Article Text

Abstract
Objectives In the management of patients with bleeding peptic ulcers, recurrent bleeding is associated with high mortality. We investigated if added angiographic embolisation after endoscopic haemostasis to high-risk ulcers could reduce recurrent bleeding.
Design After endoscopic haemostasis to their bleeding gastroduodenal ulcers, we randomised patients with at least one of these criteria (ulcers≥20 mm in size, spurting bleeding, hypotensive shock or haemoglobin<9 g/dL) to receive added angiographic embolisation or standard treatment. Our primary endpoint was recurrent bleeding within 30 days.
Results Between January 2010 and July 2014, 241 patients were randomised (added angiographic embolisation n=118, standard treatment n=123); 22 of 118 patients (18.6%) randomised to angiography did not receive embolisation. In an intention-to-treat analysis, 12 (10.2%) in the embolisation and 14 (11.4%) in the standard treatment group reached the primary endpoint (HR 1.14, 95% CI 0.53 to 2.46; p=0.745). The rate of reinterventions (13 vs 17; p=0.510) and deaths (3 vs 5, p=0.519) were similar. In a per-protocol analysis, 6 of 96 (6.2%) rebled after embolisation compared with 14 of 123 (11.4%) in the standard treatment group (HR 1.89, 95% CI 0.73 to 4.92; p=0.192). None of 96 patients died after embolisation compared with 5 (4.1%) deaths in the standard treatment group (p=0.108). In a posthoc analysis, embolisation reduced recurrent bleeding only in patients with ulcers≥15 mm in size (2 (4.5%) vs 12 (23.1%); p=0.027).
Conclusions After endoscopic haemostasis, added embolisation does not reduce recurrent bleeding.
Trial registration number NCT01142180.
- peptic ulcer bleeding
- angiographic treatment
- endoscopic treatment
- embolisation
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Endoscopic haemostatic treatment to patients with bleeding peptic ulcers reduces rate of further bleeding, the need for surgery and in pooled analyses of randomised trials overall mortality.
After endoscopic control to bleeding peptic ulcers, the current recommendation is to offer acid suppression which has also been shown to improve clinical outcomes.
A subgroup of patients, including those with initial hypotension and larger ulcers, are predicted to rebleed after endoscopic haemostatic treatment and acid suppression. Mortality in patients with further bleeding is substantially higher. The best strategy to forestall recurrent bleeding is unknown.
The role of supplementary angiographic embolisation in stable patients has not been defined.
What are the new findings?
Added angiographic embolisation after endoscopic haemostasis does not improve clinical outcomes in most high-risk patients with bleeding peptic ulcers.
In a posthoc analysis, patients with bleeding ulcers 15 mm in size or greater would benefit from added angiographic embolisation. The risk of recurrent bleeding is reduced by around fivefold.
How might it impact on clinical practice in the foreseeable future?
The results show that in patients with exigent bleeding from gastroduodenal ulcers 15 mm or greater, angiographic embolisation to the bleeding artery may be considered after initial haemostasis with endoscopic methods.
Introduction
Acute upper gastrointestinal bleeding (AUGIB) is one of the most common emergencies in gastroenterology. Despite major improvements in its management, AUGIB continues to be associated with significant morbidity and mortality. Bleeding peptic ulcers are one of the principal causes of AUGIB. Endoscopic therapy to bleeding ulcers reduces further bleeding and improves patients’ outcomes.1 The adjunctive use of a high-dose proton pump inhibitor (PPI) given intravenously renders gastric pH neutral and further reduces bleeding.2 However, a subgroup of patients rebleed after initial endoscopic control and acid suppression therapy. Mortality in patients with further bleeding increases by approximately threefold. The 2007 National United Kingdom audit reported a mortality rate of 30% mortality in patients who needed surgery because of refractory bleeding.3
We, and others, have identified predictive risk factors to recurrent bleeding and adverse outcomes in patients who received endoscopic haemostatic treatment and acid suppression therapy.4–7 These factors include old age, shock on presentation, larger ulcers and low haemoglobin level on admission. To date, the optimal strategy to prevent further bleeding is unclear. Angiographic embolisation is a minimally invasive technique in the treatment of refractory bleeding from peptic ulcers.8 9 We hypothesised that angiographic embolisation in selected patients with high-risk ulcers reduces recurrent bleeding and improves their outcomes. There have been one published randomised controlled trial10 and several retrospective series with or without a comparative group on the subject of prophylactic angiographic embolisation after endoscopic hemostasis to bleeding peptic ulcers.11 12 Due to their study design and small sample size, the role of prophylactic angiographic embolisation has yet to be established.
