG and the ESGE and sent to all individual ESGE members and member societies prior to publication. Conflict of interest statements were submitted by all authors. This guideline was produced in 2015 and will be considered for review in 2019, or sooner if new evidence becomes available. This guideline has been co-published with permission in both Gut and Endoscopy.
4.0 Warfarin
For low-risk endoscopic procedures we suggest that warfarin therapy should be continued (low quality evidence, moderate recommendation). It should be ensured that the INR does not exceed the therapeutic range in the week prior to the procedure (low quality evidence, strong recommendation).
Tell the patient to continue warfarin and check the INR during the week before the endoscopy;
If the INR result is within the therapeutic range then continue with the usual daily dose;
If the INR result is above the therapeutic range, but less than 5, then reduce the daily warfarin dose until the INR returns to within the therapeutic range;
If the INR is greater than 5 then defer the endoscopy and contact the anticoagulation clinic, or a medical practitioner, for advice.
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing warfarin 5 days before the procedure (high quality evidence, strong recommendation). Check INR prior to the procedure to ensure <1.5 (low quality evidence, strong recommendation)
Stop warfarin 5 days before the endoscopy;
Check the INR prior to the procedure to ensure its value is <1.5;
On the day of the procedure restart warfarin with the usual daily dose that night;
Check INR one week later to ensure adequate anticoagulation.
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend that warfarin should be temporarily discontinued and substituted with LMWH (moderate quality evidence, strong recommendation).
Warfarin should be stopped 5 days before the procedure;
Two days after stopping warfarin commence daily therapeutic dose of LMWH;
Administer the last dose of LMWH at least 24 h prior to the procedure;
Check the INR prior to the procedure to ensure its value is <1.5;
Warfarin can be resumed on the day of the procedure with the usual dose that night;
Restart the daily therapeutic dose of LMWH on the day after the procedure;
Continue LMWH until a satisfactory INR is achieved.
For all patients on warfarin we recommend advising that there is an increased risk of post-procedure bleeding compared to non-anticoagulated patients (low quality evidence, strong recommendation).
Updated literature searches were conducted on the use of warfarin and heparin in patients undergoing endoscopy. Two studies of colonic polypectomy on warfarin for small polyps have been retrieved. A retrospective study of 223 polypectomies (<1 cm) in 123 patients on continued warfarin therapy found a rate of haemorrhage requiring transfusion of 0.8%. This was despite routine prophylactic clipping of polypectomies.6 In a randomised controlled trial (RCT) (159 polyps <1 cm in 70 patients) examining hot versus cold snaring of polyps in anticoagulated patients, the rate of immediate haemorrhage in the hot snare versus the cold snare group was 23.0% vs 5.7%, respectively, and that of delayed haemorrhage requiring intervention 14% vs 0%, respectively.7 These findings should be considered in the context that polyps have been found at colonoscopy in 22.5–32.1% of patients in large studies8 ,9 and up to 42% in a bowel cancer screening programme,10 many will be greater than 1 cm in size, and the rates of haemorrhage in the latter study above were greater than the 0.07–1.7% overall rates of haemorrhage reported in non-anticoagulated patients.9 ,11–14 Routine discontinuation of warfarin therapy may therefore be considered necessary in most colonoscopy services. Even when temporarily discontinued, warfarin therapy is associated with an increased risk of post-polypectomy bleeding (PPB)15 and patients should be advised of this.
For patients with non-valvular atrial fibrillation (AF), bridging of warfarin therapy with LMWH has not been recommended in previous guidelines.2 ,16 This policy has been tested in a large RCT of 1884 AF patients with peri-operative interruption of warfarin therapy, randomised to bridging with LMWH or placebo.17 Approximately half of these patients underwent endoscopic procedures. In the placebo group, there was no increase in thrombotic events, but in the heparin group there was an increase in major bleeding events. Both groups included patients with AF and mitral stenosis (MS) or CHADS218 scores of 5 or 6, situations considered at high risk of thrombotic events. The proportion of these patients was however low (≤2% for MS and ≤3.4% for CHADS2 5,6), and the study was not designed for this subgroup analysis. AF with MS is considered particularly high risk for thromboembolic events19 ,20 and remains in this category for these guidelines. There are insufficient data to make specific recommendations for patients with high CHADS2 scores undergoing endoscopy.
Retrospective studies of LMWH bridging for metal heart valves have suggested that this practice is safe with regard to thrombotic risk.21–23 Intravenous unfractionated heparin (UFH) is an alternative, and local cardiological advice may influence which is preferred. Bridging with UFH does, however, require a prolonged inpatient stay as warfarin is discontinued, and then restarted, to achieve satisfactory INR. Comparison of LMWH versus UFH for bridging for metal heart valves found no difference in adverse events between the groups in a multicentre registry study.24
Some patients with a personal or family history of venous thrombosis are found to have identifiable laboratory evidence of a predisposition, so called thrombophilia. In most cases the risk of venous thrombosis if anticoagulation is temporarily interrupted is not substantially different in patients with and without such abnormalities. Therefore, a thrombophilia does not indicate a high-risk condition per se and bridging with LMWH is not indicated when warfarin is interrupted. Factor V Leiden and the common prothrombin mutation F2G20210A are low-risk thrombophilias and bridging is not required. Patients with deficiencies of antithrombin, protein C or protein S are at higher risk of thrombosis, but in most of these patients bridging therapy will not be required. Thrombophilia syndromes have therefore been reclassified as low-risk conditions for the purposes of these guidelines, but we suggest that haematological advice is sought in these cases.
Apart from reclassification of the risk of thrombophilia, no new data were found to alter the recommendations for the use of warfarin or heparin stipulated in the 2008 BSG guidelines.2 Evidence was reviewed in its entirety and recommendations re-classified using GRADE.
5.0 Antiplatelet agents
For all endoscopic procedures we recommend continuing aspirin (moderate evidence, strong recommendation), with the exception of ESD, large colonic EMR (>2 cm), upper gastrointestinal EMR and ampullectomy. In the latter cases, aspirin discontinuation should be considered on an individual patient basis depending on the risks of thrombosis versus haemorrhage (low quality evidence, weak recommendation).
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing P2Y12 receptor antagonists (eg, clopidogrel) five days before the procedure (moderate quality evidence, strong recommendation). In patients on dual antiplatelet therapy, we suggest continuing aspirin (low quality evidence, weak recommendation).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend continuing aspirin and liaising with a cardiologist about the risk/benefit of discontinuing P2Y12 receptor antagonists (eg, clopidogrel) (high quality evidence, strong recommendation).
