Article Text

Abstract
Objective This study evaluated the preresection accuracy of optical diagnosis of T1 colorectal cancer (CRC) in large non-pedunculated colorectal polyps (LNPCPs).
Design In this multicentre prospective study, endoscopists predicted the histology during colonoscopy in consecutive patients with LNPCPs using a standardised procedure for optical assessment. The presence of morphological features assessed with white light, and vascular and surface pattern with narrow-band imaging (NBI) were recorded, together with the optical diagnosis, the confidence level of prediction and the recommended treatment. A risk score chart was developed and validated using a multivariable mixed effects binary logistic least absolute shrinkage and selection (LASSO) model.
Results Among 343 LNPCPs, 47 cancers were found (36 T1 CRCs and 11 ≥T2 CRCs), of which 11 T1 CRCs were superficial invasive T1 CRCs (23.4% of all malignant polyps). Sensitivity and specificity for optical diagnosis of T1 CRC were 78.7% (95% CI 64.3 to 89.3) and 94.2% (95% CI 90.9 to 96.6), and 63.3% (95% CI 43.9 to 80.1) and 99.0% (95% CI 97.1 to 100.0) for optical diagnosis of endoscopically unresectable lesions (ie, ≥T1 CRC with deep invasion), respectively. A LASSO-derived model using white light and NBI features discriminated T1 CRCs from non-invasive polyps with a cross-validation area under the curve (AUC) of 0.85 (95% CI 0.80 to 0.90). This model was validated in a temporal validation set of 100 LNPCPs (AUC of 0.81; 95% CI 0.66 to 0.96).
Conclusion Our study provides insights in the preresection accuracy of optical diagnosis of T1 CRC. Sensitivity is still limited, so further studies will show how the risk score chart could be improved and finally used for clinical decision making with regard to the type of endoresection to be used and whether to proceed to surgery instead of endoscopy.
Trial registration number NTR5561.
- colorectal adenomas
- colorectal cancer
- colonoscopy
- colorectal carcinoma
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Successful treatment of large non-pedunculated colorectal polyps (LNPCPs) starts with accurate optical differentiation between adenomas and T1 colorectal cancer (CRC), and predicting the depth of invasion when CRC is suspected.
The preresection accuracy of prediction of malignancy within a LNPCP is one of the key research questions that has yet to be answered.
What are the new findings?
We are the first to report the preresection accuracy of optical diagnosis of T1 CRC and endoscopically unresectable lesions (ie, ≥T1 CRC with deep invasion) within LNPCPs during colonoscopy in a Western multicentre setting using a standardised procedure for optical assessment.
The recommended treatment was en bloc endoscopic resection in 58 LNPCPs (17.1%), of which T1 CRC was histologically diagnosed in 20 cases (34.5%) consisting of 7 T1 CRCs with superficial invasion (12.1%).
A risk score chart was developed and validated, providing the predicted probability of T1 CRC within a LNPCP based on white light and narrow-band imaging features.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
This multicentre study provides insights in the preresection accuracy of optical diagnosis of T1 CRC, and facilitates a risk score chart which could help to further develop optical criteria for selective use of en bloc resection techniques in LNPCPs with a high risk of T1 CRC. Further studies will show how the risk score chart could be improved and finally used for clinical decision making with regard to the type of endoresection to be used and whether to proceed to surgery instead of endoscopy.
Introduction
Endoscopic resection is the first-line treatment for large non-pedunculated colorectal polyps (LNPCP, ie, sessile/flat polyps exceeding 2 cm in size).1 2 Piecemeal endoscopic mucosal resection (pEMR) is a widely available technique and has proven its efficiency with curative resection rates >90%.3 However, malignant LNPCPs require a different treatment approach.4 Endoscopic treatment is curative for superficial invasive T1 colorectal cancers (CRCs) provided that the risk for lymph node metastasis (LNM) and incomplete resection is low. pEMR hampers evaluation of histological high-risk factors for LNM and resection margins, leading to subsequent surgical resection.5–7 Advanced resection techniques such as endoscopic submucosal dissection (ESD) however enable to remove LNPCPs in an en bloc fashion in up to 90% of polyps, hereby enlarging the potential for curative endoscopic resection of T1 CRCs with superficial submucosal invasion.8 Successful treatment of LNPCPs therefore starts with accurate optical differentiation between adenomas and T1 CRC, and predicting the depth of invasion when cancer is suspected.