Methods
Study design
The study was a multicentre randomised controlled trial between January 2010 and July 2014 conducted at four university hospitals. These were the Prince of Wales Hospital in Hong Kong, King Chulalongkorn Memorial University Hospital in Thailand, Erasmus MC University Medical Centre in the Netherlands and Xijing Hospital in China. The study was conducted in compliance with ICH-GCP guidelines. Institutional ethics review boards to individual centre approved the study protocol.
We performed endoscopic treatment in the form of haemoclipping or thermocoagulation with or without preinjection with diluted epinephrine to patients with bleeding gastroduodenal ulcer. We screened consecutive patients who required endoscopic haemostatic treatment to their bleeding peptic ulcers at respective endoscopy centres. These were patients with actively bleeding gastroduodenal ulcers (Forrest type I) or ulcers with non-bleeding visible vessels (Forrest IIa) treated by either haemoclipping or contact thermos-coagulation with or without preinjection with diluted epinephrine. Treatment endpoints were cessation of bleeding, flattening of the bleeding vessel follow thermos-coagulation. With the use of haemoclips, the prongs of the clips were placed directly on either side of the vessel. After endoscopic haemostasis, patients were invited to participate in the trial if one or more of the following criteria were met. These were: (1) spurting haemorrhage during endoscopy; (2) ulcers 20 mm in size or larger; (3) haemoglobin on admission of <9 g/dL; (4) signs of haemorrhagic shock before or during endoscopy defined by systolic pressure of <90 mm Hg and pulse rate of >110 beats per minute. We excluded pregnant or lactating patients, those aged less than 18, patients moribund from terminal malignant diseases or other end-stage illnesses with a limited life expectancy and those with known allergy to intravenous contrast. We did not include patients with a serum creatinine of 300 µmol/L or more with the concern of contrast nephropathy.
A biostatistician generated a randomisation sequence using a computing software. Sealed envelopes in blocks of 50 containing equal assignments were used. After obtaining a written informed from an eligible patient, a research nurse independent of the trial then opened the next numbered sealed envelope with assigned treatment. Patients received either added angiographic embolisation or standard treatment. Due to the nature of intervention, patients, clinicians and study team could not be blinded to treatment allocation.
Patients randomised to receive added angiographic embolisation received the procedure as soon as possible and within 12 hours after endoscopic therapy. In patients on warfarin, the international normalisation ratio was corrected to around 1.5. The procedure was performed in the angiographic suite and under local anaesthetics to the patient’s groin. The celiac and then gastroduodenal artery or the left gastric artery was selectively cannulated depending on ulcer location. To patients in both groups, the bleeding point had previously been marked applying haemoclips during endoscopy. We used a ‘sandwich’ technique using dual embolic agents. Coils were deposited distal to the bleeding point. Gel foam particles were then packed into the artery and its collaterals. This was followed by further coils deposited in its proximal portion until complete cessation of arterial flow. Our protocol requested empiric embolisation of the artery even in the absence of active contrast extravasation or a pseudoaneurysm.
Patients in both groups received a bolus intravenous injection of PPI 80 mg followed by an infusion of 8 mg per hour for 3 days. Helicobacter pylori eradication therapy was started on day 4 after randomisation. In patients on aspirin or warfarin, these drugs were restarted on day 4.
Outcomes
Our primary outcome endpoint was recurrent clinical bleeding defined by fresh haematemesis, melena or haematochezia and/or signs of hypovolaemic shock (systolic blood pressure of <90 mm Hg and pulse rate >110 per min) or a drop in haemoglobin of >2 g/dL per 24 hours despite transfusion to around 8 g/dL. When a patient was judged to be rebleeding as defined, he would undergo an immediate endoscopic examination. A clinical rebleed was confirmed if endoscopy found fresh blood in stomach or active bleeding from a previously seen ulcer.
We followed patients for 30 days after randomisation. We contacted those by phone on day 30 if they were discharged earlier. Secondary outcome endpoints included: (1) further interventions: endoscopic treatment, embolisation or surgery; (2) transfusion requirements; (3) hospital stay including intensive care unit stay; (4) 30-day and in-hospital mortality.