5.1 Aspirin
Aspirin is standard of care in patients with ischaemic heart disease. It reduces the mortality associated with acute myocardial infarction (MI) as well as the risk of fatal and non-fatal recurrent MI in patients with unstable coronary syndromes. It also reduces mortality and recurrent stroke in patients with acute cerebrovascular ischaemia. When given as long-term secondary prevention aspirin reduces vascular events by approximately one-third and vascular deaths by about one-sixth. Intra-platelet pathways can still be activated even in the presence of aspirin. Most patients who have suffered an acute coronary event will therefore be on dual anti-platelet therapy (DAPT), that is, aspirin plus an inhibitor of the P2Y12 receptor, either clopidogrel, prasugrel or ticagrelor.
In the context of endoscopy, aspirin monotherapy has been found to be safe in colonoscopic polypectomy and endoscopic sphincterotomy.25–28 Studies of aspirin in the context of ESD29 ,30 or large (>20 mm) colonic EMRs31–33 have found an increased risk of haemorrhage; EMR in the upper gastrointestinal tract confers a high risk of haemorrhage, but there are no studies on continuous aspirin therapy. The thrombotic risk to the patient should also be considered, particularly in those receiving aspirin for secondary prevention as they are at greater risk from discontinuation of therapy than those taking it for primary prevention. In patients on long-term low-dose aspirin for secondary prevention, aspirin interruption was associated with a three-fold increased risk of cardiovascular or cerebrovascular events, and 70% of these events occurred within 7–10 days after interruption.34 ,35 In an RCT of 220 patients on low-dose aspirin for secondary prevention undergoing non-cardiac surgery, patients were randomised to continuation or temporary replacement of aspirin by placebo (-7 to +3 days after surgery).36 Major cardiac events occurred within 30 days in 1.8% of the aspirin group compared to 9% in the placebo group (p=0.02). No difference in bleeding complications was seen between the two groups.
Haemorrhage secondary to high-risk endoscopic procedures can often be controlled by further endoscopic therapeutic measures, and is rarely fatal. A thrombotic stroke may result in lifelong disability, and a major cardiac event may result in death. The risks of thrombosis versus haemorrhage need to be assessed on an individual patient basis, and caution should be exercised if discontinuing aspirin when prescribed for secondary prevention of ischaemic or thrombotic events.
5.2 Clopidogrel
The interlinked processes of platelet deposition, adherence, and aggregation are central to the initiation of the process of thrombus formation in the arterial system. The trigger is arterial wall injury, either spontaneous with an acute plaque event (rupture or erosion) as in acute coronary syndromes (ACS) (ST-segment Elevation Myocardial Infarction: STEMI or non N-STEMI: N-STEMI), or when angioplasty and stenting are used to treat coronary narrowings. Uncontrolled activation of platelets when stent struts are still exposed can lead to occlusive thrombus and heart attack.
Clopidogrel is an inhibitor of ADP-induced platelet aggregation.37 Clopidogrel plus aspirin is more effective than aspirin alone at attenuating clinical events in acute, platelet-initiated, presentations.38 DAPT has a specific and critical role in preventing occlusion of coronary artery stents. Angioplasty and stenting is the standard of care for specific sub-groups of patients with stable angina, and is the default strategy in the vast majority of patients with ACS. Like that of aspirin, the antiplatelet action of clopidogrel is irreversible and platelet function has been demonstrated to return to normal 5–7 days after withdrawal of clopidogrel, based on the regenerative production of clopidogrel-naive platelets.39
5.3 Newer APAs
5.3.1 Prasugrel and ticagrelor
Newer, more potent and more rapidly acting agents than clopidogrel have become the standard of care in patients with ACS. The two new agents now available are prasugrel and ticagrelor. Prasugrel is a thienopyridine, like clopidogrel, whereas ticagrelor is a different class of agent and reversible. Prasugrel tends to be used in selected STEMI patients, ticagrelor in both STEMI and N-STEMI ACS patients as recommended by NICE in the UK.40 Both are recommended to be continued for 12 months after discharge, in combination with aspirin. Aspirin is continued for life thereafter.
5.3.2 Vorapaxar
Vorapaxar is the first of a new class of APA; it is a protease-activated receptor (PAR-1) antagonist that inhibits thrombin. It is indicated for preventing cardiovascular events in patients with a history of MI or peripheral arterial disease, and it is administered in addition to aspirin or DAPT.41–43 It is contraindicated in patients with a previous history of stroke, transient ischaemic attack or intracranial haemorrhage due to an increased risk of intracranial haemorrhage. Vorapaxar was approved by the US Food and Drug Administration in 2014, and by the European Medicines Agency in 2015. There are no data on the peri-operative or peri-endoscopic use of this drug, and specific recommendations have not been made at this time. Peri-endoscopic management of patients on this drug should be in consultation with a cardiologist or other specialist in cardiovascular disease.
5.4 Ischaemic heart disease and coronary artery stents
Patients with ischaemic heart disease are generally treated with antiplatelet therapy rather than anticoagulant therapy. Coronary artery stenting has increasingly become the dominant therapy for treating patients with coronary artery disease. Most of the exponential increase in the use of these drugs has been due to treating patients for ACS. Patients who have undergone revascularisation therapy with coronary artery surgery will tend to be prescribed aspirin alone, while those treated with stents for stable angina are generally treated with aspirin and clopidogrel for 12 months and then aspirin indefinitely. If they have had an episode of unstable angina with a troponin release they will be treated with the more rapidly acting and more potent, newer, agents, either prasugrel or ticagrelor. Therefore, unless a patient has presented with stable angina and has been treated with a bare metal stent (a minority of patients), they are likely according to current guidance to be treated for 12 months with either clopidogrel or one of the more potent P2Y12 inhibitors as part of their DAPT regimen.
To prevent stent thrombosis DAPT is prescribed for 12 months after drug-eluting stent (DES) deployment while bare metal stents, which are used in <10% of cases, require a minimum of 1 month DAPT. Following DAPT, lifetime aspirin should be prescribed for both types of stent.
DAPT that is, aspirin plus either clopidogrel, prasugrel or ticagrelor also increases the risk of bleeding,44–46 either spontaneously or when a non-cardiac interventional procedure is required: clopidogrel > aspirin alone, ticagrelor plus aspirin > clopidogrel plus aspirin and prasugrel plus aspirin > any of the other combinations although direct head to head studies comparing prasugrel with ticagrelor have not been reported.
5.5 Clinical consequences of DAPT
If patients develop dyspepsia on low-dose aspirin, or in any patient at risk from gastro-intestinal bleeding, co-prescription of a proton pump inhibitor should be considered initially. Failing that, and after discussion with a cardiologist, the patient taking aspirin alone could be given clopidogrel instead.
