Article Text

Abstract
Objective External fistulas represent a disabling manifestation of Crohn's disease with a difficult curability and a high relapse rate despite a large therapeutic armamentarium. Stem cell therapy is a novel and promising approach for treatment of chronic inflammatory conditions. We therefore investigated the feasibility, safety and efficacy of serial intrafistular injections of autologous bone marrow-derived mesenchymal stromal cells (MSCs) in the treatment of fistulising Crohn's disease.
Patients and methods We enrolled 12 consecutive outpatients (eight males, median age 32 years) refractory to or unsuitable for current available therapies. MSCs were isolated from bone marrow and expanded ex vivo to be used for both therapeutic and experimental purposes. Ten patients (two refused) received intrafistular MSC injections (median 4) scheduled every 4 weeks, and were monitored by surgical, MRI and endoscopic evaluation for 12 months afterwards. The feasibility of obtaining at least 50×106 MSCs from each patient, the appearance of adverse events, and the efficacy in terms of fistula healing and reduction of both Crohn's disease and perianal disease activity indexes were evaluated. In addition, the percentage of both mucosal and circulating regulatory T cells expressing FoxP3, and the ability of MSCs to influence mucosal T cell apoptosis were investigated.
Results MSC expansion was successful in all cases; sustained complete closure (seven cases) or incomplete closure (three cases) of fistula tracks with a parallel reduction of Crohn's disease and perianal disease activity indexes (p<0.01 for both), and rectal mucosal healing were induced by treatment without any adverse effects. The percentage of mucosal and circulating regulatory T cells significantly increased during the treatment and remained stable until the end of follow up (p<0.0001 and p<0.01, respectively). Furthermore, MSCs have been proven to affect mucosal T cell apoptotic rate.
Conclusions Locally injected MSCs represent a feasible, safe and beneficial therapy in refractory fistulising Crohn's disease.
- Crohn's disease fistulas
- mesenchymal stromal cells
- regulatory T cells
- apoptosis
- crohn's disease
- stem cells
- T lymphocytes
Statistics from Altmetric.com
- Crohn's disease fistulas
- mesenchymal stromal cells
- regulatory T cells
- apoptosis
- crohn's disease
- stem cells
- T lymphocytes
Significance of this study
What is already known about this subject?
Fistulising Crohn's disease is usually difficult to treat and carries a high relapse rate despite a large therapeutic armamentarium.
Stem cell therapy is a novel therapeutic approach in immune-mediated conditions and, because of their peculiar biological properties, mesenchymal stem (stromal hereafter) cells represent a promising tool for regenerative medicine and chronic inflammatory diseases.
Recent experimental and clinical evidence has shown the efficacy of mesenchymal stromal cells (MSCs) in healing the intestinal lesions of patients with acute graft-versus-host disease.
What are the new findings?
The feasibility of ex vivo expanding autologous bone marrow-derived mesenchymal stromal cells and the safety of their intrafistular injections in patients with Crohn's disease.
The efficacy of this new therapeutic approach.
The promoting effect of mesenchymal stromal cells on in vivo differentiation of regulatory T cells.
How might it impact on clinical practice in the foreseeable future?
It provides the rationale for validating the efficacy of MSC local injection in patients with fistulising Crohn's disease in a phase III, multicentre, randomised study.
It could greatly improve the health-related quality of life of this kind of patient.
Introduction
Crohn's disease is a chronic inflammatory bowel disease caused by dysregulation of immune tolerance towards intestinal bacteria in genetically susceptible individuals.1 Among the clinical phenotypes,2 the fistulising behaviour is the most challenging to treat despite the large number of options available, including anti-inflammatory drugs, antibiotics, immunosuppressants, and surgery.3 Biological agents, such as anti-tumour necrosis factor (TNF)-α antibodies, became first-line treatment during the last decade, but the benefit in terms of sustained fistula healing has proven to be limited.3
Originally isolated from bone marrow (BM), mesenchymal stromal cells (MSCs) were subsequently found in several other adult and fetal tissues, and proven to home to inflamed sites and to repair injured tissues.4 5 Because of their ability to influence both innate and adaptive immune response, as well as to the lack of immunogenicity,4 6 they are now considered a promising tool in immunoregulatory and regenerative cell therapy even in an allogeneic setting.5 7 Indeed, MSCs have been employed in phase I/II clinical trials with striking results obtained in terms of resolution of steroid-refractory acute graft-versus-host disease8 and promotion of haematopoietic engraftment.9 Remarkably, no adverse effects have been reported after MSC administration, and large multicentre randomised clinical trials are warranted. As far as inflammatory bowel disease is concerned, MSCs administered intraperitoneally,10 intravenously,11 or directly into colonic tissue surrounding mucosal lesions12 proved to be of benefit in experimental models of Crohn colitis. In humans, intrafistular injections of adipose tissue-derived MSCs have been safely employed in a case series of Crohn's disease-associated fistulas,13 and proven successful to treat complex perianal fistulas of cryptoglandular origin or associated with Crohn's disease.14
On this basis, we evaluated the feasibility, safety and efficacy of serial intrafistular injections of autologous BM-derived MSCs in patients with refractory fistulising Crohn's disease. We preferred BM-derived MSCs, whose genetic stability had been assessed by conventional and molecular karyotyping,15 16 even though it should be pointed out that earlier concerns on the risk of malignant transformation after long-term ex vivo culture17–19 has now been attributed to cross-contamination with simultaneously handled tumour cell lines.20 21 Moreover, to increase the biological safety, MSC ex vivo expansion was carried out in the presence of human platelet lysate (PL) as a substitute for fetal calf serum to avoid putative transmission of zoonoses and potential sensitisation to animal proteins.22
Patients and methods
Study population and protocol
Starting from January 2007, we enrolled 12 consecutive patients with Crohn's disease with actively draining complex perianal fistulas,23 except one with multiple enterocutaneous fistulas, whose clinical features are shown in table 1. All patients had been unresponsive to or unsuitable for all previous medical treatment including biological agents (ie, anti-TNFα monoclonal antibodies) or unsuccessfully treated by surgery.
