Article Text

Abstract
Objective Lower GI bleeding (LGIB) is a common reason for emergency hospital admission, although there is paucity of data on presentations, interventions and outcomes. In this nationwide UK audit, we describe patient characteristics, interventions including endoscopy, radiology and surgery as well as clinical outcomes.
Design Multicentre audit of adults presenting with LGIB to UK hospitals over 2 months in 2015. Consecutive cases were prospectively enrolled by clinical teams and followed for 28 days.
Results Data on 2528 cases of LGIB were provided by 143 hospitals. Most were elderly (median age 74 years) with major comorbidities, 29.4% taking antiplatelets and 15.9% anticoagulants. Shock was uncommon (58/2528, 2.3%), but 666 (26.3%) received a red cell transfusion. Flexible sigmoidoscopy was the most common investigation (21.5%) but only 2.1% received endoscopic haemostasis. Use of embolisation or surgery was rare, used in 19 (0.8%) and 6 (0.2%) cases, respectively. 48% patients underwent no inpatient investigations. The most common diagnoses were diverticular bleeding (26.4%) and benign anorectal conditions (16.7%). Median length of stay was 3 days, 13.6% patients rebled during admission and 4.4% were readmitted with bleeding within 28 days. In-hospital mortality was 85/2528 (3.4%) and was highest in established inpatients (17.8%, p<0.0001) and in patients experiencing rebleeding (7.1%, p<0.0001).
Conclusions Patients with LGIB have a high burden of comorbidity and frequent antiplatelet or anticoagulant use. Red cell transfusion was common but most patients were not shocked and required no endoscopic, radiological or surgical treatment. Nearly half were not investigated. In-hospital mortality was related to comorbidity, not severe haemorrhage.
- GASTROINTESTINAL BLEEDING
- ENDOSCOPY
- GASTROINTESTINAL SURGERY
- INTERVENTIONAL RADIOLOGY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Lower GI bleeding (LGIB) is a common reason for urgent hospitalisation and red blood cell (RBC) transfusion.
Endoscopy, radiology and surgery have a role in the management of LGIB but their use, timing and access in UK hospitals is unclear.
What are the new findings?
Bleeding from colonic diverticula was the most common source, accounting for 26% cases, followed by benign anorectal bleeding in 17% cases.
Only 29% cases had an inpatient endoscopic evaluation, followed by CT in 26% cases. Endoscopic haemostasis was used in only 2% cases (8.4% of those undergoing inpatient endoscopy).
Mesenteric embolisation or surgery was used in <1% cases.
Mortality was 3.4%, with the majority of deaths attributed to comorbidity.
How might it impact on clinical practice in the foreseeable future?
Forty-eight per cent patients had a benign course requiring no intervention and could have been managed without hospital admission.
Critical appraisal of inappropriate RBC transfusion for LGIB is needed.
The value of inpatient colonoscopy for acute LGIB is questionable and is a key priority for further research.
Introduction
Lower GI bleeding (LGIB), traditionally defined as bleeding arising distal to the ligament of Treitz, is a common acute medical and surgical emergency, with an estimated incidence of 33–87/100 000.1 ,2 Commonly reported sources of bleeding include colonic diverticula, haemorrhoids and polyps.3 ,4 Presentation can range from self-limiting bleeding to life-threatening haemorrhage and interventions include transfusion, upper and lower endoscopy, diagnostic or therapeutic radiological studies and surgery. In the UK, GI bleeding is the most common indication for red blood cell (RBC) transfusion after haematological malignancy; over one-third of these transfusions are for LGIB.5
In contrast to upper GI bleeding (UGIB), there is a paucity of data describing modes of presentation, comorbidities, the use of diagnostic and treatment modalities and clinical outcomes. The limited evidence base to inform treatment guidelines was recognised in the American College of Gastroenterology Guidelines6 and the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) in the UK.7
This national audit on the management of LGIB was conducted in 2015 and attempted to cover the whole of the UK. The project was endorsed by multiprofessional bodies, including the Association of Coloproctology of Great Britain and Ireland, the British Society of Gastroenterology and the British Society of Interventional Radiology.8 In this paper, we describe the characteristics of patients with LGIB, the diagnostic and therapeutic interventions used and clinical outcomes including mortality and length of hospital stay.
