Article Text

Abstract
Objective After focal endoscopic resection (ER) of high-grade dysplasia (HGD) or early cancer (EC) in Barrett's oesophagus (BO), eradication of all remaining BO reduces the recurrence risk. The aim of this study was to compare the safety of stepwise radical ER (SRER) versus focal ER followed by radiofrequency ablation (RFA) for complete eradication of BO containing HGD/EC.
Methods A multicentre randomised clinical trial was carried out in three tertiary centres. Patients with BO ≤5 cm containing HGD/EC were randomised to SRER or ER/RFA. Patients in the SRER group underwent piecemeal ER of 50% of BO followed by serial ER. Patients in the ER/RFA group underwent focal ER for visible lesions followed by serial RFA. Follow-up endoscopy with biopsies (four-quadrant/2 cm BO) was performed at 6 and 12 months and then annually. The main outcome measures were: stenosis rate; complications; complete histological response for neoplasia (CR-neoplasia); and complete histological response for intestinal metaplasia (CR-IM).
Results CR-neoplasia was achieved in 25/25 (100%) SRER and in 21/22 (96%) ER/RFA patients. CR-IM was achieved in 23 (92%) SRER and 21 (96%) ER/RFA patients. The stenosis rate was significantly higher in SRER (88%) versus ER/RFA (14%; p<0.001), resulting in more therapeutic sessions in SRER (6 vs 3; p<0.001) due to dilations. After median 24 months follow-up, one SRER patient had recurrence of EC, requiring ER.
Conclusions In patients with BO ≤5 cm containing HGD/EC, SRER and ER/RFA achieved comparably high rates of CR-IM and CR-neoplasia. However, SRER was associated with a higher number of complications and therapeutic sessions. For these patients, a combined endoscopic approach of focal ER followed by RFA may thus be preferred over SRER.
Clinical trial number NTR1337.
- Barrett's oesophagus
- radiofrequency ablation
- endoscopic resection
- dysplasia
- neoplasia
- cancer
- endoscopic procedures
Statistics from Altmetric.com
- Barrett's oesophagus
- radiofrequency ablation
- endoscopic resection
- dysplasia
- neoplasia
- cancer
- endoscopic procedures
Significance of this study
What is already known about this subject?
Stepwise radical endoscopic resection (SRER) is safe and effective for early Barrett's neoplasia, but is associated with oesophageal stenosis.
Focal endoscopic resection (ER) followed by radiofrequency ablation (RFA) is safe and effective for early Barrett's neoplasia, but does not yield a complete specimen for histological evaluation.
What are the new findings?
SRER resulted in a higher rate of oesophageal stenosis as compared with focal ER followed by RFA.
SRER required a higher total number of therapeutic sessions due to dilation sessions for oesophageal stenoses.
How might it impact on clinical practice in the foreseeable future?
For patients with early Barrett's neoplasia a combined endoscopic approach of focal ER followed by RFA may be preferred over SRER.
Introduction
In Barrett's oesophagus (BO), the normal squamous oesophageal epithelium has been replaced by a columnar epithelium containing specialised intestinal metaplasia (IM), as a result of chronic gastro-oesophageal reflux.1 BO is an important risk factor for the development of oesophageal adenocarcinoma, a cancer with a rapidly rising incidence in the western world.2 High-grade dysplasia (HGD) and early cancer (EC) limited to the mucosa in BO can be effectively treated by endoscopic means, without the need for surgery. Endoscopic resection (ER) is the basis of endoscopic treatment. ER allows for removal of focal lesions within the BO and provides a specimen for histological evaluation which is imperative for optimal patient management: patients with HGD/EC can be managed endoscopically given their low risk of local lymph node involvement, whereas patients with lesions invading deep into the submucosa should be considered for oesophagectomy and lymph node dissection.3 However, after focal ER alone, up to 30% of patients will develop metachronous lesions in the residual BO segment during follow-up.4–6 Therefore, complete eradication of the residual BO is recommended.7–9 Currently, the two most promising strategies for complete BO eradication are stepwise radical endoscopic resection (SRER) and radiofrequency ablation (RFA).