Patients' clinical features at enrolment
Patient assessment included: clinical examination, routine laboratory tests, lower endoscopy to determine the presence of rectal mucosa inflammation, MRI to delineate fistula track anatomy and the presence of complicating factors,24 surgical examination (anaesthesia was needed in only two cases) with abscess drainage and/or seton removal when present, calculation of Crohn's disease activity index (CDAI)25 and perianal disease activity index (PDAI),23 and detection of the three NOD2/CARD15 major variants (R702W, G908R, and 1007fsinsC)26 by restriction analysis.27 Pharmacological treatment was allowed at stable dosage at least in the 4 weeks before enrolment, that is BM harvest, and throughout the duration of the study. More in detail, all patients were taking mesalamine (800 mg t.i.d.) plus azathioprine (2.5 mg/kg body weight/daily), except two patients (#5 and #7) who had been taking mesalamine (800 mg t.i.d)+prednisone (10 mg per day), and another two patients (#2 and #10) who were only on mesalamine. When used, biological therapy had been stopped since enrolment.
The feasibility, safety and efficacy of serial intrafistular injections of autologous BM-derived MSCs were tested in these patients. Feasibility was defined as the ability to obtain at least 50×106 MSCs from each patient based on scale-up experiments performed in our laboratory.16 Safety was considered in terms of changes in vital signs and adverse reactions during the first 6 h after each cellular treatment, and during the following 12-month follow-up. Efficacy was assessed by a combination of clinical, surgical and imaging evaluations at the time of each treatment and 3, 6 and 12 months after the last procedure. With regard to clinical evaluation, both CDAI and PDAI scores were calculated, while for surgical evaluation, efficacy was reported as ‘remission’ when fistula tracks appeared closed (ie, inability to insert a cannula through the external opening and no drainage despite finger compression), or as ‘improvement’ when the number of draining fistulas was reduced by at least 50% from baseline and/or when no discharge upon finger compression was present.23 Absence or loss of response was defined as the persistence or recurrence of draining fistulas. Finally, for the MRI evaluation, a blinded radiologist reviewed all patients' images according to the categories (number of fistula tracks, location, extension, hyperintensity on T2-weighted images, collections and rectal wall involvement) and score proposed by van Assche et al.28
In addition, peripheral blood samples were collected at the time of BM harvest, as well as at each treatment and scheduled visits, while endoscopy was repeated 12 months after the end of treatment.
The protocol was approved by the Institutional Ethics Committee, and each patient gave written informed consent.
Preparation of MSCs and injection procedure
Fifty millilitres of BM were harvested from each patient and MSCs were prepared according to previously described methods9 except for 5% human PL which was employed instead of 10% fetal calf serum. For PL preparation, aliquots of 50 ml platelet-rich plasma, collected by apheresis, were obtained from healthy donors after written informed consent. PL aliquots were pooled in a single culture supplement for the generation and expansion of MSC.22 All procedures were carried out according to Good Manufacturing Practice protocols. After 48-h culture, non-adherent cells were removed and medium was replaced twice a week. MSCs were propagated until passage 3, when they were harvested and cryopreserved until use. MSC release criteria for clinical use were as follows: spindle-shape morphology, absence of contamination by pathogens, viability >90%, immune phenotype showing the expression of CD73, CD90, and CD105 surface molecules (>95%) and the absence of CD34, CD45, and CD31 markers (<5%). For therapeutic purposes, thawed MSCs were re-suspended in a solution of sodium chloride and human albumin 20% (3/1 v/v), at a concentration of 2×106 cells/ml in a sterile syringe.
Due to the presence of abscesses in all patients, a 2-week course of antibiotic therapy with ciprofloxacin 500 mg twice daily, ceftriaxone 1 g twice daily, and metronidazole 500 mg twice daily was given as temporary adjunctive therapy before the first injection procedure. All injections were performed in an outpatient setting, under local anaesthesia and in jack-knife position except for the patient with enterocutaneous fistulas who stayed supine. After disinfection and exploration of both perianal area and rectal ampulla, external openings and fistula tracks were identified and cleaned with saline solution by using malleable probes. The MSC suspension was then injected both into the lumen and the wall of the tracks, moving from the deep to the external side. Finally, a sterile bandage was applied and the patient was placed on bed rest for 6 h, during which time vital signs and possible adverse reactions were monitored. Injections were scheduled at 4-week intervals, with a median of 20×106 cells each time (range 15–30, roughly 1×106 MSCs/cm length of the track). This amount was doubled when tissue loss was vast, such as in patients #2 and #11. Each patient was examined a few days (≤3 days) before each treatment and 3, 6 and 12 months after the last one in order to diagnose and record possible adverse events and to monitor clinical efficacy. The injections were stopped when ‘remission’ or ‘improvement’ was achieved, or when autologous MSCs were no longer available.
MSC–T cells co-culture experiments
We collected multiple perendoscopic specimens from both macroscopically inflamed and non-inflamed areas of colonic mucosa of six out of the 12 patients at enrolment, since two patients dropped out, one patient had jejunal localisation, and in three cases (#1, #3, #5) a complete colonoscopy was not performed because of variable degree of stenosis in the rectosigmoid tract. According to the protocol reported by Ina and co-workers,29 biopsies were rinsed and incubated in a 24-cluster plate (Celbio) with 1 ml complete culture medium containing 20 U/ml interleukin (IL) 2 (Chiron, Emeryville, California, USA) for 3 weeks, with refreshing every 3 days. Cells were then harvested for both immune phenotyping (see below) and co-culture purposes. In the latter experiments, T cells (as assessed by flow cytometry demonstrating an almost pure, ie, >90%, CD3+ population, data not shown) were incubated in triplicate both in the absence and presence of autologous MSCs at a MSC/T cell ratio of 1:10. After 5 days, cells were washed and incubated in medium devoid of IL-2 for up to 48 h. Under such IL-2 deprivation, T cell apoptosis (early and late phase), necrosis and viability were evaluated after 3, 6, 24 and 48 h using the AnnexinV/Propidium Iodide kit (ApopTest FITC; DAKO, Glostrup, Denmark) following the manufacturer's instructions. At the end of the co-culture period, the supernatants were collected and stored at −20°C for cytokine profile analysis (see below).
