Article Text

Abstract
Objective To assess the efficacy and safety of endoscopic resection of large colorectal polyps.
Design Relevant publications were identified in MEDLINE/EMBASE/Cochrane Central Register for the period 1966–2014. Studies in which ≥20 mm colorectal neoplastic lesions were treated with endoscopic resection were included. Rates of postendoscopic resection surgery due to non-curative resection or adverse events, as well as the rates of complete endoscopic removal, invasive cancer, adverse events, recurrence and mortality, were extracted. Study quality was ascertained according to Newcastle-Ottawa Scale. Forest plot was produced based on random effect models. I2 statistic was used to describe the variation across studies due to heterogeneity. Meta-regression analysis was also performed.
Results 50 studies including 6442 patients and 6779 large polyps were included in the analyses. Overall, 503 out of 6442 patients (pooled rate: 8%, 95% CI 7% to 10%, I2=78.6%) underwent surgery due to non-curative endoscopic resection, and 31/6442 (pooled rate: 1%, 95% CI 0.7% to 1.4%, I2=0%) to adverse events. Invasive cancer at histology, non-curative endoscopic resection, synchronous lesions and recurrence accounted for 58%, 28%, 2.2% and 5.9% of all the surgeries, respectively. Endoscopic perforation occurred in 96/6595 (1.5%, 95% CI 1.2% to 1.7%) polyps, while bleeding in 423/6474 (6.5%, 95% CI 5.9% to 7.1%). Overall, 5334 patients entered in surveillance, 502/5836 (8.6%, 95% CI 7.9% to 9.3%) being lost at follow-up. Endoscopic recurrence was detected in 735/5334 patients (13.8%, 95% CI 12.9% to 14.7%), being an invasive cancer in 14/5334 (0.3%, 95% CI 0.1% to 0.4%). Endoscopic treatment was successful in 664/735 cases (90.3%, 95% CI 88.2% to 92.5%). Mortality related with management of large polyps was reported in 5/6278 cases (0.08%, 95% CI 0.01% to 0.15%).
Conclusions Endoscopic resection of large polyps appeared to be an extremely effective and safe intervention. However, an adequate endoscopic surveillance is necessary for its long-term efficacy.
- ENDOSCOPIC POLYPECTOMY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Endoscopic resection is usually recommended for the treatment of large colorectal polyps.
What are the new findings?
In a systematic review on 6442 patients, endoscopic resection appeared to be effective in preventing surgery in 92% of the cases.
Endoscopic resection appeared also to be a safe technique with surgery for adverse event limited to 1% of the patients.
The main reason for endoscopic resection failure was represented by invasive cancer at histology.
Endoscopic recurrence occurred in nearly 14% of the cases, and it was amenable to further endoscopic treatment in most cases.
Endoscopic submucosal dissection appeared to reduce dramatically the risk of recurrence, but not of surgery for invasive cancer.
How might it impact on clinical practice in the foreseeable future?
These findings stress the importance in optimising and standardising endoscopic resection techniques for large polyps.
Introduction
Large (≥2 cm) colorectal polyps represent a critical issue in lower GI endoscopy. These lesions represent the morphological stigmata of the progression of a precancerous precursor into an invasive cancer due to the intimate relationship between polyps size and risk of malignancy.1 Thus, the expected benefit of endoscopic resection in term of colorectal cancer (CRC) prevention is substantial.
These lesions are often considered the most technically challenging to remove endoscopically because of their large size or, in some instances, flat shape or because of a location that is difficult to access. The common use of piecemeal technique rather than en bloc resection increases the risk of postresection recurrence. This risk is most important if there is suboptimal adherence to postresection endoscopic surveillance.2 However, the implementation in recent decades of new types of endoscopic resection—such as endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD)3 ,4– allowed endoscopy to approach large non-polypoid superficial neoplasia, such as lateral spreading tumours or large depressed lesions, further reducing the need of surgery for precancerous lesions. On the other hand, endoscopic resection of large lesions exposes patients to a higher risk of adverse events, including perforation and bleeding compared with resection of smaller lesions.5 ,6
Although the efficacy and safety of endoscopic resection for large polypoid or non-polypoid lesions has been addressed in several cohorts, there is persistent uncertainty regarding several issues. Most of the series included only a relatively small number of patients due to the low prevalence of these large lesions. This prevents definitive data on relatively infrequent, but clinically relevant outcomes, such as postresection surgery or recurrence. Second, most of the studies were performed in tertiary centres, generating doubt on the generalisability of the data. Third, there is heterogeneity in the resection technique adopted due to variable techniques for EMR and increasing implementation of ESD.
Our aim is to do a systematic review and a meta-analysis assessing the main indicators of efficacy and safety of endoscopic resection of large polyps in order to provide reliable estimates on the outcome of this relevant procedure.