The British Society of Gastroenterology together with the Association of Coloproctologists of Great Britain and Ireland, have recently provided a guideline regarding the management of LNPCPs.9 The preresection accuracy of prediction of malignancy within an LNPCP was identified as one of the key research questions that has yet to be answered, also in view of the current discussion on the role of ESD in the treatment of LNPCPs. To date, studies evaluating optical features of T1 CRC are mostly performed in Asia.10 Two Australian studies have identified optical features associated with T1 CRC, however, the preresection accuracy of Western endoscopists remains to be explored.11 12 Moreover, studies performed thus far mostly involved image analyses performed by expert endoscopists, but lack information on real-time assessment (ie, during colonoscopy).13
In this prospective multicentre study, we evaluated the real-time diagnostic accuracy of the optical diagnosis of T1 CRC in LNPCP by Western endoscopists using a standardised procedure for optical assessment. Primary aim was to assess the diagnostic accuracy of optical diagnosis of T1 CRC and T1 CRC with deep submucosal invasion. Secondary aim was to assess the diagnostic value of the individual endoscopic features, as scored with conventional (white light) view and narrow-band imaging (NBI), and to develop and validate a score chart with the estimated risk of T1 CRC within an LNPCP based on optical features.
Methods
Study design
This was a prospective multicentre study conducted between September 2015 and December 2016. Endoscopists from nine hospitals (eight non-academic and one academic hospital) participated in this study, all of whom had performed >1000 previous colonoscopies. All were dedicated advanced endoscopists and trained in the endoscopic resection of LNPCPs. The study was approved by the Medical Ethics Review Committee of the University Medical Centre Utrecht (reference number 15/435) and was carried out in accordance with the Helsinki Declaration. Patients’ data were coded and anonymity of patients was guaranteed. The study was registered in the Dutch Trial Register (reference number NTR5561).
Interactive training session
Prior to the start of this study, an interactive training session was held, with the aim to increase uniformity in optical assessment between participants and to train systematic evaluation of LNPCPs. Preceding the training session, endoscopists completed a computer module consisting of images of adenomas and T1 CRCs (collected from literature and our own image database), in which they were asked to provide their optical diagnosis. In a following 2-hour interactive training session, the definitions of endoscopic features associated with T1 CRC as identified in literature were discussed,10 together with the cases from the computer module with direct feedback on the histological diagnosis. All participating endoscopists attended the meeting.
Real-time optical diagnosis
Subsequently, the histology was predicted in consecutive patients with LNPCPs using macroscopic features and NBI during real-time colonoscopy. All LNPCPs, defined as sessile and flat colonic lesions ≥2 cm in size, detected in patients aged ≥18 years were included.9 Obvious advanced cancers (≥T2) or LNPCPs that were known to harbour cancer due to previous biopsies were not included. Patients were excluded if endoscopy suites were not equipped with endoscopes with NBI at the time of detection. Colonoscopies were performed using high-definition endoscopes (listed in online supplementary table S1).
Supplementary file 1
A standardised procedure for photographing and optical assessment was followed. Mucus was flushed away carefully. First, gross morphology was evaluated during white light assessment. Then, two white light endoscopic images were taken. Second, NBI assessment of the polyp was performed, with special interest in potential target areas such as nodules or depressed areas. If the polyp was suspected to contain T1 CRC, NBI images were taken from the suspicious area. Two magnifying NBI images were taken. After assessment, the endoscopists recorded their optical diagnosis blinded for the histology, and declared whether this was made with a low or high confidence, together with the recommended therapy based on the optical diagnosis.
Endoscopic features
Potential white light and NBI features were selected by conducting a systematic review of current literature on this topic.10 Established features were discussed during the interactive training session. Features considered relevant were selected based on availability of a definition, reported diagnostic accuracy and number of previous studies that had assessed these features. Selected white light features included polyp location, surface structure, presence of a depressed area, excavation and spontaneous bleeding.4 10 Proximal location was defined as location proximal to the splenic flexure. The surface structure was recorded as granular for LNPCPs with a nodular surface or non-granular for LNPCPs with a smooth surface.4 If granular, the lesion was further specified as being homogeneous granular, granular with a depressed area, granular with a large nodule or granular with a non-granular erythematous area. If a depressed area was observed, it was specified whether it was well demarcated or not. Excavation was defined as a crumbled, damaged area of the LNPCP that prevented observation of the surface structure.14 Multiple NBI classifications were identified in literature.15–18 The Hiroshima classification was selected for this study, as this classification has been evaluated for both the optical diagnosis of T1 CRC and T1 CRC with deep invasion in Asian studies (online supplementary table S2).10 All above-mentioned features were scored on case report forms, and stored in a centralised database together with the corresponding images.