Methods and analysis
We conducted a prospective UK-wide audit of adults presenting to hospital with LGIB. The study protocol has previously been published in full.9 This audit was undertaken as part of the NHS Blood and Transplant National Comparative Audit of Blood Transfusion programme, which supports research to improve the evidence base for transfusion in patients with GI bleeding.10 ,11 The methodology of this audit was similar to a previously conducted national audit on UGIB,12 which led to detailed evaluations of the processes of care13 ,14 and informed treatment recommendations worldwide.15
This audit collected data on established methods of care, involved no intervention and included no patient identifiers. It is therefore not subject to ethical consideration by the NHS Research Ethics Committee.16 As stated in the National Health Service Code of Practice, patient information may be collected for clinical audit without prior patient consent.17
Participants
In 2015, there were 174 National Health Service (NHS) hospitals accepting acute admissions. All were invited to participate in June 2015.9 The audit was also advertised to NHS hospitals in Scotland, Wales and Northern Ireland via their national blood services. Hospitals received no specific funding, and participation and data entry relied entirely on the goodwill of the medical staff.
Case definitions
Hospitals were asked to prospectively identify consecutive cases of LGIB from 1 September 2015 for 2 months. Unselected patients presenting with LGIB or developing LGIB while admitted for another reason were eligible if they fulfilled the following criteria: age ≥16 years, history of bright or dark blood per rectum, maroon coloured stool, blood mixed in with stool, clots per rectum or passage of melaena without haematemesis. Definitions are provided in box 1.
Study definitions
Acute lower GI bleeding (LGIB)
Bright or dark blood per rectum, maroon coloured stool, blood mixed in with stool, clots per rectum or passage of melaena without haematemesis
Clinically significant bleeding
Bleeding associated with systolic blood pressure <100 mm Hg, heart rate ≥100 bpm and ≥1 unit red blood cell transfusion
Shock
Heart rate ≥100 bpm and systolic blood pressure <100 mm Hg.
Continued bleeding
The requirement of ≥2 units red blood cell and/or a decrease in haematocrit ≥20%18
Rebleeding (further bleeding)
Additional transfusion requirements and/or a decrease in haematocrit ≥20% after 24 hours of clinical stability.18
Readmission due to further LGIB
Further episodes of LGIB that result in an unplanned admission to hospital, within 28 days of discharge
In-hospital mortality
All-cause mortality up to 28 days after admission with LGIB
Inclusion criteria were deliberately broad to optimise case identification, but inevitably meant the capture of some UGIB cases. These were identified using presenting features and findings at oesophagogastroduodenoscopy (OGD) and categorised as definite, probable or suspected UGIB (see online supplementary material).
Supplemental material
Data were collected until hospital discharge, death or day 28 (whichever occurred first). Readmission data were collected until 28 days postdischarge. Where necessary, hospitals were contacted to provide extra data until April 2016.
Data collection
Demographic data, observations, laboratory results, endoscopy and radiology reports, operation notes and discharge data were obtained for each patient and entered into an online, bespoke database, which was accessed by a site-specific, password-protected website. Comorbidities were collated using the Deyo modification of the Charlson Comorbidity Index,19 a score based on combinations of comorbidity, which can be used to predict 1-year mortality.20 This was amended to allow use in a clinical setting (see online supplementary table S1). On case completion, the central audit team was alerted and the dataset checked real-time for any missing mandatory data. This process was conducted daily throughout the study period to maximise data completeness. Case ascertainment and data collection were piloted in 10 hospitals.9
Data handling
Data were exported and screened for duplicates. The discharge diagnosis was determined by using a diagnostic hierarchy (see online supplementary material), which was then mapped to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Missing data are reported for each variable.
The development of audit standards was limited by the lack of national guidance on LGIB. Standards were adopted from transfusion and UGIB guidelines,21 ,22 or where none exist, expert consensus and published a priori in the study protocol.9
Statistical methods
Data are reported as numerator and percentage or median and IQR as appropriate. Categorical data are compared using χ2 test and continuous data by Wilcoxon rank-sum test. The ability of Charlson Comorbidity Index to discriminate mortality, rebleeding and readmission was examined by calculating the area under the receiver operating characteristic curve. Statistical analysis was undertaken using SAS V.9.4 (SAS Institute, North Carolina, USA).
Results
Of 174 hospitals invited, 143 (82.2%) participated, identifying 2781 potential cases of LGIB. After exclusions (figure 1), there were 2528 LGIB cases for analysis. Most cases were admitted under general surgery (2105/2528, 83.3%), 310/2528 (12.3%) under general medicine and only 54/2528 (2.1%) under gastroenterology. Gastroenterology admissions were younger (median age 59 years, IQR 43–80) than those admitted to general medicine (74 years, IQR 50–84, p<0.05) or general surgery (73 years, IQR 58–83, p<0.01).