Immune phenotyping
MSCs, circulating and mucosal mononuclear cells were analysed by flow-cytometry (FACSCanto, BD Biosciences; FACS Diva software; Milan, Italy) using the following FITC-, PE-, or PerCP-conjugated monoclonal antibodies: CD73, CD105 (Serotec, Kidlington, UK), CD90, CD34, CD45, CD31, CD19, CD3, CD16, CD56, CD4, CD25, HLA-DR (BD PharMingen, San Diego, California, USA). Intracellular staining for the transcription factor forkhead box P3 (FoxP3; eBioscience, San Diego, California, USA) was performed on circulating cells following the manufacturer's instructions and as previously reported.30
Immunohistochemistry
Mucosal FoxP3+ cells were evaluated by immunohistochemistry on formalin-fixed paraffin-embedded perendoscopic biopsies obtained from rectal ampulla and, when possible, also from both macroscopically inflamed and non-inflamed colonic areas of the enrolled patients before the beginning and 12 months after the end of the treatment. For this purpose, serial sections were stained with monoclonal antibodies directed against FoxP3 (Clone 236A/E7; eBioscience; San Diego, California, USA) and CD25 (Clone 4C9; Novocastra, Newcastle, UK), respectively, according to the manufacturer's instructions. Differential counts of FoxP3+ and CD25+ cells were independently estimated on high-power microscopic fields by two histopathologists and displayed in percentage of lamina propria mononuclear cells. Only cells showing strong nuclear reactivity were labelled as FoxP3+ positive.
ELISA assay
The following cytokines: IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12p70, IL-13, interferon (IFN) γ, and TNFα were assayed on patients' sera and supernatants of MSCs at passage 3, and of the MSC/T cell co-cultures by using the Thermo Scientific Searchlight Human Cytokine Array (Pierce, Rockford, IL, USA) following the manufacturer's instructions. Supernatants of BM-derived MSC at passage 3 from eight healthy subjects were also tested as controls.
Statistical analysis
The Student t test for paired data was employed to compare CDAI, PDAI, cytokine levels and percentage of CD4+CD25brightFoxP3+ cell subset. p<0.05 was considered significant.
Results
Feasibility, safety, efficacy
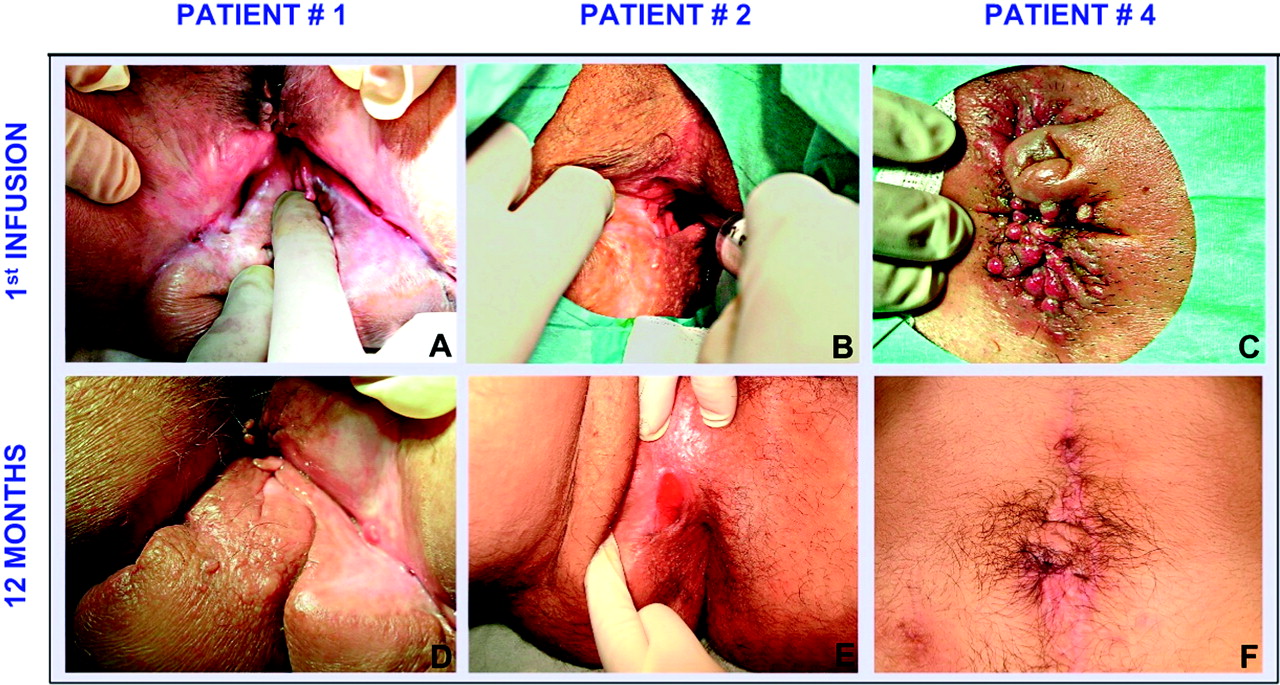
We obtained more than 50×106 BM-derived MSCs from each patient (median number at passage 3: 64×106, range 54–139). Two out of the 12 patients who underwent BM harvest did not receive treatment; one (#10, see table 1) decided to undergo cellular therapy only after any favourable outcome of the others (she has now had her first injection), and the second (#12) was planning to move abroad for work purposes. In these two cases and in patient #11, the genetic analysis of NOD2 mutations27 was not carried out. Remarkably, in all the other patients, except patient #7 (homozygous for R702W), we found that the NOD2 gene was wild-type.26 Of the ten patients who finished the study protocol, nine had complex perianal fistulas (two representative cases are shown in figure 1A,B), while the remaining patient (#4) carried multiple enterocutaneous fistulas involving the third jejunal loop just ahead of an entero-entero anastomosis, with bile juice causing severe cutaneous inflammation (figure 1C). Each patient underwent a median of four intrafistular injections (range 2–5), scheduled every 4 weeks. At surgical evaluation, 7/10 patients benefited from complete closure of fistula tracks (three representative cases are shown in figure 1D–F), while 3/10 (#3, #5, #8) experienced an ‘improvement’. Moreover, all patients showed a significant reduction of both CDAI (pre- and post-treatment median values: 294±49, range: 384–237, and 99±32, range: 150–50, at 12 months after the last procedure; p<0.001, figure 2A) and PDAI (pre- and post-treatment median values: 13.0±2.2, range: 16–11, and 4.5±2.4, range: 7–2, at 12 months after the last procedure; p<0.001, figure 2B) achieving disease remission (CDAI≤150, PDAI≤8) usually after the second procedure. When analysing the data for each variable of both indexes (figure 3A,B for CDAI and PDAI, respectively), it appears clear that some items (ie, general wellbeing and extraintestinal complications—which include fistulas—for CDAI and pain, discharge and type of perianal disease for PDAI) significantly contributed to the massive drop of the total score (p<0.01 for all). No case of persistence or recrudescence of draining fistulas was observed during the entire follow-up period, and the treatment was never stopped because of unavailability of autologous MSC. No changes in vital signs and no adverse events were recorded during the procedure and up to the end of the 6-h observation time, or during the 12-month follow-up period.

