Article Text

Abstract
Background Endoscopic mucosal healing is an established treatment target for UC, yet the value of achieving histological remission remains unclear.
Aims To evaluate histological remission compared to endoscopic mucosal healing for predicting patient outcomes in UC.
Methods Blinded assessment of endoscopic and histological measures of disease activity was performed on patients with established UC at baseline. Concordance and prognostic values of endoscopic mucosal healing (defined by Baron score ≤1) and histological remission (defined by Truelove and Richards’ index) for predicting outcomes of corticosteroid use, hospitalisation and colectomy were determined over a median 6 years follow-up, including κ statistics and Cox regression multivariate analysis.
Results 91 patients with UC were followed up for a median 72 months (IQR 54–75 months). Overall, concordance between endoscopic and histological remission was moderate (κ=0.56, 95% CI 0.36 to 0.77); 24% patients had persistent inflammation despite endoscopic remission. Histological remission predicted corticosteroid use and acute severe colitis requiring hospitalisation over the follow-up period (HR 0.42 (0.2 to 0.9), p=0.02; HR 0.21 (0.1 to 0.7), p=0.02; respectively), whereas endoscopic mucosal healing did not (HR 0.86, 95% CI 0.5 to 1.7, p0.65; HR 0.83 95% CI 0.3 to 2.4, p0.74; respectively).
Conclusions Histological remission is a target distinct from endoscopic mucosal healing in UC and better predicts lower rates of corticosteroid use and acute severe colitis requiring hospitalisation, over a median of 6 years of follow-up. Our findings support the inclusion of histological indices in both UC clinical trials and practice, towards a target of ‘complete remission’.
- INFLAMMATORY BOWEL DISEASE
- ULCERATIVE COLITIS
- MUCOSAL REPAIR
- HISTOPATHOLOGY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Endoscopic mucosal healing is an established treatment target for patients with UC.
Persistent histological inflammation is common in the setting of endoscopic mucosal healing, yet there has been little systematic analysis of the concordance between indices of remission in UC.
Observational data suggest that persistent histological inflammation in patients with UC predicts worse clinical outcomes over 12 months of follow-up.
What are the new findings?
Histological remission was shown to predict corticosteroid use and hospitalisation for acute severe colitis in patients with UC over a median of 6 years of follow-up, whereas endoscopic mucosal healing did not.
Systematic analysis revealed histological remission as a target distinct from endoscopic mucosal healing, with only moderate correlation between indices.
How might it impact on clinical practice in the foreseeable future?
Our findings support the inclusion of histological indices in both UC clinical trials and practice, towards a target of ‘complete remission’.
Introduction
Therapeutic advances in the medical management of UC have altered treatment targets.1–3 Consensus guidelines for clinical practice and trial endpoints recommend striving beyond resolution of clinical symptoms, to achieve endoscopic mucosal healing.2 ,4–7 Endoscopic mucosal healing in IBD is defined by resolution of visible mucosal inflammation and ulceration. This has been associated with prolonged clinical remission, lower rates of hospitalisation and lower rates of colectomy.8–13 The term ‘deep remission’ has evolved as a treatment target in the era of biological therapy for IBD, currently defined as the combination of clinical remission and endoscopic mucosal healing.14 ,15 The unanswered question is whether mucosal biopsies, taken at the time of endoscopy for evaluation of microscopic mucosal healing, add sufficient therapeutic value to constitute a further target: ‘complete remission’.16
Expert opinion aside, there is no gold standard for assessing or defining disease remission in UC.1 ,2 Histological remission represents a target distinct from endoscopic mucosal healing, since many studies have shown that endoscopic mucosal healing does not necessarily reflect histological mucosal healing in UC.16–19 Multiple histological scoring systems to assess disease activity in UC have been described since the 1950s, though none are fully validated.16 ,18 ,20–22 As a consequence of multiple scoring systems, there currently exists no standard definition for histological remission in UC.16 ,21 Definitions of histological remission range from residual inflammation with architectural distortion to complete normalisation of the colonic mucosa. This lack of consensus has limited incorporation of histopathological endpoints into clinical trials in UC, although this does not diminish the intuitive importance of controlling inflammation and persistent microscopic inflammation for predicting the future course of UC.
