Article Text

Abstract
Evidence-based guidelines on the management of pancreatic cystic neoplasms (PCN) are lacking. This guideline is a joint initiative of the European Study Group on Cystic Tumours of the Pancreas, United European Gastroenterology, European Pancreatic Club, European-African Hepato-Pancreato-Biliary Association, European Digestive Surgery, and the European Society of Gastrointestinal Endoscopy. It replaces the 2013 European consensus statement guidelines on PCN. European and non-European experts performed systematic reviews and used GRADE methodology to answer relevant clinical questions on nine topics (biomarkers, radiology, endoscopy, intraductal papillary mucinous neoplasm (IPMN), mucinous cystic neoplasm (MCN), serous cystic neoplasm, rare cysts, (neo)adjuvant treatment, and pathology). Recommendations include conservative management, relative and absolute indications for surgery. A conservative approach is recommended for asymptomatic MCN and IPMN measuring <40 mm without an enhancing nodule. Relative indications for surgery in IPMN include a main pancreatic duct (MPD) diameter between 5 and 9.9 mm or a cyst diameter ≥40 mm. Absolute indications for surgery in IPMN, due to the high-risk of malignant transformation, include jaundice, an enhancing mural nodule >5 mm, and MPD diameter >10 mm. Lifelong follow-up of IPMN is recommended in patients who are fit for surgery. The European evidence-based guidelines on PCN aim to improve the diagnosis and management of PCN.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Pancreatic cystic neoplasms (PCN) are estimated to be present in 2–45% of the general population.1–4 PCN comprise a clinically challenging entity as their biological behaviour ranges from benign to malignant disease. Consequently, correct management of PCN may prevent progression to pancreatic cancer while minimising the need for lifelong screening and related costs.5 Unfortunately, it is often difficult to differentiate between the various types of PCN.6 In 2013, the European Study Group on Cystic Tumours of the Pancreas, in association with United European Gastroenterology (UEG) and the European Pancreatic Club (EPC), published a European expert consensus statement on PCN.7
In 2016, as a group, these stakeholders felt that sufficient data were available to mandate an update of these guidelines. In contrast to the previous European,7 and international8 guidelines, an evidence-based approach was chosen. Similar to the previous European,7 but in contrast to other (inter-)national guidelines,8 9 the present guideline deals with all common PCN. The European evidence-based guidelines on PCN aim to improve the diagnosis and management of all PCN, and identify areas that require further research.
Methods
This guideline is a joint initiative of the European Study Group on Cystic Tumours of the Pancreas, the UEG, the EPC, the European-African Hepato-Pancreato-Biliary Association (E-AHPBA), European Digestive Surgery (EDS) and the European Society of Gastrointestinal Endoscopy (ESGE) and involves both European and non-European experts (online supplementary appendix 1).
Supplementary file 1
A methodology committee (gastroenterologists, surgeons, radiologists, oncologists, endoscopists, basic scientists) identified the nine most important topics: biomarkers, radiology, endoscopy, intraductal papillary mucinous neoplasm (IPMN), mucinous cystic neoplasm (MCN), serous cystic neoplasm (SCN), rare cysts and (neo)adjuvant treatment and pathology. Next, multidisciplinary expert groups were formed and each assigned to one topic. In March 2016, each expert group received a list of questions about their topic. The groups could suggest changes and add relevant questions based on their expertise and available literature. Once all questions were finalised, the following steps were taken: (a) a systematic literature search was performed in the PubMed, Embase and Cochrane databases, and the systematic review included randomised or observational cohort studies with a minimum of 20 patients or systematic reviews on PCN, which were published in English, and available in full text; (b) based on the literature review, recommendations were formulated including a GRADE rating for the quality of the evidence and the strength of the recommendation10–12; (c) relevant remarks concerning the recommendations—for instance, about subgroups or availability of diagnostic/therapeutic strategies, were included; (d) a table of relevant studies was provided. The results of these evidence-based recommendations were presented and discussed at a plenary meeting of the European Study Group on Cystic Tumours of the Pancreas in October 2016 during the UEG week.
In January 2017, each expert group submitted the modified version of their task to the methodology committee. A synthesis of the work from different groups was completed in April 2017 (MDC and MGB) and this document was circulated and approved by all the group leaders. Finally, in October 2017, the final recommendations were discussed at a plenary meeting of the European Study Group on Cystic Tumours of the Pancreas during the UEG week. Thereafter, in November 2017, all members of the expert groups were surveyed and asked about their agreement with the final recommendations on a five-point scale (ie, definitely agree, moderately agree, neutral, moderately disagree, definitely disagree) via an anonymous web-based vote. Recommendations with at least 75% consensus (combining ‘definitely’ and ‘moderately’ agree) were accepted as ‘strong agreement’; otherwise ‘weak agreement’ was listed. The results of this survey were added to the evidence-based recommendation in order to provide readers with more insight into the level of agreement among experts. In December 2017, the members of the methodology committee and the group leaders approved the final draft.
Each statement includes the grade of evidence, strength of the recommendation, voting result and, where appropriate, remarks.
Definitions
PCN are defined and classified according to the WHO criteria13 (table 1). Disease-free survival was defined as the length of time the patient lives after primary treatment without any signs or symptoms of recurrence.
Classification of cystic lesions of the pancreas
Recommendations
This guideline aims to provide evidence-based guidelines for the diagnosis and treatment of PCN.
1 Biomarkers
1.1 What is the role of blood and cystic biomarkers in the diagnosis and follow-up of PCN in current clinical practice?
Blood
There are no available DNA, RNA or protein biomarkers in blood for clinical use to differentiate pancreatic cyst type or identify high-grade dysplasia or cancer. Serum cancer antigen (CA) 19.9 may be considered in IPMN where there is concern for malignant transformation 14–16 (GRADE 2C, strong agreement).
Cyst fluid
DNA markers, in particular, mutations in GNAS and KRAS, have shown promise in identifying mucin-producing cysts. In cases in which the diagnosis is unclear, and a change in diagnosis will alter management, analysis of these mutations using highly sensitive techniques, such as next-generation sequencing (NGS), may be considered 17–20 (GRADE 2C, strong agreement).
Currently, there is insufficient evidence to support the use of RNA or non-carcinoembryonic antigen (CEA) protein markers in pancreatic cysts (GRADE 1B, strong agreement).
The role of CEA in cyst fluid is discussed in recommendation 3.4.
Additional biomarkers in the differential diagnosis of PCN are amylase/lipase levels. Amylase may exclude pancreatic pseudocysts (amylase <250 U/L; sensitivity 0.44, specificity 0.98), but does not differentiate between other non-mucinous and mucinous cysts.21 22
2 Radiology
2.1 What is the accuracy of MRI/cholangiopancreatography (MRI/MRCP) and CT for identifying the specific type of PCN?
The reported accuracy for identifying the specific type of PCN is between 40% and 95% for MRI/MRCP and between 40% and 81% for CT. 23–27
PCN are increasingly being detected, with a reported prevalence of 2.1–2.6% for CT28 29 and of 13.5–45% for MRI/MRCP,2 30 31 with the difference between CT and MRI most probably due to the higher contrast resolution of MRI compared with CT and thus increased sensitivity but not specificity. However, the accuracy remains relatively low, using either single, or combining imaging modalities, for identifying the specific type of PCN,6 for differentiating small PCN from non-neoplastic or non-epithelial cysts, or for connection to the ductal system.6 ,32
2.2 Which radiological (cross-sectional) imaging method is preferred for the surveillance of patients with PCN taking into consideration accuracy, cost, and modality-related risk factors?
