Article Text

Abstract
Objective We evaluated the influence of the renin–angiotensin system (RAS) on intestinal inflammation and fibrosis.
Design Cultured human colonic myofibroblast proliferation and collagen secretion were assessed following treatment with angiotensin (Ang) II and Ang (1–7), their receptor antagonists candesartan and A779, and the ACE inhibitor captopril. Circulating and intestinal RAS components were evaluated in patients with and without IBD. Disease outcomes in patients with IBD treated with ACE inhibitors and angiotensin receptor blockers (ARBs) were assessed in retrospective studies.
Results Human colonic myofibroblast proliferation was reduced by Ang (1–7) in a dose-dependent manner (p<0.05). Ang II marginally but not significantly increased proliferation, an effect reversed by candesartan (p<0.001). Colonic myofibroblast collagen secretion was reduced by Ang (1–7) (p<0.05) and captopril (p<0.001), and was increased by Ang II (p<0.001). Patients with IBD had higher circulating renin (mean 25.4 vs 18.6 mIU/L, p=0.026) and ACE2:ACE ratio (mean 0.92 vs 0.69, p=0.015) than controls without IBD. RAS gene transcripts and peptides were identified in healthy and diseased bowels. Colonic mucosal Masson’s trichrome staining correlated with Ang II (r=0.346, p=0.010) and inversely with ACE2 activity (r=−0.373, p=0.006). Patients with IBD who required surgery (1/37 vs 12/75, p=0.034) and hospitalisation (0/34 vs 8/68, p=0.049) over 2 years were less often treated with ACE inhibitors and ARBs than patients not requiring surgery or hospitalisation.
Conclusions The RAS mediates fibrosis in human cell cultures, is expressed in the intestine and perturbed in intestinal inflammation, and agents targeting this system are associated with improved disease outcomes.
- Renin-angiotensin system
- inflammatory bowel disease
- fibrosis
- myofibroblasts
- angiotensin (1-7)
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Treatment of intestinal fibrosis in IBD remains a significant unmet need. The renin–angiotensin system (RAS) has been demonstrated to influence inflammation and fibrosis in other organs, and evidence to date supports these functions in murine models of IBD.
What are the new findings?
This study characterised components of the classical and alternative pathways of the RAS in the human intestine in patients with and without IBD and are altered in inflammation and fibrosis. We demonstrated that the key RAS effector peptides, angiotensin II and Ang (1–7), influence colonic myofibroblast proliferation and collagen secretion, and the use of angiotensin receptor blockers and ACE inhibitors was associated withm improved disease outcomes in patients with IBD.
How might it impact on clinical practice in the foreseeable future?
Interventional studies targeting the RAS in patients with IBD may provide a novel strategy for addressing intestinal inflammation and fibrosis.
Introduction
Despite expanding therapeutic options, the availability of cost-effective adjunctive antifibrotic therapies represents one of the greatest unmet needs in the management of patients with IBD, especially Crohn’s disease (CD).1 2
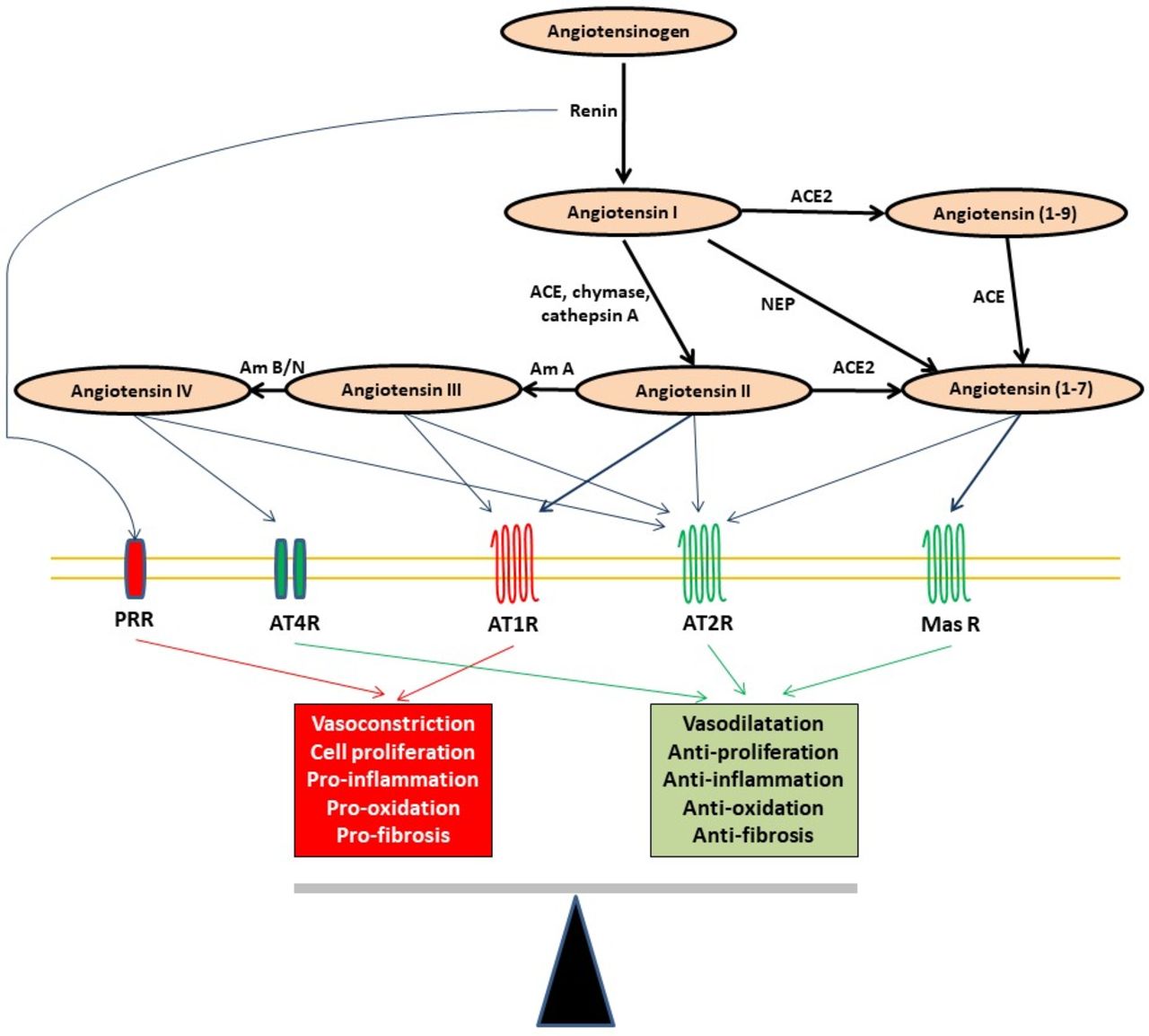
The role of the renin–angiotensin system (RAS) in cardiovascular and renal physiology and disease is well established, with important influences on vessel tone, inflammation and fibrosis (figure 1). Recent developments in understanding the RAS have revealed two complimentary pathways (classical and alternative) that mediate opposing effects on inflammation, fibrosis and cell proliferation. It is the balance of signalling from these pathways that determines tissue homeostasis (figure 1).3 While the function of these two pathways has been explored extensively in cardiovascular and renal disease, their role in GI disease is less clear. Manipulating the RAS is an attractive option as it offers inexpensive and safe therapies already in widespread use.