Observational studies have shown that persistent histological inflammation in UC is associated with an increased risk of relapse, hospitalisation and colectomy, as well as an increased risk of colorectal neoplasia.18 ,23–30 Despite such evidence suggesting the importance of microscopic inflammation as a harbinger of disease activity, histological remission is not yet recommended as a therapeutic endpoint either for clinical trials or practice in UC.1 ,2 ,4 As a consequence, there is currently no evidence from randomised controlled trials in support of treatment intensification to achieve histological healing in UC. A few studies have assessed the histological response to immunomodulator or biological therapy.15 ,31 ,32 Nevertheless, this situation is bound to change since the Food and Drug Administration (FDA) are considering documentation of histological disease activity both at inclusion and as an outcome measure in clinical trials.
The aim of this study was to prospectively analyse the value of histological remission compared with endoscopic remission, for predicting outcomes of steroid use, hospitalisation or colectomy in patients with UC over a long period of follow-up. Concordance between measures of remission was systematically evaluated.
Materials and methods
Patients
Outpatients with an established diagnosis of UC according to conventional criteria33 were recruited from the IBD Clinic of the Translational Gastroenterology Unit at the John Radcliffe Hospital, Oxford. Subjects were initially invited to participate in a study of interobserver variation for the assessment of disease activity between November 2007 and March 2008.34 Subjects were recruited regardless of the degree of clinical disease activity.
Baseline characteristics were recorded, including demographics, disease duration, extent and current medications. The Simple Clinical Colitis Activity Index (SCCAI) was calculated for each patient.35 An SCCAI ≤2 was used to define clinical remission.1 The SCCAI was selected as a validated index of clinical activity,36 since it solely depends on symptoms with a defined interobserver variation, without the need for endoscopy or laboratory tests. The Montreal Criteria were used to define disease extent.37
Patients subsequently received standard clinical care5 ,33 at the recruiting hospital, with regular outpatient follow-up (maximum interval of 12 months between appointments) to assess clinical outcomes.
Baseline assessment
Endoscopic
At the baseline visit, patients underwent a videosigmoidoscopy according to a standard technique38 by a single clinician (OCB), who was blinded to the clinical activity score. The extent of examination was to the sigmoid descending junction or to the descending colon, as tolerated by the patient. A trained central reader (AJW) later scored endoscopic disease activity for the most severely affected area, using the Baron index.39 In the absence of a validated endoscopic index of activity at the time of assessment, a Baron score ≤1 without mucosal friability was used to define endoscopic remission.2 Small patient numbers precluded further analysis within Baron score subgroups.
Histological
Mucosal biopsies were routinely taken from the sigmoid colon and rectum, targeting the area where the colitis was endoscopically most active, as well as any other areas of interest. A single specialised gastrointestinal histopathologist (AvH) scored the worst affected area using the Truelove and Richards’ index,22 blinded to the clinical and endoscopic scores. The index was selected as a clinically applicable grading system, where the category ‘no significant inflammation’ defines histological remission and refers to architectural changes in the absence of erosions, crypt abscesses or neutrophilic infiltration. It groups activity into domains (remission/mild-moderate/severe) that could be compared directly with clinical and endoscopic activity, and tested over time. The Truelove and Richards’ index is one of the few partially validated histological indices in UC.16 ,21 The best validated histological index of disease activity (Geboes index20) does not use a summative scale and avoids classification by activity tertiles.