SRER is a technique in which the complete BO segment is removed in consecutive ER sessions. Retrieval of the entire BO segment for histological assessment is ideal, as it may permit referral to surgery for advanced lesions. Single-centre studies have shown excellent results of SRER for HGD/EC with eradication of all neoplasia (CR-neoplasia) in 76–100% and complete eradication of all intestinal metaplasia (CR-IM) in 68–100%.10–15 An important limitation of SRER is the rate of complications, such as oesophageal stenosis requiring dilation, which occurs in up to 56% of cases.10–15
RFA is a new technique for endoscopic eradication of BO that is characterised by controlled and uniform thermal ablation. Several studies have shown that RFA, with and without prior ER, is an effective treatment for HGD/EC, with eradication of all neoplasia in 81–100% and complete removal of IM in 74–100%.16–20 RFA has demonstrated a favourable safety profile, with oesophageal stenosis occurring in only 0–6% of cases.16–20 RFA, however, does not yield a histological specimen; therefore, it is imperative that all visible abnormalities are removed by focal ER prior to RFA to guarantee optimal staging and to ensure that RFA is applied to flat mucosa only.9
The aim of this prospective randomised clinical trial was to compare the safety and efficacy of endoscopic treatment of BO (≤5 cm) containing HGD/EC using either SRER or RFA after focal ER of visible abnormalities.
Patients and methods
Selection criteria
Patients were eligible if they met the following criteria: (1) age between 18 and 85 years; (2) BO length ≤5 cm; (3) HGD and/or EC in BO in specimens obtained at two separate endoscopies; (4) no signs of deep submucosal invasion, regional lymph node involvement or distant metastases on endoscopic ultrasonography (EUS) and CT of thorax and abdomen (in the case of EC); (5) no prior endoscopic treatment of BO other than a single prior ER for staging; (6) in the case of a prior diagnostic ER, specimens with a negative deep resection margin, no deep submucosal invasion (≥T1sm2), no lymphatic/vascular invasive growth and no poorly or undifferentiated cancer (G3–G4); and (7) written informed consent.
Endoscopic investigation and staging
Pre-assessment consisted of two high-resolution endoscopies (GIF-Q160/GIF-Q260FZ/GIF-H180, Olympus, Hamburg, Germany) with targeted biopsies of visible lesions and four-quadrant biopsies from every 1–2 cm of the Barrett's segment.21 Oesophageal landmarks were recorded according to the Prague C&M classification.22 Visible lesions were classified using the Paris classification.23 EUS was performed for T- and N-staging, and suspicious lymph nodes were sampled by fine needle aspiration. In the case of carcinoma, a CT scan of thorax and abdomen was made for M-staging. Only patients with lesions that were deemed ‘suspicious for submucosal invasion’ by the endoscopist, based on the macroscopic appearance, underwent a focal staging ER prior to randomisation. In all other patients with visible lesions, ER was performed after randomisation: in the SRER arm the lesion was removed together with the first 50% of the BO segment in the same session (to minimise the number of ER sessions and to avoid a more difficult ER at a later stage due to scarring at the site of the lesion), whereas in the RFA arm only a focal ER of the lesion was performed for staging and to render the mucosa flat prior to RFA.
Endoscopic resection
In both study groups, the ER-cap technique and the multiband mucosectomy (MBM) technique were used as described previously.24 25 Additionally, the use of the ‘simple snare’ technique was allowed.11
Stepwise radical endoscopic resection (SRER)
In SRER, the Barrett's segment was removed in consecutive sessions at 6–8 week intervals, with a maximum of four sessions, inclusive of the baseline ER (where applicable). In the initial SRER session, piecemeal ER of 50% of the circumference of the entire Barrett's segment was performed, inclusive of the visible abnormality if not yet removed in a diagnostic ER session.26 For short segment BO (length of circumferential BO (C) ≤1, maximal BO length (M) ≤3), SRER in a single session was allowed. In cases where small bridges of residual BO were left in situ between ER wounds, these were preferably removed with additional ER, but argon plasma coagulation (APC) of tissue bridges during SRER was also allowed (60–80 W for Erbe ICC200; 30–40 W for Erbe Vio; APC-probe 2200A, Erbe Elektromedizin, Tübingen, Germany).
If visible Barrett's mucosa was present after the maximum allowable SRER sessions, patients underwent escape treatment with RFA. Escape treatment with APC or hot biopsy forceps for areas of residual BO (<5 mm) was allowed to avoid an additional ER or RFA, or when ER was not possible.