Methods
Methods of analysis and inclusion criteria were based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.7
Eligibility criteria
We considered all clinical studies (involving human subjects) for the period 1966 to 28 April 2014, in which ≥20 mm colorectal (epithelial) neoplastic lesions were treated with endoscopic resection, and the main endoscopic and surgical outcomes were reported. Animal and review studies were excluded. If there was any suspicion of cohort overlap between studies, only the most recent study was included. The terms large polyps or large colorectal neoplasia are both used here to indicate ≥20 mm polypoid or non-polypoid colorectal neoplastic lesions that were selected for endoscopic resection.
Information sources
Relevant original publications (in English language) were identified in MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials. Prespecified Medical Subject Headings (MeSH) and non-MeSH terms were used for the search and are reported in online supplementary appendix 1. In general, search terms and the related hierarchy were selected in order to be sensitive enough to retrieve all the articles dealing with the study subject, with low specificity (ie, selection of non-pertinent articles). This was due to substantial heterogeneity in the terminology on large colorectal neoplasia in endoscopic series. Abstracts were not included because of the detailed information needed for this systematic review. Additional publications were identified through searching the reference lists of retrieved papers. When further information from selected papers was needed, we attempted to contact the authors (see online supplementary appendix 2).
Study selection
All titles and abstracts of papers retrieved in the prespecified search were screened by two reviewers (CH, AZ). By using the full report of the study (3° step), studies were evaluated for inclusion in the analysis. Any disagreements were resolved through consensus. Data were extracted from the included studies by one reviewer (CH) and checked by a second reviewer (AZ), and the data were extracted into tables. Any disagreements were resolved through discussion with a third reviewer (DKR).
Data collection process and list of items
From each paper, the reviewers independently abstracted the following information: (1) country; (2) publication year; (3) enrolment period; (4) duration of enrolment in years (difference between the last and the first years of the enrolment period); (5) setting (single centre/multicentre); (6) study design (prospective/retrospective, according to the timing of the events under study in relation to the time the study begins or ends: prospective refers to events concurrent with the study, and retrospective refers to use of historical events);8 (7) application of advanced endoscopic resection techniques (EMR and/or ESD); (8) size cut-off for the definition of large polyps (20/30/40 mm); (9) number of patients with at least one ≥20 mm colorectal lesion; (10) number of ≥20 mm colorectal lesions; (11) mean size of the large polyps; (12) mean/median age of the patients with large polyps; (13) gender distribution; (14) morphological (sessile/pedunculated/non-polypoid) and (15) site distribution (proximal/distal) of the lesions; (16) number of patients in whom endoscopic resection was not attempted; (17) endoscopic technique (snare-polypectomy/EMR/ESD); type of resection (piecemeal/en bloc); (18) systematic use of argon-plasma coagulation (APC) or (19) endoscopic clips; (20) outcome of endoscopic resection at endoscopy (rate of success/failure); (21) rate of invasive cancer at histology (submucosal or deeper infiltration), irrespective of the decision to proceed or not to surgery; (22) rate of post-(endoscopic) resection surgery for unsuccessful resection; (23) rate of surgery for invasive cancer or (24) rate of surgical resections for other reasons (eg, synchronous invasive CRC); (25) setting of endoscopic resection (in-hospital admission/outpatient); (26) rate of patients in whom ≥1 sessions to complete endoscopic resection was needed; (27) rate of intraprocedural or (28) postprocedural bleeding; (29) rate of perforation; (30) rate of surgery for adverse event (ie, bleeding or perforation); (31) availability and (32) mean/median duration of post-(endoscopic) resection follow-up; (33) number of patients included and (34) rate of lost at follow-up; (35) mean number of surveillance colonoscopies per patient; (36) performance of systematic biopsies from scar; (37) whether surveillance started from the first negative surveillance endoscopy; rate of (38) early (ie, ≤6 months after resection) or (39) late recurrence; (40) outcome of endoscopic treatment of the recurrence (successful/failure); (41) rate of invasive cancer at recurrence; (42) rate of surgery for recurrence; and (43) mortality rate due to management or progression of large colorectal lesions. In the few cases where only the number of large polyps—but not of patients—was available, the former was used for the purposes of our analysis.
Risk of bias in individual studies
Information on the methodological quality of each included study was recorded and quality assessment was performed using the Newcastle-Ottawa Scale (NOS).9 ,10 Representativeness of the study cohorts, ascertainment of exposure, demonstration that outcome of interest was not present at start of study, assessment of outcome and adequate length of endoscopic follow-up were assessed for each study. Two variables of NOS, namely selection of the non-exposed cohort and comparability of cohorts on the basis of the design or analysis, were not evaluated since cohorts not exposed to endoscopic resection were not represented in the included studies.
Summary measures
The primary endpoints of this systematic review were the rates of surgery for non-curative endoscopic resection of colorectal polyps ≥20 mm in diameter (incomplete removal, invasive cancer at histology, synchronous invasive cancer, recurrence) and adverse events related to the endoscopic resection (bleeding and perforation). Secondary endpoints were the rates of (a) complete endoscopic resection, (b) invasive cancer, (c) adverse events, (d) polyp recurrence at follow-up, (e) invasive cancer at follow-up, (f) successful endoscopic treatment of any recurrence, (g) as well as the different indications for surgery, (h) the rate of patients lost at follow-up, (i) the impact of ESD on surgery for non-curative resection and recurrence, and (j) the mortality rate related with the management of large polyps. We also assessed the rate of patients who underwent surgery before any attempt of endoscopic resection.