Three representative cases of fistula healing after local injections of mesenchymal stromal cells. Two patients had complex perianal fistulas (left and middle panels), and one had enterocutaneous fistulas (right panels) at the time of the first intrafistular injection of a suspension of autologous bone-marrow-derived mesenchymal stromal cells (A–C), and 12 months after the end of treatment (D–F). In detail, patient #1 (see table 1) had multiple draining external openings along the lines of previous surgical cuts (A); complete resolution of perineal inflammation, and closure of external openings that appear covered with normal epithelium are evident (D). Patient #2 (see table 1) had complex perianal fistulas unsuccessfully treated by surgical incisions with a vast loss of tissue (B); after treatment, closure of the external opening and appearance of regenerative tissue along the fistula track are clearly evident (E). Patient #4 (see table 1) carried multiple enterocutaneous fistulas draining enteric and bile juices causing severe skin inflammation (C); disappearance of inflammation and definitive closure of all the external openings are visible (F).
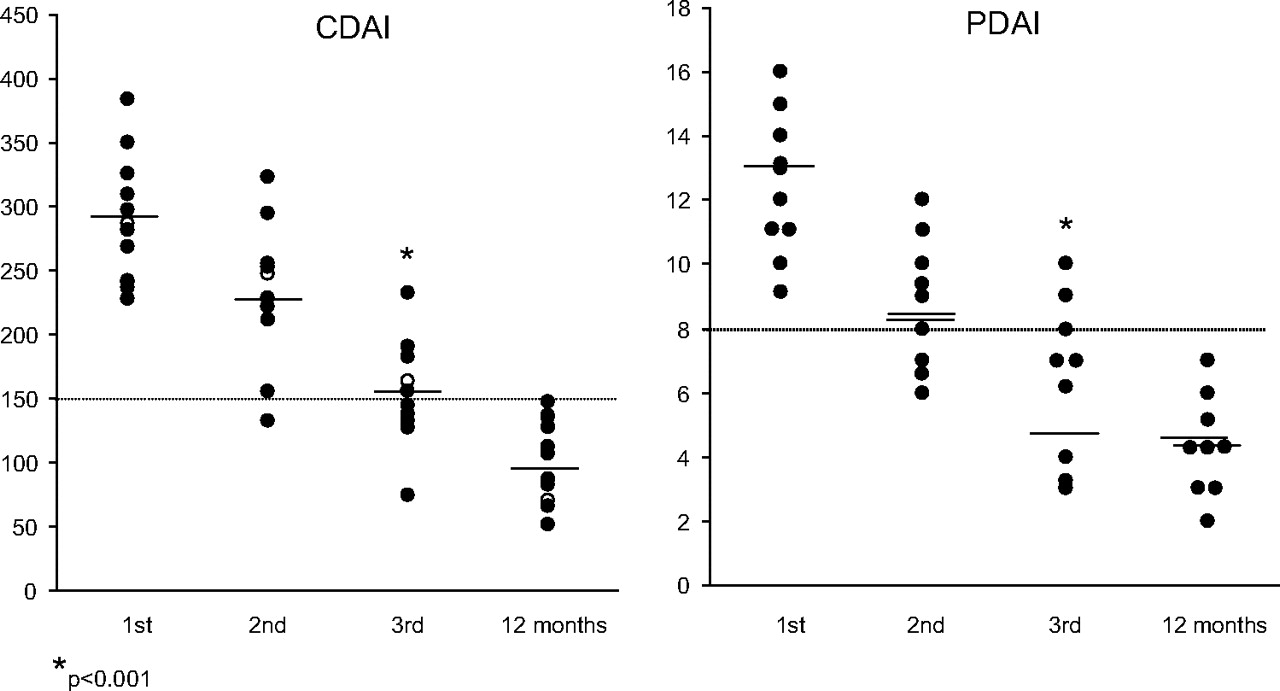
Representation of Crohn's disease activity index (CDAI) and perianal disease activity index (PDAI) score values throughout the study. The CDAI and PDAI values of each patient (the empty dots indicate patient #4, see table 1) at the time of the first (1st), second (2nd), third (3rd) injection of autologous bone marrow-derived mesenchymal stromal cells, and after 12 months follow-up (12 months) are shown in the left and right panel, respectively. A significant decrease of activity index was observed at the time of the third procedure with induction of remission (CDAI≤150 and PDAI≤8), which persisted after the 12-month follow-up. The values indicate mean±SD, the horizontal lines indicate the cut-off values between quiescent and active disease.

Representation of the values of Crohn's disease activity index (CDAI) and perianal disease activity index (PDAI) variables throughout the study. The values of each variable of both CDAI (3A) and PDAI (3B) at the time of the first (1st), second (2nd), third (3rd) injection of autologous bone marrow-derived mesenchymal stromal cells, and after the 12-month follow-up (12 months) are given. The values indicate mean±SD. At the third injection, general wellbeing and extraintestinal complications showed a value significantly lower that that found at time of the first injection. For comments see the text.
