Article Text

Abstract
Objective The serrated neoplasia pathway accounts for up to 30% of all sporadic colorectal cancers (CRCs). Sessile serrated adenomas/polyps (SSA/Ps) with cytological dysplasia (SSA/P-D) are a high-risk serrated CRC precursor with little existing data. We aimed to describe the clinical and endoscopic predictors of SSA/P-D and high grade dysplasia (HGD) or cancer.
Design Prospective multicentre data of SSA/Ps ≥20 mm referred for treatment by endoscopic mucosal resection (September 2008–July 2013) were analysed. Imaging and lesion assessment was standardised. Histological findings were correlated with clinical and endoscopic findings.
Results 268 SSA/Ps were found in 207/1546 patients (13.4%). SSA/P-D comprised 32.4% of SSA/Ps ≥20 mm. Cancer occurred in 3.9%. On multivariable analysis, SSA/P-D was associated with increasing age (OR=1.69 per decade; 95% CI (1.19 to 2.40), p0.004) and increasing lesion size (OR=1.90 per 10 mm; 95% CI (1.30 to 2.78), p0.001), an ‘adenomatous’ pit pattern (Kudo III, IV or V) (OR=3.98; 95% CI (1.94 to 8.15), p<0.001) and any 0-Is component within a SSA/P (OR=3.10; 95% CI (1.19 to 8.12) p0.021). Conventional type dysplasia was more likely to exhibit an adenomatous pit pattern than serrated dysplasia. HGD or cancer was present in 7.2% and on multivariable analysis, was associated with increasing age (OR=2.0 per decade; 95% CI 1.13 to 3.56) p0.017) and any Paris 0-Is component (OR=10.2; 95% CI 3.18 to 32.4, p<0.001).
Conclusions Simple assessment tools allow endoscopists to predict SSA/P-D or HGD/cancer in SSA/Ps ≥20 mm. Correct prediction is limited by failure to recognise SSA/P-D which may mimic conventional adenoma. Understanding the concept of SSA/P-D and the pitfalls of SSA/P assessment may improve detection, recognition and resection and potentially reduce interval cancer.
Trial registration number NCT01368289.
- COLONOSCOPY
- COLONIC POLYPS
- DYSPLASIA
- GASTROINTESINAL ENDOSCOPY
- COLORECTAL NEOPLASIA
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Sessile serrated adenomas/polyps (SSA/Ps) account for up to 30% of all sporadic colorectal cancers (CRCs).
SSA/Ps are difficult to detect, are often incompletely resected and are strongly associated with ‘interval’ CRC.
There is little existing data on the clinical and endoscopic characteristics of SSA/Ps with cytological dysplasia (SSA/P-D).
What are the new findings?
In a cohort of colonic lesions ≥20 mm referred for endoscopic resection, SSA/Ps were found in 13.4% of patients.
Dysplasia was found in 32.4% of SSA/Ps ≥20 mm.
SSA/P-D was associated with increasing lesion size, increasing age, an adenomatous pit pattern (Kudo III,IV or V) and any 0-Is or nodular component.
High grade dysplasia or cancer was associated with increasing age and any 0-Is or nodular component within the SSA/P.
Prediction of SSA/P-D was poorer where dysplasia was present as the lesion was endoscopically more likely to resemble, and consequently be predicted as a conventional adenoma.
How might it impact on clinical practice in the foreseeable future?
Simple endoscopic features can identify dysplasia within SSA/Ps ≥20 mm. Identification of these higher risk lesions may alter the endoscopic therapeutic strategy, pathology request information and surveillance recommendations. The features identified in larger lesions may be relevant to smaller lesions also, although this requires further study.
SSA/P-D may resemble conventional adenoma. Careful examination of the margins of ‘adenomas’ in the proximal colon may reveal some of them to be SSA/P-D.
SSA/P-D may represent a high-risk transition form of interval cancer. Improved awareness of the clinical and endoscopic characteristics of dysplasia may improve recognition, and reduce interval cancer.
Introduction
The serrated neoplasia pathway accounts for 20–30% of sporadic cancers.1 ,2 Serrated precursor lesions are thought to be a major contributor to the relative failure of colonoscopy in the prevention of proximal colorectal cancer (CRC),3–5 and to the 5–7% of CRCs which occur in the period after complete colonoscopy and prior to surveillance, termed ‘interval’ cancer.6–8 Sessile serrated adenomas/polyps (SSA/P) have been shown to be difficult to detect, variably recognised by endoscopists and pathologists alike and often incompletely resected.9–12 A proportion of SSA/Ps may develop cytological dysplasia (SSA/P-D) which may possess the ability to rapidly progress potentially posing even greater risk for interval cancer.2
Dysplasia within SSA/Ps can assume two broad forms; a serrated morphology or an architecture indistinguishable from conventional adenoma. Many pathologists previously reported this dysplastic change simply by describing the distinct components of the lesion and referred to them as ‘mixed polyps’. This does not reflect the fact that the dysplasia represents higher risk change within a SSA/P, and may have falsely reassured endoscopists. The lesion may also be reported as conventional adenoma if the serrated component is overlooked, disregarded or not included due to incomplete resection by the endoscopist. WHO has emphasised the classification of dysplasia within serrated lesions in its latest statement document,13 and a working party of international experts has echoed this.14 Data to guide surveillance intervals following the detection of serrated lesions is lacking, and although the US Multi-Society Task Force has incorporated SSA/P-D into its recommendations suggesting a 3 year surveillance interval,15 other authorities have suggested shorter periods based on the multiple risk factors that SSA/P-D possess.14 A better understanding of the characteristics of SSA/P-D will facilitate a more scientific approach to developing surveillance guidelines.