Planned methods of analysis
Data on the primary and secondary endpoints were extracted when available. For each endpoint, we analysed data obtained from different studies to determine pooled rates and the 95% CIs. The 95% CIs around these means were calculated by using exact binomial procedure. Heterogeneity among studies was estimated using Cochran’s Q (reported with a χ2 value and p value)11 and the I2 statistic, the latter describing the percentage of variation across studies that is due to heterogeneity rather than chance,12 and presented with a 95% CI. I2, unlike Q, does not inherently depend upon the number of studies considered, with values of 25%, 50% and 75% taken to indicate low, moderate and high levels of heterogeneity, respectively. Where heterogeneity was high (I2>75%), random effects models were used for summary statistics.13 For the primary endpoint, potential sources of heterogeneity were investigated further by arranging groups of studies according to potentially relevant characteristics and by meta-regression analysis. Factors examined both individually and in multiple variable models included socio-demographic attributes—such as geographic origin of the studies, sex and mean patient age—and methodology-related attributes—such as study design, study period, study sample size, endoscopic techniques (classified into those with only ESD and those with EMR with or without ESD) and patient enrolment. Factors with p<0.25 individually were entered into a multiple regression model to avoid model instability. Meta-regression analysis was performed by using random effect model and used logit (the natural log of odds—the division of the proportion by 1 minus the proportion) transformation of the postendoscopic surgery rate. The regression coefficients for each study characteristic on individual analysis were provided to enable comparison across diagnoses. The exponential of the regression coefficients gives an estimate of the relative change in the odds of having a postendoscopic surgery either for a unit increase in the explanatory variable (for variables measured on a continuous scale) or for each category relative to the odds of baseline category (for categorical explanatory variables). Publication bias evaluation was performed by Duval and Tweedie's Trim and Fill method.14 Egger's and Peters regression15 was also used to test for funnel plot asymmetry. The small study effect was also evaluated by cumulative analysis (cumulatively adding studies according to sample size of primary studies—from largest to smallest sample size). Briefly, primary data were ordered from high to low precision (from the largest to the smallest study), and meta-analyses were run in a step-wise fashion using the first (most precise) estimate, then the first two estimates and so on until the entire sample was fully analysed. While other methods are available, advantages of this approach are that the analysis is transparent and focused on estimates with greater information value due to their greater precision. Less precise estimates are those that are more likely to be biased on selectivity grounds. This also is a form of sensitivity analysis since results from cumulative analyses can be compared with full sample estimates or summary estimates can be examined for shifts and drift as more studies are added to the analysis16 ,17 All analyses were done in R statistical software package, V.2.15.2.18 A p value of <0.05 was considered statistically significant.
Results
Study selection
The study flow chart is shown in figure 1. In total, 923, 1043 and 230 studies were identified by the searches in PubMed, EMBASE and Cochrane Central Register of Controlled Trials (including bibliographic search), respectively. After reviewing titles and abstracts, 184 studies were found to be eligible and reviewed in full text. Of these, 50 studies were included in the analyses, while 134 were excluded (reasons listed in online supplementary appendix 3)

Flow chart of the systematic review.
Characteristics of the included studies
Main characteristics of the included studies are provided in tables 1 and 2. Overall, 38 (76%) studies were performed in Western countries, the remaining 12 being located in Asia. Eight (16%) series were published in the period 1977–1999, 11 (22%) between 2000 and 2007, and 31 (62%) after 2007. Median of the mean duration of the enrolment per study was 5 years (range: 1–21 years in 46 studies). Most of the studies were single centre (41, 82%), and 9 (8%) were multicentre. The majority (29, 58%) were retrospective.
Main characteristics of the included studies
Main characteristics of the study populations in the included studies
Participants
In most of the studies (37, 74%), the cut-off to define a large polyp was 20 mm, but in 12 (24%) and 1 (2%) series it was 30 and 40 mm, respectively (table 2). Overall, data from 6442 patients with at least one ≥20 mm polyp were included in the meta-analysis. The median of patients included per study was 89 (range: 22–505). Distribution of the population age and sex was available for 42 and 40 series, respectively. Medians of study ages and male sex were 67 (range: 60–84 years) and 54% (range: 18–78%), respectively. The cumulative number of ≥20 mm colorectal lesions included was 6779. Mean size was reported in 38 series, the median being 33 mm (range: 20–51). Morphological distribution was available for all but two series. Overall, 6089/6625 (91%) polyps were non-pedunculated (sessile or non-polypoid). Site distribution was available in 45 series. In detail, 2804/5977 (47%) large lesions were in the proximal colon, the remaining 3173 being in the distal tract.