Statistical analysis
From our earlier predictive model,3 patients judged at ‘high risk’ of recurrent bleeding (ie, who fulfilled one or more of the above criteria) had a risk of at least 16.7%. We assumed that early angiographic embolisation would decrease the rate of further bleeding from 16% to 4%. A minimum of 125 patients would be required in each group (type 1 error of 5%, 2-sided and a power of 80%) with an attrition rate of 10%.
Primary and secondary outcomes were analysed in both the intention-to-treat (ITT) and per-protocol populations (PPA). The ITT population included all patients who met inclusion criteria and randomised. The per-protocol population included patients who received angiographic embolisation. Summaries of continuous variables are presented as mean (SD) for normally distributed data and as medians with IQRs for skewed data. We used a time to event analysis to compare the proportions of patients with primary outcomes in the two groups. We calculated estimates of recurrent bleeding using the Kaplan-Meier method and compared treatment groups using the log-rank test. Additionally, we used a Cox proportional hazard model to evaluate association of treatment with outcomes (recurrent bleeding and deaths). In cases where the standard Cox regression model failed to produce estimates due to convergence problems because of zero-cell counts, we used an exact logistic regression method to approximate the significance of the treatment effect. For secondary categorical variables, we used a logistic regression model and obtained ORs and their corresponding 95% CI . For continuous variables, the effect of treatment group was analysed using the Mann-Whitney test.
In posthoc analyses, we also explored the treatment effects in different subgroups estimating the HR with 95% CI and performing tests for interaction with treatment arms. The subgroups included age, sex, presence of absence of shock (systolic blood pressure 90 mm Hg or less), ulcer size and location. We used IBM SPSS Statistics V.22 (IBM, Armonk, New York, USA) for statistical analysis. All tests were two-sided, and a p value of less than 0.05 was considered to indicate statistical significance.
Results
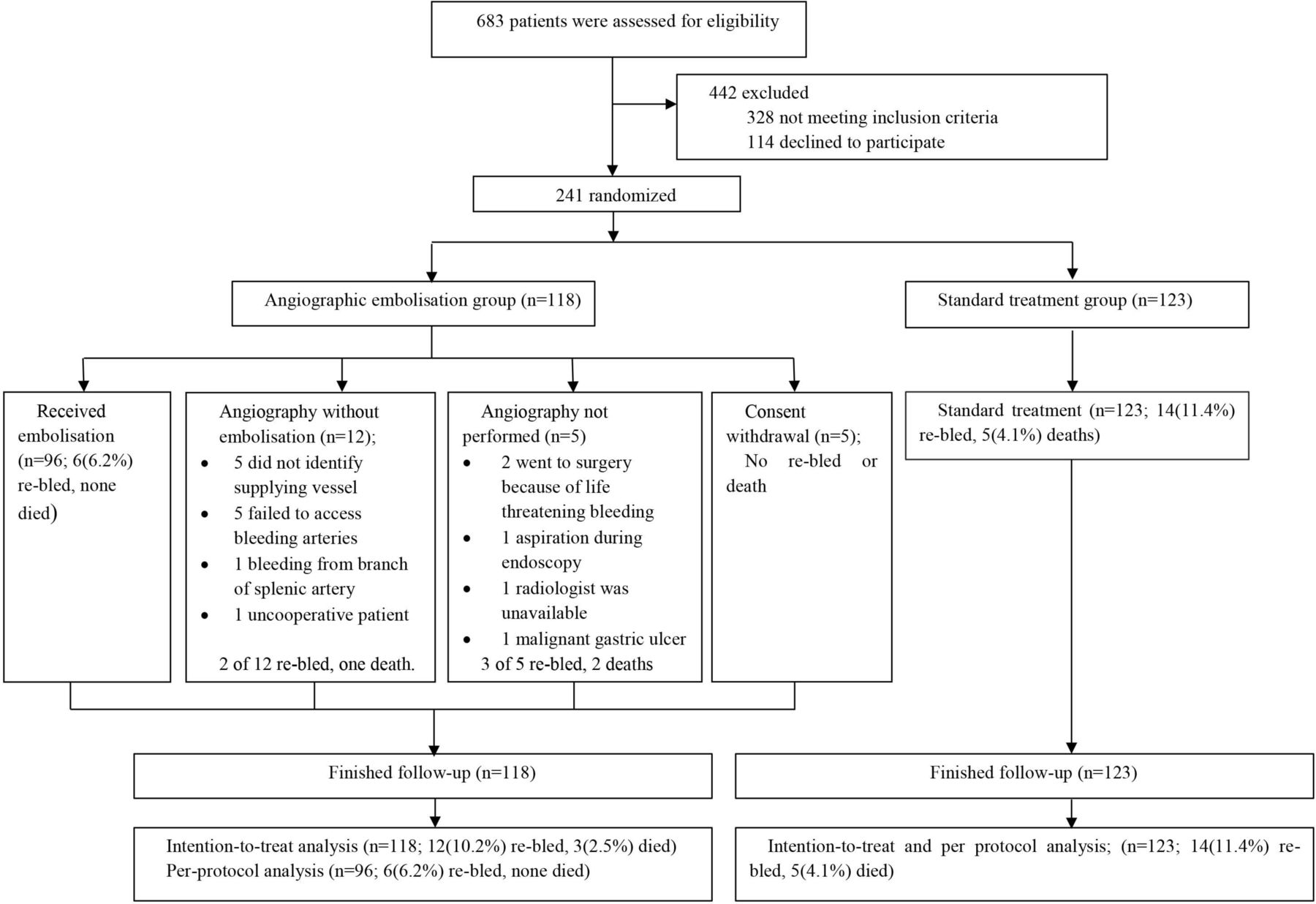
A total of 683 patients were screened between January 2010 and July 2014 at four institutions, of whom 241 patients were enrolled (118 patients were assigned to embolisation group and 123 patients to standard treatment group) (figure 1). Follow-up was complete in all patients from both groups. The baseline characteristics, severity of bleeding, history of ulcer disease and endoscopic treatment received prior to randomisation to either group of patients are listed in table 1.