Radiofrequency ablation (RFA)
Patients randomised to RFA underwent focal ER of visible abnormalities followed by RFA after 6–8 weeks, when the residual BO contained at the utmost HGD upon biopsy. RFA was performed using the HALO system (BÂRRX Medical, Sunnyvale, California, USA) as previously described.9 19 Primary circumferential ablation was performed using the HALO360 balloon catheter, with a double RFA delivery (12 J/cm2, 40 W/cm2) and a cleaning step in between two ablation passes to remove coagulum from the ablation zone and electrode surface. At subsequent RFA sessions, the HALO90 device was used for focal ablation of residual Barrett's tongues and islands <2 cm in length, and to ablate the squamocolumnar junction (‘Z-line’) circumferentially at the gastric folds. The HALO90 catheter consists of a small electrode that is fixed to the tip of the endoscope. Focal RFA was delivered twice to each area (15 J/cm2, 40 W/cm2), followed by a cleaning step and a second ablation pass, again delivering RFA twice.17
RFA was repeated every 2–3 months until complete endoscopic eradication of BO was acieved. In cases where BO persisted after four RFA sessions (≤2 HALO360 procedures), escape ER was performed using the MBM technique. For minute islands of unsuspicious BO (<5 mm), hot biopsy forceps treatment was allowed when this avoided an additional RFA session or escape ER.
Preprocedural and postprocedural care
All endoscopic procedures were performed on an outpatient basis using conscious sedation with midazolam and fentanyl, or pethidine, or monitored anaesthesia with propofol.27 After endoscopic treatment, patients were observed in the endoscopy unit for 4 h before being discharged to home with detailed instructions. During the study period, patients were administered esomeprazole 40 mg twice daily, with addition of ranitidine 300 mg at bedtime and sucralfate suspension 5 ml (200 mg/ml) four times a day for 14 days after every treatment session. Patients were allowed to take acetaminophen 500 mg (maximum 3 g per day) for postprocedural pain, or diclofenac suppositories 100 mg (maximum 200 mg per day) if not responding to acetaminophen.
Follow-up
After visible eradication of all BO was achieved, biopsies were taken from every four-quadrant/2 cm of the neosquamous epithelium throughout the original BO segment and immediately distal (<5 mm) to the neo-Z-line. When histological assessment of the biopsies showed complete eradication of IM (CR-IM) and early neoplasia (CR-neoplasia), patients were scheduled for follow-up high-resolution endoscopy with narrow band imaging and four-quadrant/2 cm biopsies at 6 months, 12 months and annually thereafter. Standard EUS was performed at 12 months of follow-up to exclude local lymph node metastasis. The duration of follow-up was defined as the time between the first treatment session and the most recent follow-up endoscopy.
Histological evaluation
All biopsies and ER specimens were routinely processed and were evaluated by a gastrointestinal pathologist. For the purpose of this study, all pre-treatment biopsies, ER specimens and biopsies obtained at the first follow-up endoscopy were reviewed by a local expert pathologist at each centre with extensive experience in Barrett's neoplasia. The study pathologists were blinded to study group assignment. Biopsies were assessed for the presence of IM and grade of dysplasia using the revised Vienna classification (IM without dysplasia, indefinite for dysplasia (ID), LGD, HGD or cancer).28 29 ER specimens were evaluated for infiltration depth, vertical resection margins, tumour differentiation or grade of dysplasia, and lymphatic/vascular invasive growth. During follow-up, biopsies of neosquamous epithelium were assessed for the presence of IM at or below the surface (subsquamous intestinal metaplasia or buried Barrett's).
Outcome parameters
Based on previous studies we expected that SRER and ER/RFA would be equally effective in the removal of neoplasia and IM, yet that SRER would result in a higher rate of oesophageal stenosis as compared with RFA.16 17 30
The primary outcome parameter was the rate of symptomatic oesophageal stenosis.
Secondary outcome parameters were:
CR-neoplasia, defined as absence of any neoplasia, including LGD and ID in all biopsies obtained at the first follow-up endoscopy.
CR-IM, defined as absence of IM in all biopsies, including biopsies obtained immediately distal to the neo-Z-line obtained at the first follow-up endoscopy.
Rate of complications other than stenosis.
Number of treatment sessions required to achieve CR-neoplasia and CR-IM inclusive of escape treatment and treatment for complications.
Proportion of patients with CR-neoplasia at the last follow-up endoscopy.
Proportion of patients with CR-IM at the last follow-up endoscopy.
Need for additional treatment for recurrent neoplasia during follow-up.