Interventions
Advanced techniques of endoscopic resection (EMR, 29 series; ESD, 6 series; ESD and EMR, 5 series) were available in 40 (80%) studies, while snare polypectomy was the only technique applied in 10 (20%) series (table 3). In detail, polypectomy, EMR and ESD were performed in 1679/6449 (26%), 3592/6449 (56%) and 1178/6449 (18%) cases, respectively (data available for 47 series). Data on type of endoscopic resection were available in 39 series, being piecemeal in 3066/4933 (62%) and en bloc in 1867/4933 (38%). In particular, 928/1867 (50%) en bloc resections were reported in the ESD series. Information on type of current adopted, systematic use of APC or endoscopic clipping was reported only by a few articles (see online supplementary appendix 4), excluding further analysis. As detailed in online supplementary appendix 7, systematic biopsy of the postresection scar at surveillance was performed only in five series.
Main characteristics of the technique of endoscopic resection in the included series
Outcomes
Information on the success rate of endoscopic resection, as well as on the rate of surgical resection for failure of endoscopic resection, due to either incomplete removal or adverse events, was available for all series (tables 4 and 5). All but two series also reported the rate of surgery due to invasive cancer. Only a few series reported on whether patients were admitted for endoscopic resection (see online supplementary appendix 4). All but one series reported on the rate of postendoscopic perforation (irrespectively of the surgical treatment), while two studies did not report the rate of postendoscopic bleeding, and an additional 16 studies did not clearly differentiate between intraprocedural and extra-procedural bleeding. All but two studies included endoscopic or clinical follow-up, and two additional studies did not clarify how many patients were lost to follow-up. All but 11 studies reported the mean duration of the follow-up, and all (but the two studies without follow-up information) detailed the rate of endoscopic recurrence (including progression to cancer), as well as the related surgical treatment or mortality. Only a small minority of the studies reported on the actual mean number of surveillance endoscopies, and whether surveillance started from the index resection or from the first endoscopic assessment of a complete resection (see online supplementary appendix 4). On the other hand, 21 series did not differentiate between early (ie, 6 months) and late recurrence. Overall, 16 studies reported information on how many patients underwent surgery before any attempt of endoscopic resection, mainly because of the endoscopic appearance suggestive for submucosal invasion.
Primary outcomes in the individual studies
Multivariate meta-regression of the logit of prevalence of postendoscopic surgery due to non-curative resection according to socio-demographic, methodological and clinical characteristic
Risk of bias assessment
Selection bias
Representativeness of the exposed cohort
No major selection bias was identified (see online supplementary appendix 5). Only in one retrospective study19 patients with invasive cancer within large lesions were a priori excluded, so that only large precancerous lesions were included. Polyp size was evaluated at endoscopy in all series, generating uncertainty on whether the size measurements were correct. However, pathological assessment of size is not feasible in the case of piecemeal resection. All the studies only included patients in whom the large lesions were considered amenable to endoscopic therapy, and the endoscopic criteria to refer large lesions directly to surgery without an attempt at endoscopic resection remain vague.
Ascertainment of exposure
All patients were included based on an endoscopic and/or histological report. Exposure to surveillance endoscopy was documented in all studies.
Outcome bias
Assessment of outcome
Postendoscopic surgery for either non-curative resection or adverse event was consistently reported by all the studies, but subindications for surgery were unclear in some series. When defining non-curative resection at endoscopy, lack of feasibility in removing the lesion was mixed with histological detection of invasive cancer in most series. Endoscopic perforation was reported consistently across the series, although most of the studies failed to provide a clear definition or workup of perforation. Similarly, bleeding and its timing (intraprocedural/postprocedural) were described/defined with substantial heterogeneity among the studies. Although most series reported on the number of polyps with invasive cancer, most did not clearly classify the lesions as low versus high risk for metastatic disease (superficial vs deep submucosal invasion). Follow-up was not systematically planned/registered in most series. Thus, information on the actual number of patients who entered or were lost to follow-up was quite heterogeneous across the series. In non-operated patients, detection of recurrence at endoscopic surveillance was the only available outcome regarding neoplasia, although some uncertainty may be due to the inability to redetect the site of original endoscopic resection.
Length and adequacy of follow-up
The main discriminator among the individual studies was the adequacy of follow-up. In 17 series, it was considered inadequate, mainly for its short duration. Thus, our results may underestimate the true postendoscopic recurrence rate.