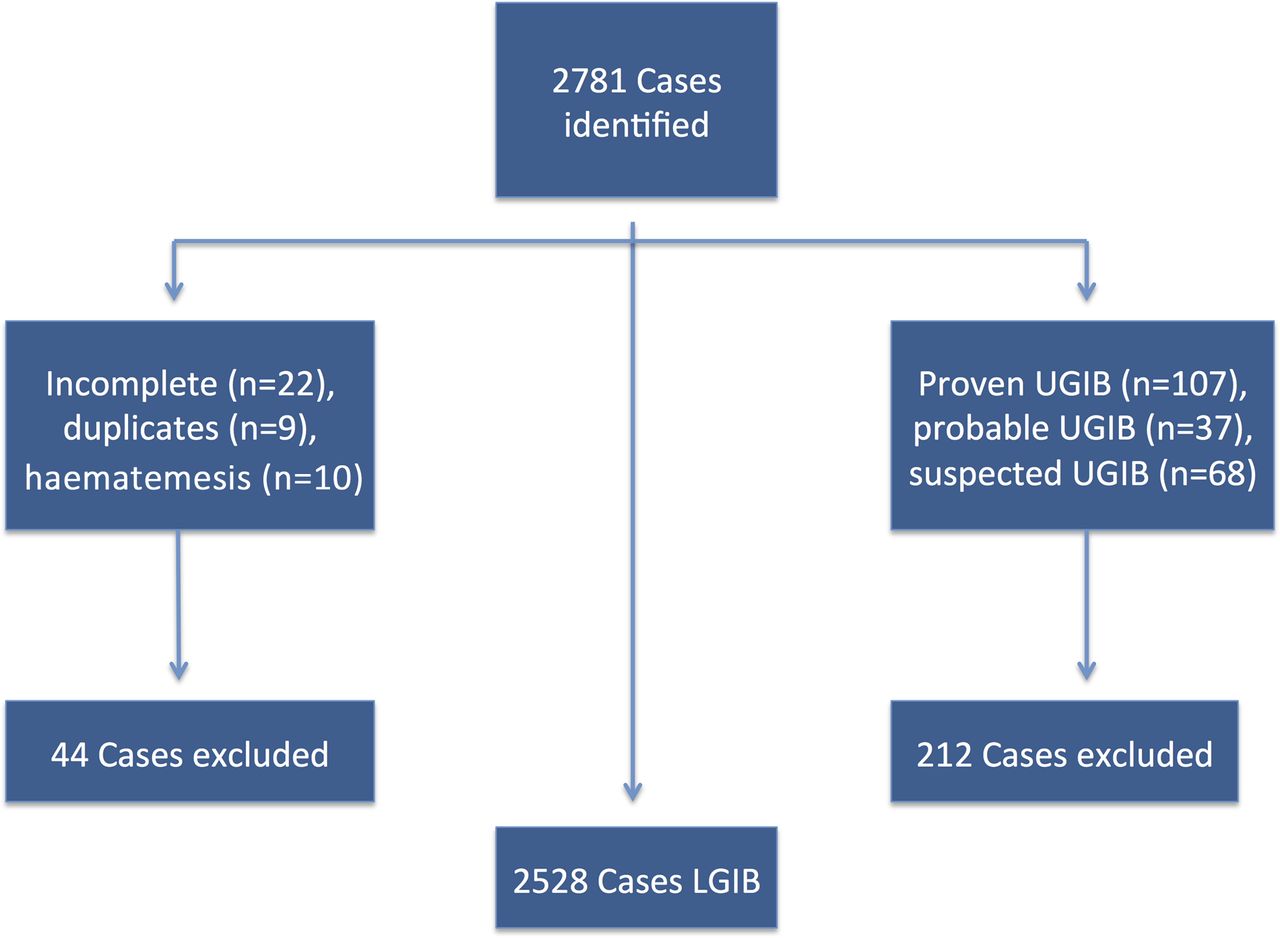
Flow chart of excluded and included cases. LGIB, lower GI bleeding; UGIB, upper GI bleeding.
Characteristics and presenting features of patients with LGIB
The median age was 74 years (57–83); 1319/2528 (52.2%) female and 1455 (57.6%) had a Charlson Comorbidity Index ≥1. Malignancy, diabetes and myocardial infarction (MI) were the most common comorbidities.
Patients who developed LGIB while hospitalised for another reason (inpatient bleeds) represented 185/2528 (7.3%) of cases. They were older (median age 73 vs 78 years, p<0.001) with more comorbid illness, including diabetes (21.6% vs 14.4%), stroke (16.2% vs 8.0%) and MI (16.2% vs 10.9%) in comparison to new admissions.