Study flow diagram.
Baseline characteristics of participants
Of 118 patients randomised to receive added embolisation, 22 (18.6%) did not undergo embolisation. Of them, 12 underwent angiography but without embolisation because of the following reasons; bleeding point could not be delineated (n=5), failed angiographic access to the artery (n=5), bleeding from a branch of splenic artery and concern of splenic infarct following embolisation (n=1), one patient became uncooperative because of confusion (n=1). Five patients did not undergo angiography due to exigent bleeding (n=2), a malignant ulcer (n=1), aspiration during endoscopy (n=1) and unavailability of a radiologist (n=1). Five patients withdrew consents prior to angiography.
Ninety-six patients received embolisation. The mean time to angiography was 4.3 hours (SD 3.6 hours). During angiography, active bleeding was seen in 5 of 96 patients (5.2%). There were three pseudoaneurysms (3.1%). Arteries embolised were the gastroduodenal artery (n=63), left gastric artery (n=18), right gastric artery (n=11) and unnamed arteries (n=4). No ischaemic or local complication occurred after these procedures. None of the patients required renal replacement therapy after angiography.
In an ITT analysis, 12 of 118 (10.2 %) in the embolisation and 14 of 123 (11.4%) in the standard treatment group developed recurrent bleeding within 30 days (HR 1.14, 95% CI 0.53 to 2.36; p=0.75) (table 2). In the embolisation group, 6 of 12 rebleeding patients belonged to the subgroup of patients (n=22) who did not receive embolisation; 2 underwent surgery because of further bleeding and severe hypotension while awaiting angiography. Two received further endoscopic haemostatic treatment. One patient underwent angiography without embolisation. She rebled and received a second angiography and embolisation to her gastroduodenal artery. She rebled again and underwent emergency surgery. One patient rebled in the ward on day 3 and died before intervention was possible. The other six rebleeding patients after embolisation received successful endoscopic re-treatment. In the standard treatment group, 14 patients developed recurrent bleeding which was controlled by endoscopic retreatment in nine patients, angiographic embolisation in four patients and surgery in one patient.
Clinical outcomes within 30 days of endoscopic therapy
In the PPA, 6 of 96 (6.2%) and 14 of 123 (11.4%) from embolisation and standard treatment groups, respectively, reached primary endpoint (HR 1.89, 95% CI 0.73 to 4.92; p=0.192) (figure 2).