To date there is little prospective data on large SSA/Ps. Most data is derived from the study of small (≤10 mm) serrated lesions, generally comprising hyperplastic polyps (HPs), or sessile serrated adenoma without dysplastic change. Even these studies prove difficult to perform as the prevalence of SSA/Ps at colonoscopy in some clinical studies is <2%, and SSA/P-D is reported to comprise 15% of SSA/Ps.12 ,16 This low prevalence may reflect variation in detection and recognition of SSA/Ps, as studies with high detector colonoscopists and expert pathologists demonstrate rates fourfold to sixfold higher,17–19 nevertheless it compounds the difficulties in accumulating cases and results in descriptions of the characteristics and morphology of SSA/P-D being limited to case reports and small series.20 ,21
In light of the difficulty studying a less common and under-recognised entity, we present data from an enriched population of large SSA/Ps in a prospective cohort of sessile or flat colorectal polyps or laterally spreading tumours ≥20 mm referred for endoscopic mucosal resection (EMR). We report on the success of prediction of SSA/Ps within this cohort and the prevalence of SSA/P-D, high-grade dysplasia (HGD) and cancer. We analysed the association of standardised endoscopic imaging features and basic clinical data with the presence of SSA/P-D, HGD and cancer. We then performed a post hoc analysis to identify features predicting SSA/P-D or HGD and cancer in SSA/Ps ≥20 mm.
Methods
Consecutive patients referred to one of eight Australian academic hospitals for the management of large sessile and flat colorectal polyps 20 mm or larger were enrolled in this prospective observational study. (The Australian Colonic Endoscopic Resection (ACE) study; ClinicalTrials.gov NCT01368289). All lesions had been initially identified and referred by a nationally accredited consultant endoscopist. Data were recorded in a comprehensive centralised database from September 2008 to July 2013. Institutional review board approval was obtained at each centre. Written informed consent was obtained from each patient on the day of the procedure. There were no exclusion criteria.
All-EMR procedures were performed by a study investigator or a senior therapeutic endoscopy fellow under direct supervision. All clinical investigators were gastroenterologists with significant prior colonic EMR experience after training in high-volume tertiary referral centres in Australia or overseas. Colonoscopy was performed using Olympus 180 or 190 series high-definition variable-stiffness colonoscopes (180/190 PCF/CF; Olympus, Tokyo, Japan). The EMR technique is standard across all centres, and has previously been described in detail.22 ,23 Data was prospectively collected at the time of patient admission, during, and then immediately after the procedure. Data included patient demographics and comorbidities, American Society of Anaesthesiologists grade and medications. Lesions were carefully examined in vivo by one of the study investigators at the initial endoscopy and classified according to Paris classification and Kudo pit pattern (KPP). Paris classification is a consensus international standard for defining superficial (‘Type 0’) GI lesion morphology.24 Elevated (>2.5 mm above the surrounding normal mucosa) sessile lesions are described as Type 0-Is and sessile lesions under 2.5 mm classed as 0-IIa (slightly elevated), 0-IIb (flat) or 0-IIc (slightly depressed). Excavated lesions are classed as 0-III. Lesions with mixed morphology are described with the dominant component listed first. A laterally spreading, slightly elevated (0-IIa) lesion with an elevated nodule >2.5 mm above the surrounding mucosa (0-Is) is described as 0-IIa+Is. KPP is a classification of the endoscopic appearance of surface mucosal crypts. In brief, KPP type I describes round regular pits associated with normal mucosa, type II stellate pits associated with hyperplastic histology whereas type III and IV patterns are associated with ‘neoplastic’ or adenomatous histology. A type V pattern is a disorganised pit pattern associated with invasive malignancy. The pit pattern analysed in this study was the ‘highest’ KPP noted in the lesion. The proportion of the lesion with each KPP was not recorded. Although initially described using magnification endoscopy, pit pattern can be discerned using high definition endoscopes although this has not been validated experimentally. An overall prediction of the polyp histology was made as part of the assessment prior to resection. Investigators did not employ an algorithm or set criteria to predict histology, and may have used other cues and features to inform their prediction; however, these were not recorded. The presence or absence of dysplasia was not predicted as it was not something that was well known at the start of the study in 2008, and has only become apparent to our group with analysis of the data from this study. Where patients had two or more lesions resected in one procedure, the largest lesion was selected for analysis. Clinical follow-up for the index procedure was obtained at 14 days by structured telephone interview. Histology data was also collected at this time. All authors had access to the study data and reviewed and approved the final manuscript.