Clinical outcomes
Patients’ clinical records were audited in July 2014 for clinical outcomes including oral corticosteroid use and requirement for escalation of therapy, hospitalisation or colectomy since the baseline assessment. Standardised practice for oral corticosteroid use in patients with UC applied during the follow-up period. Oral corticosteroids were initiated through an IBD advice telephone service or outpatient clinic on the basis of a relapse of established UC, characterised by bloody diarrhoea and urgency, with or without endoscopic confirmation, in the absence of systemic features sufficient to meet a diagnosis of acute severe colitis,33 generally after no response within 2 weeks to up-titration of 5-aminosalicylic acid therapy (oral and topical). Oral corticosteroids were initiated before escalation of therapy to immunomodulators (thiopurines, methotrexate) or biological therapy. The need for hospitalisation was defined by Truelove and Witts’ criteria for acute severe colitis.40 Colectomy was indicated in the instances of severe, treatment-refractory colitis, toxic megacolon or malignancy complicating colitis.41
Statistical analysis
Descriptive statistics are expressed as medians and IQR. Fleiss’ κ was calculated to quantify agreement between the three measures of disease activity. Qualitative interpretation of κ statistics used the convention of Landis and Koch,42 where 0 indicates poor agreement, 0.0–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement and 0.81–1.0 almost complete agreement.
Since clinical outcomes (corticosteroid use/escalation of therapy, hospitalisation or colectomy) did not occur in all patients, univariate and multivariate survival analysis with Cox regression was used to examine how endoscopic and histological measures of remission were associated with time to corticosteroid use or escalation of therapy, time to hospitalisation and time to colectomy. Kaplan–Meier survival analysis was performed for outcomes. In addition, χ2 analysis was used to compare categorical variables between groups. Analysis was performed using SPSS (V.22) software and Graphpad Prism.
Ethical considerations
Subjects were invited to participate in the study comparing disease indices between November 2007 and March 2008 (approved by the Oxfordshire Research Ethics Committee LREC 536407Q1605/58ORH). Informed consent was obtained and participant information was stored in a confidential depersonalised database. Patients also consented to the IBD Cohort Study (Research Ethics Committee reference 09/HI204/30), consenting to longitudinal follow-up of patient information.
Results
Patients
Ninety-one patients underwent baseline assessment, with clinical outcome data available on all patients over a median 72 months (6 years, IQR 54–75 months) of follow-up. Two patients died of causes unrelated to UC during the follow-up period (ruptured abdominal aortic aneurysm and acute myocardial infarction). Baseline characteristics are shown in table 1.
Baseline characteristics of patients with UC
Concordance between measures of disease activity at baseline
Disease activity was dichotomised into either remission or active disease on the basis of clinical, endoscopic and histological indices. Overall concordance between the three measures for disease activity was 55% (50/91), consistent with moderate agreement (κ= 0.43, 95% CI 0.31 to 0.55) (figure 1). Only 29% (26/91) of patients were in remission by all three measures of assessment.

Concordance between clinical, endoscopic and histological measures of remission in UC. Legend: κ statistical analysis was used to assess concordance of clinical, endoscopic and histological indices of remission.
Agreement between endoscopic and histological measures of remission was moderate (43% (42/91), κ=0.56, 95% CI 0.36 to 0.77). In the setting of endoscopic mucosal healing, 75% (42/56) of patients were also in histological remission and 11% of patients appeared to have endoscopic activity despite histological remission.
The greatest disparity arose when clinical assessment was compared with endoscopic and histological measures of remission (κ=0.29, 95% CI 0.10 to 0.49; κ=0.47, 95% CI 0.27 to 0.68; endoscopic and histological remission respectively).