Reference standard
The histological diagnosis using standard haematoxylin-eosin staining served as diagnostic reference standard. Specimens were evaluated by local pathologists, accredited for the Dutch CRC screening programme, indicating adequate experience and quality. Histological diagnosis was carried out according to the Vienna classification of gastrointestinal epithelial neoplasia and the fifth tumour, node, metastases classification of malignant tumours.19 20 T1 CRC was defined as polyps with invasion through the muscularis mucosae and into, but not beyond, the submucosa.20 Deep submucosal invasion was defined as SM2-3 according to Kikuchi et al for surgically resected specimens, or invasion depth ≥1000 µm as measured from the muscularis mucosae to the deepest point of tumour invasion for endoscopically resected specimens.21 22
Statistical analysis
Baseline characteristics were analysed using standard descriptive statistics. Primary aim was to evaluate the diagnostic accuracy of optical diagnosis of T1 CRC (ie, non-invasive vs invasive LNPCPs) and T1 CRC with deep invasion (ie, endoscopically resectable vs endoscopically unresectable LNPCPs). Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) with 95% CIs were calculated and reported as recommended in the Standards for Reporting Diagnostic Accuracy statement.23 Next, the confidence level of the optical diagnosis (low vs high) was compared between correctly and incorrectly diagnosed LNPCPs using the χ 2 test.
Secondary aim was to evaluate the diagnostic value of the endoscopic features. The prevalence of the assessed features in non-invasive polyps vs T1 CRCs and endoscopically resectable vs endoscopically unresectable LNPCPs were analysed using standard descriptive statistics. To facilitate the calculation of the risk of T1 CRC, we developed a score chart. We used a penalised multivariable logistic regression approach, that is, L1 penalised least absolute shrinkage and selection (LASSO) logistic regression augmented with fivefold cross-validation, using the individual endoscopic features as candidate predictors for the presence of T1 CRC. We conducted mixed effects binary logistic LASSO models with random endoscopist and patient intercepts to account for clustering. The score chart was assessed for discrimination (area under the receiver operating characteristic curve (AUC)), calibration and accuracy (ie, sensitivity, specificity, NPV and PPV at different probability thresholds). The chart was validated using data from 100 LNPCPs prospectively assessed in one of the participating centres (UMC Utrecht, academic centre) after the study period (ie, temporal validation). Finally, the AUC of the score chart was compared with and without NBI features to evaluate the value of NBI in addition to white light, and to the AUC of the endoscopists’ optical diagnosis using the DeLongs test in the pROC package of R. Details about all steps performed in the development and validation of the chart can be found in the online supplementary material.
IBM SPSS Statistics V.21 (SPSS, Chicago, Illinois, USA), MedCalc V.15.0 (MedCalc Software, Ostend, Belgium) and R V.3.2.2 were used for statistical analysis. A two-sided P≤0.05 was considered to be statistically significant.
Sample size consideration
Sample size was based on the pooled estimate of sensitivity of 85% (95% CI 75% to 91%) for optical diagnosis of T1 CRC as achieved in Asian studies when NBI features were assessed.10 Prevalence of T1 CRC in LNPCP was estimated to be 15%.4 With a sensitivity of 85% and considering that the lower 95% CI should not fall below 75%, the total number of T1 CRCs needed was 49. To correct for the possibility that pathology would not be available for all patients (ie, no resection performed) and ≥T2 CRC would be included (maximum 5%), the final calculated sample size was 343 LNPCPs.
Results
Baseline characteristics
In total, 343 consecutive LNPCPs in 325 patients (1 patient with 4 LNPCPs, 2 with 3 LNPCPs and 11 with 2 LNPCPs) were eligible for inclusion. Patient and lesion characteristics are provided in table 1. Median age of the cohort was 69 years (IQR 63–75) and 60.9% was male. Among all LNPCPs (n=343), 47 cancers were found: 36 T1 CRCs and 11 ≥T2 CRCs. In total, 3.2% of all LNPCPs concerned superficial invasive T1 CRCs, corresponding to 23.4% of all invasive lesions (ie, T1 CRC or ≥T2 CRC). In 6 T1 CRCs, invasion depth could not be evaluated due to piecemeal resection (n=5) or extensive fibrosis (n=1).