Pathological analysis
Histological specimens were analysed at their respective study centre pathology department. Results were then centrally collated on a prospectively maintained database. Serrated lesions, including lesions which contained any serrated morphology were identified and reviewed again by an expert GI pathologist at that centre. Any lesion with insufficient information in the histology report to adequately determine the correct classification was also examined again. Twelve SSA/Ps without cytological dysplasia, resected in 2011–2012, were unable to be formally reviewed so their diagnosis was clarified based on the original report alone. Three hundred and twelve lesions underwent formal review. Sessile lesions were classified according to the most recent WHO classification system (2010)13 as SSA/Ps without cytological dysplasia (or ‘no dysplasia’ SSA/P-ND), SSA/Ps with cytological dysplasia (SSA/P-D) or HP. Traditional serrated adenomas (TSAs) (n=13) or lesions with combined features of TSA and conventional adenoma (n=36) were separately classified. The initial diagnosis was revised in 45 of the 312 lesions reviewed. Nine diagnoses of HP were changed to SSA/P, 3 SSA/Ps were changed to conventional adenoma, 11 SSA/P-NDs were changed to SSA/P-D, 14 SSA/P-Ds were altered to SSA/P-ND, 6 SSA/Ps were changed to TSA and 2 TSAs were altered to SSA/P-D. When dysplasia was present in a SSA/P, the morphology was described as either ‘conventional’ (architectural and cytological changes resembling conventional adenoma) or ‘serrated’ (prominent eosinophilic cytoplasm, vesicular and basally located nuclei and serrated architectural changes).13 ,25 Three lesions that had a histological diagnosis of submucosal invasive cancer only where the underlying polyp type was unclear were reviewed and classified according to the morphology and molecular changes in the CRC. All were thought to have arisen via the conventional pathway to CRC and are not included in this study.
Data analysis
SPSS statistical software (IBM SPSS Statistics, V.22.0. Armonk, New York, USA) was used to analyse the data. The study design was cross-sectional, retrospectively examining demographic, clinical and procedural data at the time of resection and correlating this with histological findings. All analyses were exploratory and two-tailed tests with a significance level of 5% were used throughout. No attempt was made to correct for multiple comparisons. Mann-Whitney U tests were used to test for differences in the distribution of age, lesion size and American Society of Anaesthesiologists grade by bleeding status. The Pearson's χ2 or the Fisher's exact test was used to test for association between categorical variables and outcome. Multiple logistic regression with backward stepwise variable selection was used to identify the independent predictors of outcomes of interest. Logistic regression was calculated on a per-patient basis using the single largest lesion for each patient. Candidate variables with p values for association that were less than or equal to 0.1 on univariable analysis were considered as potential risk factors in multiple logistic regression analysis. ORs with 95% CIs from the model were used to quantify the extent of this association. Any conclusions made in this study should be confirmed in future independent studies.
Results
Between September 2008 and July 2013, a total of 1688 lesions were assessed for resection in 1546 patients, and 268 SSA/Ps (16.4% of lesions) were identified in 207 patients (13.3%).
In patients with SSA/Ps the mean age was 63.8 years (SD 12.3, range 22–88 years), 120 (58%) were female. SSA/P mean size was 29.2 mm (median 30 mm, SD 9.9, range 20–80 mm). Patient characteristics and lesion locations are described in table 1. One hundred and eighty-six lesions (89.9%) were located in the proximal colon (defined as the splenic flexure to caecum). The majority of SSA/Ps were Paris type 0-IIa (74.4%), Is (10.1%), 0-IIa+Is (7.7%) or 0-IIb (6.3%). The remaining 1.4% were grouped together for analysis and made up of lesions with a depressed or excavated component (IIc, IIa+c, 1.5%).
Characteristics of study patients with Sessile Serrated Adenomas/Polyps (SSA/P) ≥20 mm
Histopathology
One hundred and forty SSA/Ps ≥20 mm (68%) were classified as SSA/P-ND and 67 as SSA/P-D (32.4%). Dysplasia was conventional type in 36 lesions and serrated in 31. Fifteen patients had HGD or cancer arising in a SSA/P (7.2%). Eight of these patients (3.9%) had invasive cancer.
Factors associated with SSA/P-D
On a per-patient multivariable analysis, increasing age (OR 1.69 per decade; 95% CI (1.19 to 2.40, p0.004) and increasing lesion size (OR 1.90 per 10 mm; 95% CI (1.30 to 2.78), p0.001), an ‘adenomatous’ pit pattern (Kudo III, IV or V) (OR 3.98; 95% CI (1.94 to 8.15), p<0.001) and any 0-Is component within a SSA/P (OR 3.10; 95% CI (1.19 to 8.12), p 0.021) were associated with SSA/P-D (table 2).