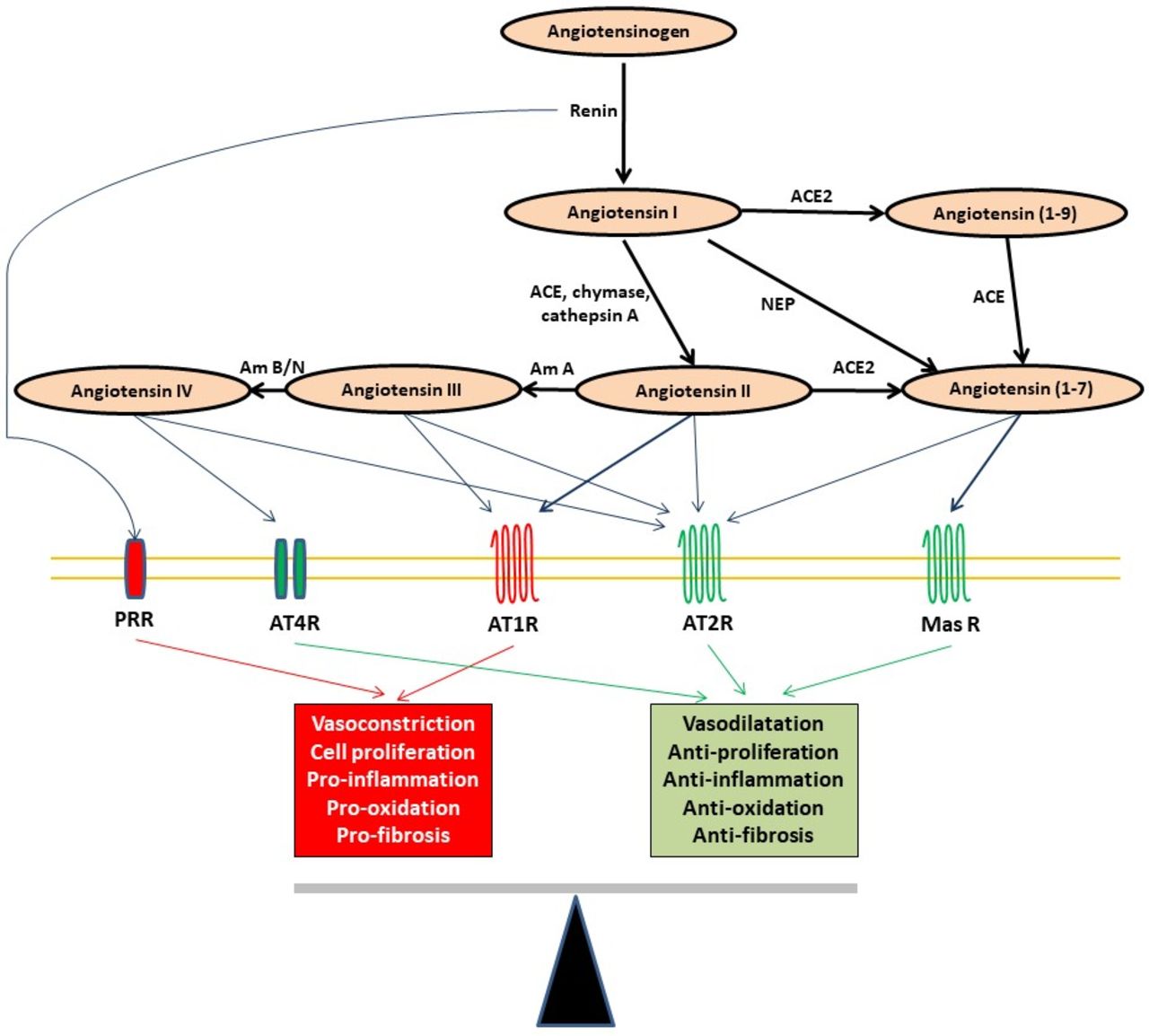
The contemporary RAS. The balance between the classical pathway, predominantly mediated via the AT1 receptor, and the alternative pathway, mainly mediated via the Mas receptor, determines the final homeostatic effect of the RAS. Am, aminopeptidase; AT1R, angiotensin type 1 receptor; AT2R, angiotensin type 2 receptor; AT4R, angiotensin type 4 receptor; NEP, neutral endopeptidase; PRR, (pro)renin receptor; RAS, renin–angiotensin system.
Components of the RAS in the human GI tract are not well characterised, especially in patients with IBD. The key enzymes of the RAS (ACE and ACE2) are expressed in high concentrations in the small bowel and the colon.3–5 Mucosal levels of angiotensin (Ang) I and II are elevated in rectosigmoid biopsies from patients with Crohn’s colitis compared with patients with UC or controls without IBD.6 We have previously shown that patients with IBD have higher circulating alternative RAS components than patients without IBD.7 Patients with IBD treated with angiotensin receptor blockers (ARBs) have lower mucosal proinflammatory cytokines than patients not treated with ARBs.8 Targeting the RAS has been beneficial in multiple animal models of colitis.9–15 However, key components of the alternative RAS axis, namely, ACE2, Ang (1–7) and its receptor, Mas, have not been studied in the human bowel.
We report the effects of the RAS peptides, Ang II and Ang (1–7), on proliferation and collagen secretion from cultured colonic myofibroblasts. It was hypothesised that Ang II would increase and Ang (1–7) would decrease myofibroblast proliferation and collagen secretion, via their respective receptors AT2R and Mas. Components of the classical and alternative axes of the RAS were characterised in the circulation and intestinal wall of patients with and without IBD, with the hypotheses that all components can be produced within the GI tract, and therefore exhibit the potential for local action and regulation, as well as be perturbed in intestinal inflammation and fibrosis. Subsequently, using a retrospective cohort and case–control studies, we assessed the effects of ACE inhibition or Ang receptor antagonists on disease activity, hospitalisation and surgery in patients with IBD. It was hypothesised that these agents would be associated with improved disease outcomes.
Methods
Detailed methods for all studies are outlined in the Supplementary materials.
Cell culture studies
Myofibroblasts were cultured and isolated from a segment of normal human colonic tissue harvested at surgery. Proliferation studies were performed following stimulation of isolated myofibroblasts with human recombinant platelet-derived growth factor (PDGF)-BB, then treated with RAS peptides and drug interventions, using CellTiter 96 cell proliferation assay (Promega, Madison, WI, USA). Collagen secretion studies were performed following stimulation with transforming growth factor (TGF)-β1 using Sircol collagen assay kit (Biocolor, Belfast, UK).
Cross-sectional human circulating and intestinal RAS studies
Subjects
Patients with IBD and controls without IBD undergoing colonoscopy or surgery were recruited from consecutive patients attending hospital outpatient clinics, with additional control volunteers without IBD from staff at Eastern Health and Monash University for circulating markers. Ileal and colonic resection specimens from controls without IBD were those undergoing surgery for either colorectal cancer or diverticular disease. Information regarding GI symptoms, comorbid illnesses, medications, cardiovascular indices (blood pressure and heart rate) and anthropological features (height, weight and waist circumference), and peripheral blood were collected during a formal patient interview.
Analytical assays
Serum ACE was measured using the Buhlmann ACE kinetic assay (Bühlmann Laboratories, Schonenbüch, Switzerland) using a Roche Cobas instrument. Plasma renin concentration was measured by the LIAISON Direct Renin Chemiluminescence Immunoassay (C). Plasma aldosterone was calculated using the LIAISON Aldosterone Chemiluminescence Immunoassay (DiaSorin, Saluggia, Italy).
Plasma ACE2 activity was measured on enzyme inhibitor mix-added plasma (online supplementary table 1) using a quenched fluorescent substrate-based assay (QFS:(7-methoxy-coumarin-4-yl) acetyl-Ala-Pro-Lys-(2,4-dinitrophenyl)-OH; Auspep, Parkville, Australia), as described previously.16 17
Supplemental material
Patients undergoing intestinal resection and colonoscopy
A 2×1 cm full-thickness segment was removed intraoperatively during intestinal resection with a sterile scalpel blade under aseptic conditions from the terminal ileum, ascending and/or sigmoid colon where appropriate.
Colonoscopic biopsies were obtained using standard forceps from the ileum, the ascending and sigmoid colons, and any other inflamed areas up to a maximum of two regions.
