Article Text

Abstract
Introduction The risk of oesophageal adenocarcinoma (OAC) in non-dysplastic Barrett's oesophagus (BO) may have been overestimated. The objective was to estimate the incidence of OAC in patients with BO without dysplasia.
Methods The authors searched MEDLINE and EMBASE from 1966 to 2011 and performed a bibliographic review of previous publications, excluding abstracts, non-peer-reviewed publications and those not published in English, for prospective or retrospective studies of the incidence of OAC in patients with BO. They excluded patients with any degree of dysplasia at baseline and those without documented intestinal metaplasia. Studies were independently reviewed by two individuals. 57 of 3450 studies were included. The authors extracted information on number of patients with BO, length of follow-up, incident cases of OAC, mean age of patients, country of origin, whether prospective or retrospective, mean length of BO segments and mortality from causes other than OAC. Study quality was assessed by the Ottawa Newcastle criteria.
Results The 57 included studies comprised 11 434 patients and 58 547 patient-years of follow-up. The pooled annual incidence of OAC was 0.33% (95% CI 0.28% to 0.38%). Among 16 studies that provided appropriate information on mortality, there were 56 incident cases of OAC but 684 deaths from apparently unrelated causes. Among 16 studies that provided information on patients with short-segment BO, the annual incidence of OAC was only 0.19%.
Conclusions The incidence of OAC in non-dysplastic BO is around 1 per 300 patients per year. The incidence of OAC in short-segment BO is under 1 per 500 patients per year.
- Barrett's oesophagus
- oesophageal adenocarcinoma
- incidence
- meta-analysis
- Barrett's carcinoma
- oesophageal cancer
- gastroesophageal reflux disease
- Helicobacter pylori–treatment
- duodenal ulcer
- proton pump inhibition
Statistics from Altmetric.com
- Barrett's oesophagus
- oesophageal adenocarcinoma
- incidence
- meta-analysis
- Barrett's carcinoma
- oesophageal cancer
- gastroesophageal reflux disease
- Helicobacter pylori–treatment
- duodenal ulcer
- proton pump inhibition
Significance of this study
What is already known about this subject?
The annual incidence of oesophageal adenocarcinoma (OAC) in Barrett's oesophagus (BO) has been reported to be 0.5%.
What are the new findings?
Having eliminated duplicate and redundant studies and confined analysis to patients without baseline dysplasia, the authors estimate an annual incidence of OAC in non-dysplastic BO of 0.33%.
Among patients with non-dysplastic short segment BO, the authors estimate the annual incidence of OAC to be 0.19%.
During surveillance, patients with non-dysplastic BO may be at least 10 times more likely to die from an unrelated cause than to develop OAC.
How might it impact clinical practice?
Surveillance strategies for patients with non-dysplastic BO, particularly those with short segments, may need to be reconsidered.
Introduction
Barrett's oesophagus (BO) is the major risk factor for the development of oesophageal adenocarcinoma (OAC), which is rapidly increasing in incidence in North America and Europe. In the USA, the American College of Gastroenterology and the American Gastroenterological Association currently advise surveillance endoscopy for patients with BO.1 2 The annual incidence of OAC in patients with BO is widely estimated to be around 0.5%1—or 1 in 200 patients per year. This estimate dates back to a meta-analysis from 2000,3 which also highlighted the problem of publication bias in the reporting of studies of OAC incidence in BO. Prior to 2000, the incidence of OAC in BO had been widely assumed to be higher. However, that analysis did not account for the presence of baseline dysplasia, which is an intermediate stage in the development of OAC. Furthermore, many of the included studies were published in 1991 or before. Patients in these studies are unlikely to have been treated for prolonged periods with proton pump inhibitors, which may have reduced the risk of progression to OAC.4 Furthermore, the entity of short-segment BO (SSBO) was only identified in 1994.5 Consequently, studies before then would likely have included only patients with long-segment BO (LSBO); this may, therefore, have led to an overestimate of the risk of OAC. Therefore, at least some of these studies may not be relevant to contemporary practice; patients with BO now almost routinely receive long-term proton pump inhibitor treatment, and SSBO is a widely recognised clinical entity. In an editorial in 2000, Spechler noted that the estimate of 0.5% annual incidence of OAC did not concur with the clinical experience of practicing gastroenterologists, at least in the USA.6 Aside from the impact of publication bias, Spechler noted that published studies often emanated from tertiary care centres and suggested that such data might not be generalisable.