Synthesis of results
Primary endpoints
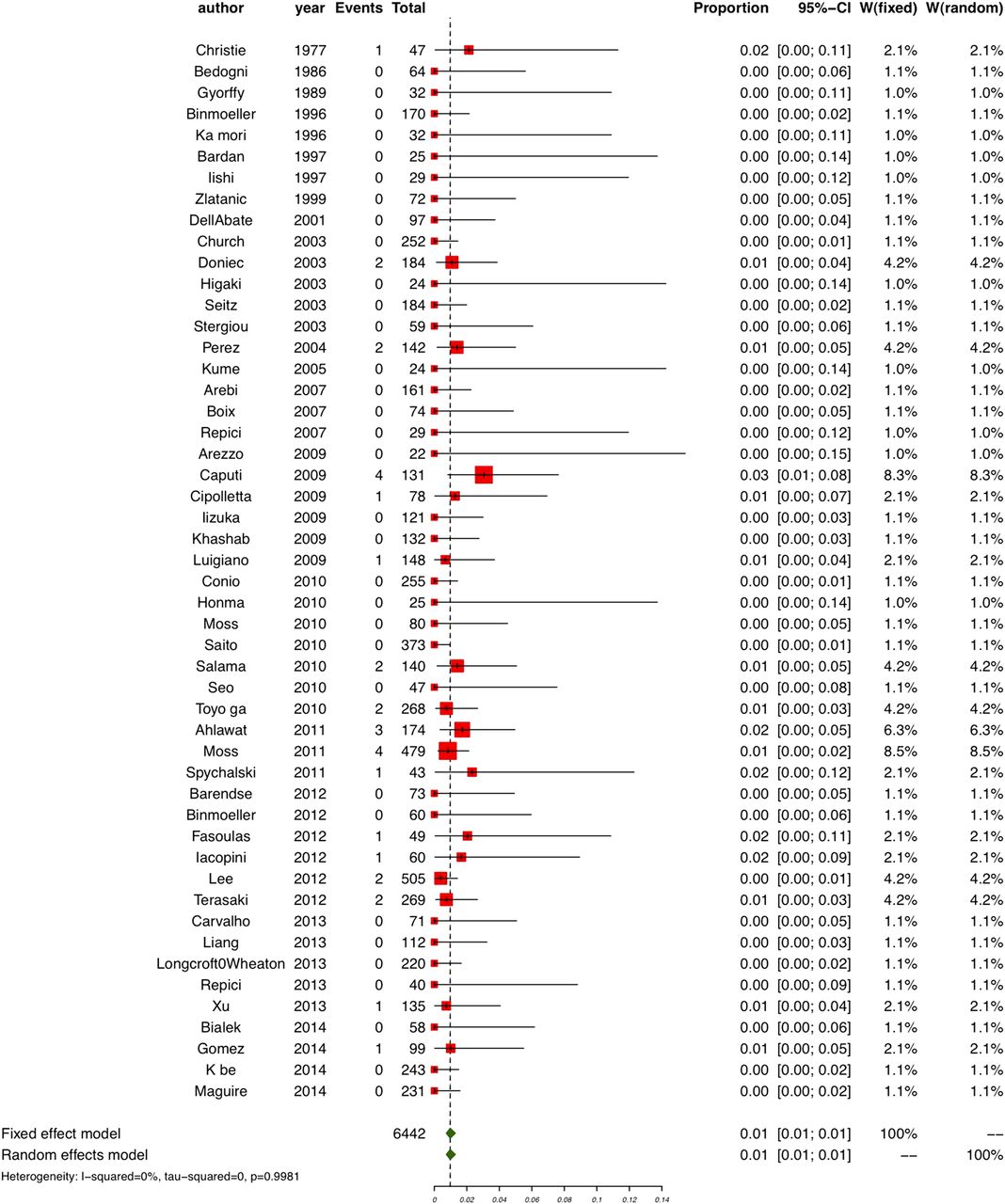
Following endoscopic resection of a ≥20 mm polyp, a total of 534 (8.3%) patients underwent surgery for any reason, with a random effect pooled rate of 8% (95% CI 7% to 10%) (tables 4 and 5, figures 2 and 3, online supplementary appendix 6). This estimate was associated with substantial heterogeneity among the studies (χ2=229.22, p<0.001, I2=78.6%, 95% CI 72.2% to 83.5%; see figure 2). Of the 534 surgeries, 31 were due to adverse events, while 503 were due to non-curative resection. As shown in figure 3, no significant heterogeneity (χ2=25.2, p=0.998, I2=0%, 95% CI 0% to 0%) was detected in the analysis of rates of surgeries for adverse events from different studies (pooled estimate, 1%; 95% CI 0.7% to 1.4%).

Rate of postendoscopic resection surgery. Chronologically order by year of publication (random effects model).