Bright red blood per rectum was the most common presenting symptom, and was more common in acute admissions than inpatient bleeds. Inpatients were more likely to present with melaena, clots per rectum and shock. Presentation with haemodynamic shock was uncommon, reported in 58/2528 (2.3%) cases. Anaemia was also uncommon (median haemoglobin (Hb) 122 g/L, full range 36–192); only 272/2528 (10.8%) presented with Hb ≤80 g/L. Overall, 408 (16.1%) patients had previously been admitted with LGIB, 95/408 (23.3%) in the preceding 28 days (table 1).
Presenting features and demographics of patients admitted with or developing LGIB while an established inpatient
Medications
At the time of presentation, 742/2528 (29.4%) patients were taking antiplatelet agents; 584 (23.1%) taking aspirin. Warfarin use was reported in 270 (10.7%) and direct oral anticoagulants (DOACs) in 131 (5.2%) patients (table 1). Aspirin was withheld in 417/584 (71.4%, missing data in 21 cases) for a median duration of 4 days (IQR 2–7), and clopidogrel in 167/235 (71.1%, missing data in 13) for a duration of 4 days (IQR 2–7). Most patients had their DOAC stopped (116/131, 88.5%) for a duration of 4 days (IQR 2–7). Five patients with DOAC also received prothrombin complex concentrate and three fresh frozen plasma (FFP). Warfarin was withheld in 236/270 (87.4%) cases, for a duration of 3 days (IQR 2–6).
Most patients had normal coagulation profiles on presentation (median international normalised ratio (INR) 1.1, IQR 1.0–1.2). There were 267/2528 (10.6%) cases presenting with an INR >1.5, and 58 (2.3%) with an INR ≥5 (INR missing in 404). Of those presenting with an INR >1.5, 195/267 (73.0%) were taking warfarin, 26 were taking a DOAC, 3 had liver disease and 1 had a congenital bleeding disorder.
Use of blood components
RBC transfusion was administered in 666/2528 (26.3%) cases with 258 (10.2%) receiving ≥4 units (table 2).
Inpatient interventions for LGIB
Most patients were transfused with an Hb >8.0 g/L, 190/666 (28.5%) with an admitting Hb >10.0 g/L, Shock was uncommon even in patients transfused at higher Hb thresholds (see online supplementary table S2). Early transfusions (within 12 hours of presentation) accounted for only 153/405 (37.7%) transfusions that were given with Hb >8.0 g/L. Although most patients met the criteria for restrictive transfusion, most were not managed in accordance with this practice (see online supplementary table S3). Only 117/599 (19.5%) eligible patients were transfused at an appropriate threshold (Hb <7.0 g/L in patients who do not have major haemorrhage or acute coronary syndrome)21 and only 115 (19.2%) were transfused to an appropriate Hb target (Hb 7.0–9.0 g/L).21 FFP and platelet transfusion are discussed in the online supplementary material.
Endoscopy and endoscopic haemostasis
In 99/136 (72.8%) hospitals, 24/7 lower GI endoscopy was available (see online supplementary table S4). The remainder provided this service only during normal working hours and used an agreed referral protocol to another hospital, or on ‘ad hoc’ provision by on-call teams and emergency theatres.
The most frequent inpatient investigation was flexible sigmoidoscopy, used in 543/2528 (21.5%) cases. OGD (285, 11.3%) and colonoscopy (99, 3.9%) were used less frequently. Capsule endoscopy and push enteroscopy were rarely used (table 2).
The highest diagnostic yields were on flexible sigmoidoscopy (418/543, 77.0%) and colonoscopy (71/99, 71.7%). Bedside proctoscopy or rigid sigmoidoscopy was undertaken in 73/2528 (2.9%) patients. Of the 2455 patients who did not undergo proctoscopy or rigid sigmoidoscopy, 526/2455 (21.4%) had an inpatient flexible sigmoidoscopy, with readily identifiable anorectal pathologies (anal cancer, anal fissures, haemorrhoids and rectal prolapse) identified in 69/526 (13.1%) of these.
The median time to procedure was 3 days (IQR 2–5) for flexible sigmoidoscopy, 2 days (IQR 1–4) for OGD and 4 days (IQR 2–7) for colonoscopy. The majority of flexible sigmoidoscopes and colonoscopes were performed in the endoscopy department (475/543, 87.5%, missing data in 17, and 85/99, 85.9%, missing data in 1, respectively), with 39/543 (7.2%) flexible sigmoidoscopes and 10/99 (10.1%) colonoscopes performed in emergency theatre. Forty-four patients underwent a repeat lower GI endoscopy: 14 for further bleeding, 10 due to poor bowel preparation, 6 patients had a full colonoscopy after an initial non-diagnostic flexible sigmoidoscopy and 3 were repeated to allow therapeutic intervention.