Pancreatic MRI is the preferred method for follow-up of PCN (GRADE 2C, strong agreement).
Dedicated pancreatic protocol CT and pancreatic MRI/MRCP are reported to have a similar accuracy for the characterisation of PCN.33–35 MRI/MRCP is more sensitive than CT for identifying communication between a PCN and the pancreatic duct system, and the presence of a mural nodule or internal septations. In addition, MRI/MRCP is very sensitive for identifying whether a patient has single or multiple PCN, with the latter favouring a diagnosis of multifocal side-branch IPMN.25 33 36 37 Patients with PCN may require lifelong imaging follow-up. This is important, as studies have shown that repeated exposure to ionising radiation following CT increases the risk of malignancy.38 39
2.3 Are there specific clinical scenarios where use of one cross-sectional imaging modality (CT/MRI) instead of another, or combined use is preferable?
In general, MRI is the preferred method for the investigation of patients with PCN. Multimodality imaging should be considered in cases where the identification of calcification is important, for tumour staging, or for diagnosing postoperative recurrent disease (GRADE 2C, strong agreement).
The use of CT should be considered in the following clinical situations:
For the detection of parenchymal, mural or central calcification, and especially when differentiating pseudocysts associated with chronic pancreatitis from PCN.40 41
When there is suspicion of a malignant PCN or concomitant pancreatic cancer, and when assessment of vascular involvement, peritoneal, or metastatic disease is required.
When there is suspicion of postoperative recurrence of pancreatic cancer.
2.4 What are the minimum technical requirements for MRI or CT for the diagnosis and surveillance of patients with PCN?
No definite MRI or CT protocol can be recommended for the diagnosis or surveillance of patients with PCN because of the wide spread of published data and the lack of dedicated comparative studies (GRADE 2C, strong agreement).
In 2016, a short protocol for the surveillance of PCN that included T2-weighted ultrafast spin echo technique (T2-HASTE) and T1-weighted pre-contrast imaging was found in one retrospective study to provide equivalent information to a longer protocol which included diffusion-weighted imaging (DWI) and contrast enhanced T1-weighted sequences.42 DWI may be added to this short protocol in order to minimise the risk of missing a concomitant pancreatic cancer. A combination of T2-HASTE and DWI has been shown to have similar accuracy to a comprehensive contrast-enhanced MRI protocol for the detection of pancreatic cancer.43 A recent study suggested that MRI with MRCP has a better diagnostic performance than endoscopic ultrasound (EUS) for differentiating malignant from benign pancreatic IPMN and MCN,44 but conclusive evidence is lacking.
3 Endoscopy
3.1 What are the indications for performing EUS in PCN?
EUS is recommended as an adjunct to other imaging modalities (GRADE 2C, strong agreement).
EUS is helpful for identifying PCN with features that should be considered for surgical resection. Similar to MRI andCT (see 3.1 statement), EUS is imperfect at identifying the exact type of PCN (GRADE 2C, strong agreement).
EUS is recommended if the PCN has either clinical or radiological features of concern identified during the initial investigation or follow-up (GRADE 2C strong agreement).
Data for EUS-based differentiation between benign and malignant PCN are conflicting.45–48 In addition, there is considerable interobserver variation in EUS-based diagnoses.49 50
3.2 When should contrast harmonic enhanced EUS (CH-EUS) be performed for PCN and does it alter management?
CH-EUS should be considered for further evaluation of mural nodules. CH-EUS is also helpful in assessing vascularity within the cyst and septations (GRADE 2C, strong agreement).
The presence of hyperenhancement of a mural nodule, solid mass, or septations on CH-EUS raises concern for malignant transformation, and EUS-fine needle aspiration (FNA) of the lesion should be considered (GRADE 2C, strong agreement).
CH-EUS seems superior to standard EUS and CT for the identification of mural nodules.51 52 Interobserver agreement is excellent for Sonazoid, and moderate for Sonovue.51 53
3.3 What are the indications and contraindications for EUS-FNA for PCN?
EUS-FNA improves diagnostic accuracy in PCN for differentiating mucinous versus non-mucinous PCN, and malignant versus benign PCN, in cases where CT or MRI are unclear (GRADE 2C, strong agreement).
A combined analysis of cyst fluid CEA, cyst fluid lipase levels, and cytology provides the highest accuracy for differentiating mucinous from non-mucinous PCN (GRADE 2C, strong agreement).
EUS-FNA should only be performed when the results are expected to change clinical management (GRADE 2C, strong agreement).
EUS-FNA should not be performed if the diagnosis is already established by cross-sectional imaging, or where there is a clear indication for surgery (GRADE 2C, strong agreement).
Relative contraindications for EUS-FNA in PCN is a distance of >10 mm between the cyst and the transducer, the presence of a high-risk of bleeding due to bleeding disorder, or the use of dual antiplatelet drugs (GRADE 2C, strong agreement).
The role of EUS-FNA in the diagnosis of PCN is still a matter of debate and consensus in the literature is lacking.54 55
3.4 When EUS-FNA is performed, which tests should be performed and what is their yield?
Evaluation of cyst fluid CEA, combined with cytology, or KRAS/GNAS mutation analyses (although the latter is not yet standard management), may be considered for differentiating an IPMN or MCN from other PCN (GRADE 2C, strong agreement).
To differentiate benign PCN from those harbouring high-grade dysplasia or cancer, EUS-FNA may be considered, and any solid component or thickened cyst wall targeted for cytology (GRADE 2C, strong agreement).
Brush cytology, and forceps biopsy are not recommended owing to a lack of high-quality evidence. Further studies are required before these tests can be considered in clinical practice (GRADE 1C, strong agreement).
In a recent meta-analysis cytological analysis of cyst fluid had 42% sensitivity and 99% specificity for differentiating mucinous from non-mucinous PCN.56 A cyst fluid CEA level of ≥192 ng/mL can distinguish mucinous, from non-mucinous cysts, with a sensitivity of 52–78% and specificity of 63–91%.57–64 Differentiating between MCN and IPMN based on CEA and/or cytology is not possible and CEA seems inaccurate to differentiate between benign mucinous cysts and cysts with high-grade dysplasia or an associated invasive carcinoma.65
3.5 What is the diagnostic performance of EUS +/−FNA?
EUS morphology alone has a modest diagnostic yield (GRADE 2C, strong agreement).
EUS-FNA is recommended to achieve a better performance for diagnosing PCN (GRADE 1C, strong agreement).
The reported accuracy of EUS morphology alone for differentiating mucinous from non-mucinous PCN is relatively low (48–94%),54 58 59 66 67 with a sensitivity of 36–91%, and a specificity of 45–81%.54 58 59 66 Although cytology is highly specific (83–100%),54 58 59 66 68 it is relatively insensitive (27–48%),54 58 59 66 68 resulting in low diagnostic accuracy (8–59%).58 59 66
Combination tests, such as EUS morphology, cytology and cyst fluid CEA, provide greater accuracy in detecting mucinous PCN than either EUS morphology or cytology alone.58 59
3.6 What are the potential adverse events associated with EUS-FNA of PCN? Are there any measures that can be taken to prevent complications?