Baseline characteristics of included patients and polyps
Three patients (three LNPCPs) were excluded from further analyses. In two patients, reason for exclusion was that the polyp was not removed due to comorbidity, so no histology was available. In one patient, the polyp was histologically diagnosed as hamartoma, and excluded from the analyses as this is a distinct polyp category. This resulted in 340 LNPCPs in 322 patients eligible for analyses.
Accuracy of optical diagnosis
The overall agreement for differentiating invasive from non-invasive LNPCPs was 92.1% (95% CI 88.9 to 94.8) (table 2). Among all invasive lesions (T1 CRC or ≥T2 CRC, n=47), 37 were correctly identified as such corresponding to a sensitivity of 78.7% (95% CI 64.3 to 89.3). In the 10 misidentified CRCs, optical diagnosis was high-grade dysplasia (HGD) in four cases and low-grade dysplasia (LGD) in six cases.
Diagnostic accuracy of optical diagnosis of T1 CRC (ie, non-invasive vs invasive LNPCPs) and T1 CRC with deep submucosal invasion (ie, endoscopically resectable vs endoscopically unresectable LNPCPs)
Diagnostic agreement for differentiating deep invasive CRC (T1 CRC with deep invasion or ≥T2 CRC, n=30) from non-invasive or superficial invasive T1 CRC (n=304) was 95.8% (95% CI 93.4 to 97.9). In three LNPCPs, the endoscopist incorrectly predicted the polyp to contain deep invasive T1 CRC, whereas it appeared to be adenomas with LGD (n=2) and HGD (n=1). In 11 LNPCPs, the endoscopist incorrectly predicted the polyp to contain LGD (n=2), HGD (n=3) or superficial invasive T1 CRC (n=6), whereas histology revealed deep invasive CRC. This resulted in an NPV of 96.5% (95% CI 94.5 to 97.7).
In 32 LNPCPs (9.4%) biopsies had been taken before optical assessment, in 35 LNPCPs (10.3%) biopsies were taken after optical assessment and in 273 LNPCPs (80.3%) no biopsies were taken. Diagnostic accuracy was comparable when excluding patients in whom biopsies had been taken before optical assessment. Moreover, excluding patients with ≥T2 CRCs provided similar outcomes (online supplementary table S3).
Confidence level
In 111 LNPCPs (32.6%), the confidence level of optical diagnosis was low. Optical diagnosis of T1 CRC (ie, non-invasive vs invasive LNPCPs) was significantly more often incorrect when endoscopists had a low vs high confidence about their prediction (16.2% vs 3.9%, P<0.001). This was also observed for optical diagnosis of endoscopically unresectable LNPCPs (7.5% vs 2.6%, P=0.04). Among the misidentified T1 CRCs (n=8), confidence level of optical diagnosis was low in 62.5% of cases (5/8).
Recommended treatment
The recommended treatment based on optical diagnosis was en bloc endoscopic resection in 58 LNPCPs (17.1%; table 3), of which T1 CRC was histologically diagnosed in 20 cases (34.5%), consisting of 7 T1 CRCs with superficial invasion (12.1%). Among 11 superficial T1 CRCs, 4 were at high risk for LNM (ie, presence of lymphovascular invasion or poor differentiation); all others were low-risk T1 CRCs (ie, no histological high-risk features). In addition, histological high-risk criteria were present in one of six T1 CRCs with undetermined invasion depth.
Recommended treatment for 340 LNPCPs based on the optical diagnosis of the endoscopist with the corresponding histological diagnosis
White light and NBI features
The presence of white light and NBI features in non-invasive polyps (n=293) vs T1 CRCs (n=36) and in endoscopically resectable (ie, non-invasive polyps and T1 CRCs with superficial submucosal invasion, n=304) vs endoscopically unresectable (ie, T1 CRCs with deep submucosal invasion, n=19) LNPCPs are presented in table 4. White light features significantly more often observed in T1 CRCs and endoscopically unresectable LNPCPs were: location in distal colon or rectum, non-granularity, a depressed area, excavation and spontaneous bleeding (table 4). In granular LNPCPs, T1 CRCs and endoscopically unresectable LNPCPs more often had an erythematous non-granular area or depressed component. The risk for T1 CRC increased with increasing Hiroshima classification (type C vs type A–B: 77.8% vs 17.1%, P<0.001). Hiroshima classification type ≥C2 (68.4% vs 3.6%, P<0.001) and type C3 (47.4% vs 1.0%, P<0.001) were more often observed in endoscopically unresectable LNPCPs.