PCR analyses
RNA extraction was performed using the RNeasy Plus Universal Mini Kit (Qiagen, Melbourne, Australia) following tissue disruption and homogenisation, with reverse transcription of all RNA samples performed using the SuperScript III First-Strand Synthesis Supermix for quantitative reverse transcription (qRT)-PCR (Invitrogen, Mount Waverley, Australia). Probes and primers were designed using the Primer Express V.3 software programme (Applied Biosystems, Foster City, CA, USA) (online supplementary table 2). Multiplex qRT-PCR reactions were run and analysed in duplicate with eukaryotic 18S ribosomal-VIC the endogenous reference gene. The median of the terminal ileal non-IBD control tissue threshold cycle (Ct) was then determined, and subtracted from all values to obtain the DDCt. The expression of the target genes relative to non-IBD control terminal ileal tissue was evaluated using fold induction calculated as 2−(DDCt).
Immunohistochemistry
Immunohistochemistry was performed on 3 µm sections of paraffin-embedded colonoscopic biopsies and resection specimens using primary antibodies as listed in online supplementary table 3. Aperio Scanscope AT Turbo (Leica Biosystems, Mount Waverley, Australia) photographed slides were semiquantitatively analysed using Image J v1.47 (NIH, USA) and qualitatively analysed for localisation of specific antibodies. Two experienced GI histopathologists (PH and SM) independently graded colonic biopsies from patients with IBD for histological activity as previously published.18 19 Semiquantitative Masson’s trichrome intensity was analysed using a colour deconvolution algorithm in Aperio eSlide Manager (Leica Biosystems), calibrated for Masson’s trichrome following manufacturer’s instructions.20
ACE2 activity analyses
Enzymatic activity of ACE2 on intestinal samples was measured by a fluorescence-based assay using the commercially available synthetic fluorogenic ACE2 substrate Mca-APK (Dnp) (Enzo, USA).
Retrospective cohort and case–control studies
Retrospective cohort analysis
All medications and duration of use among consecutive patients attending the IBD Clinics at two metropolitan hospitals over 3 months, and disease characteristics over the previous 2 year period, were reviewed. Only patients with IBD and RAS blocker use for at least 2 years were included.
Disease activity over the previous 2 years was graded based on clinical data, biomarkers and endoscopic results, blinded to RAS blocker use. A five-point scale was used: 0 – quiescent disease, 1 – up to two flares per year with quiescent disease in between, 2 – more than two flares per year or persistent disease activity for less than 50% of the time, 3 – persistently active disease for over 50% of the time, 4 – persistently active disease for over 50% of the time with flares.
Case–control studies
To adjust for age as a potential confounder for disease activity and clinical outcomes, two case–control studies were performed. ‘Cases’ comprised patients with IBD who required (1) surgery or (2) hospitalisations due to IBD not requiring surgery, over the previous 2 years. ‘Controls’ were patients with IBD matched 2:1 by age (within 2 years), sex and disease. If two controls were not found, one control only was selected. Use of RAS blockers, β blockers, thiazide diuretics, calcium channel blockers and statins was recorded.
Statistical analyses
Statistical analyses were performed using SPSS V.23 and GraphPad Prism V.7.02 (Graphpad Software). Analysis of variance and unpaired t-tests (two-sided) were used for comparison of means between groups, with Tukey’s test for correction of repeated measures. The Kruskall-Wallis and Mann-Whitney tests were used to compare non-parametric variables between groups, with Dunn’s test for correction of multiple measurements. The relationship between variables was assessed by bivariate and partial correlations using Pearson’s coefficient for parametric variables and Spearman’s coefficient for non-parametric variables as appropriate. Values for faecal calprotectin were normalised by log transformation. A p value of 0.05 or less was considered statistically significant.
Results
Ang (1–7) reduces human colonic myofibroblast proliferation via Mas, and Ang II increases myofibroblast proliferation via angiotensin type 1 receptor (AT1R)
Ang (1–7) reduced cultured colonic myofibroblast cell proliferation at 48 hours in response to PDGF in a dose-dependent fashion, an effect blocked by A779 (figure 2). Captopril, an ACE inhibitor that also inhibits breakdown of Ang (1–7) to the inactive Ang (1–5), marginally but not significantly enhanced the effect of Ang (1–7) but by itself did not inhibit the effect of PDGF. Ang II marginally increased myofibroblast cell proliferation in response to PDGF, an effect that was completely reversed by candesartan. Together, these results confirm the antiproliferative effect of Ang (1–7) via Mas and the proproliferative effect of Ang II via AT1R.

Effect of Ang (1–7) and Ang II on colonic myofibroblast proliferation. (A) Ang (1–7) reduced PDGF-induced myofibroblast proliferation in a dose-dependent manner, an effect almost completely reversed by the Mas receptor antagonist A779. (B) CAND abrogated PDGF-induced myofibroblast proliferation. (C) CAPT mildly but not significantly accentuated the inhibitory effects of Ang (1–7) on myofibroblast proliferation. Concentrations are in mol/L (M). *, p<0.05; ***, p<0.0001; repeated measures two-way analysis of variance with Tukey’s test. n=6 in each group. Ang, angiotensin; CAND, candesartan; CAPT, captopril; PDGF, platelet-derived growth factor.
Ang (1–7) reduces colonic myofibroblast collagen secretion, and Ang II increases collagen secretion via AT1R
Ang (1–7) reduced and Ang II increased myofibroblast total soluble collagen secretion at 72 hours stimulated by TGF-β1 alone (figure 3). Candesartan reversed the effects of Ang II, and captopril reduced TGF-β1-induced collagen secretion, even in the presence of Ang (1–7). Together, these findings confirm the antifibrotic effect of Ang (1–7) and the profibrotic effect of Ang II via AT1R on colonic myofibroblasts.
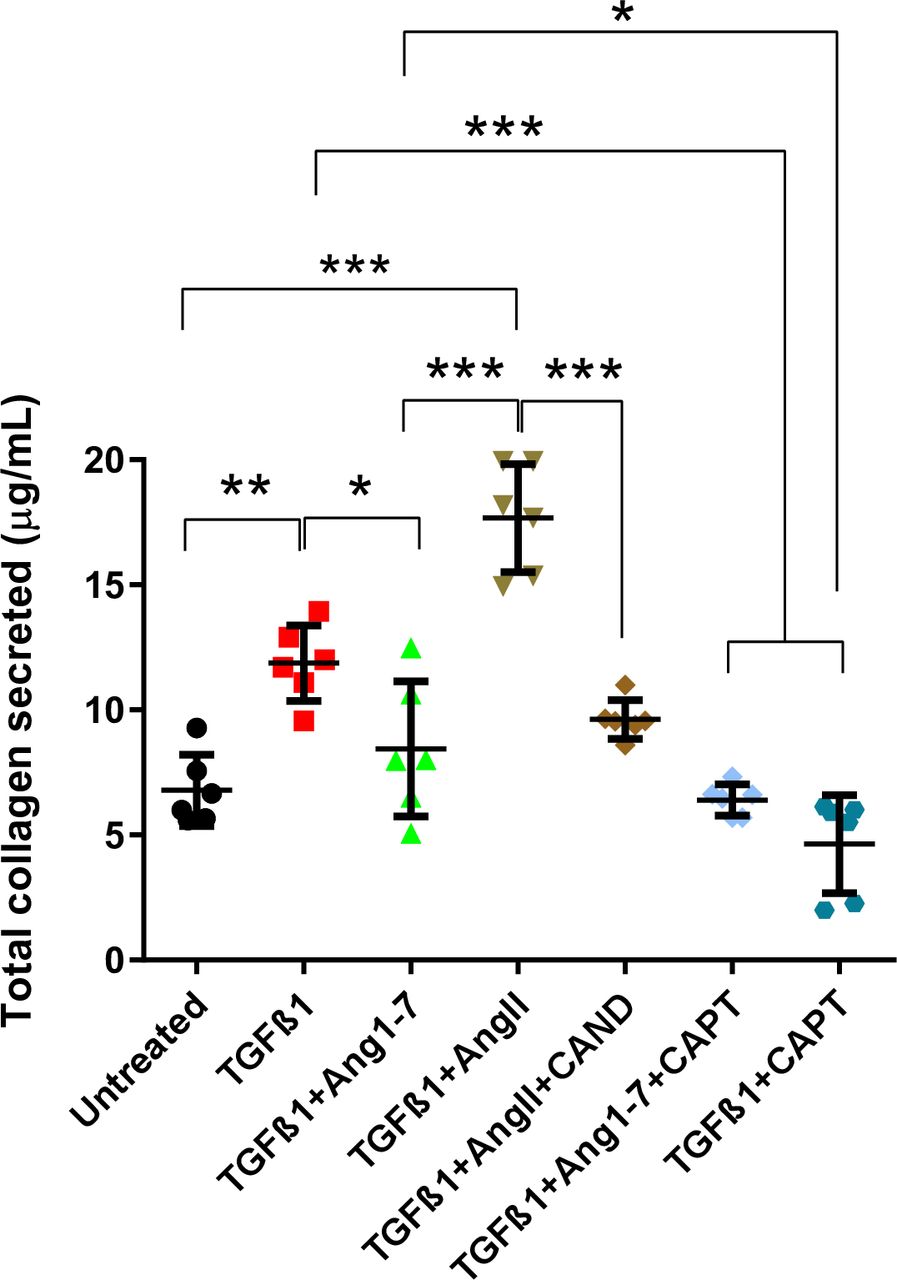
Effects of Ang (1–7) and Ang II on colonic myofibroblast collagen secretion. Ang (1–7) reduced and Ang II increased collagen secretion in response to TGF-β1. CAND reversed the effect of Ang II, and CAPT independently and in combination with Ang (1–7) reduced collagen secretion. *, p<0.05; **, p<0.001; ***, p<0.0001; repeated measures two-way analysis of variance with Tukey’s test. n=6 in each group. Ang, angiotensin; CAND, candesartan; CAPT, captopril; TGF, transforming growth factor.