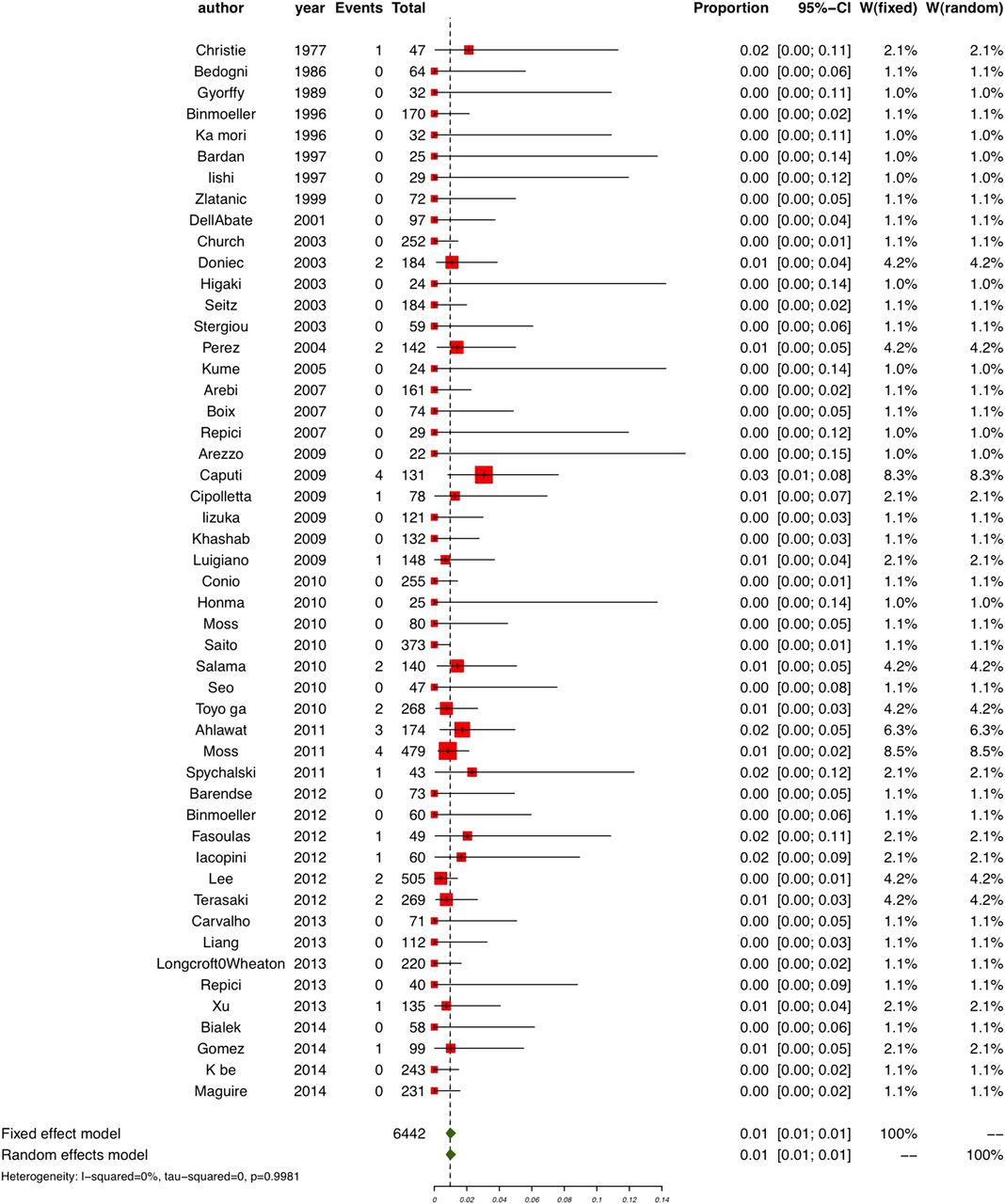
Rate of postendoscopic resection surgery due to adverse events. Studies are ordered by year of publication. Both fixed effects and random effects parameters are shown.
The random effect pooled rate of surgeries due to non-curative resection was 7.4% (95% CIs 6% to 9%), with substantial heterogeneity across the studies (χ2=236.34, p<0.001, I2=79.3%, 95% CI 73.1% to 84%), as shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of postendoscopic resection surgery due to non-curative resection. Chronologically order by year of publication (random effects model).
Individual variable meta-regression analyses are reported in online supplementary appendix 6. At multivariate analysis (table 5), the only variables that remained weekly significantly associated with the pooled rate of postendoscopic surgeries due to non-curative resection among studies were ‘patient enrolment’ (≥29 vs <29 patients per year; 10.0% vs 6.1%; p=0.05, random effects model) and ‘mean age of the study population’ (>67 vs ≤67 years; 8.7 vs 5.7; p=0.05, random effects model). No other variable appeared to be statistically significantly associated with the selected outcome. In particular, the average rate of surgeries for non-curative resection was 7.9% (95% CIs 3% to 20.8%) in studies where only ESD was used, while the average rate for studies using various endoscopic techniques was 8.4% (95% CIs 6.7% to 10.8%; p=0.9).
Secondary endpoints
Surgery
Of the 503 surgeries for non-curative resection, 310/6442 (4.8%, 95% CI 4.3% to 5.3%) operations were due to invasive cancer, 150/6442 (2.3%, 95% CI 1.9% to 2.7%) to non-curative resection of precancerous lesions, 12/6442 (0.2%, 95% CI 0.1% to 0.4%) to reasons other than the endoscopic resection (synchronous cancer, 11 cases, perforation for a small polyp, 1 case) and 31/6442 (0.5%, 95% CI 0.3% to 0.6%) to a not endoscopically manageable (residual) recurrent lesion at surveillance endoscopy, corresponding to 58% (310/534), 28% (150/534), 2.2% (12/516) and 5.9% (31/534) of all the postendoscopic surgeries, the remaining 5.9% (31/534) being due to adverse events (see online supplementary appendix 7). Overall, 248/1797 (14%; 95% CI 12% to 15%) patients underwent surgery before any attempt of endoscopic resection.
