Article Text

Abstract
Objective Ulcerative colitis is associated with increased interleukin 13 (IL-13) production by natural killer T cells. Taking advantage of the inhibitory actions of interferon β on IL-13 expression, this proof-of-concept study aimed to show that decreasing IL-13 production is associated with clinical improvement of ulcerative colitis symptoms.
Design Open-label interventional drug trial.
Setting Outpatient clinical research hospital.
Patients Adult patients with active ulcerative colitis (Short Clinical Colitis Activity Index (SCCAI)≥5).
Interventions Treatment with 30 μg IM interferon-β-1a (Avonex) weekly for 12 weeks with 6 month follow-up.
Main outcome measures Clinical response was defined as ≥3 point drop in the SCCAI for at least two consecutive monitoring visits, and cytokine production was measured in cultured peripheral blood and lamina propria mononuclear cells (LPMC) before and after treatment.
Results 11 of 16 patients were clinical responders, and 4 were in remission (SCCAI ≤ 2) at the end of treatment. Rectal bleeding subscores improved dramatically by week 4 (38% with frank bleeding vs 87% pretreatment). Increased IL-13 production by LPMC T cells fell significantly in clinical responders (690±99 vs 297±58 pg/ml p=0.015) but was unchanged in non-responders (542±83 vs 510±39 pg/ml). In addition, non-responders had significantly higher production of IL-17 and IL-6 pre-treatment compared to responders.
Conclusions Interferon-β-1a induces clinical response and remission in a large subset of patients with ulcerative colitis that is associated with significant inhibition of IL-13 production. In addition, increased IL-17 and IL-6 production is associated with no response to interferon-β. These data provide a proof-of-concept that IL-13 is an effector cytokine in ulcerative colitis and should be a target for novel therapies.
- Interleukin-13
- colitis
- ulcerative
- interferon-beta
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Ulcerative colitis is associated with excess mucosal IL-13 production by NKT cells.
Type I interferons can block IL-13 production by human T cells.
IL-13 is directly toxic to gut epithelium and increases permeability.
What are the new findings?
Only patients with ulcerative colitis responding to interferon-β-1a had a significant decrease in mucosal T cell IL-13 production after treatment.
Primary non-response of patients with ulcerative colitis to interferon-β-1a was associated with high baseline levels of IL-17 and IL-6 production.
No other significant decreases in inflammatory cytokines accompanied clinical improvement after interferon-β-1a treatment.
How might it impact on clinical practice in the foreseeable future?
These data should encourage further testing of novel agents specifically targeting IL-13 for efficacy in ulcerative colitis.
Studies of IL-17 expression in ulcerative colitis may identify a subset a patients with unique therapeutic requirements and disease determinants.
Introduction
The inflammation of ulcerative colitis has recently been shown to be associated with excess production of IL-13 in both oxazolone colitis and a mouse model of ulcerative colitis, as well as in ulcerative colitis occurring in humans.1 In oxazolone colitis, interleukin 13 (IL-13) produced by an invariant NKT cell population in the lamina propria is a prominent feature of the gut inflammation and, indeed, the inflammation can be prevented by NKT cell depletion or IL-13 immuno-neutralisation.2 In patients with ulcerative colitis, NKT cells (here, a non-invariant subset) are also present which serve as a source of increased IL-13 production, in sharp contrast to patients with Crohn's disease or healthy individuals that lack a similar IL-13-producing cell population.3 Consistent with its role as an effector cytokine in ulcerative colitis, IL-13 has been shown to enhance NKT cell cytotoxicity for epithelial cells and, in addition, can directly damage gut epithelial cells and/or increase epithelial barrier permeability.4 These findings suggest that strategies that diminish the production of this cytokine or inhibit its signalling mechanism offer a novel approach to the treatment of ulcerative colitis.
Type I interferons (α and β) possess properties that would make them leading candidate agents to target IL-13 function. First, type I interferons have been shown to inhibit IL-13 production and secretion by human T cells.5 6 Second, type I interferons have been shown to block IL-4 and IL-13 signalling events in human CD4 T cells via interferon-induced expression of SOCS proteins.7 Lastly, there is evidence that type I interferons can counter inflammation by induction of the regulatory cytokine IL-10 production or by enhancing the activity of regulatory T cells.8–11
These findings and/or the success of type I interferon in the amelioration of other inflammatory diseases have led to several open-label and placebo-controlled clinical trials designed to evaluate the therapeutic efficacy of this agent in ulcerative colitis. However, these trials were inconclusive because type I interferon treatment gave rise to a range of efficacies across the different agents, doses, durations of treatment, and populations studied.12–16 One possible reason for these mixed results is that patients differ with respect to how they respond to type I interferon, as recently suggested by the study of the efficacy of this agent in multiple sclerosis.17 We therefore conducted a study of the effect of interferon β on ulcerative colitis inflammation to determine the relation between its therapeutic effect and its effect on IL-13 production or the production of other cytokines.