Endoscopic haemostasis was used in just 54/2528 (2.1%) of the total cohort and 54/642 (8.4%) of the cases undergoing endoscopy: 36/54 at flexible sigmoidoscopy, 14 at colonoscopy, 3 at proctoscopy and one unknown. The most frequent methods were banding (n=13), argon laser (n=11) and clipping (n=9). Two modalities were used in 12/54 cases and three in 3/54. Rebleeding following endotherapy occurred in 7/54 (13.0%) patients; one required embolisation, one underwent angiography that did not demonstrate contrast extravasation and two required further endoscopic haemostasis. No cases of rebleeding required surgery. Two perforations were reported at endoscopy, both requiring surgical intervention. Both followed flexible sigmoidoscopy, one showing pseudomembranous colitis and one multiple colonic ulcers. Neither had attempted endoscopic haemostasis. Of the 77 patients were admitted with LGIB following endoscopy, 49/77 (66.6%) were indicated as postpolypectomy bleeds. Of these, only six underwent inpatient lower GI endoscopy, four receiving endotherapy. An additional four underwent CT angiography (CTA) and two were successfully embolised.
Radiology
CT of the abdomen/pelvis was undertaken in 507/2528 (20.1%) cases, but CTA was used in only 149 (5.9%) and formal angiography in 37 (1.5%) (table 2). CT of the abdomen/pelvis and CTA led to a diagnosis of the source of bleeding in 283/507 (55.8%) and 74/149 (49.7%) scans, respectively. The most frequent diagnoses found on CT of the abdomen/pelvis were colitis (170/507, 33.5%) and diverticular disease (123/507, 24.2%). Colorectal mass lesions were identified on 42/507 (8.9%) scans, whereas no source of bleeding was identified in 138/507 (27.2%). The median time to procedure was 2 days (1–3) and 1 day (0–2) for CT of the abdomen/pelvis and CTA, respectively.
Of the 37 patients that underwent mesenteric angiography, only 19 (51.3%) received embolisation. Rebleeding following embolisation was reported in 7/19 patients; one successfully re-embolisation and one requiring surgical control. Two patients developed embolisation-related ischaemia; one requiring surgical resection. Both survived to hospital discharge.
Surgery
Six (0.2%) patients underwent laparotomy for bleeding, one following embolisation. Three patients had preoperative CTA identifying an actively bleeding rectal cancer and two diverticular bleeds, one patient had a CT of the abdomen/pelvis that identified angiodysplasia and one had no preoperative investigations. None of the patients undergoing surgery were shocked on first presentation, but all had ongoing bleeding and subsequently became unstable. Surgery was conducted between 20:00 and 8:00 in three of six cases and all were performed or supervised by a consultant surgeon. Three of six patients who underwent laparotomy for bleeding died; all had significant comorbidities (table 3).
Patients requiring emergency laparotomy for LGIB
Clinically significant bleeding
Only 36/2528 (1.4%) patients met the criteria for clinically significant bleeding; 8/36 received CT of the abdomen/pelvis, 7/36 CTA and 7/36 flexible sigmoidoscopy. Fourteen patients received no inpatient investigation. Angiography was undertaken in two, one receiving embolisation. None underwent endoscopic haemostasis or laparotomy for bleeding.
Patients undergoing no inpatient investigations
Overall, 1213/2528, 48.0% cases had no investigations for LGIB during their admission. Of these, 210/1213 (17.3%) received RBC transfusion and 126/1213 (10.4%) were readmitted by 28 days; 59/126 (46.8%) due to further LGIB. Hospitals reported that 105/1213 (8.7%) patients did not warrant inpatient investigation as they had been investigated previously. Additionally, 93/1213 (7.7%) had an anorectal source that was identified on digital rectal examination. Outpatient investigation was planned in 518/1213 (42.7%) cases, the most frequent being flexible sigmoidoscopy or colonoscopy (490 requests). Sites reported that 347/490 (70.8%) lower GI endoscopes and 21/41 (51.2%) CT scans were scheduled to occur more than 2 weeks postdischarge. Reasons why the remaining 497/1213 (41.0%) cases were not scheduled for outpatient investigation included ‘trivial, self-limiting bleeding with no change in haemodynamic status’ and ‘unknown’. Ten patients refused investigation and 62 (5.1%) were considered to be for palliative care only. Outcomes of patients who were not investigated in comparison to that did receive inpatient investigation are presented in the online supplementary material.