Endoscopy
At per polyp level, endoscopic resection, irrespectively of postendoscopy surgery and (in some series) histology, was deemed as successful in 6530/6779 (96.3%, 95% CI 96% to 97%) cases (see online supplementary appendix 7). At histology, invasive cancer was diagnosed in 491/6301 endoscopic resections (7.8%, 95% CI 7.1% to 8.5%) (data not available for three series). Endoscopic perforation occurred in 96/6595 (1.5%, 95% CI 1.2% to 1.7%) polyps (not reported for one series), and bleeding in 424/6474 (6.5%, 95% CI 5.9% to 7.1%) polyps (not reported for three series). Thirty-two series differentiated between intraprocedural and postprocedural bleeding, and postprocedural bleeding accounted for 98/304 (32%) of all the bleeding episodes with an estimated incidence of 95/3585 (2.6%, 95% CI 2.1% to 3.2%) endoscopic resections.
Follow-up
When limiting the analysis only to those patients in whom endoscopic surveillance was indicated, 5334/5836 entered into surveillance, and 502/5836 (8.6%, 95% CI 7.9% to 9.3%) were reported as lost to follow-up (46 series) (table 6). Median of the mean length of follow-up was 2 years (range: 0.4–4.5 years, 39 series). Endoscopic recurrence was detected at surveillance in 735/5334 patients (13.8%, 95% CI 12.9% to 14.7%; I2: 90%), also corresponding to an incidence rate of 90 cases per 1000 person-years of follow-up. When comparing those series in which only ESD was used with the remaining series, ESD appeared to reduce the risk of endoscopic recurrence (5/508, 1% vs 730/4826, 15%; p<0.01). In the 19 series where this information was retrievable, endoscopic recurrence occurred early in 257/320 (80%) cases and was delayed in the remaining 63 cases. When focusing on the very few series that reported the actual number of surveillance colonoscopies performed (see online supplementary appendix 6), endoscopic recurrence rate was higher in the series reporting ≥2 colonoscopies for at least part of the initial study population compared with those who reported only one (68/253, 27% vs 30/399, 7.5%; p<0.01). It was also higher in those series that reported the systematic performance of biopsy on postresection scar compared with the remaining series (113/596, 19% vs 622/4738, 13%; p<0.01, online supplementary appendix 6). Detection of invasive CRC at follow-up occurred in 14/5334 patients (0.3%, 95% CI 0.1% to 0.4%) corresponding to 1.9% (14/735) of all recurrences. This was due to a recurrence of a previously removed polyp with already invasive cancer in four cases (ie, treated without surgery), while it was a new diagnosis of invasive cancer at recurrence in the remaining 10 cases. Endoscopic treatment of recurrence was reported as successful in 664/735 cases (90.3%, 95% CI 88.2% to 92.5%), and (see also above) surgery was needed in 31/735 cases (4.2%, 95% CI 2.8% to 5.7%).
Secondary outcomes on the follow-up of endoscopic resection in the individual studies
Mortality directly due to endoscopic or surgical management of larger polyps was reported in 5/6278 cases (48 series) corresponding to a rate of 0.08% (95% CI 0.01% to 0.15%).
Publication bias
We evaluated the possibility of publication bias for the main outcome. Egger's regression (p<0.001) and the Trim and Fill test (see online supplementary figure 1 appendix 8) were positive, suggesting the presence of small studies effects, which can be attributable to publication bias or other factors (eg, heterogeneity, chance). However, the pooled effect size adjusted for publication bias was statistically similar to the original effect (observed postendoscopic surgery rate: 8%, 95% CIs 7% to 10%; seven studies imputed: adjusted postendoscopic surgery rate 9%; 95% CIs 7% to 11%). Moreover, according to Peters regression (using a function of study size as predictor variable), there was no evidence of bias due to publication bias (p=0.393). A cumulative meta-analysis was also used as a publication bias method (see online supplementary figure 2 appendix 8). The results indicate that less precise estimates cause some shift, although it is fairly small. The pooled rate of postendoscopic surgeries obtained with the inclusion of the 10 largest studies (including over 200 patients individually), with a cumulative sample size of >2600 patients, was 7%, 95% CIs 4% to 13%. As less precise studies were added, the pooled rate estimate showed a slight drift higher such that by the time the cumulative sample size reaches 5383 (37 studies including >60 patients individually), the mean was 8%, 95% CIs 6% to 10%. The point estimate and its confidence levels did not shift with the addition of another 10 smaller studies.
Discussion
According to our analysis, endoscopic resection appears to be an effective and safe intervention, sparing surgery in >90% of the cases with only a low and acceptable risk of severe adverse events. In detail, the risk of surgery due to adverse events appeared to be as low as 1%, indicating that endoscopic resection of large polyps has a favourable risk/benefit ratio. Although the risk of endoscopic recurrence affected one in every seven patients, such risk appeared to be highly manageable at endoscopy and there was a very low risk of progression to cancer during follow-up. The very low mortality associated with the endoscopic approach to these lesions—one every 1250 patients—confirms the intrinsic safety of endoscopic resection.