As regards the imaging study, MRI serial examinations provided a useful and precise description of fistula anatomy and complicating factors, and made it possible to follow the healing process (a representative case in figure 4A,B). In 7/10 cases a complete substitution of the fistula tracks with regenerative tissue without signs of fibrosis was clearly evident usually after the second injection onwards (a representative case in figure 4B), while in three patients (#3, #5, #8) the persistence of the main fistula tracks, even though of smaller size and without secondary branches, was found. Remarkably, the seven cases of fistula healing described at MRI study overlapped with those having fistula closure at surgical evaluation. However, this result does not indicate an agreement between the two methodologies in the assessment of fistulising Crohn's disease since the imaging examination gave a more accurate description in terms of number of tracks identified, anatomic connections, and complicating factors than surgical evaluation. In addition, the MRI study was useful in the preliminary establishment of the amount of cells needed for every injection. Finally, as regards the evaluation of serial patients' images according to van Assche et al,28 the categories whose score significantly decreased since the time of the third injection were hyperintensity, collections and rectal wall involvement (p<0.0001 for all), whereas the extension and number of fistula tracks was only slightly modified because usually only the branches of the main tracks completely disappeared, and no modification of the location was observed (figure 5).

Representative cases of fistula and mucosal healing. (A) Axial T1-weighted magnetic resonance image of a case of complex perianal fistulas (patient #1, see table 1) before treatment, showing a large fistula track extending from the rectum to the gluteal surface (black arrows) and a fluid collection (red arrow). (B) Axial T1-weighted image after administration of intravenous contrast medium showing a strong enhancement of the fistula track (black arrows) and replacement with regenerative tissue (red arrow) 12 months after the end of treatment. (C) A case of active rectal disease (patient #9, see table 1) as evident at the first endoscopy showing mucosal inflammation, friability, and longitudinal ulcers. (D) At the control examination 12 months after the end of the treatment, a healthy mucosa was clearly evident.

Representation of MRI score values throughout the study. The modification of the magnetic resonance imaging score for every category as proposed by van Assche (see reference28) at the first (1st), second (2nd), third (3rd) injection, and at the end of the 12-month follow-up (12 months) is shown. The values indicate mean±SD. At the third injection, hyperintensity, collections and rectal wall involvement showed a value significantly lower that that found at time of the first injection. For comments see the text.
To evaluate rectal mucosa, all patients with perianal Crohn's disease (9/10) underwent lower endoscopy before the first MSC injection, and an inflamed mucosa with oedema, friability, erosions and sometimes ulcers (a representative case is shown in figure 4C) was invariably present. In six of them, endoscopic examination reached the ileocaecal valve, demonstrating variable extension of active inflammation, while in three cases the examination (#1, #3, #5) was stopped between the rectal ampulla and the sigmoid tract due to some degree of luminal restriction. The examination was repeated in seven out of nine patients at the end of the follow-up period, and a healthy rectal mucosa with a normal vascular pattern was evident in all cases (a representative case is shown in figure 4D). Two patients (#6 and #11) refused because of their general wellbeing and absence of perianal active disease, and preferred to undergo endoscopy only in the event of relapse.
Regulatory T cells and cytokine levels
The percentage of FoxP3+ T cells found in rectal mucosa 12 months after the end of cellular treatment significantly increased (p<0.0001) compared to that observed before the start of therapy (figure 6A). Moreover, in those six patients in whom a total colonoscopy was performed, a slight increase in the percentage of regulatory T cells at the end of the follow-up period compared to the pre-treatment situation (7.2±3.1 vs 4.5±2.7, respectively) was observed in inflamed areas, whilst no difference was found in non-inflamed areas (3.5±2.1 vs 5.5±1.9, respectively). As expected, all FoxP3+ cells also resulted positive to anti-CD25 monoclonal antibody at serial sections (data not shown). Similarly, the serial immunophenotype characterisation of circulating T lymphocytes showed an increase in the number of T cells expressing a regulatory phenotype, that is CD4+CD25brightFoxP3+ cells, which became significant (p<0.01) after the second injection, as compared with the value at the beginning of treatment, and remained stable up to the end of the follow-up period (figure 6B). On the contrary, no modification in levels of serum cytokines was observed at any time point (data not shown).

Study of mucosal and peripheral blood regulatory T cells. (A) Immunohistochemical detection of FoxP3+ cells on the rectal mucosa of a representative case (patient #2, see table 1) before (left panel) and 12 months after the end of the cellular therapy (central panel) when an increase of the number of positive cells (those with black nuclei) is clearly evident (immunoperoxidase, ematoxilin counterstain; original magnification, ×200). Quantification of mucosal FoxP3+ T lymphocytes, expressed as mean percentage of mononuclear interstitial cells of lamina propria+SD, before (I) and 12 months after the end of the local cellular therapy (III) is given in the right panel. (A) Significant increase in the percentage of FoxP3+ cells was evident up to the 12-month follow-up. (B) Flow cytometric analysis of circulating FoxP3+ cells on gated CD4+CD25bright lymphocytes (filled histograms) of a representative case (patient #2, see table 1) before (left panel) and 12 months after the end of the cellular therapy (central panel) when an increase of the positive cell count is clearly evident. Quantification of circulating CD4+CD25brightFoxP3+ T lymphocytes, expressed as mean percentages+SD, at time of the first (I) and third intrafistular (II) injection of a suspension of autologous bone marrow-derived mesenchymal stromal cells (MSC), and 12 months after the end of the treatment (III) is given in the right panel. A significant increase in the percentage of CD4+CD25brightFoxP3+ cells was present from the third procedure onwards, and persisted up to the 12-month follow-up.
