Article Text

Abstract
Objective Hepatitis D virus (HDV) is a defective virus that completes its life cycle only with hepatitis B virus (HBV). The HBV with HDV super-infection has been considered as one of the most severe forms of the chronic viral hepatitis. However, there is a scarcity of data on the global burden of HDV infection.
Design We searched PubMed, Embase, Cochrane Library and China Knowledge Resource Integrated databases from 1 January 1977 to 31 December 2016. We included studies with a minimum sample size of 50 patients. Our study analysed data from a total of 40 million individuals to estimate the prevalence of HDV by using Der-Simonian Laird random-effects model. The data were further categorised according to risk factors.
Results From a total of 2717 initially identified studies, only 182 articles from 61 countries and regions met the final inclusion criteria. The overall prevalence of HDV was 0.98% (95% CI 0.61 to 1.42). In HBsAg-positive population, HDV pooled prevalence was 14.57% (95% CI 12.93 to 16.27): Seroprevalence was 10.58% (95% CI 9.14 to 12.11) in mixed population without risk factors of intravenous drug use (IVDU) and high-risk sexual behaviour (HRSB). It was 37.57% (95% CI 29.30 to 46.20) in the IVDU population and 17.01% (95% CI 10.69 to 24.34) in HRSB population.
Conclusion We found that approximately 10.58% HBsAg carriers (without IVDU and HRSB) were coinfected with HDV, which is twofold of what has been estimated before. We also noted a substantially higher HDV prevalence in the IVDU and HRSB population. Our study highlights the need for increased focus on the routine HDV screening and rigorous implementation of HBV vaccine programme.
- hepatitis D
- hepatitis B
- meta-analysis
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
In the Sub-Saharan Africa study, the prevalence of hepatitis D virus (HDV) was assessed among HBsAg-positive populations in the African regions.
More studies are needed to determine the HDV burden and the risk factors for HDV infection worldwide.
These data are substantial to impel the routine screening for HDV and encourage hepatitis B virus (HBV) vaccine programme.
What are the new findings?
The prevalence of HDV among two special groups (intravenous drug users and people who have high-risk sexual behaviour) was both higher than the mixed population.
The pooled prevalence of HDV among population with HBsAg-positive was twofold as what was estimated before.
The emergence of new HDV genotypes in Europe highlights future challenges.
How might it impact on clinical practice in the foreseeable future?
The trend of HDV infection is not as optimistic as we imagined, suggesting further implementation of international guidelines of HDV screening and HBV vaccination programme.
Introduction
It was estimated that about 248 million individuals were HBsAg positive in 2010 globally.1 As of 2016, an estimated 468 million people were living with hepatitis B and 119 million people were newly infected in this year.2 Scientific studies have shown that the hepatitis B virus (HBV) infection, which was discovered in 1963 by Blumberg, is the most common cause of hepatocellular carcinoma (HCC) worldwide.3 The percentage of patients with liver cirrhosis and liver cancer due to HBV have increased substantially between 2006 and 2016.2 Hepatitis D virus (HDV) was first discovered by Rizzetto and colleagues in the mid-1970s while investigating a group of patients with HBV with severe hepatitis.4 HDV is a satellite virus that can propagate only with the existence of HBV.4 It is estimated that about 5% of chronic HBV carriers are coinfected with HDV based on the data published between the 1980s and 1990s,5 which means that around 15–20 million people are HDV carriers worldwide.6
Studies have consistently shown that the chronic HBV and HDV coinfection is the most severe form of viral hepatitis,5 which has a much higher risk of developing cirrhosis and HCC than HBV monoinfection.4 By 2015, 97 nations have included the HBV birth dose vaccine, and 180 countries included the HepB3 vaccine (HepB3=three doses of hepatitis B vaccine) in their routine immunisation schedule.7 However, clustered outbreaks of HDV infection still occur8 and the treatment options of HDV infection remain limited. Relapse could still be observed after the use of interferon (IFN) α−2α9 or pegylated IFN α−2α.10 Whereas there are three novel therapeutic approaches currently available for chronic HDV infection namely lonafarnib,11 REP2139-Ca12 and Myrcludex B,5 there is no study published in the literature which has evaluated the global burden of HDV infection. Reliable estimates are needed to establish the updated prevalence of HDV infection. We, therefore, aim to investigate the current prevalence, genotype and risk factors causing HDV infection.