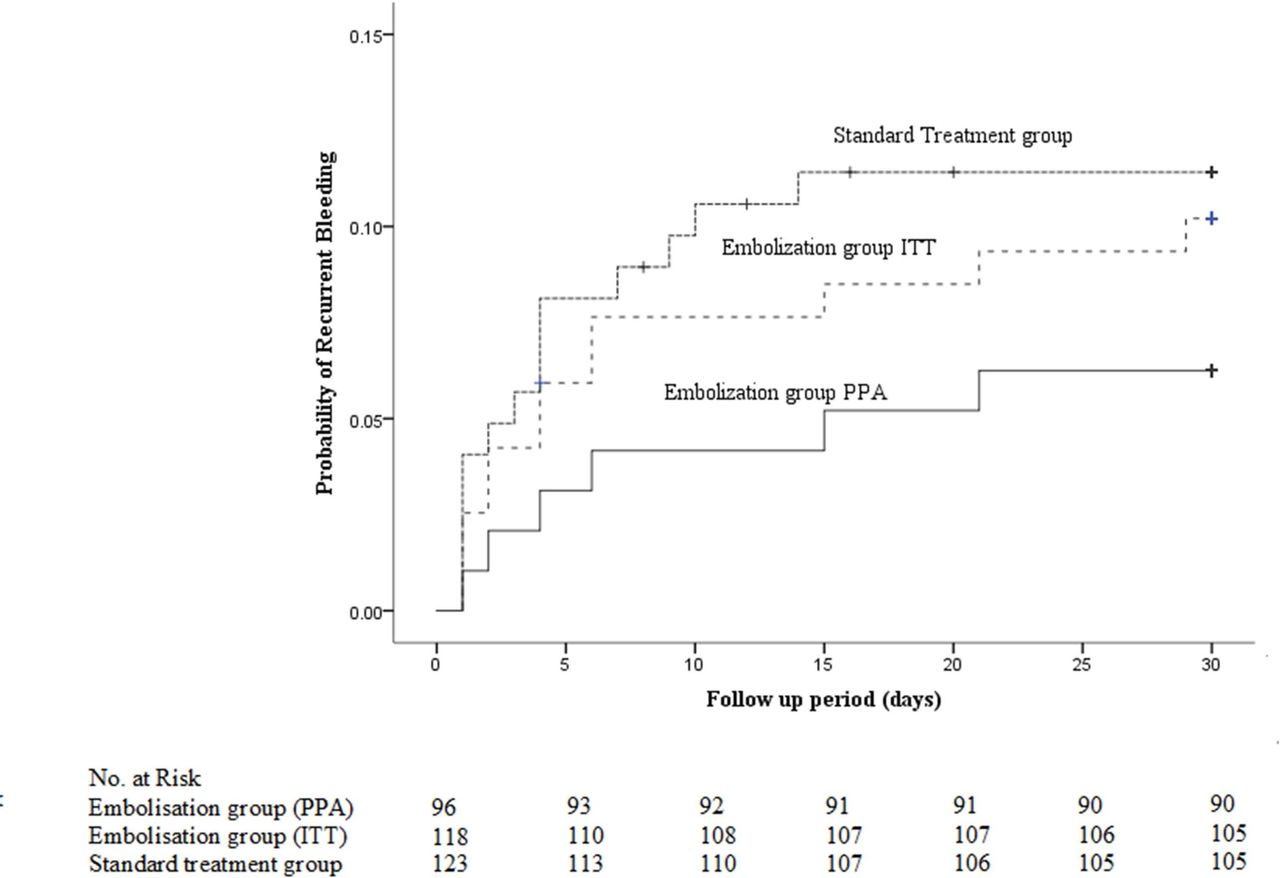
Probability of recurrent ulcer bleeding in both ITT and PPA (ITT, p=0.743; PPA, p=0.182). ITT, intention-to-treat; PPA, per-protocol analysis.
Fewer patients required blood transfusion in the embolisation group in both ITT and per-protocol analyses (55 vs 73, p=0.048 and 44 vs 73, p=0.047, respectively). The median units of blood transfused were also significantly less on either analysis (p=0.048 in ITT analysis and p=0.027 in PPA, respectively). There was, however, no significant difference in ICU and hospital stay between the two groups.
There were three (2.5%) deaths in the embolisation group within 30 days of randomisation, compared with five (4.1%) in the standard treatment arm (HR 1.6, 95% CI 0.38 to 6.7; p=0.519). In the embolisation group, all of the three deaths did not receive intended embolisation. An 84-year-old woman died after surgery complicated by pyloroplasty dehiscence and abdominal sepsis. A 60-year-old man died after major bleeding on the ward. The last patient with atrial fibrillation and heart failure died without signs of recurrent bleeding. In this group, one additional patient died on day 37 from peritonitis after surgery. Similar to the other three patients, she did not receive embolisation per randomisation and rebled. In the standard treatment group, the causes of death were nosocomial sepsis (n=3), acute ischaemic stroke (n=1) and congestive heart failure (n=1). None of the 96 patients who had received added angiographic embolisation died within 30 days.
In a posthoc analysis among patients in the per-protocol population, we explored treatment effects in subgroups and performed tests of interaction. When we divided ulcers into different size categories, in those with ulcers 15 mm or greater in size, 2 of 44 (4.5%) rebled after embolisation compared with 12 of 52 (23.1%) in the standard treatment group (HR 5.43; 95% CI 1.22 to 24.3; p=0.027) (figure 3). The same was observed in patients with ulcers 20 mm in size or greater, embolisation led to a reduced rate of rebleeds (2 of 38, 5.2% vs 9 of 39, 23%; HR (95% CI), 4.76 (1.03 to 22.04)). The p value for interaction was significant only when we divided ulcers with the cut-off of 15 mm (pinteraction=0.018) (figure 4). In ulcers<15 mm in size, rate of further bleeding was not different between groups (4 (7.5%) vs 2 (2.8%); HR 0.37, 95% CI 0.07 to 2.00; p=0.254).

Probability of recurrent ulcer bleeding in patients with ulcers less than 15 mm in size and 15 mm or larger. In patients with ulcers less than 15 mm in size, angiographic embolisation did not reduce recurrent bleeding (4 in 52 (7.7%) in the embolisation group vs 2 in 71 (2.8%) in the standard treatment group; HR 0.37, 95% CI 0.07 to 2.03; p=0.254). In patients with ulcers 15 mm or larger, angiographic embolisation reduced recurrent bleeding (12 in 52 (23.1%) vs 2 in 44 (4.5%); HR 5.43, 95% CI 1.22 to 24.29; p=0.027).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of recurrent bleeding by randomised group with subgroups analyses for ulcer size and other factors. Angiographic embolisation was more effective in reducing recurrent bleeding in ulcers 15 mm in size or larger (HR 5.56, 95% CI 1.24 to 24.87; p interaction=0.018).
Furthermore, in patients with shock prior endoscopy, embolisation also reduced rate of rebleeds (none of 13 rebled after embolisation compared with 7 of 19). The p interaction was 0.07.
Discussion
In this clinical trial, we have not shown a clear benefit adding angiographic embolisation to endoscopic haemostasis in patients with bleeding gastroduodenal ulcers. Nearly one-fifth of the patients randomised to receive embolisation did not receive the treatment. Half of the rebleeding and all of the deaths occurred in this subgroup of patients. In an ITT analysis, we were unable to show any difference in the rate of recurrent bleeding between groups. In our PPA, we, however, observed a trend in reduced recurrent bleeding and death after adding embolisation. It remains possible that with a larger sample size, we will detect a significant difference in favour of added embolisation. An alternate explanation to a negative trial is because our inclusion criteria were not sufficiently precise in identifying those likely to benefit from embolisation.
Other groups have studied the concept of prophylactic angiographic embolisation. Laursen et al reported a randomised controlled trial that enrolled 105 patients.10 The study enrolled patients with Forrest I a or I b bleeding and with a Rockall score of 5 or above. Thirty-one of 49 patients in the angiography group received embolisation. With an ITT analysis, recurrent bleeding occurred in 2 (1 did not receive embolisation) of 49 patients in the embolisation group compared with 8 of 56 patients in the standard treatment group (p=0.10). The authors used a composite outcome endpoint based on mortality, severity of rebleeding and blood transfusion and observed a trend in the reduction of rebleeding with supplementary angiographic embolisation. In a retrospective series of 70 patients with high-risk bleeding duodenal ulcers who received added embolisation, the rate of further bleeding was 11%.11 Kaminskis et al reported a retrospective comparison between patients with (n=25) or without embolisation (n=50). The rate of surgery was higher in those without embolisation (8% vs 35%, p=0.012).12 Similar to our study, the sample size of these studies did not allow a firm conclusion to be made on the role of prophylactic embolisation.