Should the patient spontaneously bleed or require a non-cardiac operative procedure within the recommended time period of DAPT administration, it may seem obvious to stop the DAPT but the clinical risks associated with stopping antiplatelet therapy are high. In one study which examined factors associated with stent thrombosis, discontinuation of therapy was associated with a HR of 161 for death and MI.47 Development of stent thrombosis carries an approximate risk of 40% for MI and death. The risk of stent thrombosis increases after 5 days without antiplatelet therapy; if clopidogrel needs to be temporarily stopped in the context of an acute gastro-intestinal haemorrhage then discontinuation of therapy should be limited to this interval.
Issues related to the need to consider discontinuation of DAPT for non-cardiac surgical procedures are complex and dependent on a number of potentially confounding factors.48 For patients with known high risk of needing a future non-cardiac surgical procedure (eg, planned future surgery for cancer) bare metal stenting will be undertaken because DAPT will only be required for 1 month. However this is valid for patients stented for stable conditions only since ACS patients currently still need 12 months DAPT. The variables around stent type and clinical indication, timing of need for non-cardiac operation and or bleeding make conversations with the interventional cardiologist imperative.
5.6 Developments in antiplatelet therapy
These include:
The introduction of the newer, more potent, P2Y12 inhibitors described above (prasugrel and ticagrelor);
The reversibility of one of these (ticagrelor) such that discontinuation may allow for an earlier procedure than for clopidogrel and prasugrel that have irreversible effects. Although platelet inhibition starts to reverse within 48 h it is still recommended that if clinically feasible 5 days should be allowed to lapse;
Newer DES (generation 3 DES) may need DAPT absolutely for only 3–6 months.49 There are a number of on-going trials comparing short duration (3 months) versus standard duration (12 months) of DAPT administration.50
If the patient has received DES for ACS then the recommendations are still that the DAPT (aspirin plus either prasugrel or ticagrelor) be maintained for 12 months, irrespective of DES type;
If, after discussion with a cardiologist, DAPT needs to be modified for a non-cardiac procedure during the 12 months following coronary stent insertion, then only the P2Y12 inhibitor should be discontinued (for 5 days prior to the procedure)—the aspirin should be continued;
The situation is further complicated by recent data (DAPT trial)51 which suggests that certain patients may benefit from an extension of their DAPT till at least 30 months. This study reported fewer ischaemic events in patients receiving DAPT up till 30 months than those discontinuing at 12 months, but at the cost of a higher risk of (non-fatal) bleeding;
The PARIS registry52 studied a real-world population of 5000 patients, and provided insight into the outcomes from physician-recommended discontinuation of DAPT, or brief interruption (for surgery), disruption (patient non-compliance), or because of bleeding. Compared with patients on continued DAPT, the adjusted HR for major adverse cardiovascular events due to interruption and disruption was 1.41 (95% CI 0.94 to 2.12; p=0.10) and 1.50 (95% CI 1.14 to 1.97; p=0.004), respectively. Within 7 days, 8–30 days, and more than 30 days after disruption, adjusted HRs were 7.04 (95% CI 3.31 to 14.95), 2.17 (95% CI 0.97 to 4.88), and 1.3 (95% CI 0.97 to 1.76), respectively. These data suggest that the risk of discontinuation is highest soon after stent deployment and attenuate the longer time elapsed;
Considering the risk associated with very early discontinuation of DAPT, patients with an early gastrointestinal haemorrhage (within the first 3 months) should be considered for endoscopic haemostasis without discontinuing DAPT.
6.0 Direct oral anticoagulants
For low-risk endoscopic procedures we suggest omitting the morning dose of DOACs on the day of the procedure (very low quality evidence, weak recommendation).
For high-risk endoscopic procedures in patients on DOACs, we recommend that the last dose of DOACs be taken at least 48 h before the procedure. For patients on dabigatran with a CrCl (or eGFR) of 30–50 mL/min we recommend that the last dose be taken 72 h prior to the procedure (very low quality evidence, strong recommendation). In any patient with rapidly deteriorating renal function a haematologist should be consulted (low quality evidence, strong recommendation).
6.1 Summary
Orally active drugs that directly inhibit thrombin (dabigatran etexilate)53 ,54 and factor Xa (rivaroxaban,55 ,56 apixaban57 ,58 and edoxaban59) are now licensed for prevention of stroke and systemic embolus in patients with non-rheumatic AF and for prevention and treatment of deep vein thrombosis and pulmonary embolus. These drugs should not be used as anticoagulants in patients with metal heart valve prostheses. These drugs are referred to as NOACs (Non-vitamin K antagonist Oral Anti Coagulants) or DOACs (Direct Oral Anti Coagulants).
For some patients DOACs offer benefits over oral vitamin K antagonists (VKA) such as warfarin. The drugs are prescribed at fixed dose without the need for monitoring or dose adjustment and the rapid onset of anticoagulation and short half-life of DOACs make initiation and interruption of anticoagulation considerably easier than with VKAs.
Specific antidotes are not yet available for clinical use, but are in development60–62 and will likely be licensed for use in the next 1–2 years.
As with all anticoagulants produced so far there is a correlation between intensity of anticoagulation and bleeding. Consequently, the need to consider the balance of benefit and risk with a DOAC is no less important than with warfarin. When a patient taking warfarin with a known INR undergoes endoscopic biopsy the intensity of anticoagulation is quantifiable. The pharmacokinetic profile, and hence pharmacodynamic effect, of DOACs varies such that some individuals will have higher peak levels 2–6 h after oral administration.63 Consequently, at the time of an endoscopic biopsy the anticoagulant effect due to a DOAC is not accurately predictable. In a patient taking a DOAC the intensity of anticoagulation may be relatively high compared to the average intensity and hence until further safety data in this specific situation are available we suggest omitting the morning dose of a DOAC on the day of a low-risk procedure so that biopsies can be sampled at a trough level. In patients undergoing a high-risk procedure with a low thrombotic risk we recommend that the last dose of a DOAC is taken 2 days before the procedure, that is, no dose in the 48 h before the procedure. This will ensure a minimal residual anticoagulant effect in the majority of patients. All DOACs are excreted to some extent by the kidneys but dabigatran pharmacokinetics are most influenced by renal function. Therefore, dabigatran may have to be stopped for more than 48 h before a procedure when renal function is known to be significantly reduced.64 For patients on dabigatran with creatinine clearance (CrCl) of 30–50 mL/min we recommend that the drug is stopped at least 72 h before the procedure. Dabigatran therapy is contraindicated in patients with CrCl <30 mL/min. eGFR is a suitable alternative measurement of renal function and the same numerical values apply for the purposes of these guidelines. If a patient on any DOAC is clinically deteriorating, his/her renal function should be checked before the procedure, and if there is possible drug accumulation a quantitative measurement of DOAC intensity should be performed, for example, by calibrated anti-Xa assay for Xa inhibitors or Hemoclot assay for dabigatran. In patients undergoing high-risk procedures with a high thrombotic risk then advice from a haematologist is recommended. The highest thrombotic risk patients are those with mechanical heart valve prostheses but DOACs are not indicated in such patients, so patients taking DOACs will not require bridging therapy.