Optical features in non-invasive vs invasive LNPCPs and in endoscopically resectable vs endoscopically unresectable LNPCPs, as scored with white light and NBI
Risk chart
Selected variables for the risk chart were: location, surface structure, depressed area, spontaneous bleeding and the Hiroshima classification. Using these features, discrimination of T1 CRCs from non-invasive polyps was good (cross-validation (cv)AUC 0.85; 95% CI 0.80 to 0.90). Including age and sex as candidate predictors did not improve the risk score (ie, did not improve the cvAUC). The coefficient profile plot, ROC curve plotted for each cross-validation set, the calibration plot, regression coefficients and LASSO-derived multivariate ORs can be found in online supplementary figure S1-4 and table S3 supplementary material.
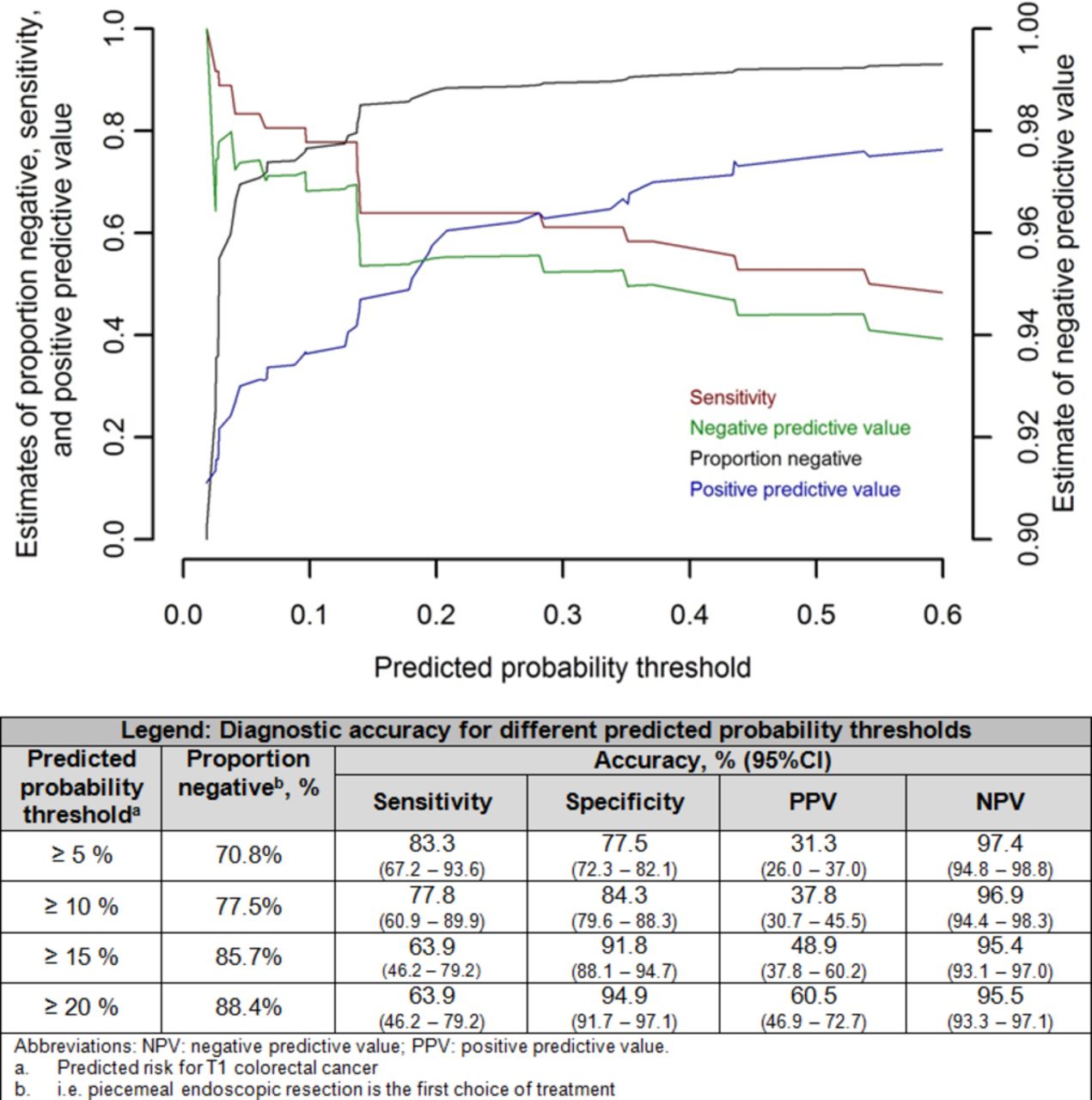
Table 5 shows the score chart for prediction of T1 CRC within LNPCPs in the presence or absence of these features. In our data, the (apparent) AUC of the score chart was 0.87 (95% CI 0.78 to 0.95). Within our cohort, 70.8% of LNPCPs had an estimated risk of T1 CRC <5%, 77.5% <10% and 85.7% <15%. Figure 1 shows the corresponding sensitivity, PPV and NPV for different probability thresholds (ie, estimated risk for T1 CRC). For example, using an estimated risk of 10% as an indication for en bloc resection results in a sensitivity for optical diagnosis of T1 CRC of 77.8% (95% CI 60.9 to 89.9), specificity of 84.3% (95% CI 79.6 to 88.3), a PPV of 37.8% (95% CI 30.7 to 45.5) and an NPV of 96.9% (95% CI 94.4 to 98.3).
{kind=link}
Estimates of proportion negative (ie, piecemeal endoscopic resection is the first choice of treatment), sensitivity, positive and negative predictive value for different predicted probability thresholds for T1 CRC within an LNPCP as provided in table 5. The table legend provides the diagnostic accuracy for different probability thresholds.
The LASSO-derived predicted probability in percentage (with 95% prediction intervals) of T1 CRC within an LNPCP based on location, white light features and NBI features