MSC-T cell co-culture experiments
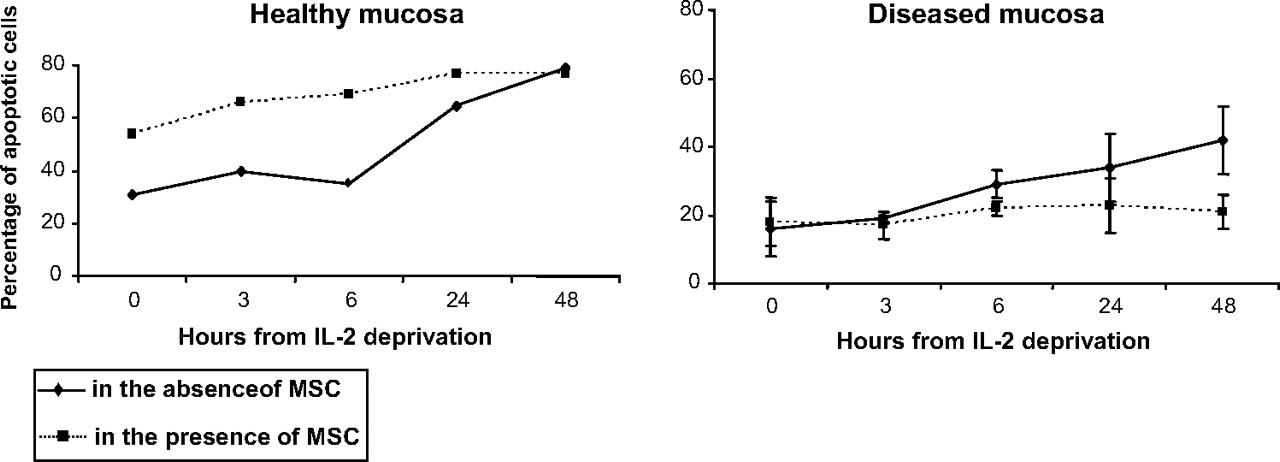
With the aim of investigating whether MSCs from patients with Crohn's disease have the ability to favour mucosal T-lymphocyte apoptosis, T cells obtained from both inflamed (diseased mucosa) and non-inflamed areas (healthy mucosa) at the first endoscopy were cultured for 5 days either in the presence or absence of autologous MSC, followed by 48 h of IL-2 deprivation, used as a pro-apoptotic stimulus. As expected,29 31 in the absence of MSC the apoptotic rate of T lymphocytes from healthy mucosa after 48 h of IL-2 deprivation was higher than that of T lymphocytes from diseased mucosa (figure 7). Co-culture of MSC with T lymphocytes from healthy mucosa induced a further striking increase in the apoptotic rate since the start of IL-2 deprivation, whilst it did not affect the percentage of apoptotic cells throughout the 48 h of IL-2 deprivation when T lymphocytes were collected from diseased mucosa (figure 7). A low percentage (<10%) of both necrotic and living cells was detected in all experimental conditions (data not shown). It is noteworthy that, in experiments performed with T cells from inflamed mucosa, we observed an unexpected progressive reduction of MSCs until their complete disappearance on day 4.

Mesenchymal stromal cell (MSC) and T cell apoptosis. The proportion of mucosal T cells at late phase of apoptosis, as assessed by flow cytometry using the AnnexinV/Propidium Iodide kit, at time 0, and 3, 6, 24 and 48 h after interleukin (IL) 2 deprivation used as pro-apoptotic stimulus, is shown. In the absence of MSCs (unbroken lines), the apoptotic rate of T lymphocytes from healthy colonic mucosa (left panel, mean of one experiment) after 48 h of IL-2 deprivation was higher than that of T lymphocytes from diseased mucosa (right panel, mean±SD of three experiments). Co-culture of T lymphocytes from healthy mucosa (left panel, mean of one experiment) with MSCs (broken line) induced a striking increase in the apoptotic rate since the start of IL-2 deprivation, whilst it did not affect the percentage of apoptotic cells throughout the 48 h of IL-2 deprivation when T lymphocytes were collected from diseased mucosa (right panel, mean±SD of three experiments).
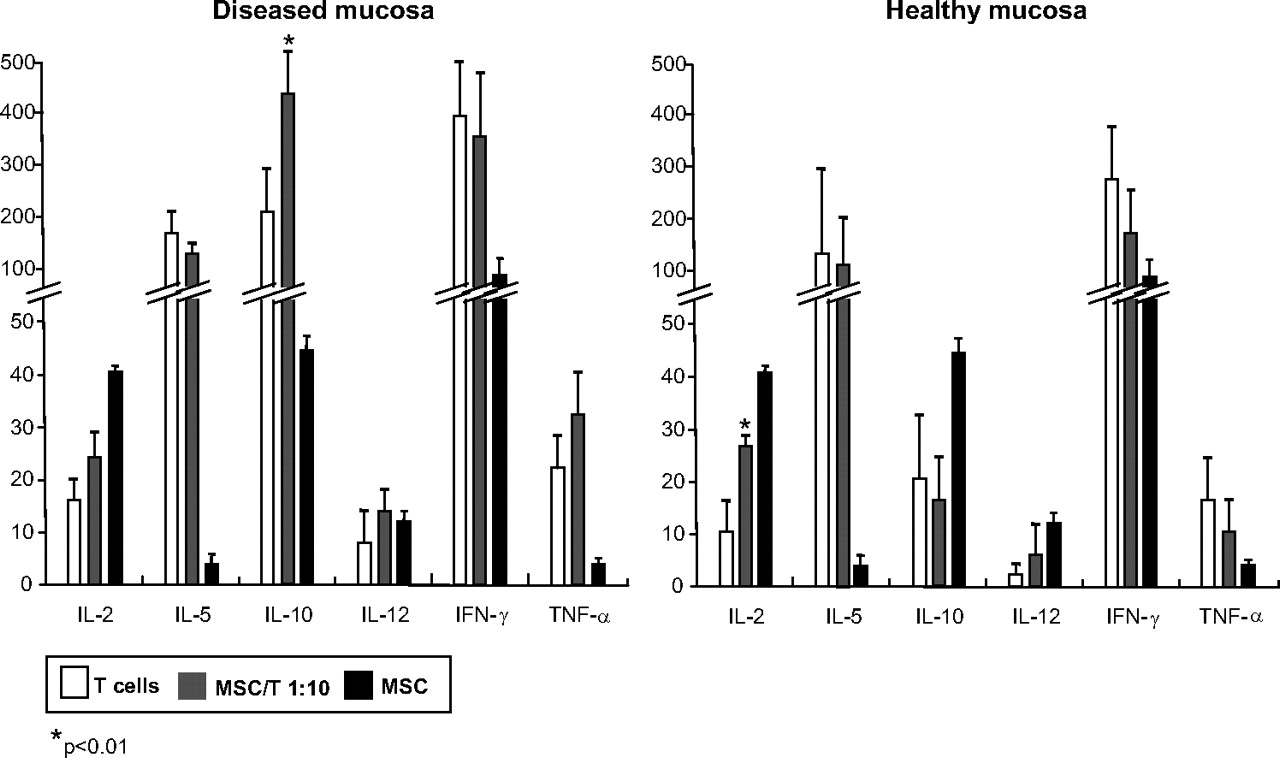
Finally, as regards the cytokine profile of the supernatants of MSC/T cells co-cultures, we found that when T cells from diseased mucosa were studied, a larger amount of IL-10 than that secreted by T cells alone was found (p<0.01), while the levels of the remaining cytokines were similar (figure 8 left panel). On the contrary, when using T cells from healthy mucosa, a significant increase of the level of IL-2 was found (p<0.01), about double that found in supernatants of T cells alone, with no significant modification of the levels of the other cytokines (figure 8 right panel). Moreover, the production of IL-10 by T cells from diseased mucosa was much greater than that of T cells from healthy mucosa even in the absence of MSC, together with a slight increase in the levels of IL-12, IFNγ and TNFα (figure 8). In addition, the levels of IL-6, IL-8 and IL-13 were over the detectable levels in all the co-culture experiments (data not shown). We cannot exclude a contribution of MSC in determining the levels of all the cytokines detected, except for IL-5, IL-13 and TNFα which are not produced by MSC.32 33 However, in the case of experiments with T cells from diseased mucosa, no live MSC were evident after 5 days co-culture. Furthermore, we did not find any significant difference in the cytokine pattern of MSC supernatants of patients with Crohn's disease in comparison to that of MSC from healthy donors (data not shown).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cytokine profile of mesenchymal stromal cell:T cell co-cultures. Expression of interleukin (IL)-2, -5, -10, -12, interferon (IFN) γ and tumour necrosis factor (TNF) α on the supernatants of T cells from both diseased (left panel) and healthy mucosa (right panel), mesenchymal stromal cells (MSCs), and co-cultures of T lymphocytes with autologous MSCs. The values indicate mean±SD. For comments, see the text.
Discussion
Treatment of fistulising Crohn's disease has radically changed in the last decade, shifting from a surgical-based approach to a medical-based approach as a result of the availability of immunosuppresants and biological agents.34 Although a large proportion of patients achieve fistula healing in the short/medium term, that is, 4–12 weeks, the percentage of relapsing patients over time is still very high.3 Moreover, in view of the significant side effects of such therapies, safer strategies are highly desirable.3 34