It is of the utmost importance that clinicians are aware that unlike reintroduction of warfarin, which results in delayed anticoagulation for several days, a therapeutic intensity of anticoagulation is restored within 3 h of taking a therapeutic dose of a DOAC. Because of the high risk of bleeding associated with therapeutic intensity anticoagulation after an invasive procedure, we suggest a delay in reintroducing a DOAC after a high-risk procedure. This delay will depend on the risk of haemorrhage specific to the procedure and will usually be 24–48 h. For procedures with a significant risk of delayed haemorrhage such as EMR or ESD, a longer period of discontinuation may be considered in the context that DOAC patients are in a relatively low thrombotic risk category.
6.2 Drug characteristics
Compared with VKAs, DOACs are associated with a lower overall risk of major haemorrhage and particularly a significant reduction in the risk of intracranial bleeding, of the order of about a 50% risk reduction. The incidence of gastrointestinal bleeding was, however, increased with dabigatran and rivaroxaban compared to warfarin in large RCTs,53 ,56 although this was confined to the elderly (>75 years old) in a real-world study.65
Additional advantages of DOACs are:
A predictable dose response;
The absence of need for routine monitoring;
A reduced need for dose adjustment;
The absence of food interactions;
Limited drug interactions.
6.3 Dabigatran
In the RE-LY study of patients with AF there was an increase in the rate of lower gastrointestinal bleeding in the higher dabigatran dose (150 mg bd) group.53 This may be due to the low bioavailability (6.5%) and consequent high concentrations of dabigatran in the faeces causing a local anticoagulant effect at the level of the bowel wall.66 Dyspepsia was more common with dabigatran (11.3% and 11.8% in the 150 and 110 mg dabigatran groups) compared with warfarin (5.8%). The combination of higher rates of lower gastrointestinal bleeding and drug discontinuation due to dyspepsia may be a reason to choose a different anticoagulant for patients with a history of gastrointestinal disorders.
Dabigatran reaches a peak plama concentration 3 h after ingestion. After multiple doses a terminal half-life of about 12–14 h is observed. The half-life is independent of dose, but prolonged if renal function is impaired. With CrCl of 80 mL/min the half life of dabigatran is 13 h and it increases to 27 h if the CrCl is below 30 mL/min. The recommended dose is 150 mg bd with a dose reduction to 110 mg bd over the age of 80 years and in patients with a CrCl <50 mL/min. It should not be prescribed in patients with a CrCl ≤30 mL/min. Patients with liver enzymes more than twice the upper limit of normal were excluded from the RE-LY study. Nevertheless, there is no liver toxicity associated with dabigatran and so the drug might be used as long as there is no coagulopathy associated with liver disease. Aspirin or clopidogrel should be used with caution or avoided, and non-steroidal anti-inflammatory drugs should be avoided as their concomitant use was associated with an increased bleeding risk in the RE-LY study.
6.4 Rivaroxaban
Rivaroxaban is a direct competitive inhibitor of factor Xa and limits thrombin generation in a dose dependent manner. Absorption of this drug is rapid and it presents a half-life of 7–11 h. Two thirds of rivaroxaban are metabolised in the liver but it can be used in patients with liver disease if there is no coagulopathy. Only about one third of active rivaroxaban is cleared by the kidneys and there is no accumulation of drug when the CrCl is above 15 mL/min. However, a dose reduction from 20 mg once daily to 15 mg once daily has been recommended for patients with a CrCl between 15 and 30 mL/min. Rivaroxaban is not recommended when the CrCl is ≤15 mL/min. As with dabigatran, lower gastrointestinal bleeding occurred more frequently in the elderly with rivaroxaban than with warfarin.
6.5 Apixaban and edoxaban
Apixaban and edoxaban are Xa inhibitors that were approved subsequently to rivaroxaban for prevention of stroke in patients with non valvular AF and for treatment and prevention of venous thrombosis.67 Less than 50% of these drugs are cleared by the kidneys and similar recommendations to those made for rivaroxaban apply to interruption and recommencement of these drugs.
6.6 Measurement of anticoagulant effect of DOACs
Measurement of the anticoagulant effect of DOACs may be required when a patient is bleeding or scheduled for a high-risk intervention. Laboratories should ideally be aware of the sensitivity of their own prothrombin time (PT) and activated partial thromboplastin (APTT) assays to each drug. The result of a qualitative test such as the PT or APTT can indicate whether anticoagulation is supratherapeutic, therapeutic or subtherapeutic but cannot be used to determine the plasma concentration of the drug. The test results are dependent on when the last dose of drug was taken and therefore require interpretation with reference to the dose, anticipated half-life and factors that influence pharmacokinetics.
The Hemoclot thrombin inhibitor assay is a sensitive dabigatran-calibrated thrombin clotting time which can be used to determine the drug concentration.68 Anti-factor Xa assays are sensitive to factor Xa inhibitors.69–71 By using specific DOAC calibrators and controls, the anti-factor Xa chromogenic method is suitable for measuring a wide range of plasma concentrations of Xa inhibitors, which covers the expected plasma levels after therapeutic doses.
6.7 Bridging therapy
Compared to warfarin, requirement for bridging with heparin when interrupting DOACs are different due to the fast on and off effects of DOACs. In the Dresden DOAC registry heparin bridging for patients on rivaroxaban did not reduce cardiovascular events and led to a significantly higher rate of major bleeding compared to no bridging (2.7% vs 0.5%, p=0.01).72 In addition, a sub-study of the RE-LY trial found that bridging of dabigatran with LMWH resulted in higher rates of major bleeding (6.5% vs 1.8%, p<0.001) with no reduction in thromboembolism compared to no bridging.73
6.8 Triple antithrombotic therapy
Patients on dual antiplatelet therapy for coronary artery stents may develop AF requiring anticoagulation with warfarin or DOACs. Conversely, patients anticoagulated for chronic AF may develop ACSs requiring dual antiplatelet therapy. Consensus guidelines have been produced for the management of these situations,74 but patients on triple antithrombotic therapy have a high risk of haemorrhage and caution is advised.75 ,76 There are no data on endoscopy in these patients and advice should be sought from a cardiologist, or other relevant specialist such as a stroke physician, if endoscopy is essential.