In a final step, we validated the risk score chart using data from 100 consecutive LNPCPs (15 T1 CRCs and 85 non-invasive LNPCPs) assessed by two endoscopists (LMGM and PD) after the study period. In the validation set, an AUC of 0.81 (95% CI 0.66 to 0.96) was achieved (online supplementary figure S5). As these LNPCPs were assessed in a tertiary centre with a higher prevalence of T1 CRC (15.0%), we expected an underestimation of the observed risk for T1 CRC which was indeed seen (online supplementary figure S4C). The calibration plot with an updated intercept (−1.90 to −1.20, ie, the intercept of the same centre in the development set) revealed good calibration (online supplementary figure S4D).
Comparison of AUCs
The (apparent) AUC of the score chart was comparable with the AUC of the endoscopists’ optical diagnosis (AUC: 0.86; 95% CI 0.79 to 0.93), with an absolute difference of 0.01 (95% CI −0.09 to 0.10) in favour of the risk chart, P=0.92. When NBI features were excluded from the risk chart, the AUC decreased to 0.78 (95% CI 0.69 to 0.87), an absolute difference of 0.08 (95% CI 0.03 to 0.14), P=0.002.
Discussion
To our knowledge, our study is the first to report the preresection accuracy of optical diagnosis in LNPCPs by Western endoscopists during colonoscopy. Sensitivity for optical diagnosis of T1 CRC was 78.7% (95% CI 64.3 to 89.3), comparable to sensitivities reported in Asian studies varying between 78% and 100% when NBI is used.15 17 24 25 Specificity for optical diagnosis of endoscopic unresectable lesions (ie, ≥T1 CRC with deep invasion) was 99.0% (95% CI 97.1 to 100), also comparable to reported specificities between 85% and 100% in Asian studies.10 Optical diagnosis was significantly more often incorrect when endoscopists had a low versus high confidence about their prediction, suggesting that an en bloc excision biopsy or consultation of a trained colleague in situations where the confidence of optical diagnosis is low might help to further reduce the number of misidentified T1 CRCs. Moreover, we observed that the performance to discriminate non-invasive LNPCPs from T1 CRCs with only a few white light and NBI features was good (cvAUC of 0.85 (95% CI 0.80 to 0.90) in the development set, AUC of 0.81 (95% CI 0.66 to 0.96) in the validation set).