Three subsequent meta-analyses have specifically attempted to address the incidence of OAC in BO.7–9 Wani et al7 and Sikkema et al8 each reported an annual incidence of OAC of around 0.6% but included some patients with low-grade dysplasia (LGD) at baseline. Yousef et al9 estimated the risk of OAC to be 0.41% annually when patients with early incident cancers and baseline high-grade dysplasia (HGD) were excluded, although they also included some patients with baseline LGD. The meta-analyses by Wani et al7 and Sikkema et al8 did not provide a specific estimate of OAC incidence for patients with SSBO. The risk of OAC in SSBO and LSBO may not necessarily be the same, and it may not be appropriate to combine patients with SSBO and those with LSBO in studies evaluating the incidence of OAC. Yousef et al9 estimated the risk of OAC in SSBO to be 0.61% based on a subgroup analysis of six studies but did not account for baseline dysplasia.
In order to obtain a current, accurate estimate of the risk of OAC in patients with BO who were free of dysplasia at baseline, we performed an updated meta-analysis of observational studies.
Methods
We initially conducted a computerised literature search of the MEDLINE and EMBASE databases from 1996 until December 2009 for prospective or retrospective studies that reported the incidence of OAC among patients with BO. The search string and keywords used were ‘Barrett's oesophagus, Barrett's metaplasia, Barrett's epithelium, columnar-lined oesophagus, specialised intestinal epithelium’ and ‘esophageal adenocarcinoma, esophageal cancer, esophageal neoplasm, or dysplasia’. The search was undertaken by two individuals (TKD and KK) independently. Using the same search criteria, we updated our search in May 2011 to include studies published between January 2010 and May 2011. This strategy was supplemented by a search of the citations from previous meta-analyses.7–9 Studies published only in abstract form were not included. We defined BO as the presence of intestinal metaplasia (IM) in the distal oesophagus; we excluded patients who were specified in the articles as having gastric metaplasia but no documented IM in the distal oesophagus. Information was extracted on numbers of patients with BO included, mean age of patients, length of follow-up, number of patient-years of follow-up and incidence of OAC. Articles were scrutinised for information on the presence of any dysplasia among patients at baseline. We excluded from analysis all patients who had evidence of LGD or HGD or who had biopsies graded as ‘indefinite’ for dysplasia, as specified in the individual articles. Those articles that did not provide clear and specific information on the follow-up of patients with and without dysplasia were excluded as having ‘not distinguished dysplasia’. Where available, information was also extracted concerning deaths during follow-up from causes unrelated to OAC and on patients receiving surgical treatment for gastro-oesophageal reflux disease (GORD) and/or BO. We excluded as ‘prevalent’ all cases of OAC that were diagnosed within 1 year of commencing surveillance. Articles were scrutinised for specific data on patients with SSBO. If provided, these data were included in a separate preplanned subgroup analysis. We defined SSBO as BO with a maximum segment length of 3 cm. Incident cases of OAC in BO segments of up to 3 cm were considered to have arisen within SSBO. Any discrepancies between the findings of the two reviewers were resolved by consensus. We excluded any redundant studies that were earlier reports of subsequent series.
The incidence of OAC was calculated by dividing the number of incident cases of OAC by the number of patient-years of follow-up among patients with non-dysplastic BO (NDBO). The mortality rate from unrelated causes was calculated by dividing the number of patients who died of a cause other than OAC by the number of patient-years of follow-up among patients with NDBO. Study authors were contacted to clarify details when necessary. When directed in the manuscript, the journal website was visited for additional data not included in the original manuscript.
Since all of the studies included were observational in nature, quality was assessed using the Ottawa Newcastle criteria of Wells et al.10 Specifically, three factors were considered indicators of good study quality as described by Yousef et al.9 These were a study size of >500 patient-years follow-up, the use of strict criteria for the definition of BO based on a clinically visible segment of columnar-appearing mucosa and histologically confirmed IM, and low selection bias. Selection bias was considered to be present if <70% of the total inception cohort was followed. With respect to study size, a minimum of 5 years follow-up was required to define a high-quality study. We performed a post hoc subset analysis of only the high-quality studies.
Statistics
We performed a meta-analysis of included studies using StatsDirect version 2.7.8 (Altrincham, Cheshire, UK). We assessed for heterogeneity using the Cochran Q and I2 statistics.11 We defined heterogeneity a priori as statistically significant if the p value for the Cochran Q statistic was 0.10 or below. Where no statistically significant heterogeneity was detected, we planned to use a fixed-effect model. If statistically significant heterogeneity was found, we planned to use a random-effects model. We assessed for publication bias using Egger's test and by visual inspection of funnel plots.12 A p value of 0.10 or below on Egger's test was considered to indicate risk of publication bias or evidence of a ‘small studies effect’. When the counts of OAC were zero, a correction of 0.5 was added to the number of incident cases of OAC and person-years of follow-up, prior to calculation, as previously described.13
We performed secondary or post hoc analyses confined to studies that reported mortality rates from causes unrelated to OAC, studies that had excluded patients treated surgically for GORD and/or BO and studies considered to be of the highest quality.
Results
Figure 1 is a flow diagram of our search strategy and results. Our initial and updated searches together identified 3450 citations. After exclusion of abstracts and non-peer-reviewed articles, 100 studies were initially identified; 18 redundant or duplicate studies were subsequently excluded.14–31 Twenty-four studies were excluded because they did not account for baseline dysplasia.30 32–54 One study that was limited to patients with ulcerated BO was excluded because such patients likely represent a high-risk group and their natural history should not be extrapolated to the general population of patients with NDBO.55 Therefore, we included 57 studies in the meta-analysis.4 56–111 Summary data are given in table 1.

Search strategy for identifying studies to be included in the meta-analysis.
Details of the 57 included studies
Combined, these 57 studies accounted for 11 434 patients with histologically confirmed NDBO and 58 547 patient-years of follow-up. The mean age of patients included in these studies ranged from 44 to 65 years. There were 186 incident cases of OAC documented during follow-up. Since there was no statistically significant heterogeneity among these studies (Cochran Q=64.6; p=0.20; I2=13.3%), a fixed-effect model was used for meta-analysis. The pooled incidence of OAC among all 57 studies was 0.33% (95% CI 0.28% to 0.38%). There was no evidence of publication bias (Egger's test, p=0.19).
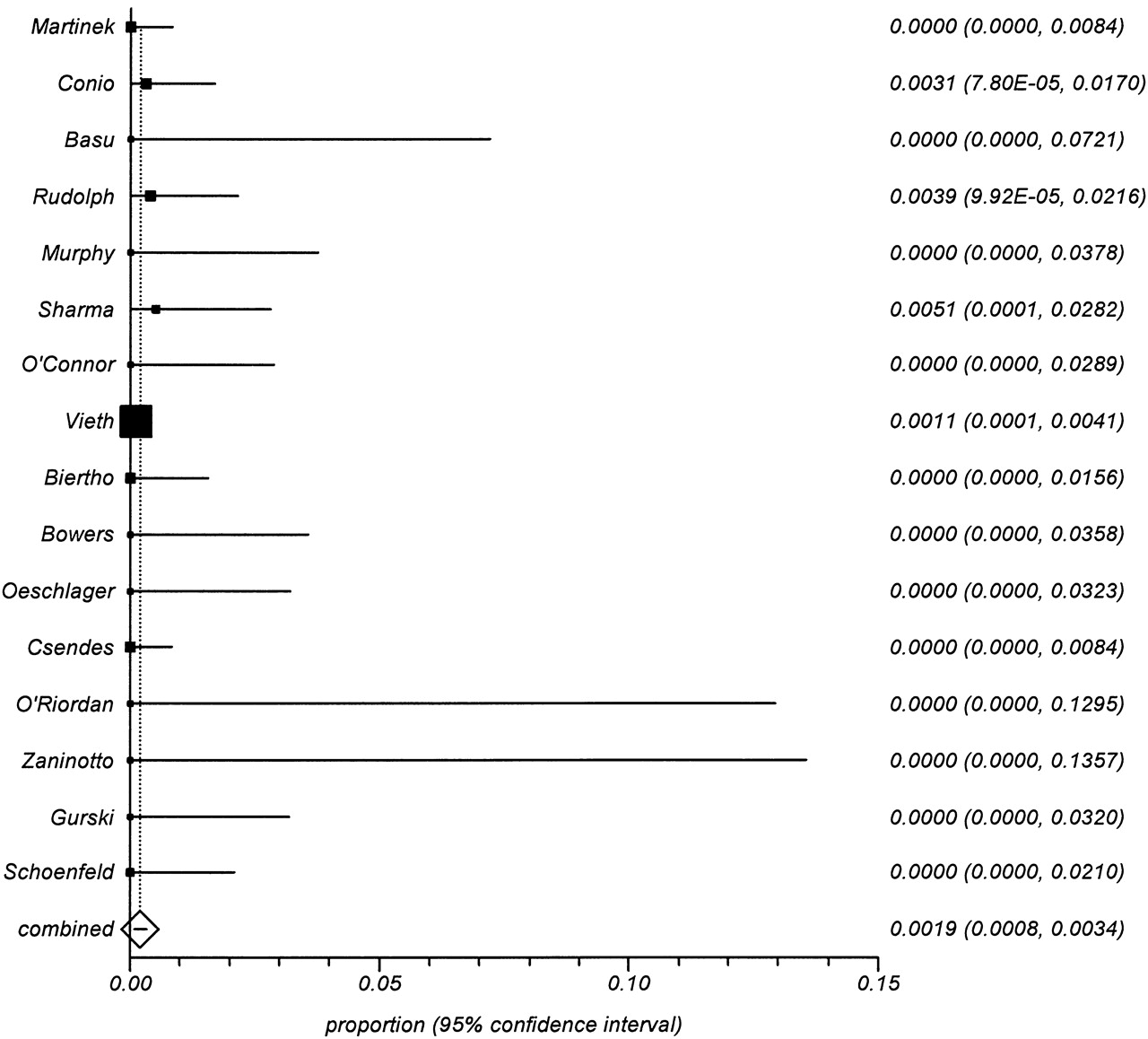
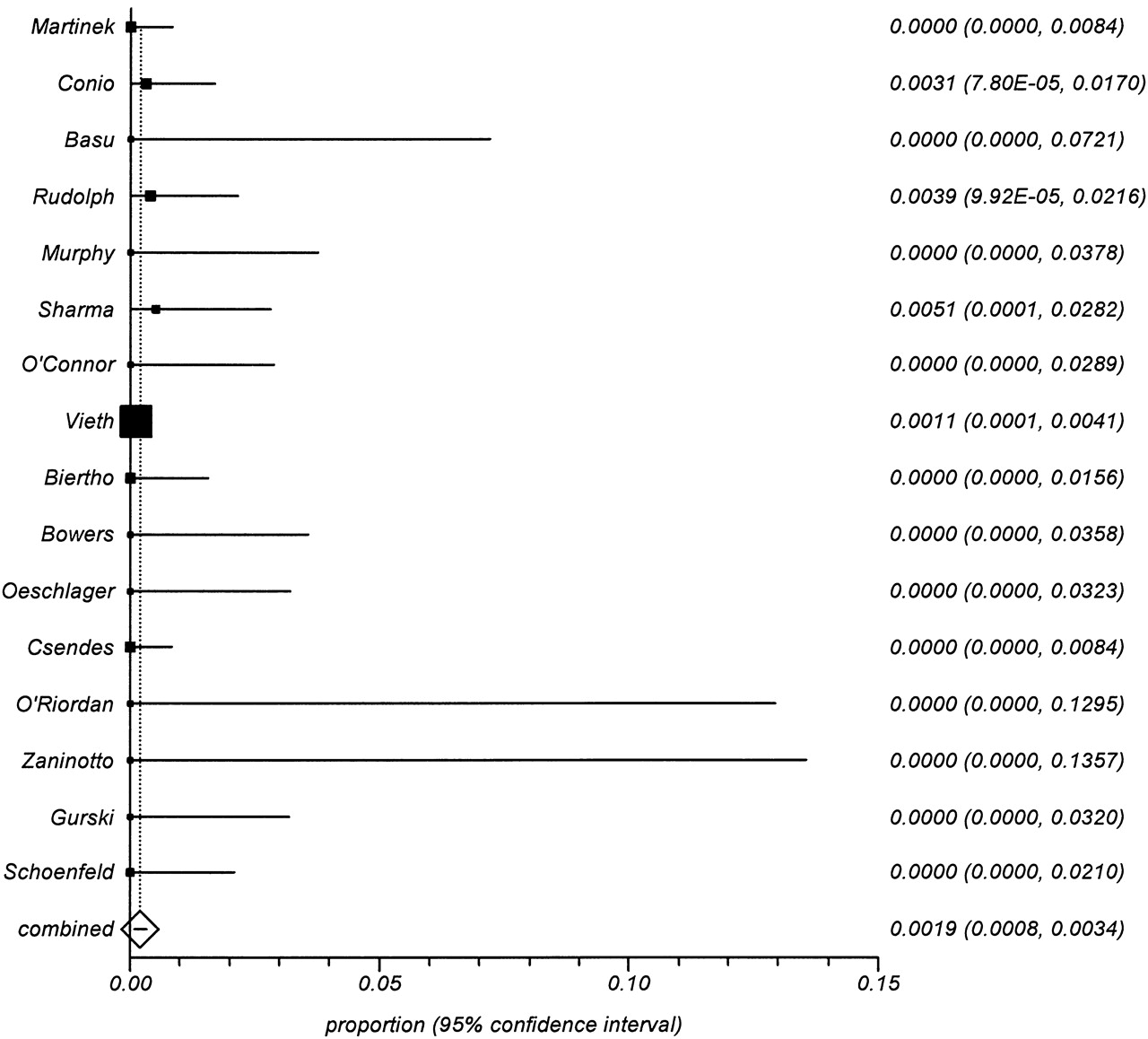
Ten studies were considered to be of the highest quality in that they had no evidence of selection bias, more than 5 years of mean follow-up and at least 1 year of minimum follow-up.4 65 66 74 76 79 84 95 110 111 These comprised 3345 patients and 23 984 patient-years of follow-up. There were 77 incident cases of OAC identified. Since there was no statistically significant heterogeneity among these studies (Cochran Q=11.8; p=0.23; I2=23.5%), a fixed-effect model was applied (figure 2). The pooled annual incidence of OAC remained at 0.33% (95% CI 0.26% to 0.40%). There was no evidence of publication bias among these studies (Egger's test, p=0.20). These 10 studies alone accounted for 41% of the total patient-years of follow-up and of the cases of OAC among all 57 studies.

Forest plot of the post hoc meta-analysis of the 10 studies of highest methodological quality.
We identified 16 studies that supplied adequate information regarding the incidence of OAC among patients with SSBO, as defined above.18 21 27 57–59 61 62 69 79 82 85 86 95 99 112 Three of these studies18 21 27 were used only for the analysis of OAC incidence in SSBO. These studies were subsequently amalgamated into a larger study31 that is included in our overall analysis. The 16 studies comprised 967 patients and 4456 patient-years of follow-up. There were five incident cases of OAC, including one that arose from a BO segment of 3 cm.61 There was no significant heterogeneity among these studies (Cochran Q=5.74; p=0.98; I2=0%). Using a fixed-effect model, the pooled annual incidence of OAC was 0.19% (95% CI 0.08% to 0.34%) (figure 3). There was no evidence of publication bias (Egger's test, p=0.96).
{kind=link}
{kind=link}
{kind=link}
Forest plot of the planned subgroup analysis of the 16 studies that supplied adequate information on the incidence of oesophageal adenocarcinoma among patients with documented short segment Barrett's oesophagus.
After excluding studies that had employed surgical treatment for GORD and/or BO, 37 remained,4 57 61 65–68 70–72 74–76 78–83 89 90 92–98 100 101 105–111 accounting for 6599 patients and 33 549 patient-years of follow-up. There were 128 incident cases of OAC detected. There was statistically significant heterogeneity among these studies (Cochran Q=38.12; p=0.09; I2=26.5%); accordingly, a random-effects model was used. The pooled annual incidence of OAC was 0.41% (95% CI 0.32% to 0.51%). There was evidence of significant publication bias (Egger's test, p=0.06).
Sixteen studies provided information about mortality during follow-up from causes unrelated to OAC.59 61 65 66 68 70 73 75 76 79 81 92 100 108 110 111 These accounted for 2916 patients and 17 214 patient-years of follow-up. There were 56 incident cases of OAC detected during follow-up and 684 deaths from causes apparently unrelated to OAC. There was no statistically significant heterogeneity among these studies (Cochran Q=15.4; p=0.42; I2=2.9%). Using a fixed-effect model, the pooled annual incidence of OAC was 0.34% (95% CI 0.26% to 0.44%). There was, however, evidence of significant publication bias (Egger's test, p=0.08).
Discussion
In this meta-analysis, we have attempted to assess the risk of OAC in patients with BO who were free of dysplasia at the time of entry into a surveillance programme. We believe that this is the first meta-analysis to have focused specifically on OAC incidence among patients with NDBO. A further strength of our approach is that we carefully tried to exclude from analysis any duplicate or redundant studies. Our estimate of 0.33% annual incidence of OAC among patients with NDBO (or approximately 1 case per 300 patients per year) is lower than previously estimated and might affect the results of any cost benefit analysis of surveillance strategies. Furthermore, our pooled estimate is based on studies in which the majority of patients had LSBO. This estimate of OAC incidence of 0.33% annually may not be applicable to all patients with BO; many patients with BO who are currently undergoing endoscopic surveillance, at least in the USA, have SSBO. We estimate that the annual incidence of OAC in SSBO is only 0.19% (or just under 1 case per 500 patients per year). At such a low incidence of OAC, routine surveillance endoscopy among patients with carefully confirmed non-dysplastic SSBO may not be justified.
Subsequent to our meta-analysis, Bhat et al reported their population-based study from Northern Ireland.113 They included patients with BO with or without IM in the distal oesophagus and reported combined rates of OAC, HGD and gastric cardia cancer. Among the 46% of their patient cohort who had IM of the oesophagus, the combined annual incidence of HGD, OAC and gastric cardia cancer was 0.38%, which is very similar to our estimate of OAC incidence among patients with BO with IM.
As with any meta-analysis, there are limitations. The included studies varied with respect to numbers of patients followed, duration of follow-up, frequency of endoscopic surveillance, numbers of biopsies taken at endoscopy and overall study quality relating to such items as accounting for patients during follow-up. Regarding overall study quality, our post hoc subset analysis of the 10 studies with the highest overall quality also found a pooled annual incidence of OAC of 0.33%. These 10 studies accounted for 41% of the total patient-years of follow-up and of the cases of OAC in all of the included studies.
Most of the studies included in our analysis were from countries outside the USA. Furthermore, within the USA, more than half of the total patient-years of follow-up were among patients in the Veterans Affairs healthcare system. However, the Veterans Affairs experience may not be directly applicable to US community practice where so many resources are currently devoted to the surveillance of patients with BO. The remaining US data on OAC incidence in BO were largely derived from tertiary care centres, and these too may not be representative of the community practice setting.6 There is a lack of information concerning the risk of OAC in patients with BO who are not being cared for at academic centres.
Relatively few patients with SSBO were included in the studies that we examined; overall, they accounted for <10% of the total number of patient-years of follow-up. However, our estimate of the risk of OAC among patients with SSBO is notably lower than the pooled estimate for all patients with BO. Rudolph et al had reported that the incidence of OAC among patients with SSBO is similar to that among patients with LSBO.112 However, six of the seven cancers that developed were in patients with SSBO who had HGD at baseline endoscopy. We specifically excluded from analysis all patients with any degree of dysplasia at baseline.
Earlier meta-analyses included some patients with BO who had undergone antireflux surgery. Since that has not been shown to reduce the risk of OAC in BO, we included some surgical series in our full analysis. However, when we excluded the surgical series, our estimate of the pooled annual incidence of OAC rose slightly from 0.33% to 0.41%. The significance of this small difference is highly questionable. Any influence of antireflux surgery on the risk of OAC among patients with BO cannot be adequately addressed by this meta-analysis. However, we have not found any evidence to indicate a major beneficial effect of antireflux surgery on OAC risk.
Patients with BO who undergo endoscopic surveillance have substantial mortality rates from causes unrelated to OAC. This high mortality rate may be due in part to the relatively advanced age and high rates of comorbidity of the population undergoing surveillance and may not apply to younger patients with BO. This must be factored into any cost benefit analysis of surveillance and/or ablation of NDBO.
In conclusion, our analysis demonstrates a lower incidence of OAC among patients with BO who are free of dysplasia at the start of surveillance than is generally supposed. This is especially true for patients with non-dysplastic SSBO. The utility and cost-effectiveness of surveillance among patients with BO should be re-evaluated, with particular attention paid to SSBO.
References
Footnotes
Previous presentation: These data were presented in poster form at the annual meeting of the American Gastroenterological Association in Chicago, Illinois, USA, on 7 May 2011.
Correction notice This article has been corrected since it was published Online First. The captions of figure 2 and 3 were changed, and the name of the American Gastroenterological Association was corrected.
Competing interests Dr Howden: consultant for Takeda, Otsuka, Boehringer-Ingelheim, Novartis, Eisai, XenoPort; speaking fees from Takeda, Otsuka, GlaxoSmithKline.
Provenance and peer review Not commissioned; externally peer reviewed.