Circulating renin and alternative RAS components are higher in patients with IBD compared with controls without IBD
Higher circulating renin (p=0.026, independent samples t-test) but lower aldosterone:renin ratio (ARR, p=0.003) and higher ACE2:ACE ratio (p=0.015) were observed in 93 patients with IBD (n=51 with CD, n=42 with UC) (figure 4, patient and disease characteristics in online supplementary table 4–6) than controls without IBD. Following adjustment for faecal calprotectin (as a marker of intestinal inflammation) and C reactive protein (CRP) (a marker of systemic inflammation) on binomial logistic regression analysis, non-significant trends towards higher renin (p=0.091) and ACE2:ACE ratio (p=0.096) were noted. Together, these results suggest an upregulation of the initial enzyme of the RAS pathway, and an imbalance of ACE and ACE2, in the circulation, in patients with IBD, at least partly related to extent of intestinal and systemic inflammations.

Levels of circulating RAS components in patients with IBD and controls without IBD. Patients with IBD, especially CD, had higher circulating renin levels and ratio of ACE2 activity to ACE than controls without IBD. CD, n=51; UC, n=42; controls without IBD, n=35. ANOVA, analysis of variance; CD, Crohn’s disease.
The major components of the classical and alternative RAS are expressed in the normal human ileum and colon
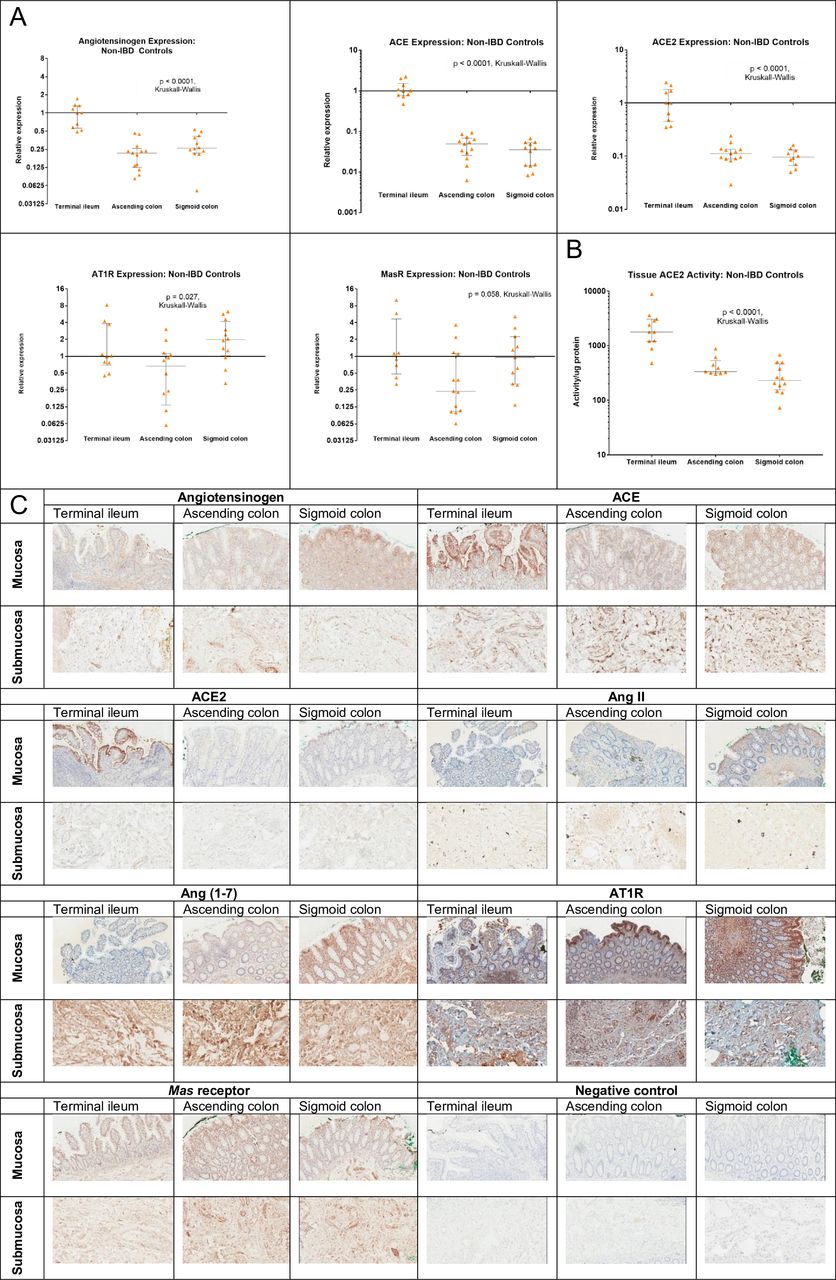
In colonoscopic biopsies from the terminal ileum and the ascending and sigmoid colons collected from 14 controls without IBD, 20 patients with CD and 15 patients with UC, and full-thickness resection specimens from 15 patients (5 with CD, 5 with UC and 5 controls without IBD), messenger RNA expression was measured for angiotensinogen, renin, ACE, ACE2 and the main receptors for Ang II and Ang (1–7)–AT1R and the Mas receptor in the terminal ileum, ascending and sigmoid colons from patients with CD and UC and controls without IBD (figure 5A). Immunohistochemical studies confirmed that angiotensinogen, ACE, ACE2, Ang II, Ang (1–7), AT1R and Mas receptor were present across the small and large intestinal layers, predominantly in the enterocytes. For ACE and ACE2, the most intense staining was seen at the brush border of the terminal ileum and the colon, as well as lamina propria and submucosal mesenchymal cells (figure 5B). Ang II, Ang (1–7) and their respective receptors AT1R and Mas also stained intensely in the lamina propria and submucosa (figure 5B). Functional activity of ACE2 in non-IBD control colonoscopic biopsies by enzyme activity assay detected 7-fold to 10-fold higher activity in samples from the terminal ileum than samples from the colon (figure 5C).