Diagnoses
The most commonly reported diagnoses were diverticular disease (668/2528, 26.4%), benign anorectal disorders (422, 16.7%) and colitis (344, 13.6%, table 4). Haemorrhoids were reported as the source of bleeding in 305 (12.1%). Angiodysplasia accounted for only 1% of cases. Of the patients diagnosed with diverticular bleeding, 333/668 (49.9%) had no inpatient investigations and 49/668 (7.3%) were diagnosed using previous investigations. Similarly, 7/25 diagnoses of angiodysplasia were made without inpatient investigation, 3/25 having been investigated previously.
Discharge diagnoses by age
Most cases admitted under gastroenterology had a discharge diagnosis of IBD or other colitis (15/54, 27.8%), whereas most patients admitted under general surgery were diagnosed with diverticular bleeding (565/2105, 26.8%). In 576/2528 (22.8%) cases, patients were discharged with no formal diagnosis. In this ‘unknown’ group, 248/576 (43.1%) had investigations that were non-diagnostic and the remainder had no investigations.
Rebleeding
Continued bleeding during the first 24 hours of admission was reported in 279/2528 patients (11.0%, 135 cases missing data). Rebleeding occurred in 343/2528 patients (13.6%, missing data in 126); 283 (11.2%) patients had one episode of rebleeding, 43 (1.7%) had two (each preceded by 24 hours of clinical stability) and 17 had three or more. Rebleeding occurred a median of 3 days (IQR 2–5) after presentation. Rebleeding was more common in inpatients (26.5% vs 12.6%, p<0.0001), and patients taking aspirin (107/552, 19.4%, p<0.0001, 32 cases missing data), versus those taking no antiplatelet or anticoagulant agents (156/1365, 11.4%). There was no difference in rebleeding in patients taking warfarin (38/254, 15.0% p=0.11, 16 cases missing data). The relationship between Charlson Comorbidity Index and rebleeding is shown in figure 2. The area under the receiver operator characteristic curve was non-discriminative at 0.59.

{kind=link}
{kind=link}
The relationship between Charlson Comorbidity Index and death and rebleeding.
The highest rate of rebleeding was seen in angiodysplasia (9/25), but significant numbers of patients diagnosed with diverticular bleeding (98/668, 14.7%, 21 cases missing data), haemorrhoids (30/305, 9.8%, 16 cases missing data) or inflammatory, infective or undetermined colitis (33/344, 9.6%) also rebled during admission.
In-hospital mortality
In-hospital mortality was 85/2528 (3.4%), and was higher for inpatients compared with new admissions (33/185, 17.9% vs 51/2296, 2.2%, p<0.0001) and in patients who rebled (24/338, 7.0%, p<0.0001, missing data in five cases). In four (0.2%) patients, the cause of death was attributed to uncontrollable haemorrhage. In 27 cases, deaths were attributed to morbidity associated with LGIB (GI malignancy, intra-abdominal sepsis) but 26 deaths were attributed to other comorbidity (pneumonia, MI, stroke, frailty and other, table 5).
Outcomes and cause of death of patients admitted with or developing LGIB while an established inpatient
Figure 2 shows the relationship between Charlson Comorbidity Index and mortality. The area under the receiver operating characteristic curve was 0.75, reflecting reasonable ability of Charlson Comorbidity Index to discriminate between patients who survived to discharge and those who did not. In contrast, the C-statistic for Charlson Comorbidity Index and readmission was 0.57.
Length of stay and hospital transfer
The median length of stay (LOS) for new admissions was 3 days (IQR 1–6) and was longer for patients who developed LGIB as an inpatient (9 days, IQR 5–21, table 4); 136/2528 patients (5.4%, missing data in 344) were discharged to a nursing home or rehabilitation facility, which added on average an extra 2 days to total LOS. In total, 56/2528 (2.2%) patients required transfer to another hospital for treatment, only 6 cases for interventional radiology procedures (see online supplementary table S5).
Readmission
Readmission occurred in 260/2528 (10.3%) patients by 28 days. In 111 (4.4%) cases, this was attributed to further LGIB. Readmission with further bleeding was highest for patients diagnosed with haemorrhoidal or diverticular bleeding (18/305, 5.9%, missing data in 50, and 38/668, 5.5%, missing data in 155, respectively). The majority of patients readmitted with further LGIB had no inpatient investigations during their index admission (59/111, 53.2%).