Endoscopic versus histological remission in predicting patient outcomes
Corticosteroid requirement
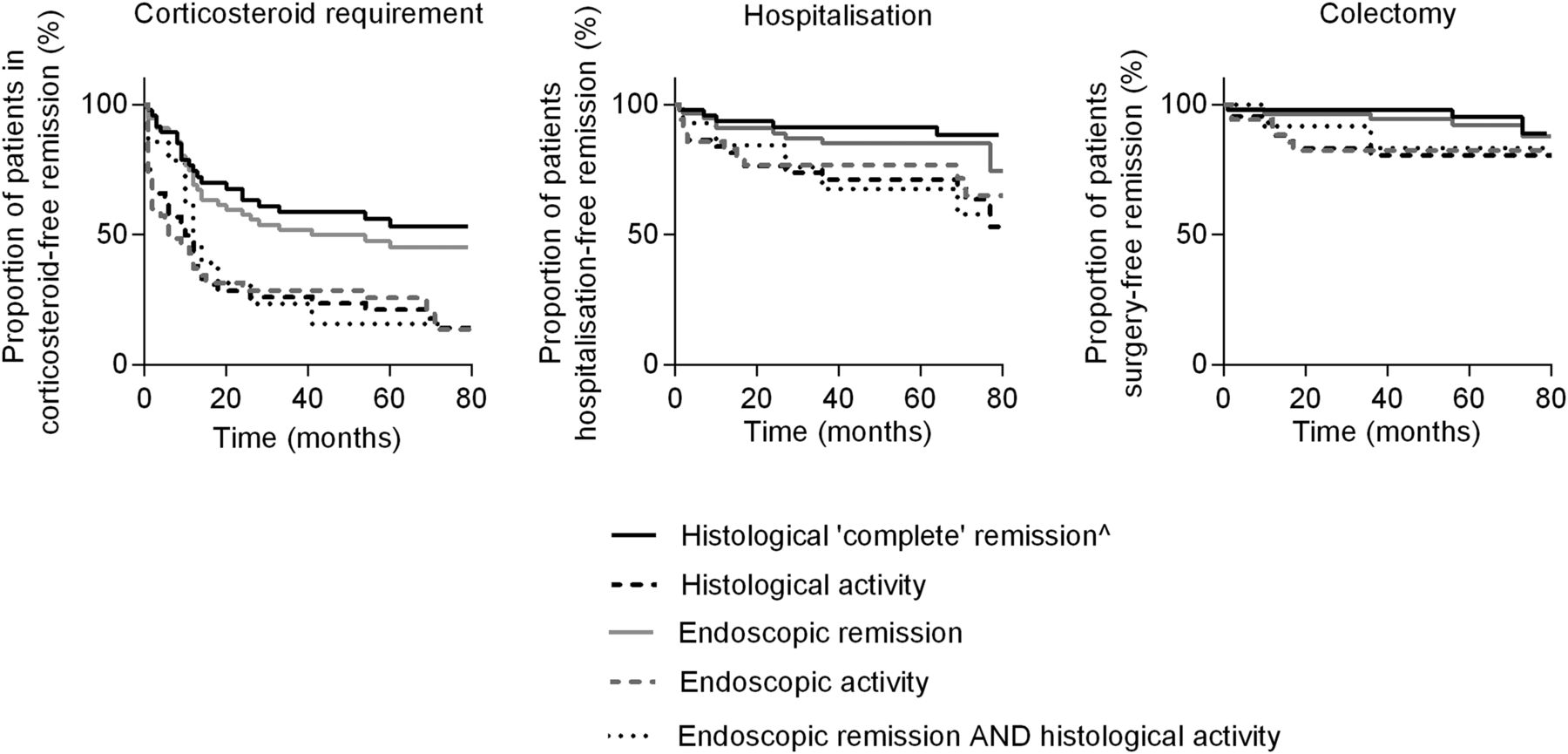
During the 6-year follow-up period, 63% (57/91) of patients received oral corticosteroids, with 33% (30/91) needing more than one course. In multivariate Cox regression analysis, a reduced corticosteroid requirement was predicted by histological remission (HR 0.42, (0.2 to 0.9), p=0.02 respectively) (table 2). Endoscopic remission, however, did not predict a lower requirement for corticosteroids (HR 0.86 (0.5 to 1.7), p=0.65). Numbers of patients with a more stringent endoscopic definition of remission (Baron score=0) were too small for statistical analysis. ‘Complete remission’, as defined by both endoscopic and histological remission, predicted future corticosteroid requirement (HR 0.38, (0.2 to 0.9), p=0.02). Among those patients in ‘complete remission’ at baseline, 43% required corticosteroids over the follow-up period, as opposed to 78% of those in endoscopic remission but with persistent histological activity (p=0.02) (figure 2 and table 3).