Levels of intestinal RAS components in colonoscopic biopsies from controls without IBD controls. (A) Messenger RNA expression of angiotensinogen, ACE, ACE2, AT1R and Mas receptor in terminal ileal and colonic biopsy specimens. The major components of the RAS are constitutively expressed in the terminal ileum and colon in healthy tissue, with greater expression of angiotensinogen, ACE and ACE2 in the terminal ileum than in the colon; (B) ACE2 activity in terminal ileum and colonic biopsies. ACE2 activity was approximately 10-fold higher in the terminal ileum than in the colon; (C) immunohistochemical localisation of angiotensinogen, ACE, ACE2, Ang II, Ang (1–7), AT1R and Mas receptor in intestinal resection specimens as evidenced by diaminobenzidine (DAB+) chromogenic substrate staining in brown. All RAS components were localised within the terminal ileum and colon, predominantly in the epithelium and the lamina propria. Ang, angiotensin; AT1R, angiotensin type 1 receptor; RAS, renin–angiotensin system.
ACE2 activity, Ang (1–7) and Mas receptor, but not components of the classical RAS pathway, are deficient in the inflamed mucosa in patients with IBD
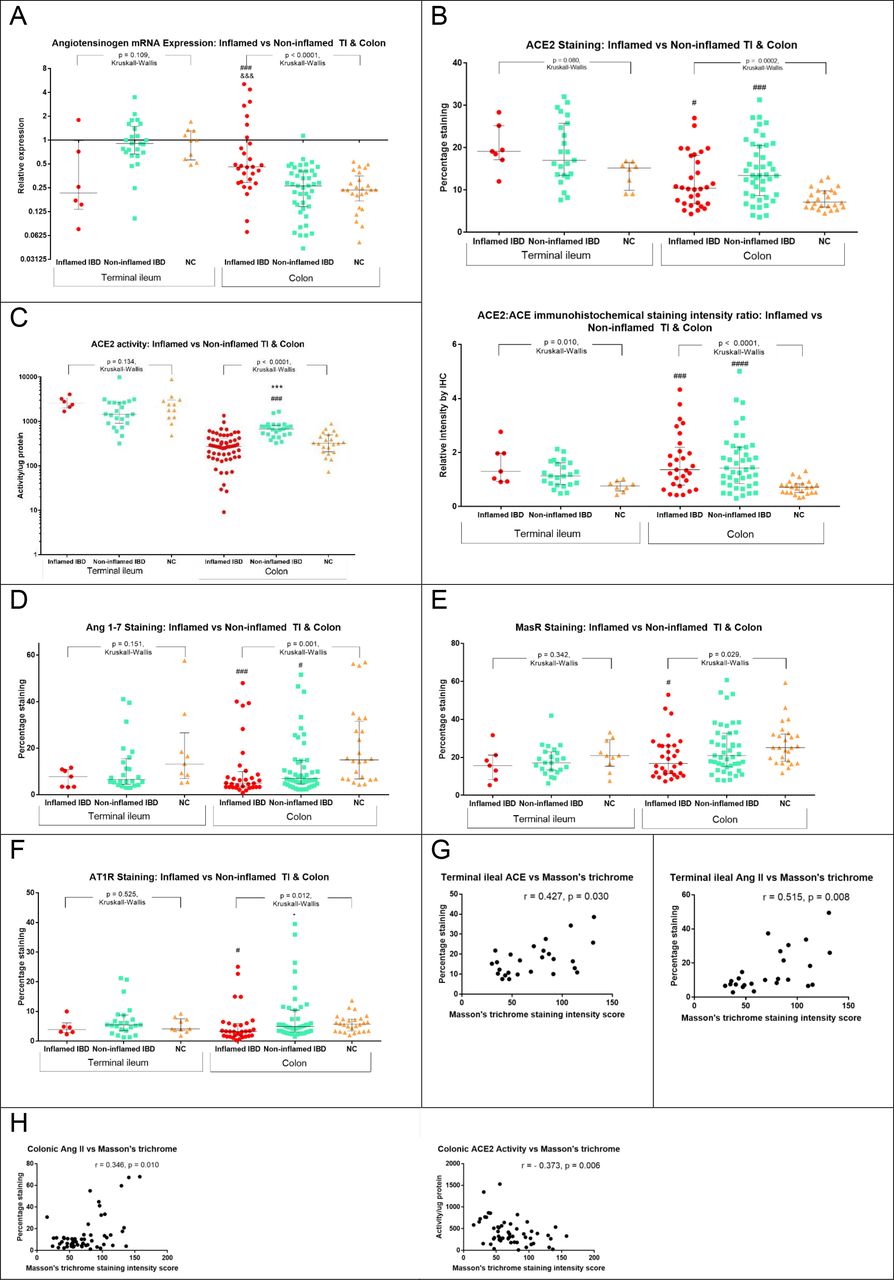
Messenger RNA expression of the angiotensinogen, renin, ACE, ACE2, AT1R and the Mas receptor in colonoscopic biopsies from the terminal ileum, ascending colon and sigmoid colon were similar across patients with CD, UC and controls without IBD (online supplementary figure 1). However, colonic biopsies from inflamed areas in patients with IBD had significantly higher mRNA expression for angiotensinogen than biopsies from the non-inflamed areas (figure 6A). Immunohistochemical staining intensity of ACE2 was significantly higher in both the inflamed and non-inflamed colonic biopsies from patients with IBD than from controls without IBD (figure 6B). The ratio of ACE2:ACE staining intensity in the terminal ileum and the colon was also higher in both inflamed and non-inflamed mucosa in patients with IBD than from controls without IBD (figure 6B). ACE2 activity was significantly higher in non-inflamed biopsies of patients with IBD than controls without IBD, but activity was significantly lower in inflamed biopsies than non-inflamed biopsies (figure 6C), suggesting reduced functional activity of ACE2 in areas of colonic inflammation. In contrast, Ang (1–7) and Mas receptor staining intensity were much lower in inflamed and non-inflamed biopsies in patients with IBD than those from controls without IBD (figure 6D and E). AT1R staining intensity was lower in inflamed colonic biopsies (figure 6f). Non-inflamed biopsies from patients with CD had higher ACE2:ACE ratio than patients with UC (p=0.005, Mann-Whitney), but no other significant differences between biopsies from inflamed and non-inflamed segments when comparing patients with CD and UC were noted. Comparison of inflamed ileal and colonic biopsies from patients with CD showed terminal ileal ACE mRNA and ACE2 mRNA expression (p<0.001), ACE and ACE2 immunohistochemical staining intensity (p<0.05) and ACE2 activity (p<0.0001) were higher than those in the colon. No associations between renin, ACE, Ang II and inflammation were observed, nor were there any associations between classical or alternative RAS components and the presence of inflammation in the terminal ileal biopsies (online supplementary figures 1 and 2). These results suggest an upregulation of ACE2 protein in the colon in patients with IBD, and inhibition or downregulation of ACE2 activity in areas of inflammation. The decreased activity of ACE2 may be responsible for the deficiency of Ang (1–7). No correlation between degree of histological activity and RAS component mRNA expression or immunohistochemical staining intensity was seen.