Univariable analysis and best fitting multiple logistic regression model for factors associated with sessile serrated adenomas with cytological dysplasia (SSA-D)
Conventional type dysplasia was associated with an adenomatous KPP (Kudo III, IV or V in conventional dysplasia 28/35 (80.0%), serrated dysplasia 16/31 (51.6%), p 0.015) and there was a weak trend to association with any Paris 0-Is component (0-Is in conventional dysplasia 15/36 (41.7%), serrated dysplasia 7/31 (22.6%), p 0.086). After multivariable adjustment the presence of conventional cytological dysplasia in SSA/P-D was associated with a KPP III, IV or V (OR 3.8; 95% CI 1.26 to 11.1), p 0.017) (figure 1). Hosmer-Lemeshow goodness of fit was adequate and there was no significant evidence of departure from the fitted model.

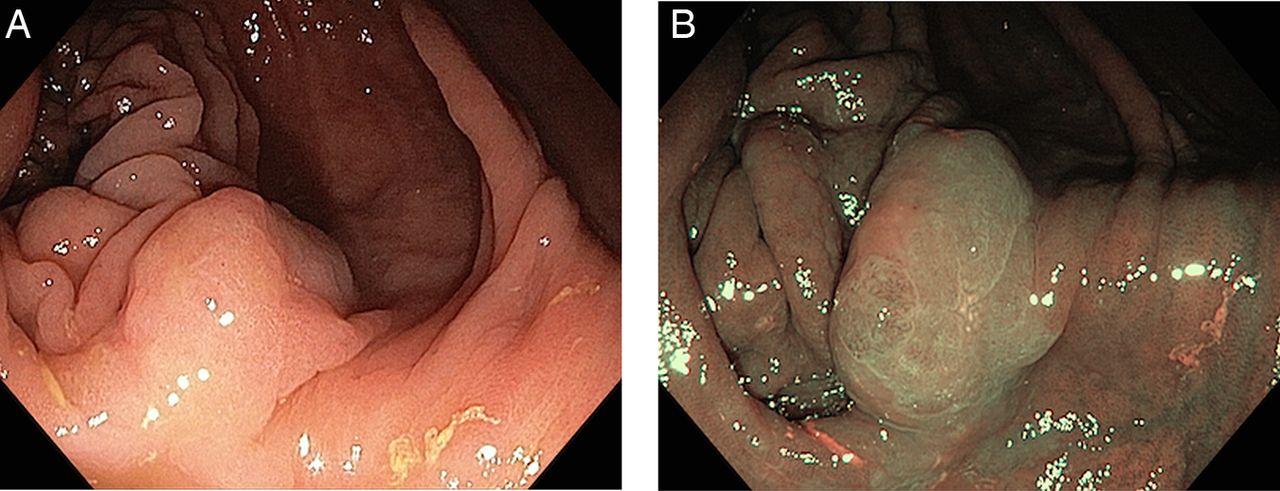
(A) A 20 mm ascending colon 0-IIa+Is sessile serrated adenomas/polyp with cytological dysplasia (SSA/P-D) (conventional dysplasia). The nodular element is visible in the foreground (arrowed). This has a Kudo III pit pattern. The majority of the lesion is covered in adherent mucus. (B) After washing and submucosal injection incorporating indigo carmine, the nodular element is easily distinguishable from the surrounding sessile lesion. A clear and obvious transition in surface morphology can be appreciated. (C) This Paris 0-IIa+Is lesion in the ascending colon is covered with adherent mucus on initial inspection. Two nodules are apparent in the centre of the lesion (arrowed) (D) After submucosal injection, one of the nodules is more clearly defined. The adenomatous pit pattern in the clearly defined nodule becomes distinct from the surrounding typical serrated surface morphology. Histological examination of the nodular component showed conventional type dysplasia. In the context of the surrounding lesion composed of non-dysplastic SSA/P this represents SSA/P-D.
Factors associated with HGD or cancer
Univariable analysis identified increasing age, increasing lesion size, any 0-Is component and an ‘adenomatous’ pit pattern (III, IV or V) as associated with HGD or cancer (table 3).