There is a narrow gap between LNPCPs in which piecemeal resection is sufficient (non-invasive lesions) and LNPCPs in which surgery is the preferred treatment (≥T1 CRC with deep invasion). In our study, T1 CRCs eligible for endoscopic resection accounted for 3.2% of all LNPCPs and 23.4% of all malignant polyps. Moreover, superficial T1 CRC was diagnosed in only 12.1% of LNPCPs in which en bloc endoscopic resection was recommended, illustrating that the proportion of patients benefiting from a selective en bloc endoscopic resection approach is still small. This may however change in the near future. Improvements in risk stratification might increase the number of T1 CRCs in which surgery can safely be omitted. To date, only 19%–29% of all T1 CRCs can be identified as low-risk T1 CRCs, due to the inaccuracy of the current used histological factors to sufficiently predict the presence of LNM.5 6 In this study, an invasion depth ≥1000 µm was used as cut-off for deep invasive T1 CRC, in line with previous studies.10 26 However, it is questionable whether this is the ideal cut-off, as cut-offs of 2000 or 3000 µm have also been proposed.27–29 Moreover, earlier studies reported that the risk of LNM is extremely low in deep invasive T1 CRC in the absence of other high-risk factors.29–32 Evolving molecular diagnostics have the potential to improve the prediction of LNM, and may expand the number of curative local minimal invasive resections.33 Furthermore, increased experience with en bloc endoscopic resection techniques such as ESD and full-thickness resection, and a better infrastructure to expert centres once cancer is suspected, might increase the number of en bloc resections with negative resection margins. In our cohort, five among seven en bloc EMR attempts on T1 CRCs ended up in a non-curative piecemeal or R1 resection (with histological high-risk factors in only two cases), and five deep invasive T1 CRCs in which en bloc endoscopic resection was performed had no other high-risk factors (poor differentiation or lymphovascular invasion) other than deep invasion. This underlines that, parallel to improvement in optical diagnosis, continuous effort to improve resection techniques and risk stratification is needed to further increase the number of patients that benefit from optical diagnosis.
We developed and validated a risk chart enabling to estimate the risk for T1 CRC within an LNPCP, which might have two important clinical implications. First, the chart will allow to develop strict criteria for selective use of expensive and time-consuming en bloc resection techniques. The role of ESD in the treatment of LNPCPs is currently under debate.34–36 It is questionable whether the prolonged procedure time and still limited availability in Western countries outweigh the benefits of high en bloc resection rates, low recurrence rates and the potential for curative endoscopic resection in a subset of T1 CRCs.8 37 Selective use of ESD in lesions with a high-risk of T1 CRC reduces the number of patients needed to treat with ESD to prevent surgery in one patient, and preliminary evidence shows that this strategy appears more cost-effective than an universal ESD or wide-field EMR approach.38 Second, the chart is a simple, pragmatic and easily assessable tool for less experienced endoscopists. The endoscopists that participated in this study were dedicated advanced endoscopists that were—in addition to the scored features—also informed about other factors (eg, hardness of the polyp and lifting). The risk chart was build using LASSO analysis, an approach in which only the strongest predictors remain in the model. The observation that the AUC of the risk chart (0.87; 95% CI 0.78 to 0.95) was comparable to the AUC of these advanced endoscopists (0.86; 95% CI 0.79 to 0.93) supports that these features can be used to achieve an accurate optical diagnosis. This will be more time-efficient than referring every patient with an LNPCP to an expert endoscopist for optical assessment, which can then be restricted to situations in which low confidence about the assessment of features and corresponding optical diagnosis exists. Application of the chart only necessitates assessment of white light and NBI features, which has the advantage over magnifying chromoendoscopy that it only requires light adjustment without time-consuming extra steps such as application of dye. This can be performed in just a few minutes, making it an easy-to-use and pragmatic tool applicable in clinical practice.
Although the risk chart showed good calibration in both the development and validation set (online supplementary figure S4), it also showed outliners (ie, adenomas with an estimated high risk of T1 CRC and vice versa). Among eight T1 CRCs with an estimated risk <10% in our cohort, all but one were granular, and in all of them vessel distribution and pattern were scored regular. If the invasive part within a polyp is small and surrounded by LGD, it will be very difficult to optically diagnose it as the cancer will unlikely manifest to the surface (ie, no visible distorted vascular and surface pattern), as also concluded by the Australian Colonic Endoscopic Resection (ACE) group.12 The poor sensitivity of white light features makes it unlikely that white light features not scored in this study will improve diagnostic accuracy.10 12 It could be that extra steps such as other advanced imaging techniques for situations in which no cancer is suspected could further improve optical diagnosis; however, this remains to be explored in future studies.