Comparison with UGIB
Full comparison with patients in the 2007 audit of UGIB12 is included in online supplementary table S6, but briefly, patients presenting with LGIB were older, with more comorbid illness. Fewer patients with LGIB presented with shock. Rates of inpatient endoscopic investigation were much lower in comparison to UGIB (25.9% vs 74%), although the frequency of interventional radiology procedures was similar. Fewer patients required laparotomy for haemorrhage control in LGIB (0.4% vs 1.5%) and in-hospital mortality was also lower (10% vs 3.4%).
Discussion
This is the largest and most comprehensive study of LGIB conducted to date and has defined its causes, interventions, processes of care and outcomes. Patients were elderly with a large burden of comorbidity; over one-third had a Charlson Comorbidity Index ≥2. At presentation, 28% were taking aspirin, clopidogrel or a non-steroidal anti-inflammatory, with an additional 16% taking either warfarin or a DOAC. Overall, 16% had been previously admitted with LGIB, 14% cases rebled during admission and 4.4% were readmitted within 30 days due to further bleeding. Over half of the latter were not investigated during their index admission.
Haemodynamic instability was present in only 18% of cases, the majority with just an isolated tachycardia and normal blood pressure. Thus, it is surprising that RBCs were transfused to over one-quarter of patients, despite only 11% presenting with a Hb <8.0 g/L. This indicates a liberal approach to RBC transfusion in real-life practice, which is contrary to guideline recommendations for transfusion.21 Randomised data from UGIB and other critically ill populations indicate a causal relationship between transfusion above Hb >7.0–8.0 g/L and rebleeding and death.10 ,11 ,23 ,24 Thus, many transfusions in this study would be considered inappropriate and require critical review of institutional practice in line with patient blood management initiatives.25
This study showed that case fatality rates following LGIB are low and considerably lower than those reported from other population-based studies. In a study from 10 Spanish hospitals, Lanas et al1 reported mortality of 8.8%, although the ICD-10 coding for case ascertainment may have captured cases of UGIB. The reported in-hospital mortality in the present study is limited by the duration of hospital admission (3 days) so may not be directly comparable to studies with a longer follow-up. Although, another database study of LGIB reported a similar in-hospital mortality of 3.9%.3 The present study confirms that death due to uncontrolled bleeding is very rare, with a strong observed association between increasing comorbidity and mortality. The almost eightfold increase in unadjusted mortality seen in inpatient bleeds is also likely to reflect a greater burden of comorbidity, but may also reflect more severe bleeding, as previously noted for UGIB.12 ,26
Decisions regarding withholding antiplatelets in patients presenting with LGIB are difficult since continued antiplatelet use is associated with rebleeding,27 but withholding them may lead to increased cardiovascular morbidity.28 Guidelines recommend that patients receiving aspirin for secondary prevention of high-risk cardiovascular disease should not have this drug stopped.6 This audit demonstrates that this principle is not being adhered to in many patients with LGIB suggesting uncertainty as to optimal management. We believe this to be a key area for further research. DOACs can also be a challenging, as most have no specific antidote at this time.
It was surprising that just 29% cases underwent lower GI endoscopy (flexible sigmoidoscopy, colonoscopy and anoscopy), given guideline recommendations.6 However, studies examining the role of colonoscopy have not demonstrated that inpatient endoscopy improves clinical outcomes.29 Hospitals reported that only half of the patients not investigated as an inpatient were booked for outpatient investigation. More than 50% of outpatient endoscopes and CT scans were scheduled to take place more than 2 weeks postdischarge. This raises concerns regarding the potential for missed lesions and contradicts the National Institute for Health and Care Excellence recommendation that patients aged 50 years or over with unexplained rectal bleeding should be referred for specialist assessment within 2 weeks.30 Additionally, more than half of the 4.4% that were readmitted due to further bleeding had not been investigated during their index admission, possibly suggesting that early discharge without investigation was inappropriate. Indeed, the proportion of patients undergoing flexible sigmoidoscopy or colonoscopy was lower than that reports of 34.7%–46.3% in other observational studies of LGIB3 ,4 and questions how diagnoses such as diverticular bleeding or angiodysplasia were confidently made.
The most common discharge diagnosis was diverticular bleeding, and across all age groups benign anorectal conditions were the second most common cause. Angiodysplasia accounted for only 1%, which is less frequent than previously reported.31 The proportion of LGIB attributed to polyps and colon cancer is also lower,2 ,3 but this may be due to the use of hospital codes or endoscopy referrals to identify cases in previous studies.