EUS-FNA for PCN is a safe procedure with a relatively low risk (3.4%) of complications (GRADE 2B, strong agreement).
No specific measures are suggested to minimise the risk of complications in EUS-FNA (GRADE 2C, strong agreement).
Following EUS-FNA, 44/1313 (3.4%) patients developed an adverse event.69–75 These complications were mild in 34, moderate in nine, and severe in one patient(s). One retrospective study of 253 patients found that antibiotic prophylaxis had no effect on the risk of infection (7% vs 9.3%), although conclusive evidence is lacking.76 Current practice is often a single shot antibiotic treatment after EUS-FNA of a cystic lesion.
3.7 Is there any role for endoscopic retrograde cholangiopancreatography (ERCP) and/or pancreatoscopy and/or confocal laser endomicroscopy (nCLE) in the diagnosis of PCN?
ERCP should not be used as a diagnostic modality for differentiating PCN (GRADE 1C, strong agreement).
Pancreatoscopy may be used in selected cases to provide information on the location and extent of main duct (MD)-IPMN and can be useful in differentiating chronic pancreatitis from MD-IPMN (GRADE 2C, weak agreement).
nCLE should not be used for the differential diagnosis of PCN (GRADE 1C, weak agreement).
ERCP has a higher risk of adverse events, and a lower sensitivity and specificity for identifying the type of PCN than conventional radiology and EUS, and should not be used for this indication.77 78
The accuracy rate of pancreatoscopy is higher in MD-IPMN (88%) than in branch duct (BD)-IPMN (67%).79 Intraoperative main pancreatic duct (MPD) pancreatoscopy combined with frozen section of intraductal biopsies may be helpful in establishing the extent of IPMN involvement of the MPD, and assist surgical decision-making about the extent of resection required.80 Although promising, further studies are required and it should not be used in routine clinical care. A major concern about nCLE is the rate of adverse events (7–9%).81 82 Some suggest that nCLE could be useful in correctly diagnosing serous cystadenomas, and thereby might prevent unnecessary surgery in these patients.83 84
4 IPMN
4.1 What is the risk of malignant progression of an IPMN lesion and what risk factors are predictive of cancer progression?
Jaundice, the presence of an enhancing mural nodule (≥5 mm) or a solid component, positive cytology, or a MPD measuring ≥10 mm are highly predictive of malignancy and should be evaluated in all patients fit for surgery (GRADE 1B, strong agreement).
MPD dilatation between 5 and 9.9 mm, cystic growth-rate ≥5 mm/year, Increased level of serum CA 19.9 (>37 U/mL), symptoms, enhancing mural nodules (<5 mm), and/or a cyst diameter ≥40 mm are also associated with an increased risk for high-grade dysplasia or cancer (GRADE 1B, strong agreement).
Nine studies, including 1510 surgically resected IPMN, have concluded that the presence of jaundice, a contrast-enhancing mural nodule or solid component, or MPD dilatation of ≥10 mm, has a positive predictive value for malignancy of 56–89%.85–92 Several series including surgically resected IPMN have reported a high risk of harbouring at least high-grade dysplasia or cancer of 37–91% even for a MPD size of 5–9.9 mm.93–95 Several studies have recently identified serum CA 19.9 as an independent predictor of malignancy in IPMN.14–16 Analyses of surgical series of patients with BD-IPMNs who have undergone surgical resection, have found that a mural nodule measuring ≥5 mm on EUS has a sensitivity of 73–85% and specificity of 71–100% for the presence of high-grade dysplasia or cancer.96–99 The presence of a cyst size ≥30 mm, without any other radiological or clinical risk factors, has a positive predictive value for malignancy of between 27% and 33%.85–92 Patients with an IPMN measuring ≥30 mm have a 5% risk of developing malignancy, from which they will die within 3 years, whereas the 5 years disease-free survival after resection of IPMN is 96%.100 Even for BD-IPMN <30 mm, the 5-year risk for developing malignancy is reported to be 45% if a cyst increases in size by >2 mm/year.101 One study, with imaging surveillance for 36 months, detected a 20-fold higher risk of malignant progression in IPMN whose size increased >5 mm/year or had a total growth of 10 mm.102 In predominantly surgical series the presence of new-onset diabetes, pancreatitis, and abdominal pain have been associated with malignancy at varying rates, indicating that the level of evidence for these risk factors is low.14 85–91 Table 2 shows the risk of high-grade dysplasia or malignancy according to the dilatation of the main pancreatic duct in IPMN.
Risk of high-grade dysplasia or malignancy according to dilatation of the main pancreatic duct in IPMN
Follow-up of BD-IPMN is required as progression of disease is expected in about 10–15% of patients during 3–5 years of follow-up. Surveillance should also include the entire pancreatic gland because of an increased risk of new-onset cancer.103 104 In patients with MD-IPMN and those with mixed-type (MT)-IPMN several factors may predict progression during surveillance (eg, diffuse MPD dilatation, serum CA 19-9, serum alkaline phosphatase, and absence of extrapancreatic cysts).105 106
4.2 What are the clinical implications of the presence of potential risk factors, including morphological features, with regard to determining follow-up investigations, and the decision to proceed with surgical resection
For patients with an IPMN without an indication for operative intervention, routine follow-up is recommended. A 6-month follow-up in the first year, and yearly follow-up thereafter is adequate when no risk factors are present that establish an indication for surgery. Changes in clinical symptoms should trigger investigations (GRADE 1B, strong agreement).
For patients with relative indication for surgery (see statement 4.12), the ‘elderly’, and those affected by severe comorbidity, a 6-month follow-up is recommended. (GRADE 1B, strong agreement).
In young individuals, the risk of malignancy and surgery has to be balanced against the burden of lifelong follow-up.107 However, after partial pancreatectomy for IPMN lifelong follow-up is still indicated. Resection therefore does not eliminate the need for regular follow-up screening.
4.3 Is there a certain size cut-off point for resecting an IPMN regardless of the absence of clinical symptoms or (other) risk factors? Is age of the patient a co-factor that should be analysed to define better management strategy?
Patients with IPMNs >40 mm have an increased risk of harbouring malignancy (GRADE 1B, strong agreement).
Several studies including both surgically resected or observed IPMN have reported an increased risk of malignancy ranging from 12% to 47% in cases of a cyst ≥30 mm.85 96 108–110 In some of these series, the risk of malignancy produced by cyst size was stratified by the presence of other features for malignancy, indicating that cyst size alone is not an appropriate indication for surgery since the risk of malignancy is actual but low.92 111 If multiple risk factors are present the sensitivity to detect malignancy increases.89 112
4.4 What is the best imaging modality for the follow-up of IPMN?
MRI is the preferred imaging modality for the follow-up of IPMN. EUS can be used in selected cases (GRADE 1B, strong agreement).
See section 3 for details.