Materials and methods
Patients
Patients were enrolled at the NIH Clinical Center under NIAID IRB approved protocol 03-I-0019 (NCT00048347 http://www.clinicaltrials.gov/). Eligible adult patients had a verifiable diagnosis of ulcerative colitis (endoscopic or histologic) and a Simple Clinical Colitis Activity Index (SCCAI) score ≥5. Acceptable concomitant colitis medications included stable doses of mesalamine drugs, prednisone (≤25 mg/day or prednisone equivalent), azathioprine or 6-mercaptopurine and probiotics. Exclusion criteria included pregnant or nursing women, use of any biological drug or methotrexate, ciclosporin, tacrolimus, thalidomide, or mycophenolate mofetil within 4 months of treatment, concomitant use of highly hepatotoxic drugs, active autoimmune disease or infection, or a history of major depression.
Study protocol
After giving informed consent and following a 14-day screening period, eligible patients received interferon-β-1a (Avonex, Biogen) 30 μg/week SC for 12 weeks. Clinical status was assessed on days 8, 15, 22 and 28, and biochemical and haematological parameters were assessed on days 4, 8, 11, 15, 22 and 28. Clinical response was recorded if the SCCAI score fell at least three points from baseline, and remission was defined as SCCAI score ≤2 points. A patient was considered a responder if he/she reported either a clinical response for at least two consecutive visits during the first 12 weeks or a remission for at least two consecutive visits during treatment or within 3 months of follow-up. Patients were followed for up to 24 weeks after the final injection of interferon-β-1a, assessed at weeks 4, 8, 16 and 24 for safety monitoring. Colonoscopy was performed just prior to the first injection and within 48 h after the final injection. Biopsy specimens were restricted to areas of endoscopically active inflammation (or to previously active rectosigmoid mucosa in settings where endoscopic healing had occurred following treatment).
Patients were eligible for retreatment if they had previously reported a remission and then experienced pre-treatment symptom levels even if it was beyond the 6 month follow-up period.
Cytokine measurement
Peripheral blood mononuclear cells were prepared from 50 ml whole blood using Ficoll–sodium diatrizoate gradient centrifugation. CD4 cells were further enriched from peripheral blood using CD4 columns (R&D Systems, Minneapolis, Minnesota, USA). Lamina propria mononuclear cells were prepared as previously described.3 Cells were immediately cultured and stimulated for 48 h with antibodies (1 μg/ml) against CD2 and CD28 (to elicit T cell responses) or with Staphylococcus, Cowans I (SAC) (Pansorbin beads, CalBiochem) or Lipopolysaccharide plus IFN-γ and CD40L trimer (to elicit macrophage responses). Culture supernatant cytokine concentrations were determined using multiplex bead Luminex100 instrumentation (Luminex Corporation, Austin, Texas, USA) with Lincoplex assay kits (LINCO Research, Inc. St. Charles, Missouri, USA). The assays were performed and analysed, using a Logistic-5PL regression method, with the Bio-Plex manager 3.0 software. The coefficient of variation for both intra- and inter-assay variability was 10–15%.
Statistical analysis
Changes in cytokine production and cell populations were analysed in an exploratory fashion. Differences between means within groups (baseline and post-treatment results in responders, for instance) were tested using a paired t test and differences between groups (post-treatment results for responders and non-responders, for instance) were tested using a non-paired t test and categorical demographic and side effect data were tested using Fisher's exact test (InStat, GraphPad Software, San Diego, California, USA). In some instances due to the small sample size, significance testing was repeated using non-parametric Mann–Whitney testing to assess the robustness of the results.
Results
Patient characteristics
Eighteen patients were enrolled in this study, and 16 completed the protocol, seven women and nine men. Two other patients were not included due to screen failure and early voluntary withdrawal. The mean age was 39.4±4.3 years (range 17–68); one subject was enrolled as a minor at age 17 after approval from the IRB. The mean SSCAI score at baseline was 8.5±1.4 (range 6–11). Table 1 shows the summary of relevant demographic and exposure data.
Patient demographic and clinical information
Thirteen patients were continued on concomitant medications including prednisone, azathioprine, or a mesalamine drug. Three patients had been treated with infliximab, two with primary non-response and one with secondary non-response. There were no significant differences between the group of patients that reported a clinical response to interferon-β-1a and those with no response in terms of age, gender, age at diagnosis, duration of disease, location of disease, or use of concomitant medications.