Univariable analysis and best fitting multiple logistic regression model for factors associated with high grade dysplasia (HGD) or cancer in sessile serrated adenomas/polyps ≥20mm
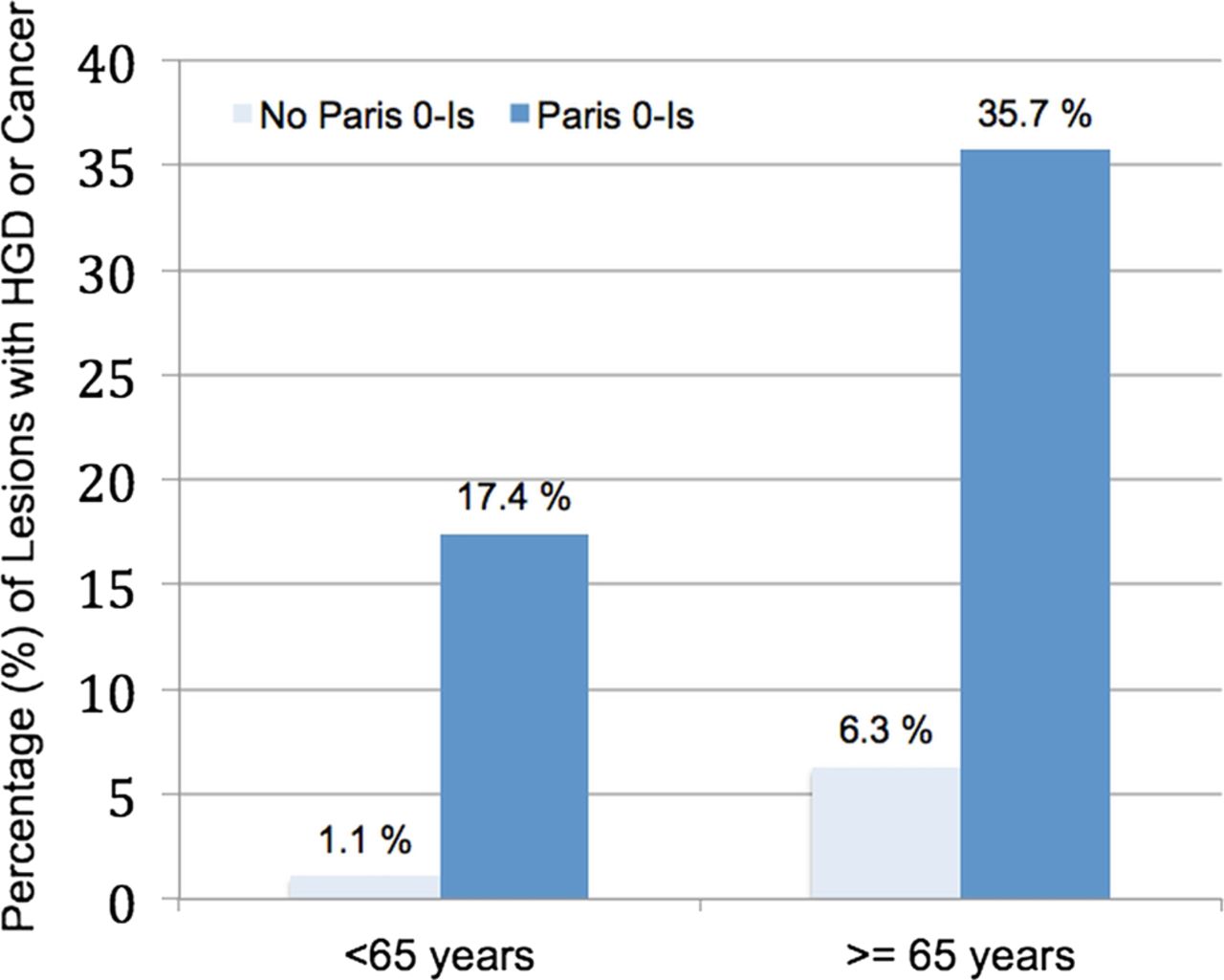
After multivariable adjustment, increasing age (OR 2.0 per decade; 95% CI 1.13 to 3.56), p 0.017) and a Paris 0-Is component (OR 10.2; 95% CI 3.18 to 32.4), p<0.001) were associated with HGD or cancer (table 3). Patients under the age of 65 years without a Paris 0-Is component to their lesion had a low risk of HGD or cancer (1.3%) compared with those over the age of 65 years with a Paris 0-Is component (41.3%) (figure 2). Hosmer-Lemeshow goodness of fit was adequate and there was no significant evidence of departure from the fitted model.

Percentage of sessile serrated adenomas/polyps (SSA/Ps) with high grade dysplasia (HGD) or cancer stratified by age and Paris 0-Is component (p 0.07).
Age correlation with dysplasia
The median age for SSA/P-ND was 64.0 years (SD 12.7), 68.5 years (SD 9.8) for low grade dysplasia (LGD), 67.0 years (SD 12.6) for HGD/cancer (p 0.009).
Prediction of sessile serrated adenomas/polyps
The ability of the study endoscopists to discriminate SSA/Ps was examined across the whole cohort. Data was available in 1509 patients (97.6%) where a prediction of the lesion histology had been recorded. Specificity was high at 96.9% (95% CI 95.8% to 97.1%) and negative predictive value 95.3% (95% CI 94.1% to 96.4%). Sensitivity was 69.8% (95% CI 63.2% to 75.8%), and positive predictive value 77.7% (95% CI 71.3% to 83.3%). Accuracy was 93.2% (95% CI 91.8% to 94.4%). SSA/P-D was over-represented in situations where SSA/P was missed, comprising 55.9% of cases; by comparison it was under-represented in those that were correctly predicted comprising 21% of cases. When prediction was examined according to the presence and type of dysplasia (conventional, serrated or absent (SSA/P-ND)), correct prediction was most common with SSA/P-ND (81.3%) compared with serrated SSA/P-D (54.8%) or conventional SSA/P-D (37.1%), p<0.001 (table 4).