4.5 Should the progress of IPMN be followed for as long as the patient is fit for surgery?
The risk of IPMN progression increases over the time, therefore patients affected by IPMN without indication for surgery should be followed up until they are no longer fit for surgery (GRADE 1B, strong agreement).
The risk of progression of IPMN increases over the time as does the risk of developing indications for surgical resection. Interruption of surveillance is not recommended if the patient is fit for a potential surgical resection.107 113 114 A single study on IPMN concluded that patients with a Charlson-age comorbidity index ≥7 have an 11-fold risk of comorbidity-related death within 3 years and only 6% of patients will die of malignant IPMN.115
4.6 Should patients with IPMNs be screened for other tumours (including pancreatic cancer)?
The incidence of new extra-pancreatic neoplasms during the follow-up evaluation of pancreatic IPMN is not significantly greater than in the general population. Comprehensive screening outside the national protocols might not be necessary. Patients with IPMN are at risk of developing pancreatic cancer and attention should be paid to its concomitant development even when an IPMN has been successfully resected (GRADE 1C, strong agreement).
A systematic review concluded that the available data remain inconclusive.116 Two large studies including both surgically resected or followed IPMN did not find any difference in terms of incidence of extra-pancreatic neoplasms in patients with IPMN if compared with the general population.117 118
4.7 Should MD-IPMN always be resected?
Patients with MD-IPMN who are fit for surgery should undergo resection (GRADE 1B, strong agreement).
Surgery for MD-IPMN is universally accepted considering the high-rate of malignancy due to MD-IPMN,93 119 even though no randomised trials comparing surgery with observation are available. As discussed in statement 4.1 above, a MD-IPMN measuring between 5 and 9.9 mm is a relative indication for surgical resection, while MD-IPMN measuring ≥10 mm (see statement 4.1 for details) is an absolute indication for surgical resection.
4.8 Should mixed-type (MT)-IPMN be managed in a similar manner to MD-IPMN?
MT-IPMN carries a risk of malignant transformation that is comparable to MD-IPMN, and resection is therefore advised in patients who are fit for surgery (GRADE 2C, strong agreement).
Few studies have investigated MT-IPMN as a single entity. Malignancy rates appear similar for MT-IPMN and MD-IPMN.120 Recently, a pathological classification distinguishing minimal (microscopic) and extensive (macroscopic) involvement of the MPD showed a significant difference in the risk of high-grade dysplasia or cancer (17% and 70% respectively).121 However, this classification can be used only after resection, and is thus irrelevant for clinical assessment before surgery.
4.9 What type of resection is indicated when the entire MPD is dilated on imaging?
Pancreatoduodenectomy with frozen section analysis of the resection margins is recommended for patients with MPD dilatation comprising the entire length of the pancreas (GRADE 2C, strong agreement).
In cases in which there is a mural nodule within the MPD further along the duct, or in patients with an increased risk for malignancy (ie, patients with familial pancreatic cancer), a total pancreatectomy can be considered (GRADE 2C, strong agreement).
It is important to assess the MPD for a mural nodule before surgical exploration (see sections 2 and 3 for details). There are conflicting data and opinions about the extent of surgery for MD-IPMN.122 Some authors advocate total pancreatectomy in every patient affected by MD-IPMN with radiological involvement of the entire MPD because of the relatively high-risk of high-grade dysplasia and cancer.123 124 Others suggest total pancreatectomy only when there is a positive family history of pancreatic cancer,125 or partial pancreatectomy followed by close surveillance, with completion pancreatectomy where progression or recurrence is suspected.126 In this situation, pancreatoscopy may be useful to determine the extent of MPD involvement (see statement 3.7 for details). Where there is either a radiological suspicion, or histological proof of an IPMN-associated invasive carcinoma in the head of the pancreas, total pancreatectomy is not recommended, as the cancer will determine the prognosis.
4.10 At what MPD diameter should surgery be considered?
Recent studies demonstrate malignancy rates of 30–90% even in cases with a MPD dilatation of >5 mm. 93–95 127–131 Consequently, the threshold of MPD dilatation for surgical resection is >5 mm in both MD-IPMN and MT-IPMN (GRADE 2C, weak agreement).
The main goal of surgery is to resect IPMNs when high-grade dysplasia is present, and before patients develop pancreatic cancer. Given the recent studies, and the goal of surgery, a cut-off point of >5 mm is reasonable (see figure 1).
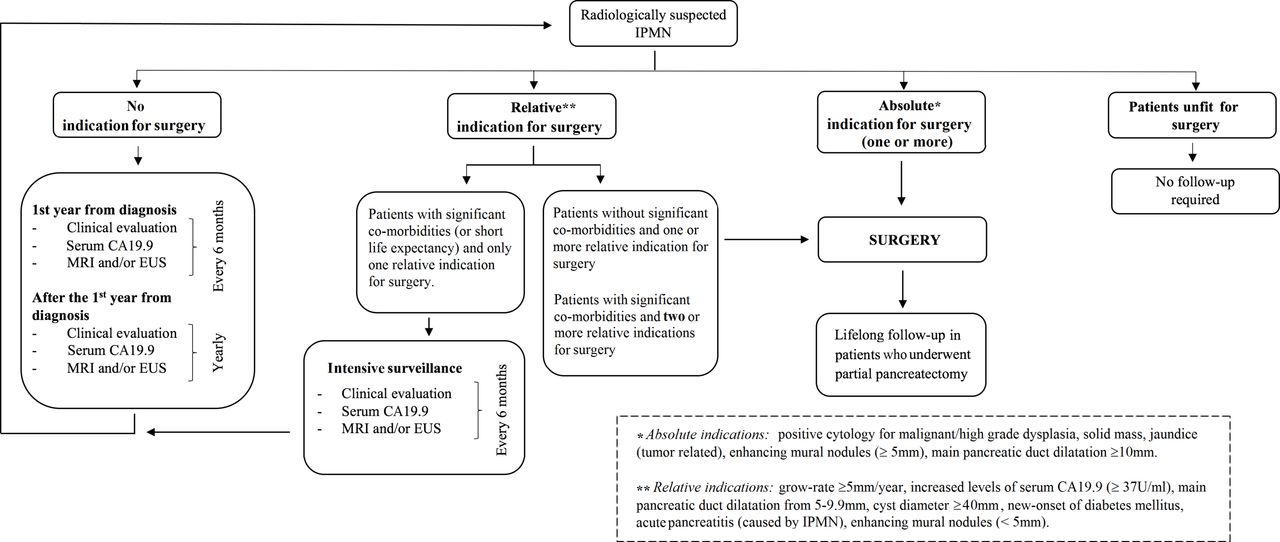
{kind=link}
Indications for surgery. EUS, endoscopic ultrasound; IPMN, intraductal papillary mucinous neoplasm.
4.11 What are the absolute criteria for resection of BD-IPMN?
The presence of jaundice, cytology positive for high-grade dysplasia or cancer, the presence of a contrast-enhancing mural nodule (≥5 mm) or solid mass should be considered as absolute indications for surgery (GRADE 1B, strong agreement).
See statements 4.1–4.2, for a detailed description of the rationale for this.