The advent of regenerative medicine, mainly based on cellular therapy, has provided clinicians with a potentially efficacious armamentarium to treat and, for the first time, to cure several degenerative and immune-mediated conditions.35 MSCs have recently been demonstrated to display both differentiation ability and immune modulatory functions, thus contributing to tissue repair and immune tolerance.4 Crohn's disease is characterised by an uncontrolled immune response to intestinal bacteria causing tissue damage which, in the penetrating phenotype, involves the entire gut wall up to formation of fistula tracks.1 It has been preliminarily shown that a single local injection of adipose tissue-derived MSC is a feasible and safe therapeutic approach for fistulising Crohn's disease.13 In the phase II study from the same group, a heterogeneous population of patients with perianal complex fistulas, both of cryptoglandular (n=35) and Crohn's disease origin (n=14), were treated by a combination of adipose tissue-derived MSC and fibrin glue or fibrin glue alone.14 However, even though the general results are promising in terms of efficacy, when considering the data of the Crohn's disease group, no difference was observed in comparison with those treated with fibrin glue. The reason may lie in the low number of patients and/or in the procedure based on a single injection.
On this basis, we carried out a prospective study to assess the feasibility, safety and efficacy of serial intrafistular injections of autologous BM-derived MSCs in the treatment of fistulising Crohn's disease. Twelve consecutive patients with active disease, as assessed by using both CDAI and PDAI score, were selected on the basis of refractoriness or unsuitability to all other treatments, and their BM blood was harvested to perform ex vivo isolation and expansion of MSCs. In all cases, an almost pure population of MSCs, similar in terms of morphology, proliferative potential, immune phenotype, differentiation ability, and genetic stability to that obtained from healthy donors, as already proved by our group,16 was obtained. Ten patients (two dropped out) underwent serial (median 4) local injections of MSC scheduled at 4-week intervals. A remarkable decrease of both CDAI and PDAI was achieved usually after the second treatment and both values remained stable during the 12 month follow-up, with regression of those symptoms causing severe physical and emotional distress and a poor quality of life, with 7/10 patients achieving ‘remission’, and 3/10 ‘improvement’ at surgical evaluation. Even though the presence of fistulas directly affects CDAI score for a maximum of 20 points, the indirect effects due to resolution or amelioration of perianal disease (and of enterocutaneous fistulas in a case) may explain our results. In fact, all patients became able to perform regular daily routines and leisure activities, increased food intake, no longer had fever, and anaemia improved in almost all patients probably due to damping of the chronic inflammation. As regards PDAI score, the relief from pain, discharge, and induration mainly accounted for its reduction. It is likely that NOD2 gene mutations did not play any role in determining the response to cellular therapy, since only a patient was a carrier. Besides clinical and surgical evaluation, fistulising Crohn's disease was also monitored by MRI, aimed at improving diagnostic accuracy and early detection of those complications responsible for fistula relapse.24 The presence of regenerative tissue along the tracks without fibrotic tissue was invariably revealed after the second injection, and persisted throughout follow-up. This is an important issue since a fibrotic-type reparative process could lead to loss of functional integrity of anal sphincters and secondary incontinence. In addition, although the comparison among clinical, surgical and imaging evaluation was beyond the scope of our study, we found a complete agreement in determining the outcome of every patient, but not the assessment of fistula anatomy and its complications, where MRI was more precise. Finally, endoscopic examination performed at the beginning of the study always showed an inflamed rectal mucosa, whilst at the end of follow-up a healed mucosa was invariably evident. As regards the latter feature, the mucosal enrichment of FoxP3+ regulatory T cells may have contributed. It is tempting to speculate, therefore, that a number of locally injected MSC might be able to circulate in blood and/or the lymphatic stream and to reach lymph-node germinal centres, thus influencing T cell differentiation.36 Accordingly, we found an increase of circulating FoxP3+ regulatory T cells after the second MSC injection that remained stable throughout treatment and follow-up. Our findings fit in with the recent demonstration of the efficacy of MSC systemic infusion both in preventing and curing colitis in a mouse model of Crohn's disease through the generation of FoxP3+ regulatory T cells.10 Similar results were obtained in a murine model of insulin-dependent diabetes in which peripheral T cells from MSC-treated rats exhibited higher frequencies of FoxP3+ T cells compared to the PBS-treated rats,37 and in an experimental model of collagen-induced arthritis in which MSC treatment prevented tissue damage by educating antigen-specific regulatory T cells.38 Moreover, in vitro studies showed that human BM-derived MSC co-cultured with peripheral blood mononuclear cells increased the percentage of CD4+/CD25highFoxP3+ regulatory T cells30 and biological studies indicate that MSC-driven immunomodulation is associated with suppression of pro-inflammatory T-helper 1 response while rebalancing the T-helper 1/2 ratio towards T-helper 2.39 According to this evidence, the analysis of the cytokine profile of the supernatants of T cells from diseased mucosa co-cultured with MSC showed a level of IL-10 which was double that found on supernatants of T cells cultured in the absence of MSC. Hence, it is likely that MSC induce or promote a tolerogenic milieu, in which they modulate and/or suppress T cell activation.40
