Article Text

Abstract
Introduction A meta-analysis was performed using individual patient data from the five most recent randomised controlled trials (RCTs) which evaluated corticosteroids in severe alcoholic hepatitis (Maddrey discriminant function (DF) ≥32 or encephalopathy). This approach overcomes limitations associated with the use of literature data and improves the relevance of the study and estimates of effect size.
Aims To compare 28-day survival between corticosteroid- and non-corticosteroid-treated patients and to analyse the response to treatment using the Lille model.
Methods Individual patient data were obtained from five RCTs comparing corticosteroid treatment with placebo (n=3), enteral nutrition (n=1) or an antioxidant cocktail (n=1).
Results 221 patients allocated to corticosteroid treatment and 197 allocated to non-corticosteroid treatment were analysed. The two groups were similar at baseline. 28-day survival was higher in corticosteroid-treated patients than in non-corticosteroid-treated patients (79.97±2.8% vs 65.7±3.4%, p=0.0005). In multivariate analysis, corticosteroids (p=0.005), DF (p=0.006), leucocytes (p=0.004), Lille score (p<0.00001) and encephalopathy (p=0.003) were independently predictive of 28-day survival. A subgroup analysis was performed according to the percentile distribution of the Lille score. Patients were classified as complete responders (Lille score ≤0.16; ≤35th percentile), partial responders (Lille score 0.16–0.56; 35th–70th percentile) and null responders (Lille ≥0.56; ≥70th percentile). 28-day survival was strongly associated with these groupings (91.1±2.7% vs 79.4±3.8% vs 53.3±5.1%, p<0.0001). Corticosteroids had a significant effect on 28-day survival in complete responders (HR 0.18, p=0.006) and in partial responders (HR 0.38, p=0.04) but not in null responders.
Conclusion Analysis of individual data from five RCTs showed that corticosteroids significantly improve 28-day survival in patients with severe alcoholic hepatitis. The survival benefit is mainly observed in patients classified as responders by the Lille model.
- Alcoholic liver disease
- cirrhosis
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Randomised controlled trials have suggested that corticosteroids improve survival in severe alcoholic hepatitis.
The Lille model is a prognostic tool that predicts 6-month survival using a single cut-off.
Non-responders to corticosteroids have a poor survival.
What are the new findings?
This paper combines the data from 418 patients included in five recent randomised controlled trials using corticosteroids and shows that corticosteroid treatment improves survival in severe alcoholic hepatitis.
Three groups of patients are defined using two new cut-offs of the Lille score.
Using this approach, response to corticosteroids is better defined and the prediction of 6-month survival is improved.
How might it impact on clinical practice in the foreseeable future?
This paper provides additional data on the management of patients with severe alcoholic hepatitis. Using individual patient data from more than 400 patients, we demonstrated improved survival with corticosteroid treatment. A new response-guided therapy based on the Lille model is proposed that will allow clinicians to better stratify the response to treatment and improve prediction of survival. This approach should help define the subgroups of patients who are candidates for alternative therapies.
Introduction
Evaluation of whether a treatment improves survival in alcoholic hepatitis (AH) requires an accurate definition of disease severity.1 In randomised controlled trials (RCTs) in AH performed before the use of the Maddrey discriminant function (DF), survival in the untreated control arms ranged from 0% to 81%.2–14 In the absence of treatment, the survival of patients with a DF ≥32 ranges from 50% to 65%.7–15 Conversely, because survival without treatment at 28 days in patients with a DF <32 is close to 90%,15 it is difficult to document an effect of short-term treatment on survival in this subgroup.
Only corticosteroids and pentoxifylline are considered to potentially improve short-term survival.1 Meta-analyses of the 15 RCTs2–17 performed by three different groups concluded that the survival benefit of corticosteroid treatment was restricted to patients with severe AH.18–20 Conversely, Cochrane meta-analyses questioned the efficacy of corticosteroids in AH regardless of disease severity,21 22 although their most recent meta-analysis reported that corticosteroids significantly reduced mortality in the subgroup of trials that enrolled patients with a Maddrey score of at least 32 or hepatic encephalopathy.22
Meta-analysis of individual patient data can overcome limitations associated with meta-analyses of published articles because it provides the least biased and most reliable means of addressing questions that have not been satisfactorily resolved by individual clinical trials.23 The superiority of this approach is confirmed by the fact that true survival is lower for conclusions from meta-analysis of the literature than for conclusions derived from non-meta-analyses.24 We previously performed a meta-analysis of individual data from three recent RCTs of patients with a DF ≥32.15 That study showed a higher 28-day survival in patients randomised to corticosteroids. However, after collection of these individual data, two RCTs comparing corticosteroids with enteral nutrition or an antioxidant cocktail were published.16 17
Therapeutic interventions which improve liver function at an early time point are likely to improve short-term survival, and studies focusing on a strategy integrating the early impact of treatment on liver function are warranted.25 26 The Lille model, which evaluates baseline variables as well as early response to treatment, may be used to evaluate the effectiveness of different treatments in patients with severe AH. Such an analysis could represent progress in understanding the therapeutic management of patients with severe AH.