4.12 Which are the relative criteria for resection of BD-IPMN?
Growth rate ≥5 mm/year, increased serum CA 19.9 level (>37 U/mL in the absence of jaundice), MPD diameter between 5 and 9.9 mm, cyst diameter ≥40 mm, symptoms (new-onset of diabetes mellitus or acute pancreatitis), and contrast- enhancing mural nodules <5 mm can be considered relative indications for surgical resection (GRADE 2C, strong agreement).
Table 3 shows absolute and relative indications for surgery.
Absolute and relative indications for surgery in IPMN
CA 19.9 values in the serum >37 U/mL have been associated with a positive predictive value of 74.0% and accuracy of 81.7% to identify patients with invasive IPMN. Highly elevated levels of CA 19.9 may thus be helpful as an additional but not sole indicator for invasive IPMN.132
A recent large cohort of patients, who underwent surveillance for IPMN in accordance with the previous European expert statement, validates the safety of observation of BD-IPMN measuring <40 mm in the absence of other risk factors.107 However, other data show that even small IPMN may develop into high-grade dysplasia or cancer. This highlights the importance of evaluating for the presence of multiple risk factors.88 133–135 The greater the number of risk factors, the higher the probability of malignancy.136 137 Table 4 shows the risk of high-grade dysplasia or malignancy according to cyst size in BD-IPMN.
Risk of high-grade dysplasia or malignancy according to cyst size in branch duct IPMN
4.13 Which kind of surgery should be performed for patients with BD-IPMN?
The surgical approach for most BD-IPMN is an oncological resection with standard lymphadenectomy. Parenchyma-sparing pancreatectomy (PSP) is a non-oncological procedure, which is suitable only for lesions with a very low probability of malignancy—for example in patients without risk factors who have a strong wish to be operated on (GRADE 2C, strong agreement).
Considering that surgery is indicated only for lesions with a potential risk of cancer or high-grade dysplasia, the indications for PSP are very limited. Diagnostic use of these procedures is reported occasionally in patients at increased risk of malignancy (ie, familial pancreatic cancer).138 Since the morbidity of PSP is the same as that of conventional pancreatectomies, the advantage of performing PSP over conventional pancreatectomy is unclear.139 140
4.14 When is full lymph node dissection required?
An oncologic resection including standard lymphadenectomy is the preferred procedure for IPMN with an absolute indication for resection 141 142 (GRADE 1C, strong agreement).
4.15 How should multifocal BD-IPMN be evaluated for surgery? Is it safe to leave in place BD-IPMN without clinical or radiological signs of high-grade dysplasia or cancer when resecting another part of the pancreas?
In multifocal BD-IPMN, each cyst should be evaluated individually for the presence of features associated with malignancy. Cysts without concerning features can undergo surveillance 143–148 (GRADE 2C, strong agreement).
In cases of multifocal IPMN each lesion should be evaluated for surgical resection as a single entity according to the criteria reported in statements 4.10–4.11. Once this appraisal is performed, a tailored surgical approach can be planned. An intraoperative analysis of the surgical margins may help to determine the need for expanded resection.145 149
4.16 Should frozen section analysis be performed routinely in IPMN undergoing surgical resection?
Frozen section analysis of the pancreatic resection margin should be performed for all partial pancreatectomies and PSP in patients with IPMN (GRADE 1C, strong agreement).
Although frozen section analysis is recommended, data on its clinical impact on the resection margin of an IPMN undergoing surgical resection are contradictory.126 149–164
4.17 How will the frozen section result alter the surgical procedure?
If high-grade dysplasia or cancer is present at the surgical margin, further resection is warranted, up to a total pancreatectomy. In contrast, the presence of lower grades of dysplasia may not require any further resection (GRADE 2C, strong agreement).
Extending the resection may be considered in young fit patients, especially those at an increased risk for cancer (ie, familial pancreatic cancer), with low-grade dysplasia at the resection margin. Frozen section analysis is useful for detecting microscopic spread of cancerous lesions but is unable to detect the presence of discontinuous (skip) lesions, which occur in 6−42% of cases.165–167 Moreover, detailed observation of the remnant MPD using intraoperative pancreatoscopy may provide identification of preoperatively undetected lesions.80 168 169 Patients should always be counselled about the potential need for a total pancreatectomy.
4.18 What is the value of the frozen section in resected IPMN with cancer?
Frozen section examination of the pancreas resection margin should be performed in patients with an IPMN and cancer. In cases with a resection margin, which on frozen section is positive for pancreatic cancer, it is strongly recommended that the resection is extended. In cases of high-grade dysplasia at the resection margin, extension of the resection should be considered. No extension of the resection margin is indicated for low-grade dysplasia (GRADE 2C, strong agreement).
Data vary on the value of a positive frozen section to predict IPMN cancer recurrence after surgery.126 149 150 154–157 159 161 170 171 An IPMN associated with invasive carcinoma, with no lymph node metastases, appears to be associated with a better long-term outcome than pancreatic cancer.172 For this reason, extension of the resection margin in cases of cancer or high-grade dysplasia appears reasonable in these patients.
4.19 How are surgical outcomes affected by cyst location, comorbidity, patient age, and how should these features be weighted?
The surgical strategy should be individualised for each patient, based on the type of surgical resection, the patients’ age, comorbidities, and the patient’s preference (GRADE 2C, strong agreement).
A more conservative approach may be considered for IPMN located in the head of the pancreas in elderly patients or patients with multiple comorbidities.100 107 173 However, this conservative approach should be weighted with the potential risk of progression107 or development of high-grade dysplasia or cancer.174
4.20 How should patients be followed up who underwent surgical resection for an IPMN?
Lifelong surveillance is recommended following resection of an IPMN as long as the patient is fit and is willing to undergo surgery if indicated. Patients with evidence of anIPMN-associated invasive carcinoma should be followed up in the same manner as those with a resected pancreatic cancer. IPMN with high-grade dysplasia or MD-IPMN should have close follow-up every 6 months for the first 2 years, followed by yearly surveillance. IPMN with low-grade dysplasia should be followed up in the same manner as non-resected IPMN (see statement 4.2 and figure 1 for details). Patients with IPMN in the remnant pancreas, who do not have high-grade dysplasia or MD-IPMN, should be followed up in the same manner as non-resected BD-IPMN (see section 4.15 and figure 1 for details). Follow-up imaging using MRI or EUS is recommended (GRADE 2C, strong agreement).
Several studies have reported that IPMN recurrence is possible 5 to 10 years after resection.175 176 The risk of BD-IPMN and MD-IPMN recurrence is similar (7–8%).161 Resected IPMN with low-grade dysplasia have a low risk of recurrence (5.4−10%) with disease-free survival of approximately 52 months, while IPMN with high-grade dysplasia or an IPMN-associated invasive carcinoma have a higher risk (>50%), with disease-free survival of 29 months.85 161
4.21 What preoperative investigation should be performed for a patient with an IPMN-associated invasive carcinoma? Should the same criteria be used as for pancreatic cancer?
The diagnostic investigation for an IPMN-associated invasive cancer should follow the same algorithm used for pancreatic cancer 177 (GRADE 1C, strong agreement).
No studies have examined the differences between an IPMN-associated invasive carcinoma and spontaneous pancreatic cancer with respect to local tumour extension or staging for distant metastases.
4.22 Should patients with an IPMN and a family history of pancreatic cancer be managed in a similar manner to patients with an IPMN but no family history?