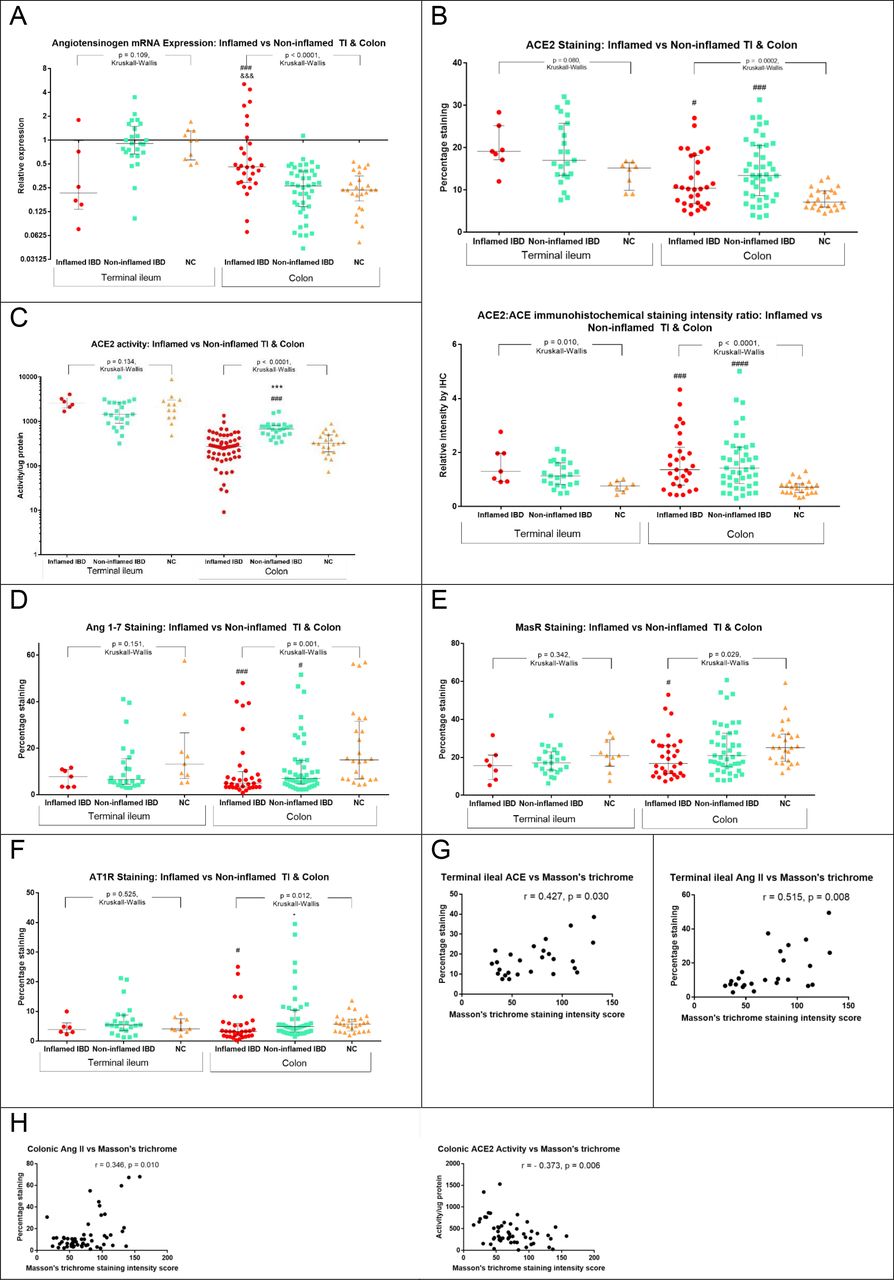
Effect of mucosal inflammation on RAS components in colonoscopic biopsies from patients with IBD (inflamed or non-inflamed areas) and controls without IBD. (A) Angiotensinogen mRNA expression; (B) ACE2 staining intensity and ACE2:ACE ratio; (C) ACE2 activity; (D) Ang (1–7) staining intensity; (E) Mas receptor staining intensity; (F) AT1R staining intensity; (G) correlation between terminal ileal mucosal Masson’s trichrome staining intensity (fibrosis) and classical components ACE, Ang II and AT1R; and (H) correlation between fibrosis and Ang II and ACE2 activity. &&&, p<0.001 versus non-inflamed IBD colonic biopsies; *, p<0.05 versus inflamed colon biopsies; ***, p<0.0001 versus inflamed colon biopsies; #, p<0.05 versus non-IBD control colon biopsies; ###, p<0.001 versus non-IBD control colon biopsies; ####, p<0.0001 versus non-IBD control colon biopsies, Dunn’s multiple comparisons test. Ang, angiotensin; AT1R, angiotensin type 1 receptor; TI, terminal ileum.
The relationship between mucosal fibrosis as assessed by Masson’s trichrome staining intensity in colonoscopic biopsies and RAS components was assessed by bivariate correlations. In the terminal ileum, fibrosis was correlated with immunohistochemical staining intensity for ACE, Ang II and AT1R (figure 6G). In the colon, fibrosis correlated with immunohistochemical staining intensity for Ang II and negatively correlated with ACE2 activity (figure 6H). Taken together, mucosal fibrosis is positively associated with classical RAS components and negatively associated with ACE2 activity.
Treatment with ACE inhibitors and Ang receptor blockers was associated with lower rates of surgery and hospitalisation in patients with IBD
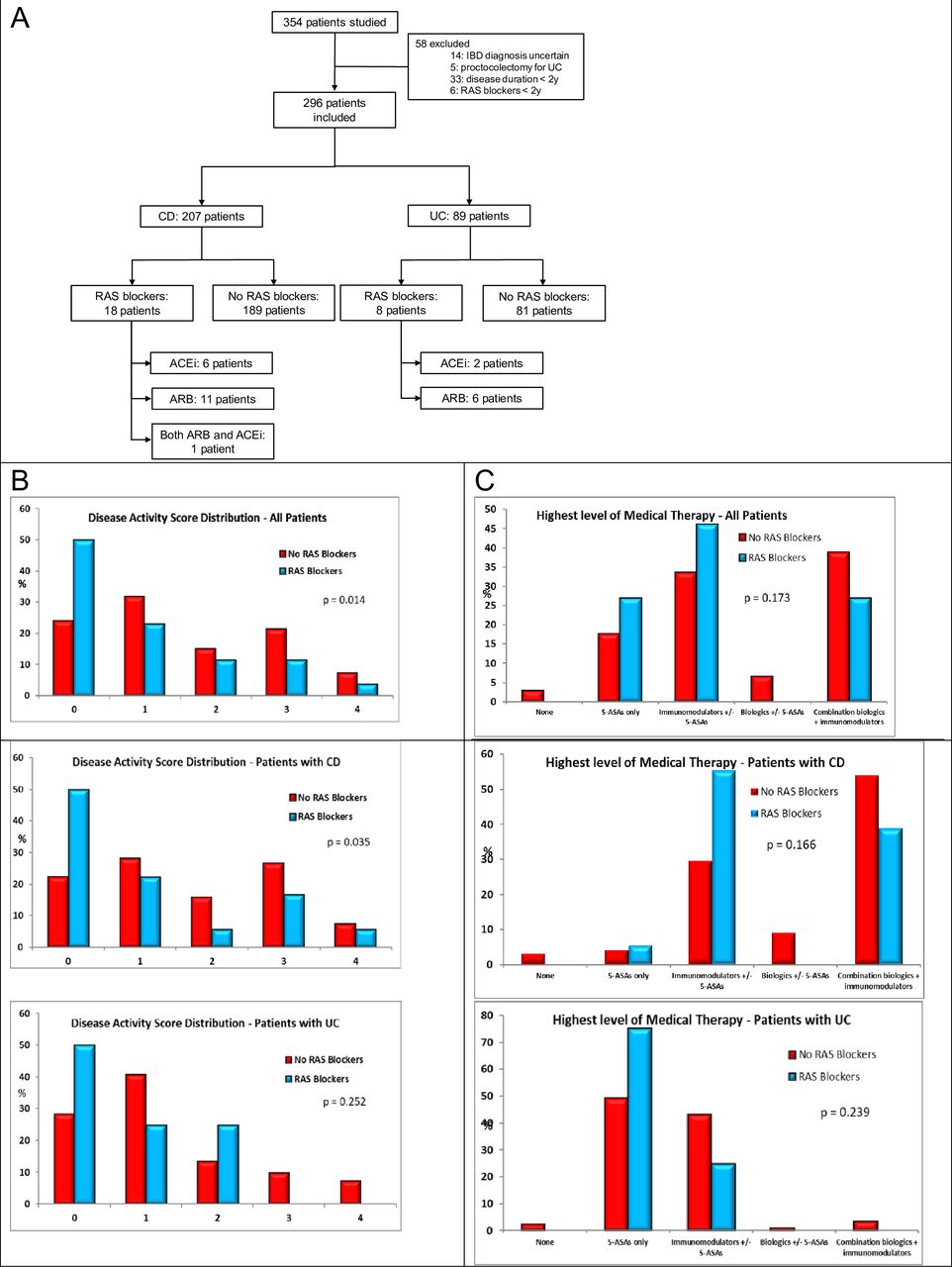
In a retrospective cohort study of patients attending IBD clinics, 26 of 296 patients studied over a 3-month period were treated with RAS blockers for at least 2 years (figure 7A) (online supplementary table 7). Disease activity scores over the previous 2 years were significantly lower in patients with IBD treated with RAS blockers (p=0.016) and in patients with CD (p=0.040) (figure 7B, online supplementary table 8). Patients with CD on RAS blockers trended to fewer treatments with biologics (39% vs 63%, p=0.074). Requirement for hospitalisation not requiring surgery was significantly lower (0% vs 15%; p=0.033) for patients with IBD treated with RAS blockers. Faecal calprotectin, measured in 96 patients within the previous 3 months, was lower in 8 patients who were using RAS blockers (p=0.046). In the first nested case–control study, 39 patients who were required to undergo surgery were compared with 75 age-matched and sex-matched controls. No significant difference in disease activity scores, IBD medication use, most recent CRP or faecal calprotectin was noted between cases and controls (online supplementary table 9). RAS blocker use was more common among patients who did not require surgery (p=0.034), all of whom had CD. In the second nested case–control study comparing 34 patients who were hospitalised with 68 controls (online supplementary table 10), disease activity scores were significantly higher among hospitalised patients with CD, and patients not requiring hospitalisation were more likely to be treated with RAS blockers (p=0.049). Use of β blockers, calcium channel blockers, thiazide diuretics, statins, non-steroidal anti-inflammatory drugs (NSAIDs) or antidepressants was not significantly different between cases requiring surgery or hospitalisation and respective controls.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Retrospective cohort study evaluating the association of disease activity and outcomes in patients treated with RAS blockers. (A) Patient flowchart. Twenty-six patients (8.8%) were treated with ACEi and/or ARBs, 8 with ACEi (7 perindopril and 1 ramipril), 16 with Arbs (7 candesartan, 4 irbesartan and 5 telmisartan), and 1 with both perindopril and irbesartan. (B) Disease activity score distribution and (C) maximal level of medical therapy over the previous 2 years in patients treated and not treated with RAS blockers. Disease activity score: 0, quiescent disease; 1, up to two flares per year with quiescent disease in between; 2, more than two flares per year or persistent disease activity for less than 50% of the time; 3, persistently active disease for over 50% of the time; 4, persistently active disease for over 50% of the time with flares. ACEi, ACE inhibitor; ARB, angiotensin receptor blocker; CD, Crohn’s disease; RAS, renin–angiotensin system.
Discussion