To classify stenosis and other complications, the following definitions were used: ‘acute’, during the procedure; ‘early’, <48 h; ‘late’, >48 h; graded as ‘mild’, unscheduled hospital admission, hospitalisation <3 days, haemoglobin (Hb) drop <3 g/dl, no need for transfusion; ‘moderate’, hospitalisation 4–10 days, <4 units blood transfusion, need for repeat endoscopic treatment including dilation; ‘severe’, hospitalisation >10 days, intensive care unit (ICU) admission, need for surgery, ≥4 units blood transfusion or, in the case of stenosis, >5 dilations, stent placement or incision therapy; ‘fatal’, death attributable to the procedure <30 days or longer with continuous hospitalisation. Only events requiring any intervention were scored.
Ethical considerations, sample size and statistics
The study protocol was approved by the local medical ethics committee of each study centre (NTR1337, http://www.trialregister.nl/). Written informed consent was obtained from all participants. Patients were randomised in each centre according to a computer-generated randomisation sequence per centre, which was concealed from the researchers who screened and enrolled patients by the use of sequentially numbered, sealed opaque envelopes. All procedures were attended by a study monitor (CS) who prospectively collected all relevant data on standardised case record forms, and data were entered into a dedicated database.
Sample size calculations were based on the assumption that SRER would result in a higher oesophageal stenosis rate compared with RFA. No differences in CR-neoplasia, CR-IM, or severe complications were expected based on previous studies.16 17 30 To confirm the hypothesis that SRER results in a significantly higher stenosis rate, with estimated stenosis rates of 52% for SRER30 31 and 4% for RFA,16 17 22 patients were needed in each arm, accounting for a drop-out rate of 10%, resulting in a total study population of 44 patients (α=0.05, β=0.10, two-sided testing).
Data analysis was performed using SPSS statistical software package (SPSS version 16.0.2). Mean (±SD) was used for normal distribution and median (IQR) was used for skewed distribution. The Fisher exact test and Mann–Whitney U test were used to compare groups when appropriate. Differences were considered statistically significant if p≤0.05. To calculate CIs the Confidence Interval Analysis package was used (Confidence Interval Analysis Version 2.2.0). For sample size calculation and random sequence generation, nQuery Adviser (Version 7) was used.
Results
Patients
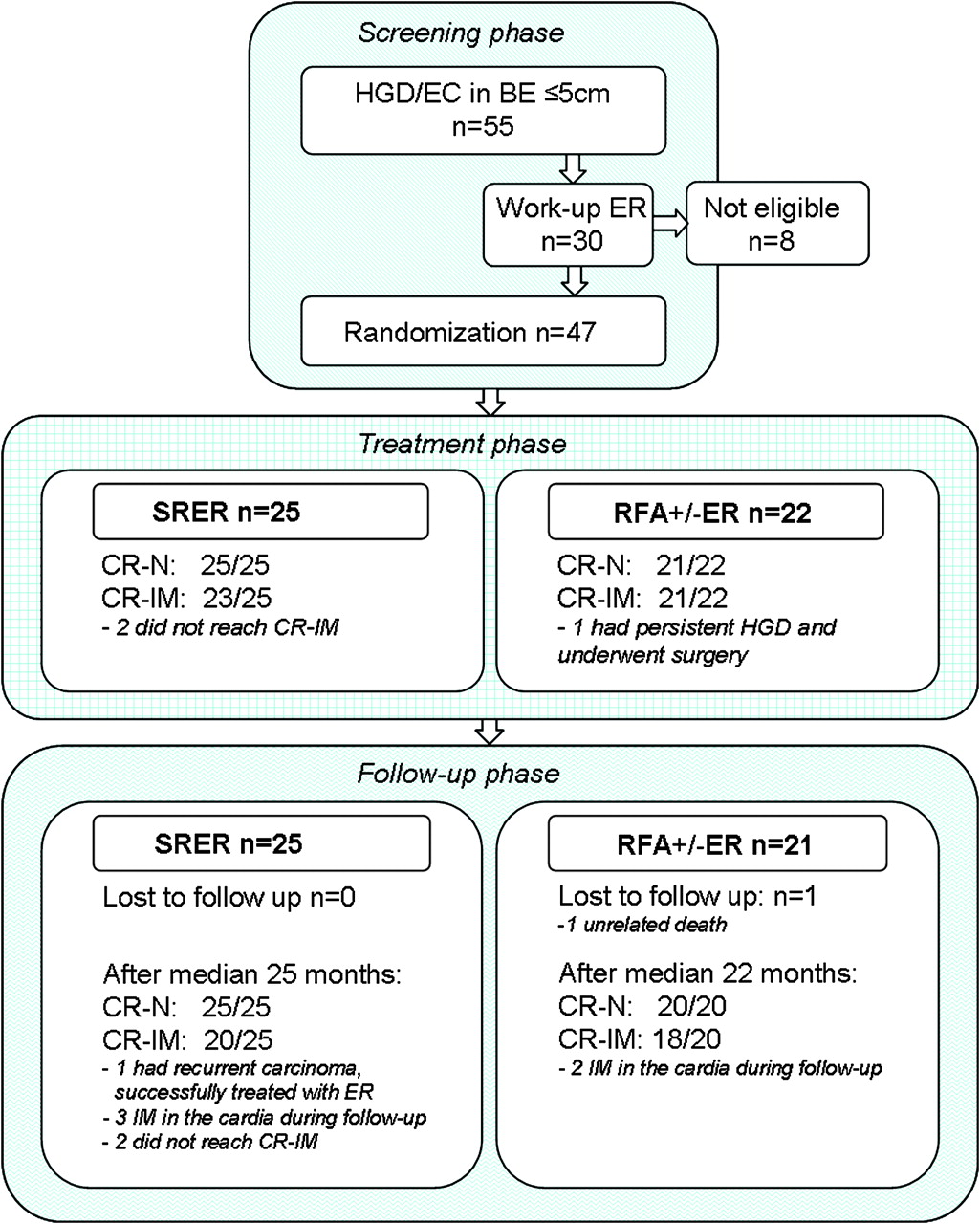
Between April 2006 and April 2008, 55 patients with HGD/EC in a BO segment ≤5 cm underwent endoscopic investigation and staging for eligibility in the Academic Medical Center (Amsterdam, The Netherlands), Sint Antonius Hospital (Nieuwegein, The Netherlands) or the University Medical Center Hamburg-Eppendorf (Hamburg, Germany) (figure 1).

Patient enrolment and outcomes of patients treated with stepwise radical endoscopic resection (SRER) or endoscopic resection (ER) followed by radiofrequency ablation (RFA). BE, Barrett's oesophagus; CR-IM, complete response for intestinal metaplasia; CR-N, complete response for neoplasia; EC, early cancer; HGD, high-grade dysplasia.
Staging ER was performed prior to randomisation in 30 of 55 patients. Eight patients were not eligible for study for the following reasons: non-lifting of the lesion (n=2), no residual IM after ER (n=2), lymphatic tumour invasion in the ER specimen (n=1), residual carcinoma after two ERs (n=1), tumour at the deep margin (n=1) and acute ER-related oesophageal perforation (n=1). In two patients, EUS-guided fine needle aspiration of local lymph nodes was performed, and malignancy was excluded. Therefore, 47 of 55 screened patients fulfilled all study criteria after investigation and staging and were randomised to SRER (n=25) or RFA (n=22) (figure 1). The baseline characteristics of patients in both groups were similar (table 1).
Baseline patient characteristics
Complete remission of neoplasia and IM
CR-neoplasia was reached in all 25 patients (100%) after SRER and in 21 of 22 patients (96%) after ER/RFA (figure 1, table 2). CR-IM was achieved in 23 of 25 patients (92%) after SRER and 21 of 22 patients (96%) after ER/RFA (figures 2 and 3).
Outcome parameters and characteristics of endoscopic treatment

Stepwise radical endoscopic resection (SRER) for Barrett's oesophagus (BO) containing early neoplasia. (A) Lesion in BO (C <1, M3); (B) lesion with narrow band imaging (NBI); (C) endoscopic resection (ER) in three pieces (T1m3 adenocarcinoma); (D) healed resection wound; (E) remaining BO is removed with ER (four pieces); (F) resection wound extending into the hiatal hernia; (G) no visible residual BO and non-symptomatic oesophageal narrowing due to scarring; (H) corresponding image (NBI); (I) normal gastro-oesophageal junction (NBI).

{kind=link}
{kind=link}
{kind=link}
Radiofrequency ablation (RFA) preceded by endoscopic resection (ER) for early neoplasia in a patient with Barrett's oesophagus (BO). (A) Lesion in BO (C3, M5); (B) lesion delineated by coagulation markers; (C) ER in four pieces (T1m2 adenocarcinoma); (D) healed resection wound; (E) circumferential balloon-based RFA; (F) removal of coagulum between two ablation passes; (G) small remaining BO islands; (H) focal RFA of BO islands using the HALO90 catheter; (I) circumferential HALO90 ablation of the gastro-oesophageal junction; (J and K) complete removal of BO (narrow band imaging); (K) corresponding image; (L) normal gastro-oesophageal junction.
The single ER/RFA patient who failed to achieve CR-neoplasia and CR-IM underwent oesophagectomy to treat persistent HGD. The choice of surgery in preference to escape ER was due to the fact that previous ER made it impossible to perform additional ER. The surgical resection specimen showed residual HGD, while 20 lymph nodes were negative for malignancy. Two SRER patients failed to achieve CR-IM: one patient had a small rim of visible BO without dysplasia after two SRER sessions, but because of post-ER stricturing and poor healing after previous treatment no further treatment was performed, and one patient had persistent IM at the neo-Z-line without visible BO after two SRER sessions and RFA.
Oesophageal stenosis
Symptomatic oesophageal stenosis occurred in 22 of 25 (88%) SRER patients versus 3 of 21 (14%) RFA patients (RR=6.2 (95% CI 2 to 18; p<0.001) (table 2). All RFA patients who developed stenosis had undergone ER of relatively large lesions prior to RFA, with stenosis developing at the ER sites. In the SRER group, five stenoses were graded as severe complications; all other stenoses were graded as moderate complications. Most stenoses resolved upon balloon or bougie dilation, while one patient required incision therapy in addition to dilation. The median number of dilations was 4 (range 1–19, IQR 2–5) for post-SRER stenoses and 3 (range 1–4) for post-ER/RFA stenoses (p=0.39).
Acute complications
There was one severe acute complication in the SRER arm: a perforation occurred during ER, which was treated non-surgically with a covered stent. After stent removal and healing, SRER treatment was continued. Additionally, in the SRER arm, five mild acute bleedings occurred and were treated endoscopically by hot biopsy forceps, epinephrine injection and/or clip placement. Acute complications in the ER/RFA arm were mild and included two bleedings immediately after ER treated endoscopically with a clip and APC, and one superficial mucosal laceration during RFA that required no intervention, but prevented a second ablation pass (table 2).
Early complications
There was one bleeding in the SRER arm, graded as a moderate complication, in a patient presenting with haematemesis within 24 h after ER due to an arterial bleed from the resection wound that was treated by placement of a clip. After blood transfusion (Hb level drop from 7 to 5.2 mmol/l, 2 units of packed red blood cells transfused), the patient was discharged.
Late complications other than stenosis
There was one delayed bleed after RFA, graded as a moderate complication. This patient developed melaena after re-initiating oral anticoagulation therapy (acenocoumarol) for atrial fibrillation 2 weeks after focal RFA. Upper endoscopy showed a visible vessel in the treatment area, which was injected with epinephrine (1:10 000) and coagulated using bipolar electrocoagulation. The patient underwent blood transfusion (baseline Hb level unknown, Hb level after bleeding 5.7 mmol/l, 2 units of packed red blood cells transfused).
Number of treatment sessions
SRER patients
For SRER, the MBM technique (n=12), ER-cap technique (n=8) or MBM and ER-cap (n=5) were used. In seven patients, SRER was performed in a single session. A median of 5 (IQR 2–7) resections was performed per session. Per patient, a total median number of 10 (IQR 6–13) resection specimens were removed. In three SRER patients (3/25, 12%), APC was used to treat residual BO tissue bridges between resection wounds. Escape treatment to reach CR-neoplasia and CR-IM was required in eight patients (8/25, 32%): RFA for residual BO because post-SRER scarring and stenosis impeded further ER (n=5); APC for residual BO because stricturing did not allow for passage of an ER-cap or HALO90 catheter (n=1); or APC for ablation of tiny islands <5 mm (n=2).
ER/RFA patients
Prior to RFA 18/22 patients underwent ER of a visible lesion with the ER-cap technique (n=11), the MBM technique (n=6) or the simple snare technique (n=1). Escape treatment to reach CR-neoplasia and CR-IM was performed in four patients (4/21, 19%): hot biopsy forceps to remove a BO island (<2 mm, n=2); ER for residual visible BO (n=1) (histology showed no IM or dysplasia); and ER plus APC (n=1) for an elevated island of BO (histology showed a radically removed T1sm1 cancer).
The median number of therapeutic sessions to achieve CR-neoplasia and CR-IM was not significantly different in both groups (SRER 2 (IQR 1-3) vs RFA 3 (IQR 3–4); p=0.07). However, due to stenosis requiring dilations, the total number of endoscopic interventions per patient was significantly higher in SRER (6 (IQR 3–9) vs 3 (IQR 3–4); p<0.001). The median duration of the treatment period was not significantly different between SRER and RFA (5 (IQR 3–13) vs 8 (IQR 5–10) months, respectively; p=0.26).
Follow-up: persistence of CR-neoplasia and CR-IM
Median follow-up from initial treatment to March 2010 was 24 months (IQR 18–29) overall, and median follow-up from the final treatment session to March 2010 was 18 months (IQR 11–23), with a median of 3 (IQR 3–4) follow-up endoscopies for both groups (table 3). Forty-five patients (96%) remained under endoscopic follow-up. Two of 47 patients were not available for endoscopic follow-up: one ER/RFA patient failed CR-neoplasia and underwent surgery; another ER/RFA patient died 4 months after reaching CR-neoplasia and CR-IM due to myocardial infarction (unrelated death).
Follow-up (FU) after endoscopic treatment
In the SRER group, one patient (4%) was diagnosed with cancer at the neo-Z-line 16 months after SRER and was treated with ER. The resection specimen showed T1m3 carcinoma. Follow-up endoscopy after 4 months revealed no dysplasia or cancer. In the ER/RFA group, no recurrence of neoplasia was observed during follow-up.
None of the patients who reached CR-IM during the treatment phase showed endoscopic signs of recurrence of BO on any follow-up endoscopy. At the last follow-up endoscopy, histological signs of IM were found in three SRER and two RFA patients: all had repeated findings of IM at the neo-Z-line and were considered failures for CR-IM at the last follow-up endoscopy (p=1.00). Six other patients had a focal IM in a single biopsy during a single follow-up endoscopy without being reproduced at subsequent endoscopies, including four SRER patients (two focal IM at the neo-Z-line, two buried BO glands in neosquamous biopsies) and two RFA patients (focal IM at the neo-Z-line). These six patients were not considered as failures for CR-IM at the last follow-up endoscopy.
Discussion
This multicentre randomised trial showed that in patients with BO ≤5 cm containing HGD or EC, both SRER and focal ER plus RFA are highly effective, with high rates of CR-neoplasia and CR-IM. After a median follow-up of 24 months after initial treatment, recurrences of neoplasia or BO were rare for both groups. Regarding safety, SRER and RFA resulted in comparably low rates of acute complications, but SRER carried a significantly higher risk for the late complication of oesophageal stenosis, resulting in more procedures per patient in the SRER group due to dilation sessions. In addition, significantly more complications were graded as ‘severe’ in the SRER arm (1 perforation and 5 stenoses) with no severe complications in the ER/RFA arm.
The most important finding of the study is a significantly higher stenosis rate of 88% in SRER compared with 14% after ER/RFA. Although all SRER stenoses were effectively treated with dilation, 5 of 22 SRER stenoses were quite resistant to treatment (>5 dilatations and need for combination treatment). In addition, dilation of these stenoses may cause significant complications as illustrated by a recent multicentre SRER study that reported two perforations after dilation for an SRER-induced stenosis.31 More importantly, treatment of SRER-induced stenoses doubled the total number of endoscopic procedures in the SRER group compared with the ER/RFA group. In the ER/RFA group, the three patients with stenosis all had undergone widespread ER prior to RFA to remove all visible lesions. Studies of patients treated with RFA, not preceded by ER, have reported stenosis rates ≤6%.32 33 This suggests that ER, not RFA, was the primary cause of stenosis in these patients.
Oesophageal stenosis is a recognised complication of SRER of BO, varying from 2% to 56%.10–15 31 Compared with other series, the 88% stenosis rate after SRER in our study is quite high. An explanation may be that the three study centres prospectively screened all patients with BO ≤5 cm with HGD/EC and offered participation to all eligible patients. In contrast, other retrospective series may have included less complicated cases, for example with a shorter BO segment or BO mainly consisting of tongues. It has been shown that the stenosis rate after SRER increases with the length of the BO.31 34 We assume that our patient population had a relatively long circumferential extent (median C2, M4, IQR C1–3, M2–5) which may account for the relatively high stenosis rate. Our rigorous follow-up in this prospective study may also have contributed to the observed stenosis rate, with all stenoses and dilations being fully recognised and transparently reported.
Although no significant differences were found in eradication rates of neoplasia and IM, we cannot conclude that SRER and ER/RFA are equally effective: the current study was powered to evaluate the difference in symptomatic stenosis rate between both treatment modalities, based on previous experience of the study centres. Uncontrolled studies have reported success rates for CR-neoplasia of SRER and ER/RFA varying between 88% and 100%.10–12 14–19 35 If a difference of >10% in CR-neoplasia for one of both treatment modalities would be clinically relevant and assuming a 90% success rate for both treatment modalities, 155 patients would have been necessary in each treatment arm to be able to prove equivalence or non-equivalence. Given the relative rareness of HGD/EC in BO this is an unrealistic number of patients for a randomised study in this field. In addition, it is debatable whether it would be ethical or clinically relevant to perform such a study, knowing that combined ER and RFA has an excellent success rate with a low risk for symptomatic stenosis.
In our study there was one recurrent carcinoma (4%) in the SRER arm, located at the neo-Z-line of a patient that had focal IM detected at this site at a previous follow-up endoscopy. This is in agreement with a recent multicentre SRER study of 169 patients in which all recurrences of HGD/EC (2%) were located at the neo-Z-line.31 This suggests that IM in the Z-line after SRER may be a relevant finding, and may predict recurrence of neoplasia. On the other hand, our patients underwent extensive biopsy sampling during follow-up (median 12 biopsies obtained from the neo-Z-line per patient). Mostly, focal IM was observed in a single biopsy during a single endoscopy and not reproduced during subsequent endoscopies. Studies have shown that IM of the cardia can be detected in biopsies of 25% of the normal population, and these studies generally obtained fewer biopsies than were obtained during follow-up in our patients.36 More data are therefore needed to address the relevance of IM distal to the Z-line.
There are two additional arguments in favour of a strategy of focal ER followed by RFA rather than SRER for the complete removal of BO. First, we studied only those patients with BO ≤5 cm. If we had studied longer segments, it is possible that the SRER group would have encountered further complications and failures. In contrast, recent data have shown that RFA is also effective and safe in longer segment BO, even in patients with BO ≥10 cm.37 Secondly, combination treatment with ER and RFA is technically less demanding than SRER.
Our study protocol allowed for escape treatment to achieve complete BO eradication after SRER or ER/RFA. Since RFA does not result in significant scarring of the oesophagus, escape ER after RFA has been incorporated in the treatment algorithm in other studies.16 17 19 Accordingly, in other SRER studies, ablation therapy has been used to treat small areas of residual BO that cannot be resected due to scarring after previous ERs.10 12 14 31 Although it can be argued that escape treatment may influence the results, we feel that comparing SRER and ER/RFA inclusive of escape treatment in both treatment arms makes our results better translatable to clinical practice.
A limitation of this study concerns its external validity: treatment was carried out in centres with a tertiary referral function for endoscopic treatment of early Barrett's neoplasia. Hence, patients were treated by endoscopists highly experienced in SRER and RFA treatment. The outcomes of our study may therefore not apply to general practice. However, because of the low incidence of early Barrett's neoplasia in the general population, it is desirable to centralise care for these patients in well-trained expert centres.
In summary, this randomised multicentre trial showed that SRER and focal ER plus RFA are highly effective in the treatment of patients with BO ≤5 cm containing early neoplasia. SRER, however, resulted in a significantly higher stenosis rate than ER/RFA, and consequently required a higher number of therapeutic sessions due to dilations. Therefore, for patients with BO containing early neoplasia, a combined approach of focal ER for visible lesions followed by RFA for complete eradication of the remaining BO may be preferred.
References
Footnotes
Funding BÂRRX Medical, Sunnyvale, CA, USA.
Competing interests Grant support from BÂRRX Medical. JJGHMB received unrestricted grants from Astra Zeneca, Olympus Medical and Cook Medical.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Academic Medical Center (Amsterdam, The Netherlands), Sint Antonius Hospital (Nieuwegein, The Netherlands) and University Medical Center Hamburg-Eppendorf (Hamburg, Germany).
Provenance and peer review Not commissioned; externally peer reviewed.