We recommend that the management of asymptomatic patients with an IPMN and a positive family history of pancreatic cancer is the same as that of patients with a sporadic IPMN (GRADE 2C, weak agreement).
There is no reported evidence that IPMN occurring in patients with a family history of pancreatic cancer have more rapid progression to high-grade dysplasia or cancer than sporadic cases.178–181
4.23 Should patients who have undergone an organ transplant, and have an IPMN be managed in the same way as non-transplanted patients with IPMN?
We recommend that surveillance of patients who have undergone an organ transplant and have an IPMN should be the same as for non-transplanted patients 182–186 (GRADE 1B, strong agreement).
4.24 Should patients who have an IPMN which fulfils criteria for surgical resection but who are not surgical candidates be treated with ablative techniques?
Further studies are required to clarify the indications for, and safety of, EUS-guided ablative injection techniques (ethanol, paclitaxel), radiofrequency ablation, or cryoablation for treatment of IPMNs. These should not be performed outside of clinical trials approved by the institutional review board (GRADE 1C, strong agreement).
EUS ablative procedures for the treatment of IPMN are not standardised and their efficacy is unclear. Furthermore, there is a lack of reliable markers to indicate successful and complete ablation.187–191
5 Mucinous cystic neoplasm
5.1 Should patients with MCN always undergo surgical resection?
MCN ≥40 mm should undergo surgical resection. Resection is also recommended for MCN which are symptomatic or have risk factors (ie, mural nodule) irrespective of their size 192 (GRADE 1B, strong agreement).
The rate at which the size of an MCN increases should be considered. Some case reports have suggested considerably faster growth of MCN during pregnancy, potentially leading to tumour rupture.193 Therefore, patients with MCN should be observed closely during pregnancy.
5.2 Is it safe to follow up presumed MCN, which measures <40 mm?
It is safe to follow up presumed MCN that measure <40 mm, in the absence of risk features such as a suspicious mural nodule or symptoms 192 (GRADE 2C, strong agreement).
For patients with MCN measuring between 30 and 40 mm, clinicians can incorporate other factors such as age, comorbidities, patient’s surgical risk, and patient preference. For cysts measuring <30 mm, it may be difficult to make a definitive diagnosis of an MCN, and smaller MCN may sometimes be difficult to distinguish other cystic lesions. We therefore recommend similar surveillance for MCN and IPMN measuring <3 cm.
5.3 How should MCN, which is not resected, be followed up?
MCN measuring <40 mm without a mural nodule or symptoms may undergo surveillance with MRI, EUS, or a combination of both. 7 194 Surveillance is recommended every 6 months for the first year, then annually if no changes are observed. Patients with an MCN measuring <40 mm and with no concerning features or symptoms should have lifelong surveillance as long as they are fit for surgery (GRADE 2C, strong agreement).
Earlier studies have evaluated features associated with malignant transformation for all mucinous lesions combined. However, IPMNs and MCN may have different rates of growth and malignant transformation and different features predictive of malignancy.195
5.4 Is cyst fluid analysis recommended for MCN?
See statement 3.3.
5.5 Which surgical procedure(s) should be performed for an MCN?
To avoid incomplete treatment of invasive carcinoma, a standard oncologic resection (distal pancreatectomy in 90–95% of MCN) with lymph node dissection and splenectomy is indicated for any MCN with imaging features indicating high-grade dysplasia or cancer (GRADE 1B, strong agreement).
MCN without suspect features with a low risk of malignancy can be treated with a non-oncological resection (distal pancreatectomy with splenic preservation with or without preservation of splenic vessels, or PSP) (GRADE 2C, strong agreement).
A PSP may be considered in selected patients to decrease the long-term risk of diabetes, provided the anatomical location is favourable (GRADE 2C, strong agreement).
PSP are associated with higher early morbidity and longer hospitalisation.139 140 196 A laparoscopic approach is feasible for MCN. Its benefit over an open approach is comparable to other indications.197
6 Serous cystic neoplasm
6.1 Does malignant SCN exist? is there a risk of malignant transformation?
SCN is a benign entity. There are essentially no deaths that are attributable to dissemination/malignant behaviour of an SCN. Specific mortality due to an SCN is nearly zero 198 199 (GRADE 2C, strong agreement).
Cases reported as ‘malignant’200–202 do not fulfil the WHO criteria for an SCN.
6.2 If there is a clear diagnosis of an SCN, can follow-up be discontinued?
Asymptomatic patients with radiological evidence of an SCN should be followed up for 1 year. After 1 year, symptom-based follow-up is recommended (GRADE 2C, strong agreement).
6.3 When does a possible SCN require follow-up?
Only when the diagnosis is uncertain is follow-up required. In these cases, a patient should undergo the same follow-up as for a BD-IPMN (see section 4.15, and figure 1 for details) (GRADE 2C, strong agreement).
6.4 When does a SCN require surgery and which procedure should be performed?
When the diagnosis of SCN is clear, surgery is recommended only in patients with symptoms related to the compression of adjacent organs (ie, bile duct, stomach, duodenum, portal vein) (GRADE 2C, strong agreement).
The size of about 60% of SCN remains stable. An increase in cyst size is seen in 40% but the rate of growth is slow and new onset of symptoms is very rare.198 203–211
7 Other uncommon and undefined cystic tumours of the pancreas
7.1 When the diagnosis of a cyst is unclear based on a specific imaging modality, should other investigations always be undertaken?
For a cyst measuring <15 mm, either cross-sectional imaging or EUS alone may be performed. 212
For cysts ≥15 mm, or if the diagnosis is unclear, both cross-sectional imaging and EUS should be performed, including EUS-FNA if warranted.
7.2 How should a small, undefined cyst be followed up?
Cysts which are of unclear aetiology, have no risk factors for malignancy, and measure <15 mm, should be re-examined after 1 year. If stable for 3 years, follow-up may be extended to every 2 years. 209 Cysts measuring ≥15 mm should be followed up every 6 months during the first year and annually thereafter 107 (GRADE 2C, strong agreement).
As an undefined cyst may be mucinous by nature, surveillance is recommended.85 107 Most studies report that the risk of malignant transformation of PCN increases with size. This probably also applies to cysts of unclear aetiology.
A prospective population-based study found that unidentified cysts are very common (49% when including diameters of ≥2 mm), increase in number and size with age of the population (57% of subjects), but have no effect on pancreatic disease-associated mortality over 5 years.32
Recommendations that include 6-month surveillance intervals may therefore constitute overtreatment in cases where IPMN and MCN have been ruled out.
7.3 Duration of follow-up of undefined cysts
Patients with undefined cysts should undergo lifelong follow-up, unless the patient is unwilling, or unfit to undergo pancreatic surgery (GRADE 2C, strong agreement).
The long-term evolution of PCN is still largely unknown, which also applies to undefined pancreatic cysts. Therefore, no rational term for termination of surveillance can be given. However, recent data suggest that the risk of progression increases over time.107
7.4 Should all solid-pseudopapillary neoplasms (SPN) be resected?
Radical resection should be performed for all SPN (GRADE 1B, strong agreement).