6.9 Management of bleeding patients treated with DOACs
Management depends on the severity of bleeding. When bleeding is not severe, temporary drug withdrawal may be the only requirement due to the short half-lives of these drugs. For more severe bleeding general treatment measures may be required and consideration should be given to general resuscitation interventions, including endoscopic haemostasis, fluid replacement, correction of anaemia by transfusion of red cells and correction of additional coagulopathy (eg, dilutional coagulopathy) with platelet transfusion and appropriate blood products. The time of last intake of DOAC should be determined and the half-life can be estimated from measurement of serum creatinine and calculation of the CrCl. The anticoagulant activity of the DOAC should be determined by the most appropriate laboratory assay.
Protamine sulfate and vitamin K have no effect on the anticoagulant effects of DOACs. The effect of antifibrinolytics on bleeding due to DOACs is not known but use of tranexamic acid would be reasonable in some patients. Similarly, the general haemostatic effect of desmopressin (DDAVP) independent of thrombin or factor Xa might be beneficial although this is unknown. Fresh frozen plasma does not reverse the anticoagulant effect of DOACs to any appreciable degree and no clinical benefit has been demonstrated. The effects of prothrombin complex concentrate (PCC) and recombinant factor VIIa (rVIIa) have not been studied in clinical trials in human patients with bleeding. The effect of rivaroxaban on coagulation tests from volunteers is reversed by PCC (50 IU/kg of 4-factor concentrate) but the effect of dabigatran is not.77 These results do not indicate one way or the other if PCCs would reduce clinical bleeding. For patients with life-threatening bleeding, administration of 40–50 IU/kg of PCC has been suggested but there is no clinical evidence as yet that this will reduce clinical bleeding.78 ,79
7.0 Endoscopic procedures: risk of haemorrhage
There is an intrinsic risk of haemorrhage associated with endoscopic procedures. Minor haemorrhage is not uncommon during therapeutic endoscopic procedures, but we have considered it to be clinically significant when haemoglobin value falls by more than 20 g/L, necessitates blood transfusion or causes an unplanned hospital admission. Haemorrhage may be immediately apparent at the time of endoscopy, or delayed up to two weeks following the procedure. The latter situation may present a higher risk for patients who are on antiplatelet therapy or anticoagulants following the procedure. It is important that, not only are patients advised of the risks of haemorrhage following endoscopic procedures, but that they are given written advice on how to seek appropriate medical help should this occur following discharge from hospital. Unless otherwise stated, the following sections review the risks of haemorrhage in patients who are not on antithrombotic therapy, and these data are subsequently used to stratify the risk of procedures (table 1).
7.1 Diagnostic endoscopy and mucosal biopsy
Diagnostic endoscopies, including mucosal biopsy sampling, harbour a minimal risk of haemorrhage, and no severe haemorrhage has been reported in studies involving thousands of patients in total.9 ,80–83 Furthermore no increased risk of haemorrhage from biopsy has been found in studies of patients on aspirin, clopidogrel or warfarin.84 ,85 In these studies only small numbers of biopsies were taken, and the safety of taking large numbers of biopsies in patients on warfarin, such as in Barrett's oesophagus surveillance, has not been studied. There have been no published reports of excess bleeding in this context, however. There are no data about biopsies in patients taking the newer APAs or DOACs. Due to uncertainty regarding the level of anticoagulation on DOACs at the time of endoscopy and the absence of reliable test of anticoagulation on these drugs, we suggest omitting the dose of DOAC on the morning of the procedure to allow an adequate safety margin. This applies to both once daily and twice daily regimens.
7.2 Post polypectomy bleeding
Published haemorrhage rates for polypectomy, EMR or ESD are confounded by heterogeneity of definitions of intra-procedural bleeding (IPB) and PPB between studies. Previous studies of colonoscopic polypectomy have identified a risk of PPB of 0.07–1.7%.9 ,11–14 In a BSG audit of 20 085 colonoscopies in the UK, 52 (0.26%) haemorrhages were reported.8 Thirty nine of these were self-limited, three (0.01%) required transfusion, and one required surgery. Data from the English National Bowel Cancer Screening Programme on 112 024 participants, of whom 69 028 underwent polypectomy, found an overall PPB rate of 1.14%.86 Polypectomy increased the risk of bleeding by a factor of 11.14 compared with no polypectomy. In large series (>1000 polypectomies),86–92 delayed PPB varied from 0.6 to 2.2% and the mean time to onset of bleeding was 4.0±2.9 days.92 It is important to differentiate between minor haemorrhage associated with polypectomy which is controlled at the time of the procedure and more significant haemorrhage which requires an unplanned admission to hospital, possibly with repeat endoscopy and/or transfusion. The incidence of severe bleeding requiring transfusion in the English Bowel Cancer Screening Programme was 0.08%.86
Polyp size is the most consistent risk factor for colonic PPB, and it has been calculated that every 1-mm increase in polyp diameter increases the risk of PPB by 9%.93 Use of pure cutting current was found to be an independent predictive factor of immediate PPB compared with blended or coagulation current in a large cohort of 5152 patients undergoing more than 9000 polypectomies (OR, 6.95; 95% CI 4.42 to 10.94).94 In a prospective cohort study, the use of a non microprocessor-controlled current was an independent predictive factor of delayed bleeding when performing a wide field EMR.32 Two recent meta-analyses have examined data on RCTs for PPB prophylaxis.95 ,96 In the first, the seven studies included a majority of pedunculated large polyps (range, 14 to 26 mm) and the primary outcome focused on the overall risk of PPB.95 The authors found that any of the prophylactic measures helped prevent PPB (RR, 0.32; 95% CI 0.20 to 0.52), and mechanical techniques (detachable loop or endoclip) were superior to submucosal injection of diluted adrenaline (RR, 0.28; 95% CI 0.14 to 0.57). Submucosal injection of adrenaline was, however, found to reduce the risk of overall PPB when compared to no treatment or saline injection alone (RR, 0.37; 95% CI 0.20 to 0.66). The second meta-analysis evaluated the impact of endoscopic prophylactic methods on early PPB (within the first 24 h).96 Diluted adrenaline injection reduced significantly the risk of early PPB (OR, 0.37; 95% CI 0.22 to 0.64) as well as any other single prophylactic modality. No significant difference was observed between endoclip and detachable snare in a recent multicentre RCT to prevent delayed PPB in patients with pedunculated polyps with a large stalk (≥10 mm) (5.1% vs 5.7%, respectively).97 One RCT showed no significant difference in delayed PPB when using clips for pedunculated polyps, and the study was closed prematurely due to complications: one perforation (1.5%) and 3 mucosal burns (4.5%).98 This result could be explained by the incorrect placement of the clip in 10/66 patients (15%) with a short stalk, resulting in thermal injury due to the contact between the snare and the clip at the base of the pedicle. In all of these studies, patients on antiplatelet therapy or anticoagulation were excluded.