Prediction of sessile serrated adenomas/polyps (SSA/Ps) ≥20 mm and sessile serrated adenomas/polyps with cytological dysplasia (SSA/P-D) ≥20 mm
Discussion
Colonoscopy has been shown to be an effective tool in the prevention of colorectal cancer, however several studies have also exposed its weaknesses. Colonoscopy provides less protection against proximal compared with distal CRC,3–5 and cancer diagnosed in the 3–5 year interval prior to surveillance colonoscopy, or ‘colonscopy (CS) interval CRC’,26 comprises 3–7% of the total disease burden of CRC.7 ,8 Multiple causes for these weaknesses have been proposed, however serrated lesions are emerging as a significant factor. The clinical or endoscopic predictors of dysplasia or cancer in SSA/Ps are not well defined and no studies specifically examine large SSA/Ps, a critical area where transition to cancer may be more likely to be evident.
SSA/Ps are implicated in the occurrence of interval CRC for several reasons. First, interval CRC is biologically and epidemiologically linked to serrated lesions.8 ,27 ,28 SSA/Ps develop hypermethylation of CpG promoter regions (CpG island methylator phenotype (CIMP)), resulting in inactivation of mismatch repair genes such as MLH-1 and microsatellite instability (MSI). Hypermethylation of MLH-1 and MSI are characteristically found in the dysplastic foci of SSA/P-D21 ,29 and are thought to represent a transition form to the 12% of CRC which is BRAF mutated, CIMP+ and MSI high.1 Second, SSA/Ps may be missed as they are difficult for endoscopists to detect being indistinct and flat, with a paucity of surface vessels and often a shrouding mucous cap.30–32 A third link to interval cancer is incomplete resection.33 This was highlighted in the Complete Adenoma Resection study which demonstrated that residual polyp was present after hot snare polypectomy in 31.0% of SSA/Ps compared with 7.2% of conventional adenomas.9 Large SSA/Ps (10–20 mm) were at particularly high risk, with residual polyp noted in 47.6%. SSA/Ps may resemble conventional adenoma, whereby only the dysplastic focus is seen by the endoscopist and the surrounding non-dysplastic component is not appreciated rendering it at risk of incomplete resection. This aspect of conventional adenoma mimicry is exemplified in our multicentre study where a group of advanced endoscopists have frequently incorrectly labelled these SSA/Ps-D as adenomas. If a small portion of a SSA/P-D lesion is left in situ, there is the potential for it to progress to CRC. Once dysplasia has developed progression to cancer may be rapid.21 ,34 Similar mismatch repair defects found in Lynch syndrome can quickly progress to MSI cancer35 and there have been reports of CRC developing from SSA/Ps within short intervals.36 Finally, pathologists can exhibit considerable interobserver variation in the reporting of serrated lesions.37 SSA/P-D with combined serrated and conventional adenomatous morphology have been misleadingly labelled as ‘mixed’ polyps13 and if the non-dysplastic component of a SSA/P-D is overlooked, disregarded or not included due to incomplete resection by the endoscopist, the lesion may be simply reported as a conventional adenoma. Interval cancer is therefore a significant risk due to the combined effects of these factors; poor detection, incomplete resection and failed recognition potentially resulting in inappropriate surveillance intervals.
In our study of SSA/Ps ≥20 mm resected by EMR at tertiary centres, SSA/Ps were found in 13.3% of patients and cytological dysplasia (SSA/P-D) was noted in 32.4% of SSA/Ps. Cancer occurred in 3.9%. The prevalence of SSA/Ps in this study was high, although the true population prevalence remains in doubt. The enriched population in our study represents an advantage in terms of the accumulation of advanced and large SSA/Ps for study, and notably nearly a third of lesions had a focus of dysplasia. SSA/P-D has been infrequently reported or absent in previous studies, which have typically been comprised of small lesions. The largest study to report on SSA/P-D is a retrospective analysis of a pathology database by Lash et al16 examining 179 111 patients in the USA and demonstrating a SSA/P prevalence of 1.7%, 15% of which were SSA/P-D. Bouwens et al38 studied SSA/P-D in a large population attending for colonoscopy at a university hospital in the Netherlands with a similarly low prevalence of SSA/P (2.9%) and found that even in this population of smaller polyps (50.1%<6 mm), dysplasia was present in 37% and high grade dysplasia in 9.2%.