We chose the need for surgical resection after endoscopic resection as the primary endpoint for the study. The need for surgery after endoscopic resection reflects both the success of the endoscopic intervention (complete endoscopic resection without cancer in the specimen) and also the age, comorbidities and expectations of patients. Thus, the rate of invasive cancer in polyps (7.8%) exceeded the rate of surgery for this indication (4.8%). Surgery represents a solid outcome corresponding to the end of the endoscopic treatment or follow-up of the endoscopic resection. Pathological or endoscopic criteria—such as R0 resection or lack of endoscopic recurrence—would appear weaker endpoints, when considering that the majority of the resections were performed with piecemeal technique and that the operator's skills, methods and technical tools (eg, advanced endoscopic imaging or biopsy on endoscopic scar) may affect the rate of endoscopic recurrence. Similarly, the rate of surgery related to adverse events is more clinically meaningful and consistent endpoint compared with the simple rate of adverse events. Although the definition of endoscopy-related bleeding was unclear and heterogeneous across the studies, it may be presumed that the decision to proceed to surgery consistently indicated a severe clinical evolution of bleeding. This may also be true to some extent for perforation since the recognition may be affected by the level of clinical suspicion and the radiological technique used for diagnosis.20
There are other concerns on the use of endoscopic recurrence as main endpoint of endoscopic recurrence. Only a few series actually reported on the actual number of surveillance endoscopies per patient performed. Additionally, in virtually all of the few reported cases, it was one surveillance colonoscopy per patient. Although based on a few series, the risk of recurrence appeared higher in those series reporting >one surveillance colonoscopy compared with those reporting only one. Thus, the real risk of recurrence is likely to be underestimated by the lack of consecutive surveillance colonoscopies. Second, only a small minority of the studies required a systematic histological assessment of postresection scar. Of note, the risk of recurrence appeared to be higher in those few series where such assessment was performed, so that the inability to include microscopic recurrences at surveillance may have further underestimated the real risk of recurrence. Third, in most series surveillance started from the index resection, and not by the first negative control. Thus, most of the detected recurrences are more likely to be residual of an incomplete resection rather than real recurrences of a complete resection. Consequently, a substantial proportion of apparent recurrences would be recategorised as residual part of the index lesion in case the first colonoscopy after a doubtful endoscopic resection was considered as a workup rather than as a surveillance procedure. This bias also prevents a clear assessment of the early and late risk of recurrence so that there is still uncertainty on the real timing of surveillance after an endoscopically proven complete endoscopic resection. For all these reasons, we maintain the correctness of using postresection surgery, and not endoscopic recurrence, as the main endpoint of our analysis.
The relatively low rate of surgery after endoscopic resection means that any future technique designed to improve the efficacy of endoscopic resection will face a substantial challenge to demonstrate improvement over current endoscopic treatment. For instance, ESD failed to reduce the rate of surgery for non-curative resection, mainly due to a similar rate of invasive cancer in the two groups. Although ESD was able to reduce the risk of postresection recurrence, the actual relevance of this finding is uncertain when considering that the vast majority of recurrences are benign and amenable to additional treatment. This has been recently confirmed in a large prospective cohort study, where most of the post-EMR recurrences were diminutive and amenable to endoscopic treatment.3
Despite the favourable risk/benefit ratio, we confirmed that management of endoscopically resectable large polyps is demanding. At least 8% of the patients reported a severe adverse event, and this rate likely underestimates the true rate since adverse events were not systematically collected in most studies.
The correctness of our estimates is strengthened by the quality examination of the included studies. The selection of the cohorts in each study was performed on the basis of endoscopic/histological data so that it is unlikely that recall or other selection bias could have affected the validity of our study.
There are limitations to our analysis. Most studies were either single centre or retrospective. This underlines the usefulness of a systematic review in which each study acts as putative centre in a hypothetical multicentre study, as well as the importance of selecting strong endpoints, in order to minimise the risk of reporting bias. Second, it remains poorly defined how authors selected which large lesions were potentially candidates for endoscopic treatment versus those immediately referred to surgery, and the criteria certainly differed between centres and endoscopists. However, irrespectively of the criteria adopted, most of the large lesions appeared amenable to endoscopic resection, only 14% being directly sent to surgery. Third, endoscopic criteria for identification of invasive cancer were not available for much of the study interval, and similarly the high definition and magnification colonoscopes necessary to identify these features were frequently not available. In future studies, the risk of cancer may be lower after successful exclusion of patients based on endoscopic evidence of deep submucosal invasion. Finally, our meta-analysis collected data from series across a large time period during which endoscopic techniques have evolved considerably. However, all these factors were considered in the multivariate model.
In our large pooled population, we clearly showed the efficacy and safety of endoscopic resection of large polyps. These findings stress the importance of optimising and standardising endoscopic resection techniques, especially when considering the implementation of population CRC screening campaigns in several European countries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors All authors contributed to study concept and design; acquisition of data; and drafting of the manuscript. CH and CS contributed to analysis and interpretation of data; and statistical analysis.
Competing interests DR: Olympus—research support; CH: Endochoice and Given Imaging—research support.
Provenance and peer review Not commissioned; externally peer reviewed.