Clinical response to interferon-β1a (IFN-β) administration in this study group
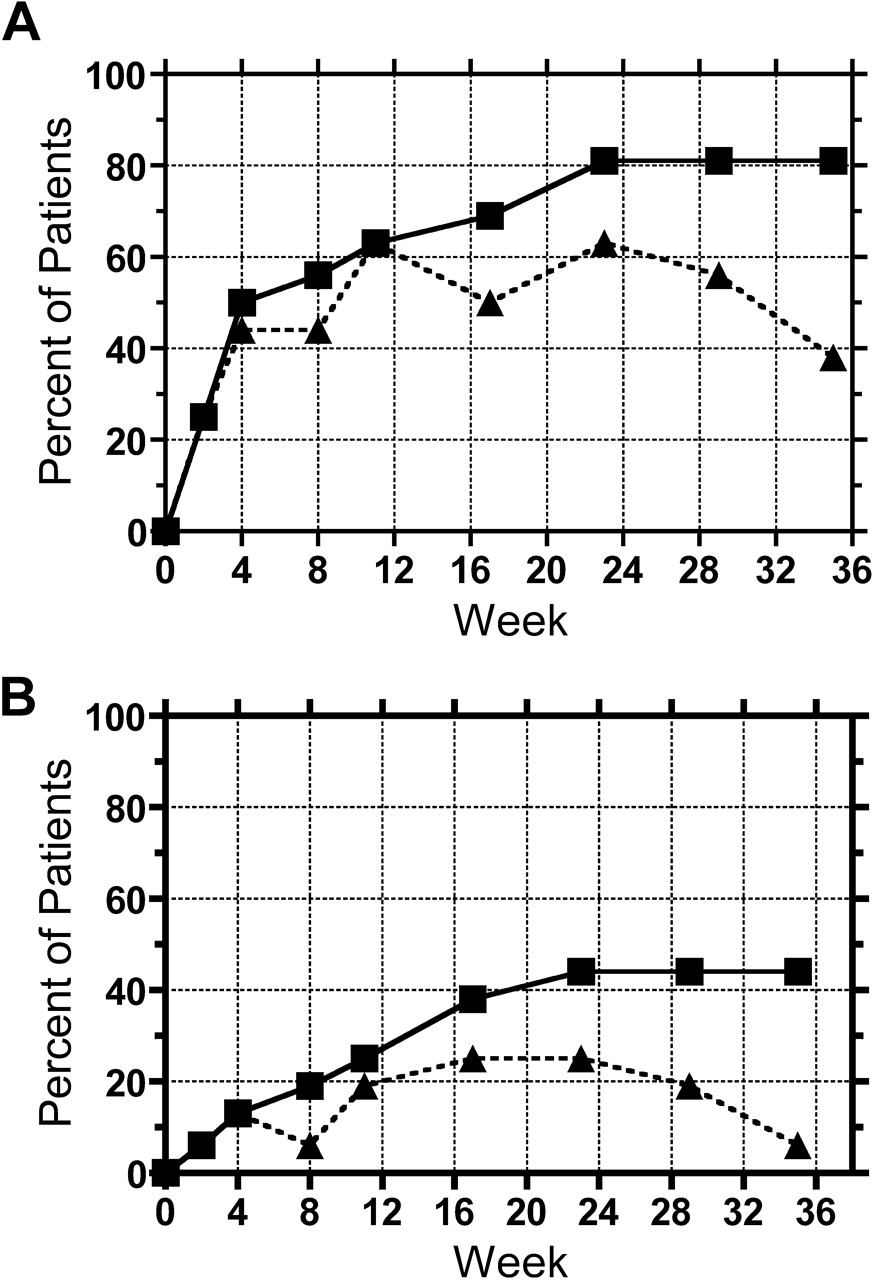
The clinical response assessment of patients with ulcerative colitis to treatment with interferon-β-1a was important for stratifying patients into groups so that effects on cytokine production, particularly the production of IL-13, could be associated with treatment effects. Seven of 16 (44%) patients reported a clinical response after four injections (week 4) and 10 (63%) were experiencing a clinical response at the end of 12 weeks' treatment (figure 1A). This high level of clinical response was durable to 18 weeks after treatment ended, falling to 38% at the end of follow-up, 24 weeks after the final dose of interferon. In all, 13 of the 16 patients (81%) reported a clinical response at any one time during their participation in the treatment or follow-up phase with more then half of these reporting a response in the first 4 weeks of treatment.
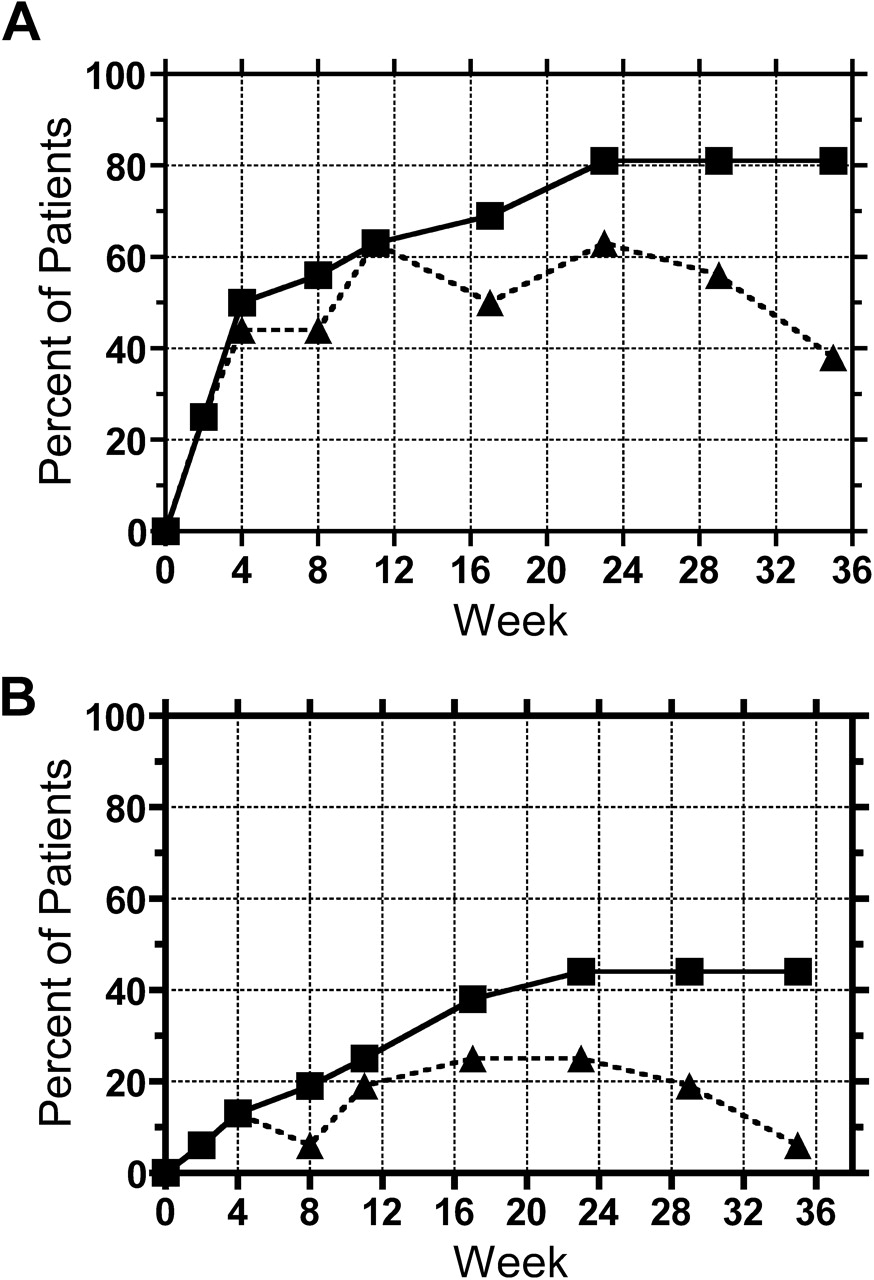
(A) Rate of clinical response to interferon-β-1a in ulcerative colitis patients. The per cent of patients reporting a clinical response at specific time points (dotted line) as well as the per cent of patients reporting a clinical response at any time up to a specific time point (solid line) are shown. (B) Rate of clinical remission (SCCAI ≤ 2) to interferon-β-1a in patients with ulcerative colitis. The per cent of patients reporting a clinical remission at specific time points (dotted line) as well as the per cent of patients reporting a clinical remission at any time up to a specific time point (solid line) are shown.
Remission was reported by two of 16 (13%) patients at week 4 and 3 (19%) at the end of 12 weeks' treatment (figure 1B). Furthermore, the per cent of patients reporting remission was stable during the follow-up period, ranging 19% to 25% over 4 months from the final dose of interferon-β. This remission rate was durable through 4 months of follow-up. In all, seven of the 16 patients (44%) reported experiencing remission level symptoms at any one time during the study. Based on our pre-defined criteria for categorisation as an overall responder, 11 patients were considered responders and five were considered non-responders.
The rectal bleeding subscore of the SCCAI showed a marked improvement during treatment. Using a point system of no bleeding=0, trace bleeding=1, occasionally frank bleeding=2, and usually frank bleeding=3, we observed that whereas 87% of patients reported occasionally frank or usually frank bleeding prior to treatment, this decreased to 38% at week 4 and 31% at the end of treatment (figure 2). This decreased rate of bleeding was maintained through 28 weeks after the final dose of interferon-β-1a. While formal endoscopic scoring of the degree of inflammation was not done, four patients in the responder group showed resolution of pre-treatment mucosal ulceration at the week 12 colonoscopy.

Distribution of rectal bleeding subscore reports from the SCCAI. The bars are patterned to represent the distribution of the degree of rectal bleeding reported by patients at specific time points. The four patterns correspond to (from bottom to top), no bleeding, trace bleeding, occasionally frank, and usually frank.
Four patients were retreated with a 12-week course of IFN-β-1a for a relapse of symptoms. All patients had experienced prolonged remission for 6 to 15 months prior to re-treatment. Three patients regained remission within 5 to 7 weeks of retreatment, reporting continuous improvement from 7 to >24 months after the final injection. A fourth patient regained a clinical response for 23 months.
In summary, in this small cohort of patients with ulcerative colitis, IFN-β-1a alone or in addition to an established treatment regimen was associated with a clinical response in a large majority of patients with ulcerative colitis. The beneficial effects were early in onset (50% experience a clinical response within 4 weeks) and durable for up to 4 months after stopping treatment. In many responding patients they included early cessation of bleeding associated in a substantial number of patients and evidence of mucosal healing. It was clear, however, that not all patients responded to administration of IFN-β; while this was unfortunate, it did allow an analysis of the relation of cytokine production with clinical response.
Safety and tolerability of interferon-β1a (IFN-β) administration in this study group
Thirteen of the 16 patients completed 100% of the scheduled study drug injections. Two non-responding patients discontinued the study drug, one after three injections and one after seven injections due to lack of response, and one patient completed nine injections when he decided to withdraw despite achieving a clinical response. Patients reported fever (63%) and mild flu-like symptoms (myalgias in 31%) after injections, but these were transient (usually resolving 4–5 h after the injection) and responded well to treatment with acetominophen. Only one patient reported limited fever after all injections, but the fever and myalgias resolved after the first two injections in most patients. There was no significant difference in reports of fever between responders and non-responders, but non-responders experienced myalgias at a significantly increased rate compared to responders (80% vs 12.5%, p=0.036). Isolated mild adverse events (one occurrence each) included eosinophilia, paraesthesias, epistaxis, headache, infected pilonidal cyst, palmar xeroderma, and recurrent C. difficile colitis.
Effect of IFN-β administration on cytokine production
Peripheral blood mononuclear cells and purified CD4+ T cells or lamina propria mononuclear cells obtained from patients just prior to treatment and within 48 h of the final IFN-β dose were stimulated in vitro for measurement of cytokine production (see Methods). As a group, IL-13 production by lamina propria T cells was significantly lower after the IFN-β-1a administration period, 337±64 pg/ml (mean±SEM), compared to production by cells sampled prior to this period, 598±104 p=0.016. Perhaps more importantly, when the patients were stratified according to their clinical response, only responders exhibited significant decreases in IL-13 production at these time points (690±99 pg/ml vs 297±58, p=0.015) compared to those patients not experiencing a clinical benefit (ie, non-responders) who showed no significant change during the same period (542±83 pg/ml vs 510±39) (figure 3). These IL-13 results were accompanied at the end of IFN-β-1a administration period by a non-significant trend towards decreased macrophage/APC-stimulated TNF-α production from responders compared to increased TNF-α production by cells from non-responders (table 2). Finally, there was no significant change in IL-10 production in either group as a result of IFN-β-1a administration, either by peripheral blood or lamina propria T cells.

IL-13 production by lamina propria t cells from ulcerative colitis patients before and after treatment with interferon-β-1a. (A) IL-13 in vitro secretion from anti-CD2 and anti-CD28-stimulated mucosal T cell cultures. These data represent the whole group of patients. (B) Mucosal T cell IL-13 secretion according to clinical response.
Cytokine production (pg/ml) by cultured peripheral blood and lamina propria mononuclear cells
Unexpectedly, two additional cytokine values correlated with the clinical effect of IFN-β-1a administration. IL-17 production by lamina propria T cells prior to IFN-β-1a administration was significantly higher in non-responders compared to responders 70±38 pg/ml vs 8±2, p=0.04) and, in general, cells from non-responders exhibited higher production of IL-17 at both time points. Similarly, peripheral blood macrophage/APC-stimulated IL-6 production prior to IFN-β-1a administration was significantly higher in non-responders compared to responders (133177±35259 pg/ml vs 42466±4982, p=0.006).
Based on previous studies one would predict that IFN-β administration would enhance IFN-γ production.18–20 This expectation was to some extent validated by the fact that both peripheral and lamina propria cells from both responders and non-responders generally showed a non-significant tendency to produce increased interferon-γ (1003±185 pg IFNγ/ml to 1438±210, 1688±647 to 2700±1455 from lamina propria T cells of responders and non-responders pre- and post-treatment respectively). By contrast, lamina propria T cells showed a tendency to exhibit lower IL-4 production (102±41 pg IL-4/ml to 30±10 and 78±69 to 24±22 from responders and non-responders pre- and post-treatment respectively) after the IFN-β-1a administration period.
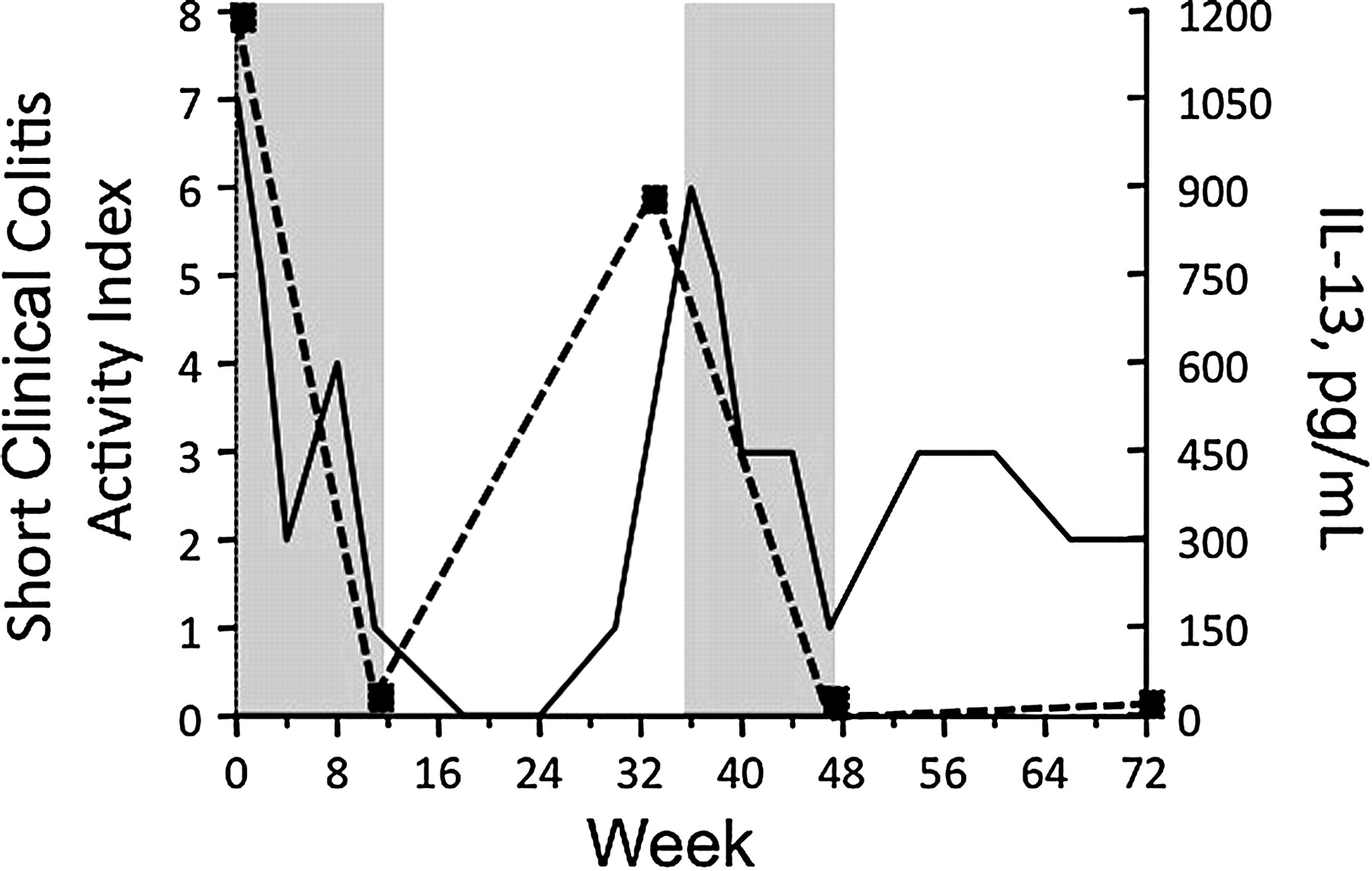
One patient who underwent two courses of IFN-β-1a administration followed by clinical remission each time provides additional evidence that this treatment efficacy is associated with decreased lamina propria T cell IL-13 production. As shown in figure 4, during an initial 12 week period of IFN-β-1a administration this patient's Short Clinical Colitis Activity Index charts his progression to clinical remission; over the same period production of IL-13 by lamina propria T cells dropped dramatically from 1211 pg/ml to 37 pg/ml. After a sustained remission lasting 16 weeks the patient relapsed clinically and lamina propria T cell production of IL-13 rebounded to 909 pg/ml. Following re-treatment with IFN-β-1a for 12 weeks, he again went into clinical remission and his lamina propria T cell production IL-13 production fell to a value too low to be detected. Remission then persisted for at least 6 months when repeat measurement of IL-13 production once again yielded a low value of 25 pg/ml.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of IL-13 production with ulcerative colitis clinical activity. This patient received two courses of interferon-β-1a. The solid line charts the SCCAI decreasing to clinical remission (SCCAI ≤2) during treatment (shaded area) and follow-up and indicating a relapse of symptoms at Week 36. Serial measurements of IL-13 production (dotted line) show that it declines with induction of remission and increased in conjunction with clinical relapse.
Discussion
The purpose of the present study was not to add or subtract from the already large amount of somewhat ambiguous data addressing the possible efficacy of IFN-β in ulcerative colitis treatment that are summarised below. Only well designed, blinded, placebo-controlled trials can settle this issue. Rather the purpose was to assess the effect of IFN-β on the cytokine profile of the patients with the aim of associating clinical response with changes in cytokine production. Of particular interest was the possible effect of IFN-β on IL-13 production by lamina propria T cells since, as already discussed, excessive IL-13 production is associated with ulcerative colitis inflammation, and IFN-β has been shown to lower IL-13 production in in vitro studies. We reasoned that if IFN-β-induced remission correlates with its ability to lower IL-13 production then we will have powerful new evidence that IL-13 is actually involved in the pathogenesis of ulcerative colitis.
Type I interferons have been used to treat ulcerative colitis in the past with variable results. Open-label studies were the first to support clinical efficacy for type I interferons in ulcerative colitis, following an initial observation of ulcerative colitis improvement in a patient treated with interferon-α for chronic hepatitis C.21 22 These studies led to a series of placebo-controlled trials using type I interferons in ulcerative colitis to test clinical efficacy. These studies used a variety of interferon preparations at different doses and durations of treatment and utilised several endpoints. In the initial study, Tilg et al treated 60 patients with active ulcerative colitis with pegylated interferon-α, 0.5 μg/kg, 1.0 μg/kg or placebo subcutaneously three times a week for 12 weeks, with an endpoint of remission (colitis actvitiy index ≤4) at 12 weeks. There was no significant difference in this outcome among groups (47.4% remission in the 0.5 μg/kg group, 33% in the 1.0 μg/kg and 35% in the placebo group). However, there was a 45–55% dropout rate across groups that hampered the analysis. In the second study, Nikolaus et al treated 17 patients with IFN-β-1a (Rebif) using a dose escalation design, 22 μg SC three times a week for 6 to 12 injections, increasing to 44 μg or 88 μg three times a week for an additional 6 to 12 injections versus placebo: endpoints included clinical response (≥3 point drop in Ulcerative Colitis Severity Score (UCSS) during treatment) and remission (UCSS=0 and endoscopy score=0); patients receiving interferon-β-1a experienced a 50% clinical response rate and 30% remission rate compared to 15% and 0% respectively in the placebo group.23 Unfortunately, this study was not powered to show that the outcome differences between the groups were significant. In the third study, Musch et al treated 91 patients with rIFN-β-1a (1 or 3 MIU SC or placebo three times a week for 8 weeks) and measured rates of clinical response (≥6 point drop in the Colitis Activity Index (CAI) and remission (CAI≤4).24 The response and remission rates for the 1 MIU group were both 56% while for the 3 MIU group these rates were 36% and 38% and the placebo group 34% and 30% respectively. This study had a 17.5% dropout rate and enrolment was stopped early. In the fourth and most recent study, Pena-Rossi et al treated 194 patients with IFN-β-1a (Rebif) 44 μg, 66 μg or placebo SC three times a week for 8 weeks; endpoints included clinical response (≥3 point drop in UCSS during treatment) and remission (UCSS=0 and endoscopy score=0 or 1).14 Patients receiving 44 μg and 66 μg interferon-β-1a experienced a 64% and 61% clinical response rate and 29% and 23% remission rate, respectively, while the placebo group experienced a 61% response and 23% remission rate. This apparently negative study is somewhat compromised by the fact the data were wildly divergent when patients were stratified by geographic location: studies of Croatian and Russian patients had high (endoscopically confirmed) remission and response rates with study drug (62.5% and 42.9%, respectively) and low remission and response rates with placebo (11.1% and 21.4%) while Western European sites experienced the opposite (eg, 18.8% drug remission versus 31.3% remission with placebo).
The disparity in the type of agent, dose, duration of treatment and the methods used to detect differences in outcomes between study groups in the placebo-controlled treatment studies cited above, makes it difficult to draw a solid conclusion regarding the overall clinical efficacy of type I interferon treatment in ulcerative colitis. Nevertheless these studies do provide intriguing signals of potential efficacy in certain patient subsets particularly when objective measures of response (endoscopic healing) were part of the study design. Assuming that a major disease mechanism at work in ulcerative colitis is the upregulation of IL-13 (based on the murine model of oxazolone colitis and excess production by mucosal NKT cells in humans with ulcerative colitis) one possible reason why the clinical efficacy of type I interferons in ulcerative colitis is inherently difficult to detect more broadly and consistently is that this agent may only indirectly modulate IL-13, and the ability to influence other primary factors driving the IL-13 response may differ from patient to patient (and is not easy to correlate with conventional clinical parameters as predictors of response). Of course, there also may not be a unifying pathological mechanism for all patients with ulcerative colitis that depends on excess IL-13 alone and so IL-13-targeted therapy may be highly successful in a just a subset of patients where the clinical efficacy of type I interferons would depend on the ability to down regulate this underlying cytokine response. Previous studies conducted well over a decade ago have provided evidence that type I interferons indeed down-regulate IL-13 responses in human peripheral blood cells from healthy subjects and that this downregulation is selective in that it affects IL-13 and IL-5 responses but not IL-4 responses.5 6 The latter suggests a unique mechanism of downregulation that quite remarkably has not yet been thoroughly investigated. Mechanisms that affect all Th2 responses (including IL-4 responses) such as induction of SOCS proteins which hinder STAT6 signalling or inhibition of GATA3 are therefore unlikely to be relevant, as are mechanisms involving immunosuppression which likewise are not IL-13-specific.7 25 One intriguing possibility arises from recent work suggesting that NKT cell production of IL-13 in experimental asthma is induced by IL-25 (IL-17E) and it is thus possible that type I interferons have a specific capacity to inhibit this cytokine.26
Regardless of which mechanism is found to ultimately explain the relation of interferon-β and IL-13, the fact that type 1 interferon treatment was only effective in some patients and not others provided us with the opportunity to test the proposition that efficacy of IFN-β in ulcerative colitis is in fact dependent on its ability to down-regulate IL-13 production by patient lamina propria cells. The data we obtained showed patients who are primary clinical responders to interferon-β-1a treatment exhibited significant decreases in lamina propria T cell production of IL-13 whereas, in contrast, patients who are primary clinical non-responders showed no decrease in IL-13 production. In that these data link clinical responsiveness to reduction of IL-13 production, they strongly support the notion that ulcerative colitis is due to an IL-13-mediated mechanism. Parenthetically, the reason for non-responsiveness to IFN-β treatment in some patients is not likely to be due to the development of neutralising antibodies since in this case we were observing a primary non-response to IFN-β administration that occurred before antibodies could have been generated. As discussed above while one mechanism of primary non-response may involve a defect related to the inhibitory effect of type 1 interferon on IL-13 responses, other mechanisms may involve other factors fundamental to a heterogeneity in disease pathogenesis. This could be due to factors either inherited or acquired, such as differences in the inflammatory milieu (see below). In addition to in vitro studies of the nature of this effect, studies of patients could help in defining patient responder status. These include studies that compare profiles of type I IFN-responsive genes in responders and non-responders in order to see whether INF-β-1a is biologically active in clinical non-responders or if its biologic activity changes from the beginning to the end of treatment.
One quite unexpected finding from this study was that positive clinical responses of patients with ulcerative colitis to interferon-β-1a could be predicted by the presence of significantly lower peripheral blood and lamina propria T cell production of IL-17A and IL-6 prior to treatment compared to non-responders. This was accompanied by the fact that interferon-β-1a administration had no effect on the IL-17 production despite previous work suggesting that it should be inhibited by type I interferons.27 28 These findings suggest that patients with ulcerative colitis with a low Th17 cytokine profile represent a subset who are more receptive to IFN-β therapy and are in accord with a recent report that there is a subset of multiple sclerosis patients within the group of non-responders to IFNβ who demonstrate high levels of IL-17F and endogenous IFN-β.17 Both findings may have a commonality in the hypothesis that success of IFN-β treatment in ulcerative colitis depends upon whether or not IL-13 elevation is driven by IL-17 and/or whether Th17 responses can be controlled.
In summary, the data from this study provide a proof-of-concept that IL-13 is an effector cytokine driving inflammation in ulcerative colitis and that IL-13 represents an important target for anti-cytokine strategies in ulcerative colitis. In addition, these findings suggest that IFN-β administration, by virtue of its capacity to inhibit IL-13 (production and activity) leads to an early decrease in rectal bleeding and induction of mucosal healing by ameliorating the detrimental effect of IL-13 on epithelial cells and the gut epithelial barrier.
References
Footnotes
See Commentary, p 430
Linked articles 229138.
Funding This project has been funded by the Division of Intramural Research, NIAID, the NIH Clinical Center and the National Cancer Institute under contract N01-CO-12400.
Competing interests PM has received consultant fees from Biogen-Idec.
Ethics approval This study was conducted with the approval of the NIH Intramural NIAID IRB.
Provenance and peer review Not commissioned; externally peer reviewed.