7.2.1 Endoscopic mucosal resection
Several studies have examined the prophylactic effect of endoclips on delayed PPB for sessile colonic polyps.99–101 One RCT of post-EMR defect closure by endoclips compared to no intervention failed to demonstrate any significant benefit.101 The study was however under-powered for this outcome. Two other studies of prophylaxis of PPB included antiplatelet therapy and/or anticoagulation users (47% and 10%, respectively).99 ,100 Pooled analysis showed a reduction of delayed PPB if the EMR defect was closed using endoclips (1.8% vs 4.4%) with an OR of 0.40 (95% CI 0.20 to 0.80), especially for large (≥20 mm) polyps. Furthermore a recent cost-efficacy analysis concluded that prophylactic placement of endoscopic clips after polypectomy was a cost-effective strategy for patients receiving antiplatelet or anticoagulation therapy, but not otherwise.102 For duodenal EMR, the use of endoclips to close the defect was recently found to significantly reduce the risk of delayed bleeding in a recent retrospective study (7% vs 32%).103 A large multicentre RCT found no reduction in significant post-EMR bleeding using prophylactic soft coagulation with forceps on visible vessels compared to no endoscopic prophylaxis.31
In large (>1000 cases) series of EMR, the incidence of immediate and delayed bleeding ranged between 3.7–11.3% and 0.6–6.2%, respectively.32 ,104 ,105 which are higher rates than those reported after conventional polypectomy. For EMR of small lesions (<10 mm), however, PPB rates were similar to those reported following conventional polypectomy.105 In two thirds of the patients, delayed bleeding developed within 48 h of colonic EMR.32 In one study, oesophageal EMR presented a greater risk of IPB compared with duodenal or colonic EMR.106 Nevertheless the rate of delayed post-EMR bleeding in the oesophagus remains low (0.6–0.9%), even in studies that include a high proportion of patients with a temporary cessation of antiplatelet therapy.106 ,107 Duodenal EMR had the highest risk of delayed bleeding. In two retrospective observational studies of duodenal EMR, delayed bleeding was reported in 14/113 (12.3%)103 and 7/111 patients (6.3%)106 despite the prophylactic use of endoclips in 82% of cases in the latter.
7.2.2 Endoscopic submucosal dissection
Compared with EMR, ESD presents a higher procedure-related bleeding rates irrespective to the location of the lesion treated (OR, 2.20; 95% CI 1.58 to 3.07).108 This is mostly a problem in the stomach; the mean rate of post procedural bleeding across five recent large studies (>6000 patients in total) of gastric ESD was 5.8% (range 3.6–6.9%).30 ,109–113 Nevertheless, severe consequences were rare (1 death, 3 angiographic interventions, and no surgery). In the oesophagus, a recent meta-analysis of 15 studies provided a pooled estimate of post-ESD delayed bleeding of only 2.1% (95% CI 1.2% to 3.8%).114 With respect to colonic ESD, a systematic review (total, 2774 patients) found a bleeding rate of 2% (95% CI 1% to 2%).115 No bleeding-related mortality was noted in oesophageal or colonic studies. A large multicentre prospective Japanese register confirmed this low rate of post colorectal ESD bleeding with only 18/816 events (2.2%).116 A higher bleeding rate was reported by a small prospective European study (6/45, 13%),117 though this included only rectal lesions, which present a higher risk of delayed bleeding.118 ,119
7.2.3 Polypectomy on antithrombotic therapy
A meta-analysis studied the risk of PPB in patients on continued clopidogrel therapy (574 patients and 6169 controls).120 Polyp size was less than 10 mm in 88% of the cases, and the proportion of patients on DAPT ranged from 54% to 87.8%.121–123 There was an overall increased risk of PPB (RR, 2.54; 95% CI 1.68 to 3.84) and of delayed PPB (RR, 4.66; 95% CI 2.37 to 9.17). Nevertheless, no patients required surgical or angiographic intervention and there were no fatalities. Another meta-analysis that included five studies demonstrated an increased risk of delayed but not immediate PPB on clopidogrel.120
A prospective study including 823 patients focused on cold polypectomy (using forceps or snare method) with a mean polyp size of 4.7±1.3 mm91; 15% of the patients were taking low dose aspirin or ticlopidine. The risk of immediate PPB was increased in patients on continued APAs (6.2% vs 1.4%; p<0.001) but all bleeding episodes were successfully treated during the procedure, and no delayed PPB was observed. No data on PPB in patients taking prasugrel, ticagrelor, or DOACs were found.
The impact of APAs on colonic post-EMR bleeding was evaluated in two recent prospective observational studies and one RCT comparing endoscopic prophylactic coagulation of visible vessels compared to no prophylaxis for wide field EMR (>2 cm).31–33 Pooled analysis of the results in 1807 patients showed that clinically significant post-EMR bleeding was associated with the use of aspirin; only 20 patients were on clopidogrel so that no conclusion can be drawn for clopidogrel. No data are available regarding the use of prasugrel, ticagrelor or DOACs in relation to colonic EMR.
There are no studies of the risk of bleeding on continuous anti platelet therapy for oesophageal or duodenal EMR. Two retrospective observational studies found no relation between previous APA use including clopidogrel (stopped 5–7 days before the procedure) and the occurrence of early or delayed bleeding.106 ,107 Caution is required if aspirin therapy is interrupted when prescribed for secondary prophylaxis due to the high risk of thrombotic events.34–36
The association of thienopyridene or aspirin use with the risk of post-ESD bleeding has been examined in several studies of gastric ESD. These studies are, however, retrospective single-centre case studies with a variety of APAs, and differences in regimens for discontinuing or continuing therapy. Bleeding end-points also vary between studies. Aspirin was an independent risk factor for haemorrhage in one study,29 and in two others there was an increased risk of post-ESD haemorrhage despite temporary interruption of antiplatelet therapy.30 ,109 Recent dual therapy with aspirin and clopidogrel was an independent predictive factor for delayed bleeding (OR >10 in two studies),29 ,124 but continued use of low dose aspirin alone,125 or after temporary discontinuation of thiopyridene, was not found to be an independent risk factor for post-ESD bleeding in other studies.110 ,126 ,127 Insufficient data were available to interpret the role of clopidogrel alone on post-ESD bleeding, and the numbers of patients on aspirin monotherapy in the above studies was small. Two studies have reported no association between post-ESD bleeding and antithrombotic agents for colorectal ESD, but the drugs were discontinued 1 week before the procedure.118 ,119 No data on APA therapy and oesophageal ESD were found. No data are available regarding the use of prasugrel, ticagrelor or DOACs in relation to ESD.