The aims of the present study of individual patient data from five RCTs of patients with a DF ≥32 or encephalopathy were: (1) to compare 28-day survival in patients receiving corticosteroids and those receiving placebo or ineffective treatments; (2) to identify independent prognostic factors associated with short-term survival; and (3) to analyse the response to treatment using the Lille model.
Patients and methods
Studies were selected if they were randomised, published as full articles and had specific data on patients with a DF ≥32 or encephalopathy, and if those RCTs compared corticosteroids with placebo or therapy without a beneficial effect on short-term mortality. Because pentoxifylline potentially improved short-term survival, studies evaluating this drug were excluded. Only the last five RCTs had available individual data. Three RCTs12–14 had been included in our previous meta-analysis of individual data15 and two had been published since the previous collection of individual data.16 17 Principal investigators from the five RCTs were invited, and agreed, to provide individual data. For this analysis we retrospectively identified patients with a DF ≥32 or encephalopathy at admission or on the first day of treatment. The authors of one RCT of patients with a DF ≥32 or encephalopathy had lost their database because of a computer system crash.16 Individual patient survival data for this RCT were therefore retrieved from the total number and the actuarial curve of survival according to the method described by Fine et al and others.27 28 Briefly, the number of steps in the Kaplan–Meier survival curve, allowing for larger steps representing two or more nearly concurrent deaths, implies that any remainder of patients not accounted for must have been censored. Careful measurement of survival probabilities at each step, and hence of the size of successive steps, indicated where censoring times must have occurred. This is possible because the size of any step depends on the number of patients at risk at that time; when a death occurs among a group of k remaining patients, the survival curve drops by a factor of (k − 1)k. The loss of a patient from the group of those remaining at risk therefore means that the following step, when a patient next dies, is larger than it would otherwise have been.
Statistical analysis
The data managers of the four remaining trials provided the following information: study centre, age, sex, presence of encephalopathy, presence of ascites, survival data until the end of the treatment period, serum bilirubin level, prothrombin time, serum albumin level, serum aspartate aminotransferase (AST), serum creatinine, white blood cell count, DF, change of bilirubin after 7 days of treatment, treatment assignment (corticosteroid or non-corticosteroid), Maddrey DF (defined as 4.6 × (patient prothrombin time − control prothrombin time (in s) + serum bilirubin level (in mg/dl)) and change of liver function blood tests during treatment. Since a DF of >32 or hepatic encephalopathy indicate severe AH and the two represent classical criteria for initiating corticosteroid treatment, only patients with a DF ≥32 or hepatic encephalopathy were included in the present study. We retrospectively identified, from Mendenhall's study, randomised patients with a DF ≥32 at admission or on the first day of treatment. The original reports from Carithers et al and Ramond et al analysed only short-term survival (28 days and 2 months, respectively). The original report from three other RCTs analysed either short-term (1 month) or long-term survival. Survival data were available only at 28 days in the study by Carithers et al. Thus, in the present study, survival at 28 days after the end of treatment was the primary end point. All p values were two-tailed. Follow-up time was defined as the period from the first day of treatment to 28 days after initiation of the assigned treatment. Data for patients who did not have events of interest were censored at the date of the last follow-up visit. Survival was assessed by the intention-to-treat method—that is, patients were included in the randomised group even if treatment was discontinued. Patient survival was estimated by the Kaplan–Meier method and compared using the log-rank test. The response to the assigned treatment assessed with the Lille model was the secondary end point. The Lille score is defined as: 3.19 − 0.101 × age (years) + 0.147 × albumin (g/l) on day 0 + 0.0165 × change in bilirubin on day 7 (μmol/l) − 0.206 × renal insufficiency (rated as 0 if absent and 1 if present) − 0.0065 × bilirubin level on day 0 (in μmol/l) − 0.0096 × prothrombin time (in s). The Lille score ranges from 0 to 1 with the use of the formula: exp (−R)/(1+exp (−R)). The change in bilirubin levels in the Lille model is defined as the difference in bilirubin levels between day 0 and day 7 of corticosteroid treatment. Using the Lille model, patients may be classified as satisfactory responders to the allocated therapy (ie, those with a Lille score <0.45) or poor responders to corticosteroids (ie, those with a Lille score ≥0.45). In order to gain more insight into the relationship between corticosteroid effects and response to therapy, we performed subgroup analysis in which patients were classified according to the percentile distribution of the Lille score (≤35th percentile, 35–70th percentile and ≥70th percentile). The percentile distribution was used to prevent an arbitrary definition of a cut-off based on subjective criteria.