Cox regression multivariate analyses for outcome measures in patients with UC over a median 6-year follow-up
Risks of clinical outcomes in patients with UC over a median of 6 years of follow-up

{kind=link}
{kind=link}
Kaplan–Meier graph of endoscopic and histological remission and clinical outcomes in patients with UC. Legend: Kaplan–Meier survival analysis of time to corticosteroid requirement, hospitalisation for acute severe colitis or colectomy. Groups were divided on the basis of endoscopic or histological healing. The numbers of patients in each group are shown in figure 1. ^The curve for ‘complete’ remission (histological and endoscopic remission, n=42) is almost identical to that of histological remission (n=47) and is depicted by a single line.
Hospitalisation
Over the 6-year follow-up period, 22% (20/91) patients were hospitalised with acute severe colitis. Disease extent and histological remission predicted reduced rates of hospitalisation in multivariate analysis (HR 3.21 (1.1 to 8.6), p=0.02; HR 0.21 (0.1 to 0.7), p=0.02; respectively), whereas endoscopic remission did not (HR 0.83 (0.3 to 2.4). p=0.74). ‘Complete remission’ also predicted lower rates of hospitalisation (HR 0.24 (0.1 to 0.9), p=0.04). Among those in ‘complete remission’ at baseline, 12% were hospitalised over the follow-up period, as compared with 36% of those in endoscopic remission but with persistent histological activity (p=0.04) (figure 2 and table 3).
Colectomy
Colectomy was an infrequent event over the 6-year follow-up period, occurring in only 12% (11/91) patients over the follow-up period. Only disease extent was a significant predictor of colectomy in multivariate analysis (HR 4.06 (1.3 to 16.2), p=0.02).
Discussion
This study is the first to systematically analyse concordance between indices of remission in UC, as well as the value of endoscopic and histological remission in predicting patient outcomes over a long period of follow-up. Histological remission as a marker of ‘complete’ remission was shown to be of more value than endoscopic remission in predicting requirement for corticosteroids or hospitalisation for acute severe colitis over the 6-year follow-up. The findings are striking but intuitive, adding weight to calls to include histological remission into definitions of the depth of remission for UC.17 ,43 ,44 In the current scramble for biomarkers that might predict the future pattern of disease, traditional measures such as histology merit re-appraisal.
Histological healing deserves distinction from endoscopic mucosal healing. We show moderate agreement between histological and endoscopic measures of remission (κ=0.56, 95% CI 0.36 to 0.77). Microscopic inflammation persists in 25% of patients with endoscopic mucosal healing, illustrating that leukocyte infiltration is not seen using conventional endoscopy.11 ,45 ,46 This is consistent with previous studies, although the large range (16%–90%) reflects different definitions of remission and activity for endoscopy and histopathology.16 ,18 ,19 ,24 ,25 ,47–49 Histological remission in the presence of endoscopic activity may relate to discontinuous inflammation, but histopathology helps avoid overinterpretation of mucosal changes that may occur due to factors such as bowel preparation.50 The greatest disparity between measures of remission occurred for clinical assessment, which is consistent with Truelove's original observations.22 Symptoms in patients with endoscopic remission are commonplace, often due to concurrent IBS, medications or infection. This is relevant both to clinical practice when trying to avoid unnecessary medical therapy and to clinical trials, since clinical symptoms alone cannot be relied upon to judge disease activity.51 This also emphasises the need for endoscopy along with mucosal biopsies to assess disease activity objectively. Histopathology is more likely to reflect inflammation than endoscopy, particularly in the presence of ‘minimal’ or ‘mild’ endoscopic activity.19 ,49 Better concordance between histology and endoscopy is reported for inactive or severely active disease,49 but the potential for disproportionate intramural extension of inflammation in severe colitis is recognised.52 ,53 Both endoscopic and histological assessment are prone to interobserver variability,54 which has implications for clinical trials, indicating the need for independent evaluation by the central reader of disease activity.54–57
Our study reveals the prognostic value of histological remission beyond that of endoscopic mucosal healing, over an extended follow-up period. Histological remission, but not endoscopic mucosal healing, was predictive of a lower requirement for corticosteroids (HR 0.42 (0.2 to 0.9), p=0.02) over the 6-year follow-up. Histological remission, but not endoscopic mucosal healing, predicted lower rates of acute severe colitis requiring hospitalisation (HR 0.21 (0.1 to 0.7), p=0.02). The rate of acute severe colitis over the follow-up period was 22%, consistent with the natural history of UC.40 Extensive disease was the only predictive factor for colectomy; the lack of association with endoscopic and histological remission is likely to represent a Type 2 statistical error from small numbers.
Guidelines do not yet recommend histological remission as a therapeutic endpoint in clinical trials.3 Paradoxically, this ignores longstanding evidence that histological inflammation may better predict clinical outcomes than clinical or endoscopic measures.30 Riley et al18 showed that an acute inflammatory cell infiltrate, crypt abscesses or mucin depletion on mucosal biopsy from patients in clinical and sigmoidoscopic remission was associated with higher relapse rates within 12 months. Other studies have shown that the lamina propria inflammatory cell infiltrate or basal plasmacytosis predicts a higher relapse rate within 12 months of colectomy in patients with quiescent clinical and endoscopic disease,23–25 ,27 ,28 although not all studies concur.47 Histological remission is also associated with a reduction in colorectal cancer risk.26 ,29
No histological definition of remission exists despite many histological indices,16 none of which are fully validated. This reflects discontinuous variation in histological activity as a treatment effect and reluctance for invasive investigation when the impact on outcomes is unclear. Our results provide some substance to the value of mucosal biopsy and histological assessment of the worst affected area. At the very least, they imply that maintenance therapy should not be decreased or stopped while microscopic inflammation persists.
Limitations of this study include the design and small number of patients, but these are mitigated by management consistency at a single centre and the long duration of follow-up. The study was underpowered to detect differences with regard to colectomy. Further limitations include an unvalidated endoscopic index of severity (Baron score) that is subject to wide interobserver variability, since the baseline assessment predated a validated index.54 ,57 Truelove and Richards’ Index for grading histological activity is prone to interobserver variability, although it is partially validated.22 It also does not take into account features such as basal plasmacytosis that have been shown to predict patient outcomes. The index is however simple, reproducible and includes a summative scale, unlike the Geboes index.20 Reproducibility of clinical, endoscopic and histological assessment of disease activity in the baseline cohort has been reported separately.34 International initiatives to standardise histopathology for UC are beginning,16 but variables such as the number of biopsies, number of sections and quality of processing need to be agreed upon.58 Other factors such as intercurrent infection or drug-induced lesions may not be resolved by histopathology. Another limitation is the dichotomisation of endoscopic and histological indices into remission or active disease, given the lack of validation of a ‘remission cut-off’ and the lack of control over variables that may have influenced clinical outcomes during the follow-up period, including changes in maintenance therapy, disease extent or smoking. Measurement of faecal calprotectin might have enhanced the study. However, retrospective analysis of mucosal calprotectin in this cohort was not associated with outcomes,59 and another group has been unable to correlate faecal calprotectin and histological activity, even if a low calprotectin was associated with a better clinical outcome.60
In spite of these limitations, we have demonstrated that histological remission represents a target distinct from endoscopic mucosal healing in UC, since it better predicts lower rates of corticosteroid use and acute severe colitis requiring hospitalisation over a median 6 years of follow-up. These data lend weight to the importance of developing standardised and validated scoring indices to measure histological remission. Our findings support the inclusion of histopathology in both IBD clinical trials and practice, which will require a paradigm shift in thinking among clinicians, towards a treatment target of ‘complete remission’ in UC.16
Acknowledgments
The authors gratefully acknowledge the assistance of Paul Bassett in the statistical analyses and the willingness of our patients to contribute to the study. The untimely death of Professor Bryan Warren, friend, tireless teacher and mentor to many, has been a loss to Medicine and to patient care, let alone to the field of Gastrointestinal Pathology in which he was a world expert.
References
Footnotes
Contributors RVB, DB, JD, SPLT—data collection, analysis and drafting of paper; AW, ST, LW, AvH, OB, OAB—data collection; SK, BW—study design.
Competing interests None declared.
Ethics approval Oxfordshire Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.