In an ancillary analysis, we observed that added angiographic embolisation significantly reduced recurrent bleeding in ulcers 15 mm in size or greater. We found significant reductions in either the cut-offs of 15 mm or 20 mm. The number needed to treat to prevent one recurrent bleeding in the subgroup of 15 mm or more is only five. Larger gastroduodenal ulcers often erode into subserosal arteries that belong to either the gastroduodenal or left gastric artery complexes in the duodenal bulb or the lesser curvature of the stomach, respectively. We unfortunately did not find a significant interaction between ulcer location and effect of angiographic embolisation. As these are posthoc observations, we should consider these hypothesis generating worthy of further confirmation.
Size of bleeding arteries is likely a critical determinant to further bleeding. Swain et al studied 27 gastrectomy specimens in patients who needed surgical control to their bleeding ulcers and found that the mean artery size was 0.7 mm (range 0.1–1.8 mm).13 About half of these arteries were subserosal and showed aneurysmal dilation. In an abstract, Lai and Swain reported postmortem findings of patients after fatal bleeding from their peptic ulcers. The mean diameter of the arteries was 3.45 mm.14 In a canine mesenteric artery model, Johnston et al showed that haemostasis by contact thermal coagulation became inconsistent among arteries beyond 2 mm in diameter.15 In large gastroduodenal ulcers with a sizeable vessel or a protuberance, it seems logical to offer angiographic embolisation. Unfortunately, a visible vessel represents a sentinel clot or a thrombus in the artery. We have currently no reliable endoscopic method of measuring size of the bleeding artery. Recently Jensen et al published a randomised trial to compare endoscopic treatment guided by either the use of a Doppler probe or endoscopic stigmata of bleeding in 148 patients. The authors found Doppler signal guided treatment led to reduced rate of rebleeding from 26.3% to 11.1% (p=0.02).16 With high-resolution endoscopic ultrasonography, Levy et al reported EUS guided injection therapy of arteries to mixed lesions with refractory bleeding.17 These included Dieulafoy vascular lesions and a pancreatic pseudoaneurysm. Endoscopic angiotherapy is an evolving treatment for refractory bleeding GI lesions. At present, percutaneous angiography remains the only reliable means to image and characterise a bleeding artery.
These are other strategies in the prevention of rebleeds. In Europe and other countries, endoscopists perform routine second look endoscopy with a view to re-treat residual bleeding stigmata. In a meta-analysis of four published studies and four abstracts on routine second look endoscopy, El Ouali et al 18 found a modest reduction in rebleeding with the use of second look endoscopy (84 of 703, 11.9% vs 125 of 698, 17.9%). The number needed to treat to prevent one rebleed was 17. Most of these clinical trials were performed two decades ago. The clinical and endoscopic practices were considered not contemporary. In a recent randomised controlled trial of 319 patients from Korea, routine second look endoscopy when compared with standard care did not reduce rebleeding. It is more logical to select highest risk patients for second look endoscopy.
In a multicentre randomised controlled trial,19 Schmidt et al compared the use of over-the-scope-clips (OTSC) to standard treatments mostly through the scope clips in the endoscopic treatment of ulcers with refractory bleeding. OTSCs were much more superior in the control of bleeding (15 of 26 vs 30 of 33, p=0.005). The addition of an OTSC may prove to be a useful strategy to forestall rebleeds in high-risk patients.
In conclusion, added angiographic embolisation after endoscopic haemostasis has not been shown to improve outcomes in most patients. In a subgroup of patients with larger ulcers, especially in those with shock, angiographic embolisation may be considered to forestall recurrent bleeding. These findings help to refine our selection of patients for angiographic embolisation. The benefit of angiographic embolisation, however, requires confirmation in a further clinical trial.
References
Footnotes
Contributors JYWL has full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. JYWL and RP are both first authors. Concept and design: JYWL, RP, K-TW, NP, PWYC, RR, ILH, EJK, K-CW, KWLA, FKLC, JJYS. Acquisition, analysis or interpretation of data: JYWL, RP, K-TW, NP, PWYC, RR, ILH, EJK, K-CW, KWLA, FKLC, JJYS. Drafting of the manuscript: JYWL. Critical revision of the manuscript for important intellectual content: JYWL, RP, K-TW, NP, PWYC, RR, ILH, EJK, K-CW, KWLA, FKLC, JJYS. Statistical analysis: KWLA. Obtained funding: JYWL. Administrative technical or material support: JYWL, RP, K-TW, NP, PWYC, RR, ILH, EJK, K-CW, KWLA, FKLC, JJYS. Study supervision: JYWL, RP, ILH, K-CW.
Funding Hong Kong SAR Government Research Grant.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The New Territories East Cluster Hospitals Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.