The endoscopic characteristics of SSA/P-D are poorly defined. The only current data is derived from a retrospective analysis of endoscopic images, finding only that SSA/Ps-D were more likely to be dome-shaped than SSA/Ps-ND.38 One study has reported on SSA/Ps expressing adenomatous pit patterns, however this study noted that these changes were associated with an increased likelihood that a SSA would be BRAF mutated and CIMP positive, and did not specifically examine the prediction of dysplasia by KPP.39 In our study, we have identified simple tools that may be applied by all endoscopists to facilitate identification of SSA/P-D. The finding of a distinct area or transition point where the pit pattern changes to a III or IV pattern suggests the development of an area of dysplasia, and a nodular area within an uniform flat or slightly elevated sessile lesion may likewise suggest this. Even without a thorough knowledge of the KPP, it is likely that dysplasia within the lesion can be appreciated as a transition point. The dysplastic area may exceed the growth rate of the underlying SSA/P, potentially creating a nodule and resulting in only a rim or small area of residual non-dysplastic serrated polyp, which as demonstrated by our results may be missed by the endoscopist who visualises only a lesion which appears to be a typical conventional adenoma. Dysplastic change was also associated with increasing age and lesion size, further discriminators for the endoscopist to consider in ascribing risk to SSA/Ps. HGD or cancer was present in 7.2% in our study, and was associated with increasing age, and any Paris 0-Is component to the lesion. Among patients >65 years of age who had a SSA/P with a 0-Is component, HGD or cancer was found in 35%, however patients without these features had negligible risk (1.1%). Endoscopists should consider this age-related risk when assessing large SSA/Ps with potential dysplasia.
The findings in this study were not preconceived by anecdote or experience, but were discerned by targeted analysis of the multicentre data to determine discriminatory factors. The endoscopic discriminators are gross features and were not uniformly present in all lesions with dysplasia, however this may be because the KPP was assessed as the majority component to the lesion, and a Paris 0-Is component is typically an easily discernable and dominant area raised 2.5 mm from the surrounding mucosa. A flat, bland SSA/P with a predominantly Type II KPP would have been assessed as Paris 0-IIa and Kudo II even if it contained a diminutive, minimally raised nodular element or transition to an adenomatous pit pattern consistent with an early area of dysplasia (figure 3). Prospective assessment of these potentially subtle endoscopic features is likely to be far more sensitive for the presence of dysplasia. We have recently reported that SSA/P-D is characterised by two key features; a transition point defining the change from the bland features of a non-dysplastic component of a SSA/P to the adenomatous surface morphology of dysplasia, and a nodule, even if not meeting the criteria for a 0-Is nodule. In this series 70% of conventional dysplasia was associated with a nodule.40

(A) A large sessile serrated adenoma/polyp with cytological dysplasia (SSA/P-D) in the ascending colon with conventional type dysplasia. The majority of the lesion displays the typical surface morphology of a SSA/P. (B) Closer examination with narrow band imaging reveals a flat 3–4 mm focus of the lesion to have an adenomatous Kudo type III surface morphology consistent with an area of conventional adenomatous dysplasia. This is seen more clearly with the use of magnification. (C) In addition, the margins of the lesion are revealed to extend beyond the dominant central nodule (arrows).
Limitations of this study include the potential for interobserver variation among the pathologists. This has been reported in serrated lesion classification, however all cases were reviewed by subspecialty GI pathologists and with the release of the updated 2010 WHO guidelines recent studies have shown very good reproducibility among pathologists.41 Molecular studies were not performed to document underlying serrated pathway mutations, hence SSA/P-D with conventional adenomatous morphology and without residual SSA/P that were endoscopically and pathologically assessed to be conventional adenomas may have been missed. It was logistically impossible to review again all conventional adenomas in the study to ensure SSA/Ps were not missed, although this is likely to have been a low yield exercise as the diagnosis of conventional adenoma is well established and without molecular studies SSA/Ps histologically mimicking conventional adenoma would have been missed anyway. Ideally mutational analysis of the non-dysplastic and dysplastic components in each lesion would allow analysis of the shared or differing molecular aetiologies, but this was not possible in this study. Lesions were endoscopically assessed on the day of the procedure by the endoscopist performing the resection, and variation between endoscopists may have introduced bias into the results. The fact that the study numbers were large, and the endoscopists were all highly experienced may have mitigated this. The study population was comprised of lesions over 20 mm in size and although this may appear to limit applicability for general colonoscopy it has been shown that the prevalence of dysplasia in smaller lesions may be equally as high.38
In 2008 when the ACE study was designed, SSA/P-D was incompletely understood, not thought to be detectable endoscopically and often not recognised as a high-risk or significant lesion. This lack of a preconceived notion of the features and form of dysplasia in SSA/Ps influencing endoscopists’ prediction was important in reducing information bias. Among the goals at study inception, the ACE study aimed to use simple endoscopic assessment tools to classify large colonic mucosal lesions and link these to histological, clinical and resection outcomes. Using these simple tools applied to a large number of prospectively classified SSA/Ps we have determined by post hoc statistical analysis key factors that predict advanced SSA/Ps. In turn, by examining these lesions, we have highlighted the fact that SSA/P-D may mimic conventional adenoma, deceiving even experienced endoscopists (figure 4). The implications of these findings are important. With appreciation of the endoscopic features of SSA/P-D, prospective studies may significantly improve the detection and recognition of SSA/P-D. Careful examination of the margins of ‘adenomas’ in the proximal colon may actually reveal some of them to be SSA/P-D, potentially altering the endoscopic therapeutic strategy, pathology request information and surveillance recommendations. Our group of advanced endoscopists incorrectly predicted adenoma in a significant proportion of cases of SSA/P however there may be room to substantially improve this prediction with an understanding of the nuances of SSA/P-D. Apparently innocuous SSA/Ps may contain a small area with dysplasia significantly elevating their risk for imminent or inevitable progression and emphasising to the endoscopist the need to ensure complete removal (figure 5).