Even in the absence of a large series, the surgical resection of SPN is internationally recommended and associated with positive long-term outcome.213 214
7.5 Can locally advanced SPN be resected? Should synchronous or metachronous metastases be resected?
In cases of locally advanced, metastatic or recurrent SPNs, an aggressive surgical approach, with complete resection is indicated (GRADE 2C, strong agreement).
SPNs are rare, and there is a lack of high-quality studies to guide care. Most studies are small, retrospective case series, making comparison between studies difficult.215–217
7.6 How is the diagnosis of a cystic pancreatic neuroendocrine tumour (PNEN) established?
A definitive diagnosis of a cystic PNEN can be established only by histological examination. A preoperative diagnosis is often suspected based on particular features of cross-sectional imaging, and can be confirmed by EUS-guided cytology (GRADE 2C, strong agreement).
Cystic PNEN often have a peripheral hypervascular rim visible on an arterial phase CT scan.218–220 However, SCN may have a similar appearance, hampering differentiation. Data on functional imaging with Octreoscan, or Gallium Octreotate positron emission tomography in cystic PNEN are limited.
7.7 What are the indications to resect cystic PNEN and which procedures are recommended?
For cystic PNEN >20 mm, surgery is recommended (pancreatoduodenectomy, distal pancreatectomy, or enucleation (including lymphadenectomy), according to tumour localisation).
For asymptomatic cystic PNEN ≤2 cm, in the absence of signs of malignant behaviour, surveillance is recommended (GRADE 2C, strong agreement).
A recent meta-analysis concluded that cystic PNENs tend to be biologically less aggressive than their solid counterparts. Despite this, cystic PNENs have an approximately 20% risk of malignancy, with a 5-year overall survival of 87–100%.221 A small tumour diameter is a favourable prognostic factor among PNENs. Therefore, small cystic PNENs ≤20 mm may be considered as indolent tumours with a small risk of malignant transformation222 and an observational strategy has been suggested in the absence of symptoms.
7.8 Which are the rare cystic pancreatic lesions? When should they be considered and how is the diagnosis established?
Rare cystic pancreatic lesions include hydatid cysts, haemangioma, lymphoepithelial cysts, acinar cell cystadenomas, desmoid cysts, and haemolymphangiomas. 223–229 Such cysts require a multidisciplinary approach, in an expert pancreatic centre, to determine the optimum management strategy. Surgery may be necessary if the diagnosis remains unclear (GRADE 2C, strong agreement).
8 Adjuvant and neoadjuvant treatment
8.1 Is adjuvant treatment recommended for resected IPMN or MCN with associated invasive carcinoma? if yes, what is the optimal regimen?
Adjuvant systemic chemotherapy is recommended for IPMN with an associated invasive carcinoma with or without positive lymph node status, as they have more aggressive biological behaviour 165 230–239 (GRADE 1C, strong agreement).
As for patients with pancreatic cancer, adjuvant treatment can also be recommended for patients without lymph node involvement, but there is no scientific evidence to support this.
Adjuvant treatment of MCN-associated invasive carcinoma is similar to sporadic pancreatic adenocarcinoma, although no evidence is available to support or refute this approach (GRADE 2C, strong agreement).
No specific recommendation can be given for which chemotherapy agent should be used, as there is substantial heterogeneity among studies. The most commonly used drugs are 5-fluorouracil and gemcitabine, similar to adjuvant treatment of pancreatic adenocarcinoma (GRADE 2C, strong agreement).
8.2 Is neoadjuvant treatment recommended for locally advanced carcinoma associated with an IPMN or MCN?
No recommendation can be made for neoadjuvant treatment of locally advanced IPMN- or MCN-associated invasive carcinoma, as there are insufficient data 240–243 (GRADE 2C, strong agreement).
Two case reports have been published, supporting the use of preoperative chemotherapy for IPMN and MCN.244 245 An approach similar to that used for patients with pancreatic cancer can be considered, given the similarities between the two diseases.
8.3 Is adjuvant or neoadjuvant treatment indicated for SPN? If yes, what is the optimum regimen?
Neoadjuvant therapy for SPN is not routinely recommended, as there are no studies proving its efficacy (GRADE 2C, strong agreement).
The only data for neoadjuvant or adjuvant therapy for SPN are from case reports, the majority of which report different chemotherapy regimens, and many of which were used in a palliative setting after postsurgical recurrence.246–252
8.4 Is palliative chemotherapy recommended for non-resectable or recurrent malignant cystic tumours of the pancreas?
Systemic palliative chemotherapy for non-resectable or recurrent malignant cystic tumours may be considered as for pancreatic adenocarcinoma, although there is no evidence available to support or refute this approach 230 253 254 (GRADE 2C, strong agreement).
Given the similarity to pancreatic cancer, palliative chemotherapy may be considered for patients with non-resectable, recurrent, or metastatic disease occurring in the setting of a malignant IPMN or MCN, analogous to pancreatic cancer.
8.5 Is surgical resection of metastases, or recurrence of an IPMN or MCN cancer justified?
Surgical resection of metastasis, or local recurrence cannot be recommended because there are no studies evaluating this (GRADE 2C, strong agreement).
9 Pathology
9.1 How should PCN surgical specimens be examined?
Specimen dissection
Axial specimen slicing is the standard in an increasing number of European countries and pancreatic centres 255 256 (GRADE 2C, strong agreement).
No studies have been published on the optimal grossing of pancreatic resection specimens with cystic lesions.
Macroscopic examination
Size, uni-/multilocularity, wall thickness, solid areas/mural nodules, cyst content, relationship to the duct system, and appearance of the background pancreas should be documented. In the case of macroscopically visible invasive carcinoma, a full macroscopic description is required, similar to that documented in ductal adenocarcinoma. The spatial relationship and distance of the cancer from the cystic lesion should be recorded. 257 258 (GRADE 2C, strong agreement).
Tissue sampling
Extensive sampling is paramount to establish an accurate diagnosis. Sampling of the resection margins should be conducted as recommended for pancreatic specimens resected for pancreatic ductal adenocarcinoma (GRADE 2C, strong agreement).
The minimum number of tissue samples that should be taken to ensure accurate diagnosis has not been established for PCN.
9.2 How should surgical specimens with an IPMN lesion be examined and reported?
Gross examination
See statement 1.1. Involvement of the MPD and/or branch duct(s), the length of the MPD that is macroscopically involved, and the largest diameter of the dilated MPD or of the cyst, in cases of BD-IPMNs, should be recorded. In cases of multifocal BD-IPMNs, the largest diameter of each lesion should be reported 257 (GRADE 2C, strong agreement).
Histopathological examination
IPMN without an invasive carcinoma:the histological subtype should be documented (gastric, intestinal, pancreatobiliary or oncocytic), based on morphology and immunohistochemical staining. 259 260 For grading of dysplasia in an IPMN, the use of a two-tiered classification system (low-grade vs high-grade dysplasia) is recommended 258 (GRADE 2C, strong agreement).
IPMNs with associated invasive carcinoma:the largest diameter of the invasive lesion should be measured and reported, in addition to the overall size of the lesion. The associated invasive carcinoma should be reported according to the WHO and Union for International Cancer Control (UICC) recommendations. 261 If transition from an IPMN to invasive carcinoma is not demonstrable, complete sampling of the intervening tissues should be conducted to substantiate whether the IPMN and invasive carcinoma are truly separate. 258 (GRADE 2C, strong agreement).