Our study builds on a recent study performed by the ACE group, who also observed an increased risk of T1 CRC in non-granular and distal LNPCPs.12 The authors observed that about 75% of LNPCPs have a risk of T1 CRC <5%, comparable to 70.8% of LNPCPs in our cohort with an estimated T1 CRC risk <5%.12 Our study adds novel elements, since NBI assessment was performed in all lesions. More importantly, our study informs about the diagnostic efficacy of different endoscopic features, and is—to our knowledge—the first to prospectively evaluate the preresection accuracy of optical diagnosis in LNPCPs, together with the confidence level indicated by the endoscopist and the consequences for the type of treatment chosen.
Several limitations should be emphasised. First, our study represents real-time optical assessment in a multicentre setting. As a result, we cannot rule out that features would have been differently scored by other endoscopists. However, the training session in which definitions were discussed might have limited large interobserver variation. Moreover, variation in rater assessment might also be of benefit for the generalisation of our results to real-world practice. The real-time setting also caused that some LNPCPs had been biopsied before optical assessment. Nevertheless, the diagnostic accuracy when excluding LNPCPs biopsied before optical assessment were comparable, suggesting that similar results would have been obtained if we would have controlled for the timing of optical diagnosis to be before biopsy. Second, we could not evaluate the individual endoscopists’ accuracy. Number of LNPCPs assessed per endoscopist were too small to provide individual data, and also did not enable to explore whether, for example, the type of scope used influenced accuracy. Third, despite our large multicentre cohort, it should be noted that the number of T1 CRCs was still limited. We therefore restricted the score chart to discrimination of T1 CRCs from non-invasive polyps, without accounting for different submucosal invasion depths. Future studies are needed to assess this, potentially by updating the risk score with other features. Although we adopted state-of-the-art data analysis techniques allowing robust multivariable prediction modelling in sparse datasets, the limited number of T1 CRCs unavoidably resulted in less precise estimates. Nevertheless, the risk-score derived estimated predicted probabilities showed good discriminative ability in the validation set strengthening the robustness of the risk chart. The overall underestimation of the risk in the validation calibration plot was expected, since the validation set was derived from a tertiary referral centre with a relatively high prevalence of T1 CRC (15.0%). Following recalibration-in-the-large by only updating the intercept—as has also been done for established risk scores such as the Framingham risk score—also good calibration was accomplished in the validation set.39
This prospective multicentre real-time assessment study was performed in the context of the current discussion regarding the preresection accuracy of optical diagnosis in LNPCPs of Western endoscopists and the role of en bloc endoscopic resection in these polyps. Although we observed a good specificity for optical diagnosis of endoscopic unresectable lesions, our study also shows that the sensitivity for optical diagnosis of T1 CRC could still benefit from improvement. Moreover, the number of patients that benefit from optical diagnosis is currently small. We provided a validated score chart with the absolute risk for T1 CRC in LNPCPs, developed using real-time information on the presence or absence of white light and NBI features, which might be an important step in the process to further define strict indications for ESD only for lesions with a high risk of T1 CRC. Further studies will show how the risk score chart could be improved and finally used for clinical decision making with regard to the type of endoscopic resection to be used and whether to proceed to surgery instead of endoscopy.
References
Footnotes
Contributors YB, MPS, FtB, FHJW, JNG, WHdVtNC, JvB, JMJG, BWMS, FPV, MML, SGE, LMGM: study concept and design. YB, LMGM: study supervision. YB, MPS, FtB, FHJW, JNG, WHdVtNC, JvB, JMJG, BWMS, PD, FPV, MML, LMGM: patient inclusion, acquisition and interpretation of data. YB, SGE, LMGM: data analysis. YB, SGE, LMGM: drafting of the manuscript. LM: principal investigator. All authors were involved in critical revision of manuscript.
Competing interests None declared.
Ethics approval University Medical Centre Utrecht.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Individual participant data that underlie the results reported in this article are available from the corresponding author following publication on reasonable request, after de-identification (text, tables, figures and appendices).