(A) A large sessile serrated adenoma/polyp without cytological dysplasia (SSA/P-ND), characterised by a bland appearance, mucus cap and sessile (Paris 0-IIa) morphology. (B) Photomicrograph of a H&E slide demonstrating SSA/P-ND. Crypts are dilated with horizontal growth along the muscularis mucosa and branching. (C) Photomicrograph of a H&E slide demonstrating sessile serrated adenoma/polyp with cytological dysplasia (SSA/P-D) with conventional adenoma-like morphology. Typical changes of SSA/P-ND are seen at the bottom right. At the upper left and bottom left, there is low grade cytological dysplasia characterised by nuclear enlargement, elongation and stratification with less obvious serration of crypt epithelium and lacking cytoplasmic eosinophilia. (D) SSA/P-D with conventional type dysplasia. Part of the lesion in the foreground displays a bland appearance with a surface morphology consistent with SSA/P (yellow arrow), however the raised nodular component of the rest of the lesion has a surface morphology more consistent with conventional adenoma. This area represents dysplastic change and marks the lesion as SSA/P-D. Endoscopists may easily mistake this lesion for a conventional adenoma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) A 20 mm 0-IIa lesion in the caecum. On initial inspection, this appears to be a bland sessile polyp with features consistent with a sessile serrated adenoma without dysplasia. (B) On closer inspection with narrow band imaging, a nodule with an altered pit pattern is discernable representing a focus of dysplasia. Histopathological examination revealed the lesion to be a sessile serrated adenoma with cytological dysplasia (SSA/P-D).
In conclusion, we have shown that SSA/P-D is present in a significant proportion (32.4%) of SSA/Ps over 20 mm in size and cancer occurs in 3.9%. SSA/P-D is associated with increasing age, increasing lesion size, lesions with a Paris 0-Is component and an adenomatous pit pattern (III, IV or V). Conventional type dysplasia is more likely to exhibit an adenomatous pit pattern than serrated dysplasia. HGD or cancer is present in 7.2% and associated with increasing age, and any Paris 0-Is component to the lesion. A renewed appreciation that SSA/P-D is endoscopically identifiable with simple tools, yet may also mimic conventional adenoma, may allow endoscopists to actively and accurately identify these lesions. This increased awareness may also promote further research into improving detection, recognition and complete resection of SSA/P-Ds and reduce rates of interval cancer.
Acknowledgments
The authors acknowledge the work of the following contributors who reviewed pathological cases: Dr Hema Mahajan, Institute of Clinical Pathology and Medical Research, Westmead Hospital, Sydney, NSW. Dr Mark Bettington, ENVOI Pathology/QIMR Berghofer Medical Research Institute, Brisbane, QLD. Assoc Prof Andrew Clouston, ENVOI Pathology, Brisbane, QLD. Dr Chris Dow, Dorevitch Pathology, Melbourne, VIC. Prof Prithi Bhathal, Melbourne Pathology, Melbourne, VIC. Dr Alan Pham, Alfred Health Pathology, Melbourne, VIC. Assoc Prof Andrew Ruszkiewicz, SA Pathology, Adelaide, SA. Dr Andrina McGivern, Princess Alexandra Hospital, Brisbane, QLD. Prof Priyanthi Kumarasinghe, Sir Charles Gairdner Hospital, Perth, WA.
References
Footnotes
Collaborators Hema Mahajan; Mark Bettington; Andrew Clouston; Chris Dow; Prithi Bhathal; Alan Pham; Andrew Ruszkiewicz; Andrina McGivern; Priyanthi Kumarasinghe.
Contributors NGB designed the study, collected organised and analysed data, performed statistical analyses, wrote the manuscript and revised the manuscript after review by the coauthors. MP, KSN, LFH, SAZ, GJB, RS, SJW, SCR, DO and AM identified and recruited patients, performed procedures, collected data and critically reviewed the manuscript. KB advised on and performed statistical analysis of data. HPN and DML collected, organised and reviewed histological and pathogical specimens and critically reviewed the manuscript. MJB initiated, designed and led the study, identified and recruited patients, performed procedures, collected data, co-wrote the manuscript and critically reviewed the manuscript.
Funding NGB was supported by a funding grant from the Westmead Medical Research Foundation (WMRF). The Cancer Institute New South Wales provided funding for a research nurse and data manager to assist with the administration of the study. There was no influence from the WMRF or the Cancer Institute on study design or conduct, data collection and management, analysis, interpretation, preparation and review or approval of the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.