To identify independent predictors of 28-day survival, baseline variables that achieved a p value of <0.1 in univariate analysis were included in multivariate analysis. The cut-off level chosen for quantitative variables was the median value. Proportional hazards models were used to identify factors independently associated with survival, including the treatment assignment, and adjusted for RCTs. To avoid bias related to the effect of colinearity, when a composite score was tested, factors included in the composite score were not included in the multivariate analysis. In all multivariate models a variable for the trial was introduced to take into account heterogeneity among the different trials. The significance of each factor was expressed by the regression coefficient and tested by the likelihood ratio test. All statistical analyses were performed using NCSS 2004 software.
Results
Identification of patients with a DF ≥32 or encephalopathy in the five trials
From the five RCTs we retrospectively identified randomised patients with a DF ≥32 or hepatic encephalopathy at admission or on the first day of treatment. In the study by Mendenhall et al, 88 and 91 patients were randomised into placebo and corticosteroid groups, respectively. Of these, 54 in the placebo group (44 with DF ≥32 and 10 with encephalopathy and DF <32) and 65 in the corticosteroid-treated group (52 with DF ≥32 and 13 with encephalopathy and DF <32) had severe AH. The remaining four RCTs included only patients with a DF ≥32 or encephalopathy; in the study by Carithers et al, 31 (30 with DF ≥32 and 1 with encephalopathy and DF <32) were randomised to receive placebo and 35 (32 with DF ≥32 and 3 with encephalopathy and DF <32) received corticosteroid, in the study by Ramond et al there were 29 (27 with DF ≥32 and 2 with encephalopathy and DF <32) in the placebo group and 32 (29 with DF ≥32 and 3 with encephalopathy and DF <32) in the corticosteroid group, in the study by Cabre et al 35 patients were treated with enteral nutrition and 36 with corticosteroids and in the study by Phillips et al 47 patients with DF ≥32 were treated with an antioxidant cocktail and 50 were treated with corticosteroids.
Characteristics of patients on the first day of treatment
A total of 197 patients in the non-corticosteroid group and 221 patients in the corticosteroid group were analysed. The demographic, clinical and biochemical characteristics on the first day of treatment of these patients is given in table 1. On day 1 of treatment there were no significant differences between the corticosteroid and control groups. Both groups had markedly abnormal liver function, as shown by prothrombin time, bilirubin and DF in the control and corticosteroid groups (16 vs 16 s, 295 vs 295.8 μmol and DF 48.5 vs 48.4, respectively).
Baseline demographic clinical, and laboratory characteristics on the first day of treatment for patients with severe alcoholic hepatitis (AH) pooled according to random assignment to control or corticosteroid treatment
28-day survival of patients with severe AH (DF ≥32 or hepatic encephalopathy)
A total of 110 patients, 67 in the group not receiving corticosteroids and 43 in the group receiving corticosteroids, died during the 28 days following the start of the assigned treatment (p=0.0007). At 28 days, patients in the non-corticosteroid group had significantly poorer survival than those in the corticosteroid group (65.7%±3.4% vs 79.97%±2.8%, p=0.0005; figure 1). In univariate analysis, seven variables on the first day of treatment, together with the Lille model, were factors predicting survival at 28 days (table 2). In multivariate analysis, corticosteroid treatment, DF, white blood cell count, Lille score and encephalopathy independently predicted survival at 28 days (table 2). After exclusion of the Lille score and considering only variables on the first day of treatment, corticosteroid treatment (p=0.0001), age (p<0.00001), creatinine (p=0.02), DF (p<0.00001), white blood cell count (p=0.002) and encephalopathy (p<0.00001) were independent predictive factors for survival at 28 days, with a trend towards significance for albumin (p=0.09).