The term ‘malignant IPMN’ should not be used. Instead, it should be simply stated whether invasion is present or not.257 258 It is important to assess the histological subtype of IPMN, since it is associated with prediction of postoperative patient prognosis. The pancreatobiliary subtype, for example, is considered to be strongly associated with malignancy.262
9.3 How to examine and report surgical specimens with an MCN?
Gross examination
See statement 9.1.
Histopathological examination
The use of a two-tiered grading system for dysplasia (low vs high-grade) is recommended. 257 The terms malignant MCN, invasive MCN, or mucinous cystadenocarcinoma should be abandoned and replaced by ‘MCN with associated invasive carcinoma’, according to the WHO and UICC recommendations 258 263 (GRADE 2C, strong agreement)
9.4 Use of potential molecular markers
See statement 1.1.
9.5 Methodology for evaluation of cytology in PCN
EUS-FNA is the preferred method for obtaining cytology in PCN. The preparation of the aspirated fluid may differ between laboratories: direct smears for thick mucus, cytospins, and liquid-based preparation for fluid material (GRADE 2C, strong agreement).
Cytology for PCN has a low sensitivity but a high specificity (see statement 3.5).263 Low sensitivity and frequent non-diagnostic yield are mainly due to low cellularity of the aspirated fluid.
9.6 How to interpret and report PCN cytology
A six-tiered classification system can be used. 259 The mucinous or non-mucinous nature of a PCN and the degree of dysplasia are the most significant determinants of patient management 264 265 (GRADE 2C, strong agreement).
International consensus on standardised terminology for pancreas cytology is lacking.
Discussion
The European evidence-based guidelines on PCN aim to improve the diagnosis and management of PCN. Eventually, the European Study Group on Cystic Tumours of the Pancreas strives to develop a global evidence-based guideline for PCN in a joint venture with the various national and international guideline groups, in order to harmonise care and to avoid confusion caused by conflicting statements. Future studies should deal with the optimal diagnosis (aetiology and neoplastic grade), appropriate selection criteria for surgery, surgical strategy (ie, partial or total pancreatectomy), and follow-up strategy. Especially, identification of patients who do not require follow-up and may be discharged deserves further attention, as patient burden and societal costs of lifelong follow-up with cross-sectional imaging are substantial.
Compared with the recently updated Fukuoka guidelines,8 this evidence-based guideline shows similar relative and absolute indications for surgery based on radiological findings. This guideline is, however, more conservative in the management of side-branch IPMN. Furthermore, new-onset diabetes mellitus is a relative indication for surgery, whereas this is not mentioned in the Fukuoka guidelines.
Also, a recent international survey revealed that consensus is lacking among international experts about the management of MT/MD-IPMN.122 These dilemmas clearly demonstrate that future prospective, multicentre studies are required to provide the necessary evidence to guide management, see box 1. The European study group supports the international multicentre PACYFIC study (www.pacyfic.net), an accessible cyst registry, which aims to obtain long-term follow-up of over 5000 people with an asymptomatic pancreatic cyst.
Current clinical dilemmas in pancreatic cystic neoplasms (PCN) and topics for future research
Diagnostic investigation
Which modality can most reliably distinguish neoplastic from non-neoplastic cysts (eg, imaging, needle-based confocal laser endomicroscopy, cyst fluid analysis, secretin-stimulated pancreatic juice collections)?
Which modality can most reliably detect high-grade dysplasia or early cancer (neoplastic progression) in patients with PCN, to enable timely resection?
Surgery
What are absolute and relative (contra)indications for surgery in main duct (MD) and branch duct intraductal papillary mucinous neoplasm (BD-IPMN), especially in the subgroup 30–40 mm BD-IPMN?
How extensive should a resection for MD-IPMN be (total vs partial pancreatectomy)?
Is there a role for pre-/intraoperative pancreatoscopy to determine the extent of resection in MD-IPMN?
What is the potential benefit of preventive surgery in relation to potential side effects, especially in patients with increased surgical risk or a limited life expectancy due to comorbidity?
Surveillance
What is a cost-effective and personalised approach to surveillance of (undefined) PCN?
Which risk factors for progression need to be considered (eg, cyst size, smoking, diabetes mellitus, concurrent immunosuppression, familial pancreatic cancer history, other genetic syndromes)?
What is the optimal modality and follow-up scheme for patients after a partial pancreatic resection for IPMN?
Acknowledgments
The European Study Group on Cystic Tumours of the Pancreas is grateful to the UEG, EPC, E-AHPBA, EDS, ESGE and Cancerfonden Sweden for their support and thanks Professor Patrick Bossuyt, Academic Medical Center Amsterdam for the methodological support.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators This guideline has been made possible by a large group of collaborators. These collaborators formed the writing committee, methodology committee, nine review groups and the manuscript committee. The initial draft of the manuscript was written by Marco Del Chiaro (Karolinska) with the help of Lianne Scholten, Marc G Besselink (both AMC). The following collaborators were each involved in one or more of the committees and review groups (see supplementary material for details): Marco Del Chiaro, Marc G Besselink, Lianne Scholten, Marco J Bruno, Djuna L Cahen, Thomas M Gress, Jeanin E van Hooft, Markus M Lerch, Julia Mayerle, Thilo Hackert, Sohei Satoi, Alessandro Zerbi, David Cunningham, Claudio De Angelis, Marc Giovannini, Enrique de-Madaria, Peter Hegyi, Jonas Rosendahl, Helmut Friess, Riccardo Manfredi, Philippe Lévy, Francisco X Real, Alain Sauvanet, Mohammed Abu Hilal, Giovanni Marchegiani, Irene Esposito, Paula Ghaneh, Marc RW Engelbrecht, Paul Fockens, Nadine CM van Huijgevoort, Christopher Wolfgang, Claudio Bassi, Natalya B Gubergrits, Caroline Verbeke, Günter Klöppel, Aldo Scarpa, Giuseppe Zamboni, Anne Marie Lennon, Malin Sund, Nikolaos Kartalis, Lars Grenacher, Massimo Falconi, Urban Arnelo, Kostantin V Kopchak, Kofi Oppong, Colin McKay, Truls Hauge, Kevin Conlon, Mustapha Adham, Güralp O Ceyhan, Roberto Salvia, Christos Dervenis, Peter Allen, François Paye, Detlef K Bartsch, Matthias Löhr, Massimiliano Mutignani, Johanna Laukkarinen, Richard Schulick, Roberto Valente, Thomas Seufferlein, Gabriele Capurso, Ajith Siriwardena, John P Neoptolemos, Aldis Pukitis, Ralf Segersvärd, A Aghdassi, S Andrianello, P Bossuyt, R Bülow, K Cárdenas-Jaén, P Cortegoso, M Fontana, L Haeberle, M Heckler, A Litvin, K Mann, C Michalski, P Michl, G Nappo, G Perri, S Persson, F Scheufele, F Sclafani, M Schmidt, L Venezia, F Volker, M-P Vullierm, and L Wüsten.
Correction notice This article has been corrected since it published Online First. Massimo Falconi has been added to the collaborator list.