Effective treatments for fibrosis remain a significant unmet need in patients with IBD. The current study has defined the distribution of multiple RAS components in the terminal ileum and colon by PCR and immunohistochemistry, identified intrinsic ACE2 activity and found differences in mucosal RAS components in inflamed and non-inflamed mucosa. Colonic myofibroblast proliferation and collagen secretion were influenced by the key RAS peptides Ang (1–7) and Ang II, with their effects modulated by ACE inhibition and AT1R blockade. Furthermore, ACE inhibitors and ARBs were associated with lower disease activity, a reduced need for surgery and fewer hospitalisations in patients with IBD. Such findings provide the foundation for the development of a new class of therapeutics for patients with IBD.
The relative influence of two complementary arms of the RAS, which present opposing functions with respect to inflammation, fibrosis, cell proliferation and angiogenesis, determines the ultimate tissue homeostatic effect.21 Circulating Ang (1–7) levels were higher in patients with IBD, especially CD, than in patients without IBD.7 In this report, circulating renin and ratio of ACE2 activity to ACE were higher, whereas ARR was lower, in patients with IBD, especially CD, than in patients without IBD. Higher circulating renin levels and low ARR may be explained by a relative hypovolemic state with potassium losses in a patient with active IBD. Lending support to this concept, ARR levels correlated with serum potassium levels among patients with IBD (Spearman r=0.313, p=0.004) and with systemic inflammation as assessed by CRP (Spearman r=0.24, p=0.024), but not intestinal inflammation as evidenced by faecal calprotectin (Spearman r=0.12, p=0.274). Higher circulating ACE2 may reflect generation via cleavage at its ectodomain by the metallosecretase, ADAM 17, which is elevated in states of endothelial stress and inflammation, including IBD.22–24
Cultured colonic myofibroblasts had reduced PDGF-induced proliferation and TGF-β-induced collagen secretion in the presence of Ang (1–7). In the presence of Ang II, myofibroblasts increased collagen secretion. The effects of Ang II on myofibroblast proliferation and collagen secretion were ameliorated by the ARB candesartan, and the effect of Ang (1–7) on myofibroblast proliferation was reversed by the Mas receptor antagonist A779. Together, these observations support involvement of intestinal RAS, mediated by Ang (1–7) via Mas receptor, and Ang II via AT1R, in mediating fibrosis in patients with IBD. ARBs, already in widespread clinical use, as well as novel therapies based on Ang (1–7), including the Mas receptor agonist AVE 0991, have been shown to ameliorate intestinal inflammation in mouse models of colitis.9 12 15 25
The presence of RAS-associated mRNAs in biopsies and resection specimens from patients with and without IBD reflects capacity for autonomous production within the intestine of many of the components of the RAS. Notably, all components including angiotensinogen, ACE, ACE2, Ang II, Ang (1–7), AT1R, AT2R and Mas receptor were seen by immunohistochemistry, including in epithelial cells, a crucial interface in the pathogenesis of IBD. As reported previously in smaller cohorts, ACE and ACE2 mRNA expression and protein intensity were higher in the terminal ileum than in the colon.4 26 Small intestinal brush border ACE and ACE2 function as peptidases, allowing mucosal digestion and peptide absorption,27 28 but their role in colonic homeostasis is undefined.
Several findings suggest dysregulation of the RAS in intestinal inflammation. These include increased angiotensinogen mRNA from inflamed colonic biopsies, and higher immunohistochemical staining intensity of ACE2, and ratio of ACE2:ACE, in inflamed and non-inflamed colonic, and to a lesser extent terminal ileal mucosa, in patients with IBD compared with controls without IBD. ACE2 activity was reduced in inflamed compared with non-inflamed colonic biopsies, and the staining intensity for Ang (1–7) and Mas receptor was reduced in inflamed and non-inflamed biopsies from patients with IBD. This suggests reduced tissue ACE2 activity, and consequently Ang (1–7), due to or predisposing to inflammation, and may be a therapeutic target in IBD.
Furthermore, the positive correlation between staining intensity for ACE, Ang II and AT1R with mucosal fibrosis in colonoscopic biopsies from patients with IBD, and inverse correlation with ACE2 activity provide evidence that fibrosis may be mediated by the classical RAS pathway, and downregulation of ACE2 activity may increase propensity to collagen deposition. Upregulation of circulating ACE2:ACE and Ang (1–7) may reflect a compensatory response to this.