7.3 Endoscopic retrograde cholangiopancreatography
Reviews of endoscopic retrograde cholangiopancreatography (ERCP) practice have found that clinically significant haemorrhage occurs in 0.1–2% of sphincterotomies.128 ,129 Risk factors for haemorrhage after biliary sphincterotomy included bleeding observed during the procedure, coagulopathy, initiation of anticoagulant therapy within 3 days after the procedure, active cholangitis, and low endoscopist case volume of endoscopic sphincterotomies. For endoscopic sphincterotomy, blended current, as opposed to pure-cutting current, is recommended as a meta-analysis of RCTs demonstrated that it reduces the incidence of post-sphincterotomy haemorrhage without significantly increasing the risk of post-ERCP pancreatitis.130 ,131
To decrease the risk of bleeding, endoscopic papillary balloon dilation (EPBD) has been proposed as an alternative to sphincterotomy for biliary stone extraction. A recent meta-analysis that included 12 RCTs (1975 patients) concluded that, compared with endoscopic sphincterotomy, EPBD was associated with a lower incidence of haemorrhage, a lower rate of stone clearance, and a higher incidence of post-ERCP pancreatitis.132 However another meta-analysis of RCTs demonstrated that prolonged (>1 min) EPBD actually reduced the incidence of post-ERCP pancreatitis (compared to short EPBD) to a level similar to that observed with sphincterotomy.133 As bleeding rates were lower with EPBD versus sphincterotomy, in a network meta-analysis, the probabilities of being the safest treatment for long EPBD/short EPBD/sphincterotomy regarding overall complications were 90.3%/1.3%/8.4%, respectively.133 Therefore, if EPBD is performed without sphincterotomy, balloon inflation should be maintained ≥1 min following waist disappearence. Usual contraindications to EPBD include biliary strictures, ampullary/pancreatic/biliary malignancies, prior biliary surgery except cholecystectomy, acute pancreatitis, precut sphincterotomy for biliary access and large common bile duct (CBD) stones.
Finally, sphincterotomy is not required for most placements of biliary plastic stents or self-expanding metal stents (SEMS). A meta-analysis of three RCTs (338 patients) that compared patients with sphincterotomy before biliary stent placement compared to without endoscopic sphincterotomy found that sphincterotomy was associated with a higher incidence of post-ERCP haemorrhage (6.2% vs 0) but a lower incidence of post-ERCP pancreatitis (3.5% vs 8.9%).134 The rate of stent migration was similar in both groups of patients. A large prospective nonrandomised study that compared patients with stent placement preceded or not by sphincterotomy (n=130 vs 1112, respectively) found that stent insertion was successful in all patients, with similar incidences of post-ERCP pancreatitis and bleeding in both groups of patients.135
7.3.1 ERCP on antithrombotic therapy
Five controlled studies of biliary sphincterotomy in patients receiving APA were found129 ,136–139; only one of them reported a statistically significant difference in haemorrhage in APA users (9.6%) versus non-users (3.9%). This study was retrospective and the difference was not significant in multivariate analysis. In addition to these studies, a retrospective study compared 40 patients with post-sphincterotomy bleeding vs 86 matched controls who had no post-sphincterotomy bleeding; similar proportions of patients taking APA were found among both groups of patients (13% aspirin and 3% clopidogrel vs 17% aspirin and 0% clopidogrel in cases vs controls, respectively).140
Endoscopic sphincterotomy followed by large balloon dilation is increasingly undertaken for large biliary stone extraction; haemorrhage has been reported in 0–8.6% of patients.141 A single series was identified that included five patients taking aspirin at the time of endoscopic sphincterotomy followed by large balloon dilation; none of them presented with significant bleeding.142 There are no data on this technique in patients on thienopyridines, ticagrelor or DOAC.
There are no data on biliary mechanical lithotripsy in patients taking APA or anticoagulants. Similarly there are no data on cholangioscopy and electrohydraulic lithotripsy therapy on these drugs.
7.4 Ampullectomy
Endoscopic ampullectomy is an established technique for resection of ampullary adenomas, and this is generally followed by pancreatic duct stenting at ERCP to reduce the risk of post-procedure pancreatitis.143 The risk of haemorrhage following ampullectomy ranges from 1% to 7% in published series.144–147 No study was found that reported on endoscopic ampullectomy in patients taking aspirin or other antithrombotic agents. Some authors have stated that aspirin can be continued in patients at high thrombotic risk148 but this should be assessed on an individual patient basis, as bleeding is a common complication and may be severe.
7.5 Endoscopic ultrasound-guided fine-needle aspiration
The incidence of bleeding following endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) has been analysed in a systematic review that included 10 941 patients (51 studies); globally the incidence of bleeding was 1.28 per thousand149 Incidences per site, per thousand, were, in increasing order: pancreas 1 (pancreatic mass, 0.7; pancreatic cyst, 3.3), mediastinum 1.5, perirectal lesion 5.2, liver 8.7, ascites 11.8. EUS-guided brushing of pancreatic cysts was associated with a relatively high incidence of bleeding in five prospective studies, including one fatality.150–154
One prospective study assessed the risk of bleeding complicating EUS-FNA in patients taking aspirin/NSAIDs.155 In this study, 241 lesions were sampled, including solid tumours, cysts and ascites with a mean of approximately 2.5 passes using a 19G or 22G needle. There was no significant difference in bleeding between those taking aspirin/NSAIDs (0 of 26 patients) compared with controls (7 of 190 patients). There are no studies identified that assessed haemorrhage after EUS-FNA in patients taking thienopyridines, ticagrelor or DOAC.
7.6 Endoscopic dilatation and stenting
7.6.1 Dilatation
Large studies of bougie-dilatation of oesophageal strictures reported no significant haemorrhage.156 ,157 Controlled radial expansion balloons are more commonly used for this purpose now. A study of 472 oesophageal dilations included a mixture of bougie and balloon dilatations, and no perforations or haemorrhage were reported,158 A series of 98 balloon dilations of anastomotic strictures of the cervical oesophagus reported no haemorrhagic complications.159 A study of the complications arising from 504 balloon dilations in 237 patients with achalasia revealed 4 (1.7%) asymptomatic haematomas, but no clinically significant haemorrhage.160 There were, however, 7 (3%) perforations. Seven case series have reported no haemorrhages following ileal or colonic dilation.161–166 Two further case series did however report haemorrhage associated with dilation of ileal or colonic strictures in 1/20 (5%)167 and 1/38 (2.6%) patients.168 One study included dilation of malignant strictures and encountered no haemorrhagic complication in 94 cases (68 malignant and 26 anastomotic strictures).169 In a RCT of pneumatic dilatation versus laparoscopic myotomy for achalasia there were no reported haemorrhages but 8/108 (9.5%) patients experienced perforation during the treatment course.170 None of the abovementioned studies was primarily designed to evaluate the risk of bleeding associated with dilation. There have been no studies evaluating the risk of endoscopic dilatation in the gastrointestinal tract in patients taking APA or anticoagulants.