Mesenteric embolisation and surgical intervention were used in just 0.8% and 0.2% cases, respectively. Embolisation is often reserved for severe bleeds to avoid surgery, or where endoscopic investigation fails.6 It is recommended that hospitals have 24/7 access to interventional radiology for this purpose either on-site or through a network;7 although just six cases required transfer to another institution to access this facility. The sources of bleeding requiring emergency laparotomy were varied, although the number was small. Ideally, laparotomy should be last resort and carried out only after attempts at colonoscopic or interventional radiological management. Only one patient who required laparotomy underwent attempted embolisation. Considering laparotomy was performed more than 24 hours after presentation in four of six cases, a rebleeding plan may have been useful to allow the organisation and planning of minimally invasive treatment should further bleeding occur. Consultant staff should be involved with the decision-making and surgery in this rare and highly comorbid group of patients, as evidenced by the 50% surgical mortality rate.
Rebleeding is frequently encountered after UGIB, is well defined32 and associated with poor prognosis.12 Comparatively less is known about its frequency and course after LGIB and there are no accepted definitions. Simply quantifying the numbers of patients who experience further symptoms of bleeding may lead to falsely high reporting, capturing trivial bleeds or delayed transit of luminal blood after the initial bleed has stopped. The definition used in this study was that described by Strate et al,18 and captures rebleeding by using associated change in haematocrit or need for further transfusion after a period of clinical stability. Accordingly, 13.6% patients rebled during admission and a further 4.4% were readmitted for further LGIB by 28 days. This is higher than previous reports of rebleeding of 8% during index admissions.18 Sites were instructed to check each patient's status at 28 days using their own electronic patient records, although it is possible that readmissions to other institutions may have been missed, thus this is likely a conservative estimate.
The 2015 NCEPOD report recommended that ‘named consultants, ideally gastroenterologists would be responsible for the emergency and ongoing care of all major GI bleeds’, although in the present study just 2.1% patients were admitted to gastroenterology. Implementing this guidance would require considerable resources and as major bleeding is yet to be defined for LGIB, may not be valid.
Limitations of this audit should be acknowledged. Sites were instructed to capture consecutive cases in order to represent an unselected case-mix of presentations, although it is inevitable that some cases will have been missed. However, we followed the same methodology of case ascertainment used in the previous British Society of Gastroenterology/NHS Blood and Transplant audit of UGIB12 that was shown to have captured over 85% of cases when compared with national hospital episode statistics data over the same time period.33 Estimates of the incidence of LGIB for comparison are scarce, but using European data reporting an incidence of 33/100 000,1 we estimate an annual UK incidence of 21 120 cases. Limiting this figure to the 82.2% hospitals that participated would equate to 17 360 cases per annum, or 2893 in 2 months, which is very close to the case ascertainment in this study. To explore whether data were skewed by a few large centres, the largest 5% hospitals (identified by the number of acute beds in 2015 as reported by NHS England)34 were removed and mortality recalculated. The overall mortality was unchanged (3.41%). An additional limitation is the lack of investigation in many patients, which may indicate that many of the diagnoses were presumptive, although the frequencies are consistent with other studies.2 ,3
In summary, this is the first nationwide audit of LGIB and one of the most detailed of its kind. Most patients had minor bleeding, only one-quarter of patients underwent inpatient lower GI endoscopy, which infrequently resulted in the use of endotherapy. Radiological or surgical intervention was rarely required to control bleeding. Further research into risk stratification is needed to allowance avoidance of admission or facilitation of early discharge of low-risk patients. Critical review of excessive transfusion practice as well as research informing the role of colonoscopy in the acute setting is needed.
Acknowledgments
Frances Seeney, Principle Statistician, NHS Blood and Transplant for assisting the statistical analysis and critically reviewing the paper.
References
Footnotes
Twitter Follow Kathryn Oakland @LGIBaudit
Collaborators UK Lower GI Bleeding Collaborative: full names listed in the online supplementary appendix.
Contributors KO designed and conducted the study, performed the analysis, interpreted the data and wrote the paper. RG, NM, MFM and RU designed the study, interpreted the data and critically revised the paper. RH performed the statistical analysis and critically revised the paper. VJ designed the study, interpreted the data and wrote the paper.
Funding This project was funded by the NHS Blood and Transplant and the Bowel Disease Research Foundation. KO is supported by a research fellowship from the Royal College of Surgeons of England.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data on the organisation of services for lower GI bleeding has been provided to all hospitals that participated and are available at www.hospital.blood.co.uk.