Interestingly, intestinal ACE2 is also required for absorption of tryptophan, an essential amino acid required for the generation of niacin (also known as nicotinamide or vitamin B3), the deficiency of which leads to pellagra, a disease of protein malnutrition that causes intestinal inflammation.29 ACE2 knockout mice had increased susceptibility to colitis and an altered microbiota profile, which was associated with higher colonic Ang II levels.29 Recently, serum tryptophan levels were shown to be lower in patients with IBD, especially CD, than in controls without IBD.30 We therefore propose that reduced ACE2 activity in the intestine in susceptible patients with IBD predisposes to inflammation, and potentially mural fibrosis, via two separate mechanisms: reduced Ang (1–7) and tryptophan deficiency. This hypothesis requires further exploration.
Whether currently available agents which target the RAS, including ACE inhibitors and ARBs, may influence disease outcomes in patients with IBD is crucial to investigate. Indeed, ARBs may increase tissue ACE2 mRNA expression as a compensatory response following blockade of downstream Ang II effects.31 In the current retrospective cohort analysis, patients treated with RAS blockers had lower disease activity indices and trended towards less requirement for biologic medication use for CD, and hospitalisations and surgery for IBD. RAS blockers are prescribed for conditions including hypertension, cardiac and kidney disease, which more commonly affect the elderly, and some (but not all) data suggest that IBD severity and risk of complications are lower in older patients compared with younger patients.32–34 Nested case–control studies adjusting for age and sex showed that patients who did not require surgery or hospitalisation, respectively, were significantly more likely to be treated with RAS blockers than those who required hospitalisation or surgery. The same relationship was not noted for other medications often prescribed for the same conditions, including β blockers, thiazide diuretics, calcium channel antagonists and statins, suggesting an independent effect of RAS blockade. Other possible confounders include potential cessation of RAS blockers in hospitalised patients with diarrhoea or dehydration, and comorbidities requiring RAS blockers influencing prescription for immunosuppression or referral for surgery due to higher risk of complications. The relatively small sample size precluded associations among patients with UC only or specific disease phenotypes of CD being found, or subgrouping for a single class of drug (ACE inhibitors vs ARBs) or dose effect. The use of NSAIDs and antidepressants,35–37 other medications which have been shown to potentially be associated with disease outcomes in patients with IBD, was not significantly different among patients requiring hospitalisation or surgery.
The strength of the intestinal RAS component analyses lies primarily in the prospective, uniform approach to collection and analyses of intestinal samples from a well-defined cohort of subjects. Nonetheless, several methodological issues require discussion. Given the intricate involvement of the RAS in vascular regulation throughout the body, the effect of tissue ischaemia on mRNA expression and immunohistochemical staining of the RAS components during collection of specimens following devascularisation is uncertain. Any such delay was minimised by careful collection and immediate fixation. Immunohistochemical staining intensity of peptides, though described previously,38–40 must be regarded as semiquantitative at best, and non-parametric analyses were performed for comparison. The finding in this study of all the RAS components in the epithelium is of great value, especially with the location of ACE, ACE2, Ang II and Ang (1–7) in the brush border of the epithelium, which has not been described previously. The cell culture studies outlined here have focused on cell proliferation and fibrosis, but localisation of RAS components, together with previously published data in other systems,3 41 suggest that functional assays evaluating immunoregulatory and inflammation-modifying properties in the intestinal wall would be prudent to investigate in future studies. The scale used in the retrospective cohort study of patients with IBD incorporated multiple factors, such as clinical data, biomarkers and endoscopic results over a finite period of 2 years, able to be interrogated from hospital records by physicians blinded to the use of RAS blockers, but is not previously described. There is no clear, validated index for retrospective longitudinal assessment of disease activity, such as for a 2-year time frame. Future studies will be required to validate this index prospectively.
Despite limitations of cross-sectional laboratory and retrospective observational clinical studies in drawing conclusions regarding causality, the presence of a locally produced and acting intestinal RAS, and the influence of effector peptides on cell proliferation and collagen secretion, supports further research regarding the potential use of therapies targeting the RAS in patients with IBD. Currently available therapies are more effective at reducing inflammatory and penetrating rather than stricturing complications of CD.1 Fibrosis is also an under-recognised feature of long-standing UC and may predispose to risk of malignancy and dysmotility.42 Modelling of the extracellular matrix by the RAS in other organs has long been recognised.43–45 Both ACE inhibitors and ARBs have potential teratogenic effects46 47 that warrant caution in reproductive-age women. Olmesartan should be avoided due to risk of coeliac sprue-like enteropathy.48 ACE inhibitors also rarely cause idiosyncratic intestinal angio-oedema.49
In conclusion, major components of the RAS are expressed and act locally in the human intestine, with circulating and intestinal RAS components, especially the alternative pathway, perturbed in patients with IBD. The key effector peptides Ang (1–7) and Ang II have the capacity to influence colonic myofibroblast cell proliferation and collagen secretion, via the Mas receptor and AT1R respectively. Conventional agents that modify the RAS, including ACE inhibitors and ARBs, may influence outcomes in patients with IBD. There is hence a need for further study of this potentially novel therapeutic pathway through well-designed prospective clinical studies in IBD.
References
Footnotes
Correction notice This article has been corrected since it published Online First. The title has been amended.
Contributors All authors approved the final version. Each author’s contribution is as follows:
MG conceived and designed the studies; performed specimen and data collection and experiments including PCR, immunohistochemistry, serum ACE2 activity analyses; analysed and interpreted the data; and wrote the manuscript.
SGR designed and performed immunohistochemistry studies and cell culture studies, analysed and interpreted the data, critically appraised the manuscript and approved the final version.
CT designed and performed PCR and tissue ACE2 activity studies, analysed and interpreted the data, critically appraised the manuscript and approved the final version.
CS performed PCR studies, critically appraised the manuscript and approved the final version.
DB performed tissue ACE2 activity assays, critically appraised the manuscript and approved the final version.
EV performed plasma ACE2 activity assays, critically appraised the manuscript and approved the final version.
LMB designed and supervised plasma ACE2 activity assays, critically appraised the manuscript and approved the final version.
LB collected patient data for retrospective cohort and case–control studies and approved the final version.
AJ collected patient data for retrospective cohort and case–control studies and approved the final version.
KB collected patient data for retrospective cohort and case–control studies, and approved the final version.
ML collected patient data for retrospective cohort and case–control studies and approved the final version.
PS performed and assisted with the PCR studies, critically appraised the manuscript and approved the final version.
HW performed and assisted with the PCR studies, critically appraised the manuscript and approved the final version.
YH isolated colonic tissue for cell culture studies, critically appraised the manuscript and approved the final version.
CWT isolated colonic tissue for cell culture studies, critically appraised the manuscript and approved the final version.
MF isolated colonic tissue for cell culture studies, critically appraised the manuscript and approved the final version.
AWB designed and supervised colonic tissue isolation for cell culture studies, critically appraised the manuscript and approved the final version.
PH analysed the histological activity of colonic biopsies, critically appraised the manuscript and approved the final version.
SM analysed the histological activity of colonic biopsies, critically appraised the manuscript and approved the final version.
MT supervised PCR and tissue ACE2 activity studies, critically appraised the manuscript and approved the final version.
PRG conceived, designed and supervised the studies, critically appraised the manuscript and approved the final version.
JL conceived, designed and supervised the studies, analysed and interpreted the data, critically appraised the manuscript and approved the final version.
Funding statement This work was supported by the Gastroenterological Society of Australia Scholarship awarded to MG and a Broad Medical Research Program Grant awarded to JL.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Written informed consent was obtained from all participants for the prospective studies where patient information and samples were collected. No informed consent was required from the patients who were part of retrospective cohort and case–control studies, in which anonymised patient data were collected. The protocols for these studies were approved by the Eastern Health Department of Research and Ethics (E03-1112 and LR93-1112).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The authors declare that most of the data supporting the findings of this study are available within the paper and its supplementary information files. All other data are available from the corresponding author upon reasonable request.