7.6.2 Endoscopic stent insertion
Historical studies of complications associated with endoscopic stenting may be confounded by the variety of stents employed and the improvements in devices with time. There have been no studies on endoscopic stenting at any site in the gastrointestinal tract in patients taking APA or anticoagulants. A US national survey of oesophageal SEMS insertion reported a haemorrhagic complication rate of 0.5% (2/434).171 A haemorrhage rate of 1% was found in a retrospective study of 92 oesophageal stent placements.172 In two studies of oesophageal stenting for palliation of malignant strictures, fatal haemorrhage occurred in 7.3%173 and 8% of patients.174 Haemorrhage was however delayed in these series, often by several weeks. Comparative studies of various types of self-expanding oesophageal stents reported similar rates of efficacy and complications.175–180 Immediate haemorrhage rates are low, but consideration should be given to delayed severe haemorrhage, and this is likely to be a particular risk in patients on APA or anticoagulant therapy.
A systematic review of duodenal stenting included 606 patients in whom 3 (0.5%) haemorrhages were reported.181 An international multicentre prospective cohort study conducted between 1996 and 2003182 assessed the efficacy and safety of enteral stents: 188 stents were placed in 176 patients and 2 (1%) of them suffered from gastrointestinal haemorrhage.
With respect to colorectal stenting, a systematic review of 58 studies (598 patients)183 found a bleeding rate of 4.5%. Twenty-four (89%) haemorrhages required no treatment, but the 3 (0.5%) remaining patients had severe haemorrhage requiring blood transfusion. A systematic review of 27 studies involving 325 patients with malignant colonic obstruction did not report any cases of gastrointestinal haemorrhage.184 A third systematic review that included 54 publications, none of which were randomised, found no cases of gastrointestinal haemorrhage in 1192 patients-185 A retrospective study of 102 stent placements revealed no haemorrhages, but 4 (4%) perforations,186 and a multicentre prospective study of 44 stent placements revealed one case of haematoma which resolved spontaneously, and no perforations.187 In a study of 463 colonic stent placements in 447 patients, there were only 2 (0.5%) cases of haemorrhage, but 15 (3.9%) perforations, 3 of which were fatal.188 In a RCT of colonic stenting versus emergency surgery in the context of acute malignant colonic obstruction there were no instances of haemorrhage in the stenting group, but 6/47 (13%) perforations.189
7.7 Percutaneous endoscopic gastrostomy
Minor haemorrhage around the wound site at percutaneous endoscopic gastrostomy (PEG) placement is not uncommon and usually ceases spontaneously or with simple pressure at the wound site. Severe haemorrhage is rare, but may occur due to vascular puncture.190 ,191 Rectus sheath haematoma has also been described.192 Continued administration of aspirin for PEG placement has not been associated with an increased risk of haemorrhage.193 Additionally, there was no increased risk of haemorhage on clopidogrel in a retrospective single-centre case-control study of 990 patients,194 although this study was statistically underpowered to demonstrate an effect due to this drug. There have been no studies examining the risk of PEG placement in patients on prasugrel, ticagrelor or DOAC.
7.8 Device-assisted enteroscopy
Single-balloon, double-balloon and spiral enteroscopy devices are commonly used. The overall risk of haemorrhage associated with double balloon enteroscopy has been estimated at 0.2%,195 and rises to 3.3% if polypectomy is performed.195 Spiral enteroscopy has not been associated with a risk of clinically significant haemorrhage.196 Double balloon enteroscopy is associated with a perforation rate of 0.1–0.4%195 ,197 and this rises to 1.5% if polypectomy is performed197 and 3% in patients with an altered surgical anatomy.195 There have been no studies examining the risks of enteroscopy in patients taking APA or anticoagulants.
7.9 Oesophageal variceal banding
Emergency variceal banding occurs in the context of active variceal haemorrhage, which is a life-threatening emergency. Elective variceal banding is also associated with a risk of delayed haemorrhage. In a study of 605 patients undergoing variceal ligation, 21 (3.5%) patients had spontaneous bleeding due to band slippages confirmed at endoscopy, and 11 died.198 Rebleeding due to band-induced ulcers has been found to occur in up to 14% of patients.199–202 Multivariate analysis in the first study found no increased risk of bleeding in those on aspirin, although this applied to only 8/605 patients.198 There have been no studies of the risks of haemorrhage following variceal banding in patients on thienopyridenes, ticagrelor or DOAC, and indeed it would be usual to discontinue these drugs, if possible, in a population at such a high risk of haemorrhage.
8.0 Endoscopy on APA and anticoagulants: risk stratification
Certain endoscopic procedures carry a higher risk of haemorrhage, and certain clinical situations will result in a high risk of thromboembolic complications should APA or anticoagulants be withdrawn. Procedures have been classified as high-risk or low-risk for haemorrhage based on baseline risks of haemorrhage or perforation associated with the procedures as well as the limited data available regarding endoscopy during therapy with APA or anticoagulants (table 1). Tables 2 and 3 stratify risk for discontinuation of APA or warfarin according to clinical scenario, and the risks of thromboembolic sequelae on discontinuation of therapy. A risk assessment matrix based on these factors is shown in table 4.
Risk assessment matrix of haemorrhagic and thrombotic risk
Diagnostic endoscopic procedures, with or without biopsy, are classified as low-risk for haemorrhage. This applies to diagnostic colonoscopy, but polyps are likely to be encountered in 22.5–34.2% of patients according to large studies,9 ,11 and endoscopists may therefore choose to manage colonoscopies as high-risk procedures with respect to APA and anticoagulants including DOAC. Similar considerations apply to ERCP if there is uncertainty as to the required therapy.
References
Footnotes
This article is published simultaneously in the journal Endoscopy. Copyright 2016 © Georg Thieme Verlag KG
Contributors All authors have contributed to literature searches, manuscript preparation and review of previous drafts of the guidelines.
Competing interests Prof Gershlick has received lecture fees for advisory boards for Astra Zeneca and Eli Lilley/Daiichi Sankyo. None of the other authors have competing interests to declare.
Provenance and peer review Not commissioned; externally peer reviewed.
Disclaimer These joint BSG and ESGE guidelines represent a consensus of best practice based on the available evidence at the time of preparation. They may not apply in all situations and should be interpreted in the light of specific clinical situations and resource availability. Further controlled clinical studies may be needed to clarify aspects of these statements, and revision may be necessary as new data appear. Clinical consideration may justify a course of action at variance to these recommendations. BSG and ESGE guidelines are intended to be an educational device to provide information that may assist endoscopists in providing care to patients. They are not rules and should not be construed as establishing a legal standard of care or as encouraging, advocating, requiring, or discouraging any particular treatment.