Materials and methods
Search strategy and selection criteria
We performed a systematic review and meta-analysis of the published studies for the prevalence of HDV infection in the six continents (except Antarctica). Author HYC searched for the articles on the topic of the prevalence of anti-HDV antibody or HDV RNA or anti-HDV antigen which were published in English and Chinese language in PubMed, Embase, Cochrane Library and China Knowledge Resource Integrated databases, between 1 January 1977 and 31 December 2016. Search strings can be seen in the appendix. PCH and HYC extracted seroprevalence data which was further verified by a third reviewer (DTS) for accuracy. Duplicate data from the same locations were excluded. Data collection included study methods, field-work dates, population sample, recruitment site, sample size, diagnostic assays and prevalence of HBV and HDV infections. Only studies which had an availability of information about HDV seroprevalence, patient selection methods and the geographical and clinical setting were included in the analysis. Data for the infants or the children were excluded because of their immature immune system. We divided people into two study groups. One is general population without any risk factors, and the other is HBsAg carriers. In general population, individuals were further divided into two subgroups (1977–1996; 1997–2016). In HBsAg carriers, Individuals without risk factors such as intravenous drug use (IVDU) and high-risk sexual behaviour (HRSB) were called as mixed population. The analytic framework and key topics that guided the review are shown in figure 1. We also contacted the study authors for the clarifications if required. Our study was done in accordance with the PRISMA recommendations.

Analytic framework: HDV epidemiology. HDV, hepatitis D virus; HRSB, high-risk sexual behaviour; IVDU, intravenous drug use.
Statistical analysis
CIs were computed by the Wilson method, and pooled seroprevalence was calculated with the DerSimonian-Laird random-effects model with Freeman-Tukey double arcsine transformation.13 14 We chose a random-effects model a priori because we anticipated a heterogeneity arising from the variation in populations and sociodemographic index (SDI) levels. To avoid small sample bias in the random effects model, we excluded studies with fewer than 50 patients. We estimated heterogeneity between the studies with the I² statistic, which describes the percentage of variation between the studies that is due to heterogeneity rather than a chance.15 16 Meta-regression was done with a residual maximum-likelihood model to examine the sources of the heterogeneity related to populations and SDI levels, publication year and the study location.
We performed sensitivity analyses to investigate the effects of population source and potentially unrepresentative samples. The analyses were done with metan, metaprop and metareg packages in Stata (V.14.2).
Results
Our search returned 2717 records, 182 of which were finally included in the analysis after meeting the inclusion and exclusion criteria (figure 2). These studies described 295 cohorts from 61 countries and regions. These cohorts were comprised a total of 40 127 988 individuals (table 1), encompassing around 0.54% of the global population. HDV prevalence in the general population was 0.98% (95% CI 0.61 to 1.42) (online supplementary appendix figure S1) and in the pooled HBsAg-positive population was 14.57% (95% CI 12.93 to 16.27) (figure 3A) worldwide. In the general population, HDV seroprevalence varied widely among countries, from 0% to 8.03% (95% CI 5.26 to 12.08) in France and Mongolia, respectively. There are approximately 72 451 000 HDV-infected individuals all over the world. China has the largest burden, representing 8.68% of the total disease burden (table 2), which is mainly due to the large population base.
Supplemental material
Summary of country and regional HDV prevalence estimates in general population and three HBsAg-positive populations
Global estimates of HDV infection in general population by global burden of disease region

Flowchart of study selection.

Forest plot showing meta-analysis of hepatitis D virus seroprevalence among selected HBsAg-positive populations (A), in general individuals with different SDI levels (B) and different gender (C). Weights are from random effects analysis. Full data available in online supplementary appendix. HRSB, high-risk sexual behaviour; IVDU, intravenous drug use; SDI, sociodemographic index.