When focusing on mechanisms responsible for tissue injury in Crohn's disease, that is delayed T cell apoptosis,29 31 we found that MSCs caused a sort of cell ‘freezing’ with lack of modification of the apoptotic rate when using T lymphocytes from diseased mucosa, while the percentage of apoptotic cells dramatically increased when incubated with T lymphocytes from healthy mucosa. The explanation for this phenomenon may lie in the ability of MSCs to suppress activated T cell functions by inhibiting Stat5 phosphorylation which results in cell cycle arrest at G0–G1 phase.41 42 The opposite effect observed on T cells isolated from healthy mucosa is consistent with the recent demonstration of a different action of MSC on immune cells depending on their quiescence or activation status.41 42
All patients enrolled in this study were taking stable doses of anti-inflammatory and/or immunosuppressive drugs, and a course of antibiotic therapy as adjunctive treatment due to the presence of abscesses was given just before the first injection. Although we cannot exclude the possibility that these therapies may have contributed to induction of ‘remission’ or ‘improvement’, their use before MSC treatment has been proven to be ineffective. In addition, no adverse effects were observed after the injection procedure or throughout the entire observation period.
In conclusion, local injection of autologous BM-derived MSCs is feasible, safe and successful in treating fistulising Crohn's disease, thus indicating that the possibility of curing this invalidating condition seems a real prospect in the not too distant future. Moreover, MSCs may compare favourably in terms of cost/effective ratio with biologicals which in the long-term management of fistulising Crohn's disease have been shown to significantly reduce indirect costs due to hospitalisation, surgery and procedures,43 but which have still very high direct costs. Phase III clinical trials are warranted to answer crucial points related to cellular therapy in Crohn's disease which have emerged from our study.
Acknowledgments
The authors are grateful to Lorenza Montagna, M.S. (Cell Factory – Research Laboratory, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy) who carried out the flow cytometric analysis of mesenchymal stromal cells and T cell subsets; to Annalisa De Silvestri, B.S. (Direzione Scientifica, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy) who performed statistical analysis; to Giacomo Fiandrino, M.D. (Servizio di Anatomia ed Istologia Patologica, Fondazione IRCCS Policlinico San Matteo, Università degli Studi di Pavia, Italy) who contributed to the cell counts on histological sections; to Elena Betti, B.S. (Laboratory of Gastroenterology, Clinica Medica I, Fondazione IRCCS Policlinico San Matteo, Università degli Studi di Pavia, Italy) who carried out the ELISA assays; and to Dr Ilaria Fulle, M.D. (Servizio di Diagnostica per Immagini, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy) who reviewed all patients' MRI examinations in a blind fashion. Drs Montagna, De Silvestri, Fiandrino, Betti, and Fulle did not receive any remuneration for their contributions.
References
Footnotes
See Commentary, p 742
FL and GRC equally contributed to this manuscript.
Funding This study was financed in part by grants from: Istituto Superiore di Sanità (National Program on Stem Cells), European Union (FP6 program ALLOSTEM), Ministero dell'Istruzione, dell'Università e della Ricerca (Progetti di Rilevante Interesse Nazionale), Regione Lombardia (Research Project: “Trapianto di cellule staminali adulte per scopi di terapia cellulare sostitutiva, riparativa e rigenerativa”), and Fondazione CARIPLO to FL; by Fondazione IRCCS Policlinico San Matteo (Progetti di Ricerca Corrente) to RC, RM, FL and GRC; by Ministero dell'Istruzione, dell'Università e della Ricerca (Progetti di Rilevante Interesse Nazionale) to RC and GRC; by Istituto Superiore di Sanità (ISS per Alleanza contro il Cancro: Programma Straordinario di Ricerca Oncologica 2006), Ministero della Salute (Progetto Ricerca Finalizzata ICS 030.4 RF 2005/07) to RM; and by Associazione Italiana Ricerca sul Cancro (AIRC) to MEB.
Competing interests None.
Ethics approval This study was conducted with the approval of the Bio-Ethics Committee of IRCCS Policlinico San Matteo Foundation, Pavia.
Provenance and peer review Not commissioned; externally peer reviewed.