Probability of 28-day survival according to treatment with corticosteroids or non-corticosteroids. The numbers below the x-axis represent the number of at-risk patients at the beginning of each time point.
Factors predicting 28-day survival in univariate and multivariate analyses
Response to treatment according to the Lille model and evolution of liver function
All analyses of response to treatment were performed only in patients from the four RCTs providing individual data on their patients. Corticosteroids induced a rapid and significant improvement in liver function at an early time point (after 7 days of the allocated therapy) compared with non-corticosteroid treatment (table 3). This improvement in hepatic function was sustained until the end of the treatment period in the corticosteroid group compared with the non-corticosteroid group (table 3).
Change in laboratory tests in corticosteroid and non-corticosteroid groups at days 7, 14 and 28 of treatment
In an analysis of all patients, the Lille score was significantly higher in those who died than in those who remained alive at 28 days (0.669 (95% CI 0.524 to 0.817) vs 0.209 (95% CI 0.175 to 0.266), p<0.00001). Patients in the non-corticosteroid group had significantly higher Lille scores than those in the corticosteroid group (table 3). The percentage of patients considered to have a satisfactory response to the allocated therapy (Lille score <0.45) was lower in the non-corticosteroid group than in the group randomised to corticosteroid (56.1% vs 68.2%, p=0.03). For the totality of patients and regardless of allocated therapy, satisfactory responders had better survival than those without a satisfactory response (88%±2.3% vs 55.1%±4.5%, p<0.00001). In sensitivity analysis restricted to patients classified as satisfactory responders, non-corticosteroid-treated patients had lower 28-day survival than corticosteroid-treated patients (79.5%±4.4% vs 94%±2.2%, p=0.002). Conversely, in patients classified as poor responders (Lille score ≥0.45) there was no significant difference in 28-day survival between non-corticosteroid-treated and corticosteroid-treated patients (50.3%±6.2% vs 60.7%±6.5%, p=0.2).
Subgroup analysis was performed according to the percentile distribution of the Lille score (≤35th, 35–70th and ≥70th percentiles). Taken together and regardless of allocated therapy, patients with a Lille score of ≤0.16 (≤35th percentile) had significantly higher 28-day survival than those with a Lille score of 0.16–0.56 (35th–70th percentile) and those with a Lille score ≥0.56 (≥70th percentile): 91.1%±2.7% vs 79.4%±3.8% (p=0.02) vs 53.3%±5.1% (p<0.0001). The difference between patients with a Lille score of 0.16–0.56 and those with a Lille score ≥0.56 was also significant (p=0.0001, figure 2). Thus, patients were considered to be complete responders with a Lille score ≤0.16 (≤35th percentile), partial responders with a Lille score of 0.16–0.56 (35th–70th percentile) and null responders with a Lille score ≥0.56 (≥70th percentile). Corticosteroid therapy had a significant effect on 28-day survival in complete responders (HR 0.18, 95% CI 0.05 to 0.71; p=0.006) and in partial responders (HR 0.38, 95% CI 0.17 to 0.87, p=0.04). Conversely, corticosteroid therapy did not have a significant effect on 28-day survival in null responders (HR 0.81, 95% CI 0.45 to 1.45, p=0.47). The estimated 28-day survival in six hypothetical patients according to treatment and Lille score are shown in figure 3A–C.