Analysis of risk factors
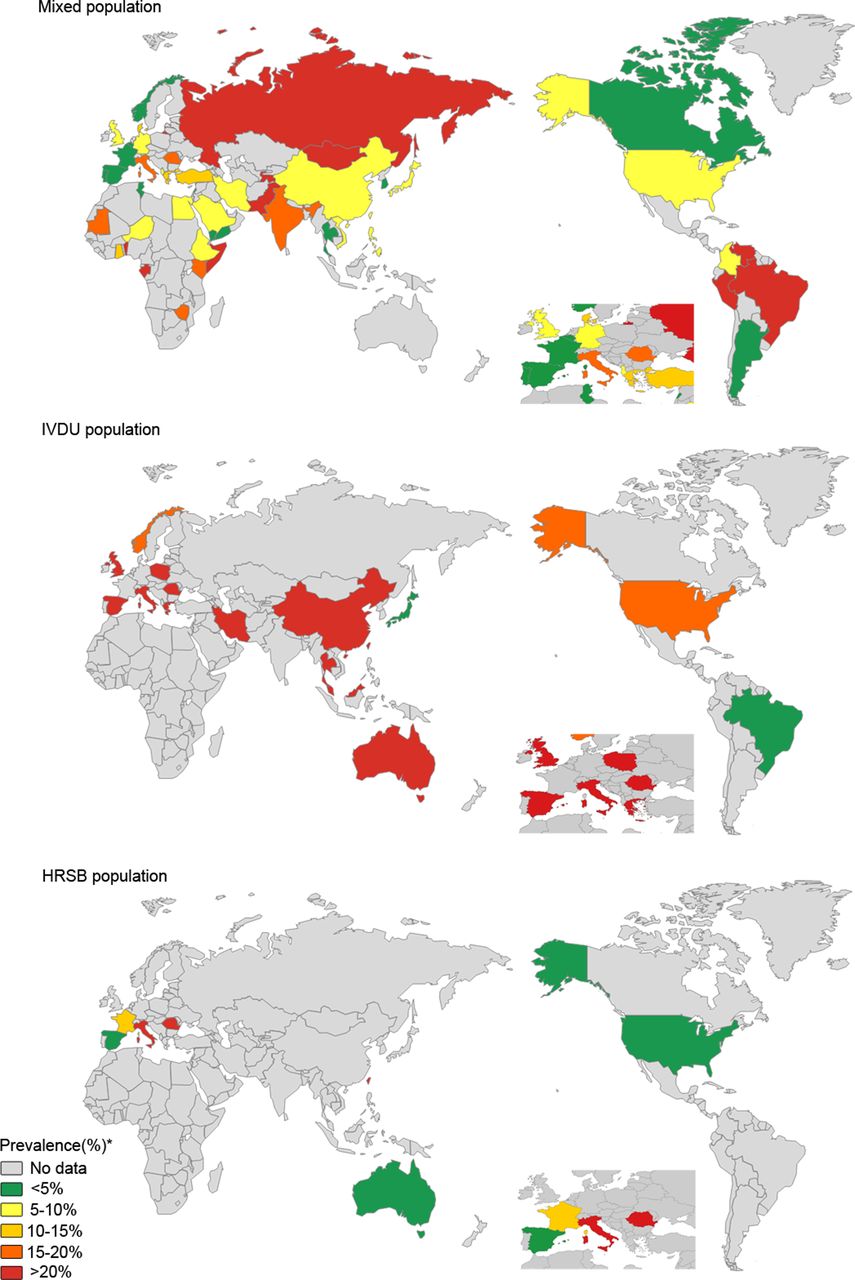
In HBsAg-positive population, HDV infection seroprevalence was from 0.00% to 83.33% in individuals without risk factors of IVDU and HRSB, whereas from 0.00% to 92.86% in the IVDU and 0.00% to 58.54% in people with HRSB (online supplementary appendix table S1). HDV seroprevalence was 10.58% in the mixed population (95% CI 9.14 to 12.11), 37.57% in IVDU only (95% CI 29.30 to 46.20) and 17.01% (95% CI 10.69 to 24.34) in HRSB only population (figure 3A). HDV seroprevalence was significantly associated with the risk factors of IVDU and HRSB (p=0.00) (figure 4). The meta-regression analysis showed that the seroprevalence substantially varied both in the IVDU and in mixed population (coefficient 1.182775 (95% CI 1.072281 to 1.30465); p=0.001). To identify whether gender is a risk factor, we analysed the 182 studies included in our article. The prevalence of HDV was 12.11% (95% CI 9.67 to 14.77) in male, 9.93% (95% CI 7.55 to 12.57) in female and 9.75 (95% CI 8.03 to 11.60) in studies with unknown gender. The overall prevalence of HDV in male is slightly higher than female (figure 3C).

Seroprevalence of hepatitis D virus among three HBsAg-positive populations. HRSB, high-risk sexual behaviour; IVDU, intravenous drug use.
Impact of HBV vaccination
We further divided the data into two groups based on the study population in 1977–2016: according to the year 1977–1996 (group A) and 1997–2016 (group B), considering the fact that the HBV vaccine was recommended to be included into the expanded programme of immunisation (EPI) for all countries since 1997.17 As expected, the prevalence of HDV infection in group B was lower than that in group A (online supplementary appendix figures S3 and S4). There was a definite association between the HBV vaccine coverage rate and the HDV prevalence (online supplementary appendix figure S5 and table S2). However, we found that the HDV seroprevalence showed an upward trend in Japan and Gabon (online supplementary appendix table S3). The number of the studies from these countries was limited. We only included one or two studies. So, the regional estimates from few studies might not be representative of the national estimates. The prevalence of HDV was extremely high among several other countries based on our estimates, such as Niger, Benin, Gabon, Mongolia, Australia, Kiribati, Marshall Islands, Nauru, Tuvalu (table 1). Most of these countries are in Africa and Oceania. However, it appears that the overall trend of the HDV prevalence has reached to a plateau in Africa (online supplementary appendix figure S3).
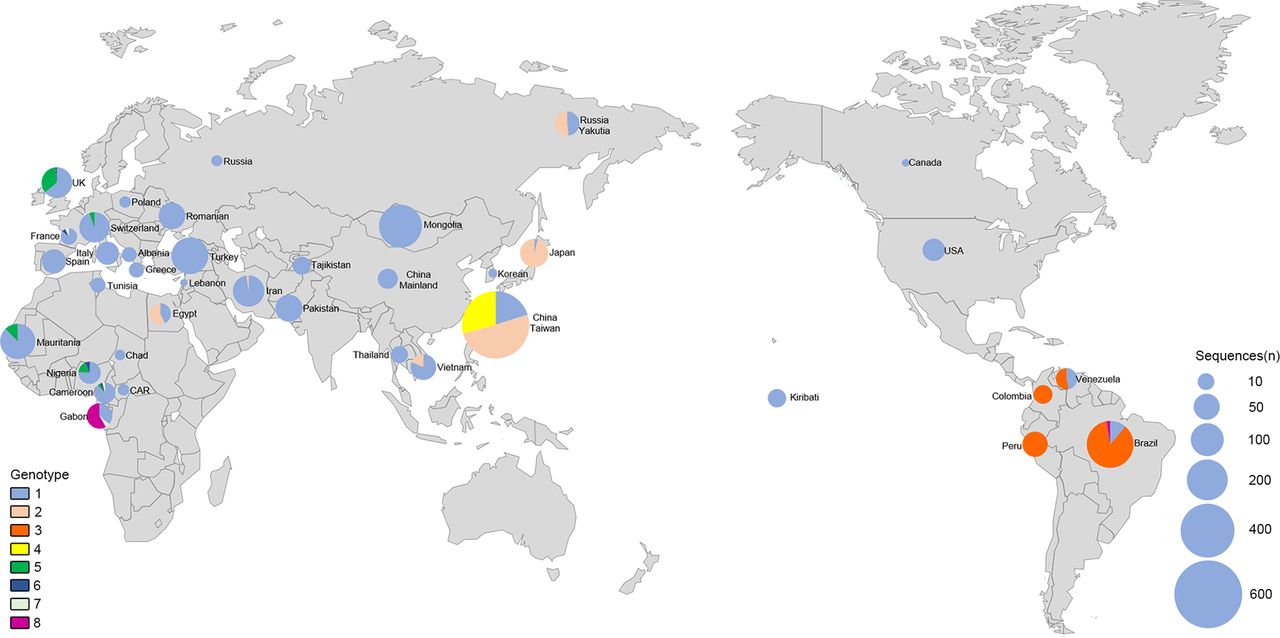
Distribution of HDV genotypes
HDV genotype 1 is still ubiquitous all over the world, whereas HDV genotype 2, which was previously confined to Asia (especially South-East Asia), has also emerged in Egypt18 and Iran.19 The geographical distributions of HDV genotype 3, genotype 4 and genotype 8 are still the same (figure 5 and online supplementary appendix table S5).20 HDV genotypes 5–7 have only been reported from Africa. However, in the last 5 years, genotypes 5 and 6 have also been found in the UK,21 genotypes 6 and 7 in France22 and genotype 5 in Switzerland.23
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Global distribution of hepatitis D virus genotypes. Each bubble represents a country or a region.
Association between SDI and HDV prevalence
HDV seroprevalence varied widely in general population among countries with different SDI levels. SDI is reported in quartiles and provides summary measure of region’s sociodemographic development and is based on three predictive indicators of health: average income per capita, education and fertility rate.24 HDV seroprevalence was 0.42% in high SDI countries (95% CI 0.08 to 0.93), 0.07% in high-middle SDI countries (95% CI 0.00 to 0.53) and 1.08% (95% CI 0.50 to 1.85) in the middle SDI countries, 1.85% in low-middle SDI countries (95% CI 0.80 to 3.26), 3.41% in low SDI countries (95% CI 0.85 to 7.36) (figure 3B and online supplementary appendix table S6). The highest HDV prevalence was in low SDI countries; on the contrary, the lowest prevalence was in high-middle SDI countries.
Sensitivity analysis
In a sensitivity analysis (online supplementary appendix table S7), exclusion of these studies did not affect estimates of the overall prevalence of HDV infection in the HBsAg-positive population.
Discussion
We conducted a systematic review and meta-analysis of the studies published on global HDV prevalence to identify the epidemiology and distribution of the HDV transmission. We found that the global prevalence of HDV is 0.98%, and approximately 10.58% of the global HBsAg carriers are also coinfected with HDV, which means the global burden of HDV infection is approximately 62–72 million individuals (table 2). We found that the HDV seroprevalence was highest in the HBsAg positive IVDU population, followed by HBsAg HRSB population and lowest in the mixed population without these two risk factors.
Our study substantiates the findings published by previous studies that the Africa, the Amazon Basin, the Eastern and Mediterranean Europe, the Middle East and the parts of Asia have highest rates of HDV carriage.4 The data from previous systemic reviews showed that about 5% of chronic HBV carriers worldwide are HDV coinfected;25 however, our result suggests that the prevalence of HDV among HBsAg carriers has climbed up to 10.58%.
WHO reckons that the IVDU are a key group which needs to be specifically targeted for HBV immunisation. Therefore, detailed data are needed for the population at risk, in order to target these people appropriately.26 Our study shows that the injecting illicit drugs is driving the HDV epidemic in HBsAg-positive individuals. We found that HBsAg-positive IVDU population has three times higher HDV seroprevalence than the population without any risk factors. The HDV seroprevalence rate was much higher in the HIV-infected IVDU than in HIV-uninfected IVDU,8 which indicates that the HIV coinfection might be a risk factor for HDV infection. High risk of HBV infection in IVDU could be related to the use and sharing of contaminated syringes.5 Thus, better implementation of preventive measures, such as the change to a disposable medical equipment, could lead to a lower prevalence of HDV.4
There is a paucity of studies about HDV prevalence in HRSB population worldwide, and these values vary across the globe. However, pooled overall seroprevalence in HRSB was still higher than that in patients without any risk factors. Comprehensive influence of multiple factors might lead to this consequence. The HRSB population in our study includes both heterosexual and homosexual population. In heterosexual group, intrafamilial spread in high endemic regions was once reported as a risk factor for HDV infection. This could partly explain the geographical distribution of HDV.5 Whereas the risk behaviour of homosexuals will raise the susceptibility of HCV infection,27 HCV coinfection and liver disease are said to be the additional risk factors for HDV infection.28 In our study, patients with liver disease had a higher prevalence than HBsAg carriers (online supplementary appendix figure S2).
The recent emergence of the HDV genotypes 5–7 in Europe could be a result of population migration from Africa to Europe.4 Immigrants contribute >50% of the HDV infection burden in both Greece and Germany.5 29 According to a 2001 population census in Greece, 7% of the local population consisted of immigrants, and the true extent might be even higher in consideration of illegal immigration. Most immigrants originate from high to low epidemic regions.4 29 Therefore, although HBV vaccination programme was recommended to be included in the EPI for all countries,17 HDV prevalence in European countries has ceased to decline and has even increased in some countries.4
Immigrant populations mostly originate in the countries with lower SDI. Our study found that the highest HDV prevalence was in low SDI countries. Locations with lower SDI always have a higher prevalence of HBV and have fewer improvements in socioeconomic conditions when compared with those with higher SDI overtime.4 HBV vaccination may be a cost-effective method to prevent viral hepatitis in lower SDI countries.17 Additionally, issues with use of unscreened blood products, unsafe medical procedures and restricted access to antiviral treatments still remain to be solved in poor-resourced countries.1 Studies have shown that the immigrant children have lower immunisation coverage and higher HBV prevalence than native ones, which implies immigrants may have limited access to medical care which is true especially for illegal immigrants.28 More attention is needed to be paid to global HBV vaccination programme, as our result showed that the decline in HDV infection is most likely due to the successful implementation of HBV vaccination programme. Studies suggest that maintaining infant HBV vaccination coverage above 80% and improving birth-dose vaccination coverage is an effective way of eradicating HBV and HDV infection.27 However, the global coverage of infants with birth dose vaccine remains very low and is estimated to be only about 38% in 2014.17
Although our global study of the prevalence of HDV infection is the largest so far, we mainly focused on published literature, and grey literature was not exhaustively included. Data on HDV prevalence was not available for many countries. Reported studies are few and limited by geographic distribution. We only had one regional study from a country in some instances. Therefore, slight variations in those studies can significantly modify the national data. Our estimates might not be representative of all countries included. Moreover, some studies on HDV prevalence did not meet the inclusion criteria for this analysis. As vaccination effects appear with a time lag,1 the line graph of the relationship between vaccination coverage rate and HDV prevalence may not reflect the true effect of vaccine and the correlation of which might be even stronger than this. The ascertainment of HBV infection is also likely to affect HDV estimates. In our study, the main criterion of HBV infection is HBsAg positive. However, in the typical course of HDV superinfection, markers of HBV infection are usually inhibited with IgM anti-HBc and HBV DNA typically testing negative.30 Moreover, the individuals who we included in the drug misusers group might have a different natural history of injecting drug use and have been exposed to additional risk factors. Because of the dearth of HDV country-level estimates in general population samples, we mainly focused on HDV prevalence among HBsAg-positive population. Thus, most of our results need to be adjusted by the prevalence of HBV.
Additionally, the serological tests might be less accurate in older studies. Enzyme immunoassay, which is thought to be less reliable, was routinely applied to the detection of HDV-antibodies. Considering the high genetic variability of HDV and the complex secondary structure of the target genomic RNA, eight HDV genotypes, and many subgenotypes have been defined with a wide divergence. Besides, many laboratories underestimated plasma HDV RNA viral load and even failed to detect HDV when compared with the French national reference laboratory for HDV (FNRL-HDV).31 Quantitative microarray antibody capture (Q-MAC) is a newly reported method, which can detect diverse HDV genotypes without limitation by using full-length recombinant HDV delta antigen.32
Our study showed that the global burden of HDV infection is not abated33 and has been underestimated. Moreover, the testing rates for HDV antibodies in the HBsAg-positive individuals are inappropriately low,29 34 which suggests a lack of awareness regarding the availability of a test for HDV in the Europe. The results of this study stress on the need for the international guidelines of HDV screening in HBsAg-positive individuals, especially in the IVDU and HRSB population. HBV vaccine has a defensive effect on the infection by HDV. Considering the lower HBV immunisation coverage in lower SDI countries, the implementation of HBV vaccination programme should also be pushed further in poor-resourced countries. All susceptible IVDUs should be given priority to HBV vaccine.
Acknowledgments
We are grateful to Manli Gu for excellent assistance and comments.
References
Footnotes
H-YC, D-TS and D-ZJ contributed equally.
Contributors All authors contributed to the draft and have seen and approved the final version of the report.
Funding This work was supported by the National Natural Science Foundation of China (81302531), Natural Science Foundation of Jiangsu Province of China (BK20131018), the Talents Planning of Six Summit Fields of Jiangsu Province (2013-WSN-037), Postgraduate Research & Practice Innovation Program of Jiangsu Province (KYCX17_1287), the National Key Clinical Department of Laboratory Medicine of China in Nanjing, Key laboratory for Laboratory Medicine of Jiangsu Province (ZDXKB2016005) and by the Priority Academic Program Development of Jiangsu Higher Education Institutions.
Disclaimer The funder of the study had no role in the study design, data collection, data analysis, data interpretation or writing of the manuscript. The corresponding author had full access to all the data in the study and has final responsibility for the decision to submit for publication.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.