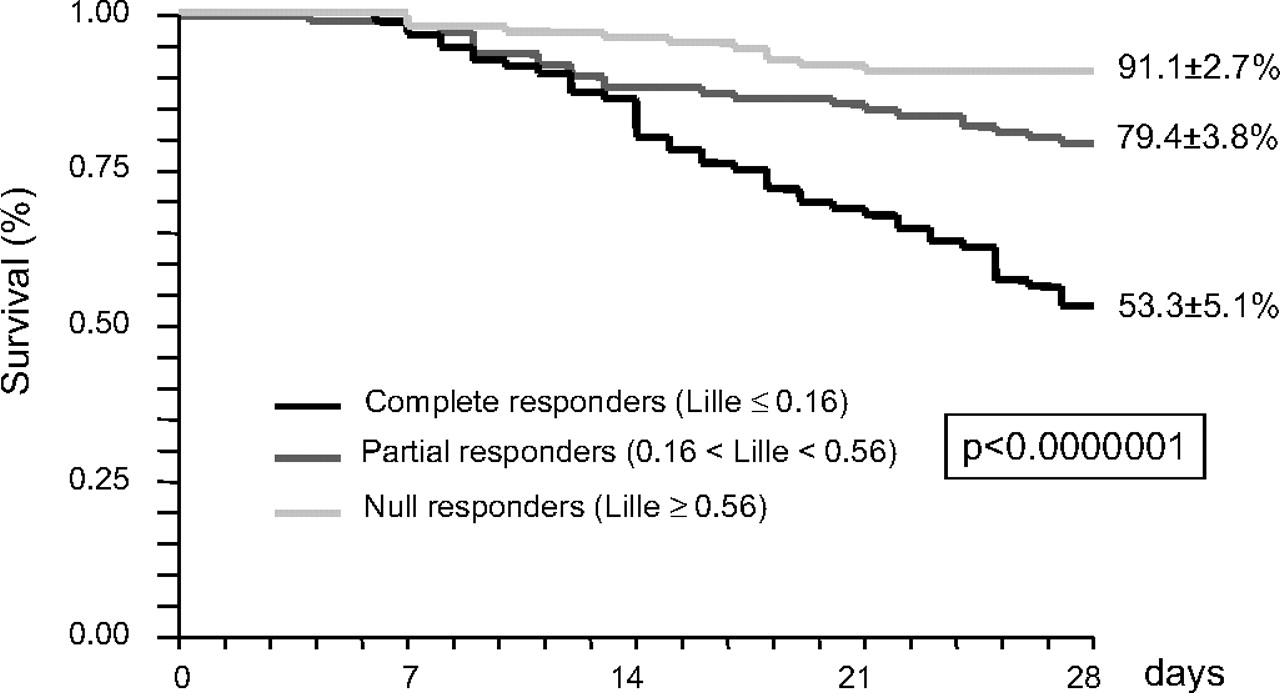
Probability of 28-day survival according to the distribution in percentiles of the Lille model: ≤0.16 (≤35th percentile), 0.16–0.56 (35th–70th percentile) and ≥0.56 (≥70th percentile). Survival between the groups differed significantly.

{kind=link}
{kind=link}
{kind=link}
Estimated 28-day survival according to treatment in (A) complete responders (Lille score ≤0.16), (B) partial responders (Lille score 0.16–0.56) and (C) null responders (Lille score ≥0.56).
Discussion
This analysis of individual patient data from five recent RCTs12–14 16 17 of corticosteroid treatment in patients with severe AH, which included more than 400 randomised patients, confirmed the efficacy of corticosteroids. Using the Lille model, the improved survival with corticosteroid treatment was restricted to patients classified as partial or complete responders. The present study confirms the need for modifying corticosteroid therapy according to the response after 1 week of treatment.
Data that aids clinicians in the management of severe AH are warranted. Indeed, a recent survey showed that the therapeutic approach of clinicians is heterogeneous, but not the assessment of disease severity.29 Indeed, 94% of hepatologists use DF for scoring AH severity since they consider severe AH an appropriate indication for short-term treatment.29 Our finding that corticosteroids improved 28-day survival in severe AH supports their use in this setting.
Early improvement in bilirubin and liver function are useful for predicting short-term survival in patients with severe AH treated or not with corticosteroids.25 30 Corticosteroid-treated patients had earlier and more substantial improvement in liver function, as assessed by the Lille model, a score which integrates early improvement into its formula. In our original publication describing the Lille model we found that a cut-off value of 0.45 separated patients who would and would not benefit from corticosteroid treatment. In the current study we re-evaluated the Lille score as a predictor of response to corticosteroids and re-confirmed that subjects with a Lille score ≥0.45 did not respond to corticosteroid treatment. However, the use of a single cut-off is too restrictive and does not permit identification of patients with intermediate risk of death. In the current analysis patients were classified according to the percentile distribution of their Lille score to avoid an arbitrary cut-off. This approach identified three patterns of responses (complete, partial and null) with significant differences in the risk of death. Using this classification, we showed that the survival impact of corticosteroids was significant in complete and partial responders but was negligible in null responders. This new classification raises questions concerning management of severe AH. It is speculated that corticosteroids may be sufficient in complete responders and that novel pharmacological therapies are relevant for intermediate responders, but that liver transplantation might be considered appropriate in null responders selected using criteria such as age, absence of other morbidities, social integration and the existence of family members able to support the patient through a liver transplantation programme.31
In summary, the present study confirms recent American Association for the Study of Liver Diseases guidelines recommending glucocorticosteroids for patients with severe AH.32 Management of such patients can be enhanced by assessment of their response using the Lille model.
References
Footnotes
Funding The cost of this study was borne by the authors' institutions.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest