Article Text

Abstract
The changing epidemiology of inflammatory bowel disease (IBD) across time and geography suggests that environmental factors play a major role in modifying disease expression. Disease emergence in developing nations suggests that epidemiological evolution is related to westernisation of lifestyle and industrialisation. The strongest environmental associations identified are cigarette smoking and appendectomy, although neither alone explains the variation in incidence of IBD worldwide. Urbanisation of societies, associated with changes in diet, antibiotic use, hygiene status, microbial exposures and pollution have been implicated as potential environmental risk factors for IBD. Changes in socioeconomic status might occur differently in different geographical areas and populations and, consequently, it is important to consider the heterogeneity of risk factors applicable to the individual patient. Environmental risk factors of individual, familial, community-based, country-based and regionally based origin may all contribute to the pathogenesis of IBD. The geographical variation of IBD provides clues for researchers to investigate possible environmental aetiological factors. The present review aims to provide an update of the literature exploring geographical variability in IBD and to explore the environmental risk factors that may account for this variability.
- Inflammatory Bowel Disease
- Epidemiology
- Ulcerative Colitis
- Crohn's Disease
Statistics from Altmetric.com
Background
The changing epidemiology of inflammatory bowel disease (IBD) worldwide provides an opportunity to study disease aetiology. As the incidence and prevalence of IBD may have stabilised in high-incidence areas such as North America and northern Europe, they continue to rise in previously low-incidence areas such as southern and eastern Europe, Asia and much of the developing world. In these countries, ulcerative colitis (UC) has emerged first followed by Crohn's disease (CD) after a variable period of time.1 ,2 This phenomenon mirrored what took place in the west 75 years ago when the disease first appeared. The burden of IBD varies in different countries and populations. These variations in disease incidence may reflect differences in the distribution or magnitude of the impact of environmental aetiological factors. All of these environmental factors have been hypothesised and not yet proved as causal. The increased incidence when there is a transition from ‘developing‘ to developed nation status is currently one of the most compelling lines of evidence linking changing epidemiology with changing lifestyle and environmental factors.3 ,4 That migrants from developing to developed countries have an increased risk of IBD further supports the importance of environmental influence, particularly modernisation and western lifestyle.5–7 Data from migration studies indicate that the children take on the risk factors of the new environment whereas the parents maintain their original risk pattern, suggesting that environmental influence during childhood is crucial.5 However, variations in lifestyle, between countries and within countries, are great. In IBD, different risk factors may cause imbalances in the environmental–host relationship in different parts of the world. Suspected consequences of industrialisation probably have variable effects on disease development in different geographical regions. A valuable clue to causative environmental factors may be found in the geographical variations of IBD incidence. Our intent is not to review the worldwide incidence or prevalence of paediatric and adult IBD, which has been reported in recent systematic reviews.4 ,8 ,9 The present review aims to summarise geographical differences between countries, within countries and over time in the epidemiology of IBD, and to define environmental risk factors of IBD at the regional and population level that may explain these variations. Finally, we propose potential studies that need to be performed in the future to understand further the associations between geographical distribution and environmental factors in IBD.
Methods
We have performed a comprehensive search on BIOSIS Previews, EMBASE, EBM Reviews, Global Health and Ovid MEDLINE of all original research studies and reviews published in English language journals from 1946 to October 2012 using the following keywords: IBD, UC, CD, epidemiology, geography, risk factors, environmental factors, smoking, appendectomy, antibiotics, hygiene, oral contraceptives, vitamin D and sunlight. In addition, a manual search of references in review articles was performed (see supplementary appendix 1, available online only). A total of 1138 citations was identified from the literature search. Potential studies were screened by title and abstract. After excluding duplicate publications, there was a total of 117 articles pertaining to epidemiology and geography of IBD, and 485 articles related to risk factors or environmental factors of IBD. We further selected human studies reporting risk factors, studies that have reported the role of environmental factors on disease development as opposed to disease course and review articles that contained original epidemiological data not previously published. This resulted in a total of 89 articles on epidemiology of IBD and 191 articles on risk factors of IBD (see supplementary figure 1, available online only). While we have reviewed all relevant reports, it was not within the scope of this report to include all the papers on epidemiology and risk factors of IBD in the current paper. Furthermore, systematic reviews on the incidence and prevalence of paediatric and adult IBD worldwide has recently been published.8 ,9 Instead, we have focused on and included papers that have reported novel disease trends and possible associations with environmental factors that could be deemed to be associated with the aetiology and epidemiology of IBD.
Studies were included if they fulfilled the following criteria: (1) original adult and paediatric studies that have reported disease trends over time including Asian migrant studies; (2) original studies that have reported disease variation within countries; (3) hospital and population-based studies from developing countries including Asia and eastern Europe that have reported disease incidence and prevalence; (4) case–control and cohort studies in adult and paediatric populations in developed and developing countries that have reported potential risk factors for IBD; (5) systematic review and meta-analysis reporting risk factors for the development of IBD; and (6) original papers or review articles that have discussed possible associations between epidemiological variation and environmental risk factors.
Geography
IBD geographical variation between countries
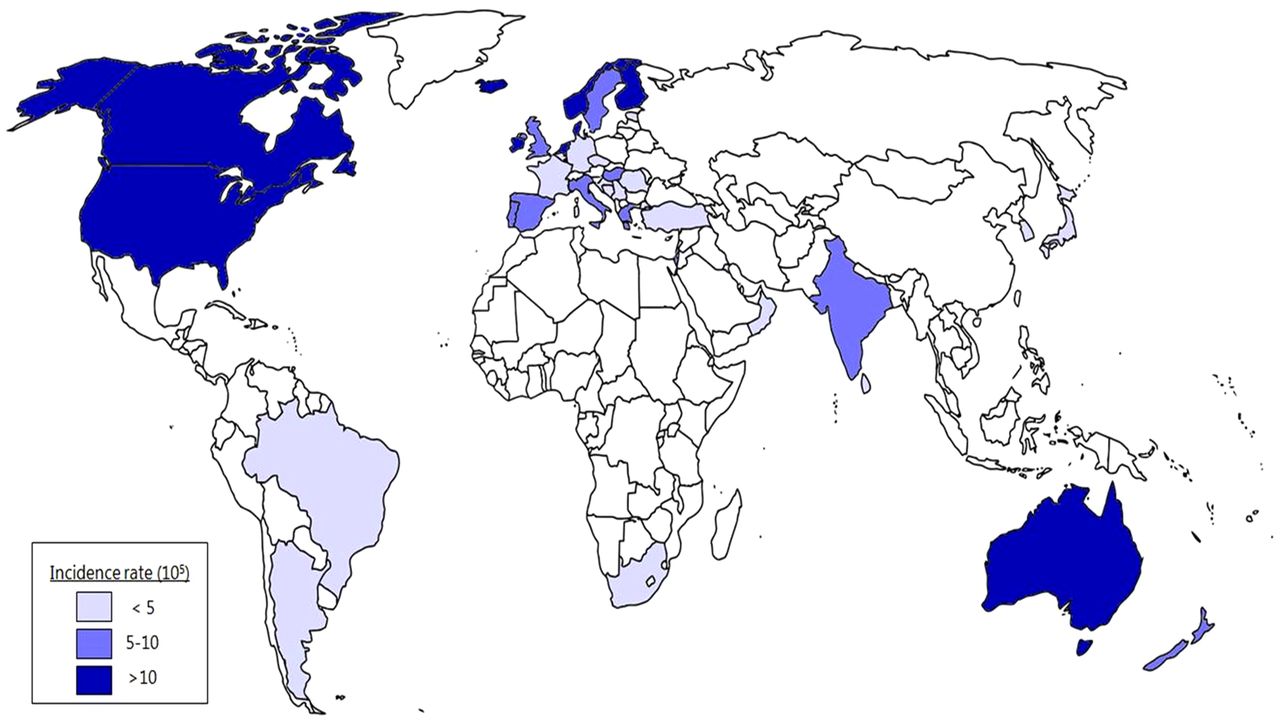
The highest incidence rates of CD and UC have been reported in northern Europe, the UK and North America.8 ,10 Such high incidence rates in these countries may indicate common aetiological factors. Countries in the Pacific, including New Zealand and Australia, which share many possible environmental risk factors and similar genetic background as north-west Europe and North America have high incidence rates of IBD. For instance, population-based studies from Canterbury in New Zealand11 and Geelong in Australia showed that the incidence rates of both UC and CD were among the highest in the world.12 In countries that are becoming more westernised, including China, South Korea, India, Lebanon, Iran, Thailand, the French West Indies and north Africa, IBD appears to be emerging. In Africa and Central and South America, data are scarce or not available. Figures 1 and 2 illustrate the incidence rates of CD and UC worldwide.

Global map of Crohn's disease incidence. This figure is only reproduced in colour in the online version.

Global map of ulcerative colitis incidence. This figure is only reproduced in colour in the online version.
Within Europe marked differences in rates of IBD between centres have been reported. The highest incidence rates have been demonstrated in the islands of Iceland and the Faroe Islands in the north, and the islands of Crete and Sicily13 in the south of Europe. Within the UK, Germany and Spain, there are no direct comparisons of national variations. Higher incidence rates have been reported from studies in Ireland, Scotland and The Netherlands compared to the UK and western Germany.13 Many of these differences, however, might be explained by differences in the type of cohorts, methods of data collection and the organisation of healthcare. In the European Collaborative Study on IBD (EC-IBD), differences in incidence rates between northern and southern Europe were less than might have been expected.13 This may reflect an increase in the incidence rate of both diseases in southern Europe.14
Within eastern Europe, recent population-based studies from Hungary and Croatia have reported sharp increases in IBD incidence rates and prevalence, comparable to that of high-incidence areas in western European countries.15–17 In contrast, studies from other eastern European countries such as Romania and Poland still report relatively low incidence rates.18 ,19 As a result of methodological bias, the reported incidence rates may have been underestimated. The reasons for these changes could be increased awareness of the disease and differences in diagnostic practices, or they could reflect real differences, as a result of environmental influence. Changes in lifestyle in eastern Europe over the past two decades have resulted in a more ‘westernised‘ way of living.20 It will be of interest to follow the temporal trends for IBD in eastern Europe to monitor whether this increase continues over time.
The impact of increasing immigration to western societies is important. Earlier reports showed that the prevalence of UC among southern Asians who migrated to the UK was higher compared with the European UK population (17 cases per 100 000 persons vs seven per 100 000).5 ,6 A recent study showed that Spanish patients who emigrated within Europe, but not those who emigrated to Latin America, developed IBD more frequently than controls.7 Individuals who have emigrated to westernised countries and subsequently returned to their country of birth also continued to demonstrate an increased risk of developing IBD, especially UC, suggesting that environmental factors related to industrialisation play an important role in disease pathogenesis.7 The critical age of living within a high-incidence area remains to be established, but undoubtedly childhood years will prove to be important.
IBD geographical variation within countries
Within certain individual countries there is evidence of epidemiological variability, as has been reported in Norway,21 France,22 Canada23 ,24 and Scotland.25 Within France,22 ,26 Italy, Spain and Portugal,13 there is a north–south disease gradient. The incidence of CD increased by 23% over 12 years in northern France while that of UC decreased by 17% during the same period.27 Using a Bayesian approach to take into account differences in population sizes of geographical units and spatial autocorrelation, more recent data from a hospital-based nationwide registry continue to show higher incidence rates and prevalence rates for CD in the north compared to the south of France.22 Other geographical risk factors for CD in France include higher urbanisation in northern areas28 and areas with less in-home sanitation.29 Data on IBD multiplex families in northern France and Belgium showed clustering in space and time,22 suggesting that shared environmental factors may contribute to these clustering effects within a defined space. A study in Scotland has shown a higher incidence of paediatric CD from postal code areas of the north compared with those of the south.25 In Sweden (within the Uppsala healthcare region), the incidence of UC and CD has been reported to be higher in urban than rural areas.30
In Norway, similar incidence rates have been shown between the south-eastern, western and northern parts.21 ,31 ,32 The distribution was more homogeneous in the north compared to southeastern and western Norway.21 The north is characterised by a generally mixed urban and rural population, whereas south-eastern and western Norway have a more defined separation between urban and rural areas.21 Both the western and south-eastern areas showed a generally higher incidence rate in the scattered rural populations, contrary to previous international experience, in which urban areas have been considered to be areas at increased risk of IBD.33 In Norway, the counties with the most scattered and rural populations were also the areas with only one hospital, in contrast to the many recording hospitals and multidisciplinary doctors in the cities. This gave a variation in incidence rate between 17 per 100 000 in Oslo and 28 per 100 000 in the scattered populated area of Aust Agder, with one hospital in the only city of the county. These data may provide evidence for the importance of access to healthcare and awareness of the population under examination.
A key factor that might be related to higher rates in cities and urbanisation is improved sanitary conditions. An epidemiological study in the UK showed that having a fixed hot water supply in childhood before the age of 11 years was associated with an increased risk of CD.34 It may be that different risk factors are acting concomitantly within an area in addition to the existence of different risk factors between areas. Furthermore, variations in the accuracy, efficiency and quality of registration between areas cannot be ruled out as a contributing factor.
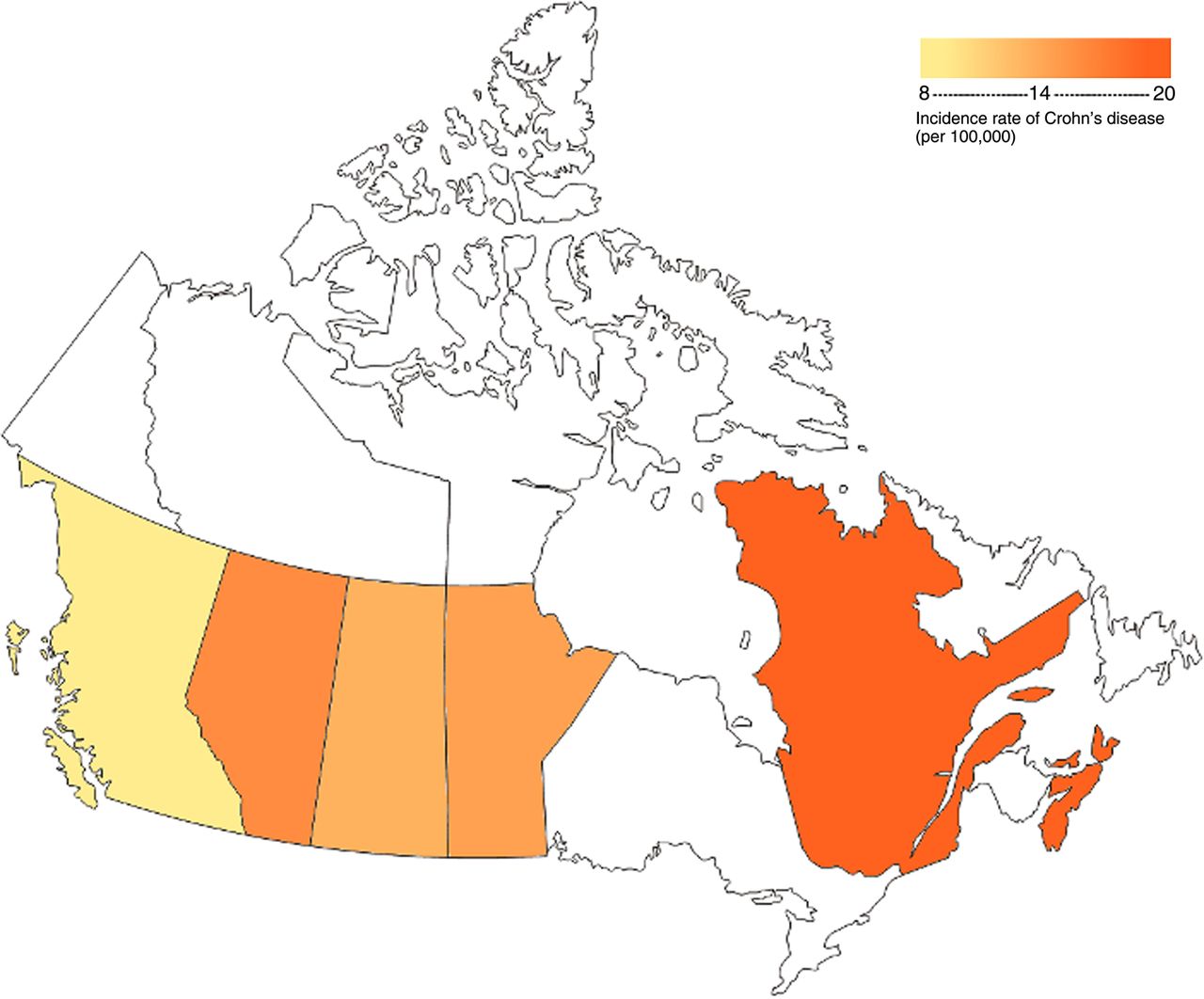
In the USA, a north–south gradient has been shown by hospital-based registrations,35 ,36 whereas in Canada, a nationwide comparison demonstrated an east–west disease gradient.37 Northern Canada is more sparsely populated than southern Canada, and its population is overrepresented by ethnic groups such as Canadian First Nations with low incidence rates of IBD,37 and thus there is a south–north gradient within Canada. The high rates in Canada and the northern USA relative to lower rates in southern USA, Mexico and Central America do suggest a north–south gradient in the western hemisphere. This gradient probably reflects differences in environmental exposure and not genetic factors.
Figure 3 shows a north-to-south disease gradient for UC in Spain and figure 4 shows an east-to-west disease gradient for CD within Canada.

Variation of incidence rates for ulcerative colitis within Spain showing a north–south disease gradient (generated from data in supplementary appendix 1, available online only). This figure is only reproduced in colour in the online version.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Variation of incidence rates for Crohn's disease within Canada showing an east–west disease gradient (generated from data in supplementary appendix 2, available online only). This figure is only reproduced in colour in the online version.
Changing epidemiology over time
The incidence of IBD is increasing with time and in different regions around the world. In the past 50 years, the incidence rate of UC first increased then stabilised or even decreased while that of CD has continued to increase. More recent data showed that the incidence rate of CD in adults in Europe has stabilised. However, temporal trends showed that the incidence of CD in Europe is still rising due to paediatric CD.38 For example, in northern France, the CD incidence rate has increased by 71% in the 10–19-year-old age group between 1988 and 2007.39
Traditionally considered an area of low incidence, Asia is witnessing a rise in incidence in parallel with rapid socioeconomic development.40–43 Recent data showed significantly higher rates in Asian populations, and time trend studies from Japan, Korea and Hong Kong have reported an increase in incidence rates of UC and a similar but lower rise in CD.4 In Japan, the prevalence of CD has risen rapidly from 2.9 cases per 100 000 persons in 1986 to 13.5 per 100 000 in 1998,44 whereas in South Korea the prevalence of UC has quadrupled from 7.6 per 100 000 in 1997 to 30.9 per 100 000 in 2005.2 In Hong Kong, the prevalence of UC almost tripled from 2.3 in 1997 to 6.3 per 100 000 over a 9-year period.45 In Singapore, the prevalence of CD increased from 1.3 in 1990 to 7.2 per 100 000 in 2004.46 In China, the number of cases of UC has increased by fourfold between 1981–90 and 1991–2000.47 There are no published studies comparing incidence rates or prevalence figures between different regions of the Asia-Pacific area. Challenges in the Asia-Pacific region include difficulty in defining catchment areas and the lack of uniform criteria for case ascertainment. Much of the aforementioned data are hospital based, and so there is a bias in terms of assessing only those populations that access the hospitals under study. Even within Asia incidence rates and prevalence of IBD vary according to geography and ethnic groups. The highest rates have been reported in India (particularly of UC), Japan and the Middle East, whereas overall rising trends of IBD are seen in east Asia. Rates of IBD appear to be higher in urban than in rural communities. In Turkey, the prevalence of UC was significantly lower in rural (2.2 per 100 000) than urban areas (5.9 per 100 000).48 Unlike Europe and North America, there are no data for a north–south or an east–west divide in the Asia-Pacific region. There is also a lack of population-based studies evaluating race or ethnicity in developing nations, although there is some suggestion that certain ethnic groups such as Indians are more susceptible to UC compared with Chinese or native Malay within the same country.49 ,50 The differences between ethnicities within one country may reflect differences in genetic susceptibility, living conditions and/or diet.51
In summary, there appears to be a north–south gradient of disease incidence in the Americas, with less of one in Europe in recent years. Some of the highest incidence rates of IBD occur in southern Australia and New Zealand.11 ,12 The east–west gradient that has evolved in Europe may be either a real phenomenon or simply a product of evolving healthcare systems and case ascertainment in eastern European countries; the reasons behind these regional differences are far from clear cut. Other data on intracontinental differences of IBD in general are few, and mostly based on results from a single country. Standardised population-based data of comparisons between the east and west of Europe as part of the European Crohn's and Colitis Organisation (EpiCOM (Epidemiologic Committee) Study) and between 10 countries within the Asia-Pacific region (Asia-Pacific Crohn's and Colitis Epidemiology Study) are in progress. Previously believed to occur less frequently among non-Caucasian compared with Caucasian populations, IBD is increasing in these populations, particularly in African Americans and Asians. Epidemiological data from migrant populations indicate that environmental factors contribute to the risk of IBD; first and second-generation migrants were at similar risk.5
Relationship between UC and CD
In addition to variations between countries and regions in the incidence and prevalence of IBD, the ratio between UC and CD also shows geographical variations. Compared to the rest of Europe,13 ,52 ,53 a higher incidence rate for UC than for CD has been reported in Nordic countries.14 ,21 ,54 The reason for this is not completely clear. In Canada and the USA,8 recent incidence rates suggest that CD is the more predominant disease, although in some North American studies the prevalence of UC is still greater than CD. The variation in ratios of UC and CD between countries and regions might reflect differences in environmental risk factors, but genetic predispositions may also play a role. In Europe, the incidence of NOD2 mutations appears to be highest in the middle part of Europe, which corresponds with regions where there is a higher CD to UC ratio.55 Interestingly, the CD to UC ratio is close to 1 : 1 in some of the eastern European countries with high IBD incidence; indeed, CD was even surpassing UC in some of the countries such as Croatia.16 ,17
In developing countries, the UC incidence increases first, followed by a rise in CD incidence.8 Reports from Asia have described a decrease in the ratio of UC to CD over time.4 In China the ratio of UC to CD has dropped from 41 to 15, whereas in Korea this has dropped from 6.8 to 2.3 in the past 20 years.56 This temporal trend suggests that CD and UC have both common and distinct risk factors. The former might explain the rise in both diseases with socioeconomic development, the latter might explain the time lag between increased incidence in UC followed by CD.
Environmental factors
It stands to reason that the driving forces behind the rise of IBD in developing nations are environmental factors, as these nations have undergone tremendous economic and social growth. The second part of this review focuses on the impact of known environmental factors on the geographical variation in IBD incidence. The two most well-established risk factors for IBD, smoking and appendectomy, cannot fully account for all variations in IBD incidence and prevalence. For instance, the incidence rate of CD is high in some populations with a relatively low prevalence of adult smokers (Sweden, Canada), and is low in populations of heavy smokers (Asia, Africa). Appendectomy also cannot explain the worldwide incidence of UC; rates of appendectomies have decreased in developed countries, whereas the incidence of UC has remained constant or even decreased. By far the most topical and likely factors that may explain geographical variability and the rising incidence in developing countries and urban areas are differences in diet, with downstream effects on the intestinal microbiota, exposure to sunlight or temperature differences, improving socioeconomic status and hygiene, which in isolation or even combination could account for variations and emerging trends in IBD epidemiology worldwide.
Smoking
In the west, smoking represents one of the most consistently reported risk factors for CD in case–control studies and in a meta-analysis.57–59 The magnitude of the risk (OR) for developing CD ranges between 1.5 and 2.0 in most studies. The association between smoking and IBD, however, may not be applicable to all ethnic groups or geographical regions for a number of reasons. First of all, smoking may not account for the worldwide trends in disease incidence. Of note, a possible explanation of this phenomenon may be at least partly the differences in the hygiene status and life expectancy. Conversely, countries with some of the lowest current smoking rates among adult male populations, such as Sweden and Canada, have among the highest incidence rates of CD. Approximately 20% of the adult male Swedish population are daily users of moist snuff (smokeless tobacco).60 In a large cohort study from Sweden, there was no significant association between the use of moist snuff and IBD.61 These data suggest that the link between smoking and IBD is mediated through airway exposure to non-nicotinic components of tobacco smoke. Second, in Israeli Jews who have a strong predisposition to IBD, smoking has not been associated with the development of CD.62 ,63 The smoking rates in the control Jewish population in Israel appeared lower than rates in other Caucasian studies (19.9–33% vs 30.9–56.2%),59 indicating that a high background smoking rate could not explain this lack of association. The disparity observed in the effects of smoking among Israeli Jews with CD compared to the non-Jewish white population may reflect a smaller role of smoking on the pathogenesis of CD in a population group with a strong genetic predisposition.59 It may be that smoking does not actually pose a risk for developing CD but modulates the disease, perhaps through a vascular effect, once the disease is present, facilitating the expression of disease. There are several studies that report that smokers have a more aggressive course of disease, including with earlier relapse rates of a medically or surgically induced remission.64
In CD, smoking may not play the same role in different ethnic groups as it does in western populations. One study in China was not able to demonstrate an association.65 In a cross-sectional observational study, there were fewer smokers among Chinese with CD in Hong Kong than Caucasians with CD in Melbourne, Australia.66 More studies are needed in Asia (a high smoking area) to determine the impact of smoking on the development and progression of CD and its association with disease phenotype. However, studies in Japan have shown a protective effect of smoking on UC,1 as has previously been shown in the west. One study showed that current smokers had a decreased risk of UC and former smokers had an increased risk.67 Similar findings have been reported in a case–control study from China.47
The effect of smoking in both UC and CD seems to be modulated by gender, with women being affected more disadvantageously than men.68 ,69 More recently, a time-dependent effect was also reported, suggesting that 4–5 years of smoke exposure may be associated with an altered risk of IBD.68 In contrast, the importance of smoking could not be confirmed in IBD patients with an elderly onset. Therefore, the effect of smoking in an individual may be the sum of the interplay of different host genetic and environmental factors (including smoking, non-steroidal anti-inflammatory drugs, or ultraviolet exposure from sunlight, etc). The mechanisms behind smoking and the onset of IBD remain unclear, but among siblings discordant for smoking, smokers had an increased risk of developing CD, whereas non-smokers tended to develop UC.70 This may suggest an interaction between smoking and genetic susceptibility or, as suggested above, that smoking is a modulating factor in those who present with the disease.
In summary, although tobacco smoking is the only environmental factor consistently predisposing to CD, there are no reliable data about the geographical distribution of tobacco smoking. It is likely that smoking does not cause CD but modulates the disease once present.
Meta-analyses confirmed that in Caucasian populations, smoking is an important environmental risk factor in IBD, with opposite effects on UC (OR 0.58) and CD (OR 1.76),59 whereas in other ethnic groups with different genetic susceptibility, smoking may play a lesser role. The reason why CD in Israeli Jews or Asians is not as sensitive to smoking as in other populations is not clear. Explanations might include differences in genetic and/or environmental factors (eg, type of tobacco, way of smoking or other dietary factors). Therefore, smoking may influence the course of CD but may not influence population trends of IBD. The biological mechanisms for the contrasting associations of smoking on UC and CD remain unknown, but microbial and immunological mechanisms are plausible, as smoking has immunosuppressive effects on T-lymphocyte function, which may lead to alterations in the gut microbiota. Smokeless tobacco has not been shown to increase the risk of CD, suggesting that the inhaled non-nicotinic components of cigarette smoke may be more important than nicotine itself in disease aetiology.
Appendectomy
The declining appendectomy rates in the past 15 years cannot account for the constant or decreasing incidence of UC in developed countries. In case–control and cohort studies from Europe and the Asia-Pacific region, appendectomy has been shown to be protective for the development of UC.71 ,72 In a large Swedish case–control study consisting of more than 200 000 patients who underwent appendectomy between 1964 and 1993, appendectomy before the age of 20 years for appendicitis or lymphadenitis (as opposed to abdominal pain or other causes) was associated with a lower risk of developing UC.71 In contrast, appendectomy without confirmed appendicitis was not associated with a protective effect.
Several studies from Asia have reported a similar protective effect of appendectomy against UC, with OR ranging from 0.11 to 0.38.47 ,73 ,74 In a Japanese multicentre study, UC patients diagnosed after appendectomy appeared to have more limited disease extent and fewer clinical relapses compared to patients with an intact appendix.73 Studies from France and Australia have demonstrated that UC patients who had undergone appendectomy before diagnosis were less likely to require immunosuppressive therapy75 or colectomy.75 ,76 In a meta-analysis of 13 case–control studies, appendectomy conferred a 69% risk reduction for the development of UC when smoking was controlled for.77
In contrast, the relationship between appendectomy and CD is less clear.78 Although several studies have demonstrated that appendectomy is a risk factor for the development of CD,11 ,79–83 others have either shown a protective effect75 or no association34 ,84–87 (table 1). A meta-analysis has demonstrated a significant risk of CD (relative risk (RR) 1.61) following an appendectomy, but heterogeneity was observed between studies.78 The risk was increased within the first year after surgery (RR 6.69), and at up to 4 years (RR 1.99), but after 5 years or more following an appendectomy, the risk dropped to baseline levels (RR 1.08).78 The increased risk of CD appeared to be higher in women than men, and in those with perforated appendicitis than non-perforated appendicitis.83 In a recent large Swedish–Danish population-based study, it appeared that diagnostic bias might account for the observed association between CD and appendectomy88 as the increased risk of CD within the first year after an appendectomy reduced significantly after 5 years, possibly reflecting a misdiagnosis of patients with incipient CD.78 There is currently no published study on the association of appendectomy and CD in Asia, Africa or eastern Europe.
Studies of appendectomy and the risk of CD from selected geographical regions
In countries where there is an excess of CD compared with UC, such as France, it has been hypothesised that a high rate of appendectomies may account for this discrepancy.22 The appendectomy rate in France was at least three times higher than that observed in other European countries or in the USA.
In summary, despite some variation, the literature overall suggests a protective effect of previous appendectomy with confirmed appendicitis (reduction of 13–26%), particularly at a young age, and the development of UC across different geographical regions and populations, and a modest association with the development of CD. The inverse association with UC may be a causal one because it is not related to surgery for non-specific abdominal pain. The mechanism by which appendectomy protects against the development of UC but increases the risk of CD is not known; proposed hypotheses include alterations in mucosal immune responses that lead to appendicitis or, as a result of appendectomy, negatively impact on the pathogenetic mechanisms of UC.89–91 The appendix may act as a reservoir of enteric bacteria involved in antigen sampling that regulates the immunological response to host microflora.89 ,91 ,92 It would appear that this proposed mechanism may apply to worldwide populations.
Dietary influence on IBD
Global variation in dietary habits probably explains the differences in the risk of IBD across geographical regions and the increase in disease incidence in migrant and developing populations. However, the effect of diet on the risk and clinical course of IBD has not received as much research attention as is probably warranted. This is because the sheer numbers of possible dietary exposures, and their interactions with host factors such as genetics and the microbiome make the identification of dietary risk factors for IBD a challenging and formidable task. The foods we eat contain macronutrients, micronutrients, additives, pollutants and caloric content of variable concentration; and the water we drink varies in the amount of trace elements, microorganisms and organic and inorganic compounds.
The rates of IBD increased steadily in Europe and the USA from 1940 to 1960, and in Asia in the early 1990s. The rising rates coincided with the introduction and expansion of fast food chains, packaged food, increased use of antibiotics and aluminum foils. In an ecological study from Japan the increased incidence of CD correlated closely with the increased intake of animal protein and dietary fat, especially n-6 fatty acids and a decreased intake of n-3 fatty acids.93 With the absence of NOD2 mutations,94 the increasing incidence and prevalence of CD in Japan is likely to be accounted for by dietary changes. In a retrospective study from Japan performed within 3 years after diagnosis, a higher consumption of sweets was positively associated with UC risk, whereas the consumption of sugars, sweets, fats, oils, fish and shellfish was positively associated with CD risk.95
The difference in the incidence of CD in the north and south of France could also be accounted for by differences in exposure to dietary components.96 Individuals living in the south of France generally consume a diet that is richer in fruit, vegetables, fish, olive oil and wine (dietary factors that have been shown to be associated with a reduced risk of IBD), whereas those in the northern regions consume more butter, eggs, potatoes, sausage, ham and beer.97
In studies from Europe, the most consistent dietary association linked to the development of IBD, particularly for CD, is increased sugar intake98–102 (table 2). A population-based case–control study from The Netherlands showed that cola drinks and chocolate are potential risk factors for IBD.103 A second key dietary factor might be animal protein.104 ,105 The European Prospective Investigation into Cancer and Nutrition, consisting of more than 200 000 subjects across five European countries, showed that an increased intake of linoleic acid (n-6 fatty acid; particularly high in red meat, cooking oils and polyunsaturated margarine) more than doubled the risk of developing UC (OR 2.49).104 The time point at which dietary factors impacted on disease evolution, however, could not be derived from the study.104 In a large French prospective questionnaire cohort study of women aged 40–65 years, a high total protein intake, specifically animal protein, before disease onset was associated with an increased risk of IBD.105 These data are consistent with an earlier Swedish population-based case–control study showing that the consumption of ‘fast food‘ was associated with an increase in UC (OR 3.9) and CD (OR 3.4).106 Conversely, intake of dietary fibre, fruit and vegetables has been reported to be protective for both CD and UC,95 ,107 although results vary between studies.102 ,103 ,106 The main difficulty with dietary studies is understanding the timing of dietary intake in relation to disease. Is it more critical to assess childhood diet, or perhaps the diet taken within 5 years of diagnosis? Studies that survey subjects after diagnosis are confounded by recall bias issues and the probability that people will change their diets once symptoms have begun. Of patients not changing their diet, a high consumption of red meat and cheese was associated with CD, while a high consumption of margarine was associated with UC.108
Studies on diet and the risk of IBD
One of the factors associated with westernisation of diet includes urbanisation. The incidence of UC appeared to rise rapidly in relation to urbanisation. This has been observed in several developing countries, while the number of patients with CD remained low or increased with a delay of 15 years compared to UC.109 It could well be that changes in lifestyle factors including diet affect UC risk more than CD, as reflected in increased incidence, years before CD risk is affected.
Using data from a population-based cohort in Norway and a registry of water quality, the risk of developing IBD was associated with high iron content. The RR of developing IBD increased by 21% when the iron content in the drinking water increased by 0.1 mg/l. A high iron concentration may work as a catalyst for oxidative stress, resulting in inflammation, or may stimulate the growth of bacteria, thus increasing the likelihood of inappropriate immune responses in genetically predisposed individuals.110
In summary, dietary antigens very likely play a role in the expression of IBD. Prospective studies suggest that a diet high in protein, particularly animal protein, is associated with a higher risk of IBD. Intake of the n-6 polyunsaturated fatty acid linoleic acid may confer risk, whereas n-3 polyunsaturated fatty acids may be protective for UC.111 No prospective data have been reported on risk related to the intake of fruits, vegetables or food microparticles on UC or CD development. However, despite an increasing number of studies examining the association between diet and IBD, no causal food item has been identified and no consensus has been reached, partly because results from studies remain difficult to interpret, and in some, findings were not reproducible. Methodology limitations include recall bias for presymptomatic food intake and the possibility of alteration of diet because of symptoms before a formal diagnosis of IBD. Based on epidemiological data and case–control series, the relationships between changes in food consumption would fit, in a timely manner, with changes in microbiota associated with IBD. With ongoing observation of existing cohorts and the development of population-based cohorts, more data on dietary risk factors may be expected during the coming years. Such data may benefit from considering interactions between the gut microbiota and any confirmed dietary factors.
Environmental effects on microbiota
Dysbiosis reported in IBD is likely to be a consequence of changes in environment including hygiene and food, resulting in an imbalance in the microbial–host relationship with mucosal barrier dysfunction and reduced microbial diversity.112 Dysbiosis with a decrease in beneficial bacteria, such as the Bifidobacteria, Lactobacilli, Bacteroides and Firmicutes,113 and an increase in pathogenic bacteria, such as adherent invasive Escherichia coli (AIEC)114–116 and Mycobacterium avium paratuberculosis ssp (MAP),117 ,118 have been reported in IBD. Little is known about how diet affects the microbiome. It has been postulated that dietary fructose, sucrose, animal fat and iron preferentially stimulate the growth of pathogenic bacteria, while poorly absorbed oligosaccharides promote the growth and metabolic profile of beneficial bacteria.
It remains controversial whether primary pathogens such as MAP, which causes Johne's disease in cattle,117 may be an aetiological factor for CD, but problems related to diagnosing the infection and having a biomarker of its presence remain a key obstacle to either moving this hypothesis forward or fully eliminating it. Clinical studies up to now have been inconclusive with regard to the impact of MAP in IBD. Several studies have detected a high prevalence of MAP in CD patients, and a meta-analysis of 28 case–control studies showed a positive association, both for enzyme-linked immunosorbent assays and PCR.118 A recent study,119 however, performed with highly sensitive methods in the intestinal mucosa, failed to detect the presence of MAP in newly diagnosed, treatment-naive cases, in contrast to many affected cases among hospitalised CD patients on treatment, within the same catchment area. MAP was not found among patients with long-standing UC. A study of seropositivity showed a high seroprevalence for Manitobans at approximately 35%, but failed to demonstrate a difference between CD, UC and controls.120 Furthermore, no interaction between the NOD2 genotype and MAP serology in relation to CD or UC has been identified.121 Whether seropositivity reflects past infection in humans is unknown. Based on these data, MAP is probably not an aetiological factor. It may be a bystander appearing during the course of disease, or it could be that MAP is a permissive infection (for instance, impacting on macrophage function) facilitating the pathogenicity of a second organism.122
The high prevalence of AIEC associated with ileal CD represents another potential primary pathogenic strain of bacteria.115 ,123 ,124 Colonisation leads to strong inflammatory responses in the gut suggesting that AIEC could play a role in CD immunopathogenesis. Furthermore, the presence of AIEC in the mucosa of patients with CD at initial diagnosis suggests that they may play a role in the early stages of disease onset.125 In France, it was found that AIEC reference strain LF82 was able to adhere to intestinal epithelial cells, to invade epithelial cells and to survive and replicate within macrophages,126 ,127 whereas in Canada other strains of AIEC including UM146 and UM147 that produce an increase in serine proteases have been reported.116 ,128 Much of the work on this organism, and its potential role in CD, has been undertaken in areas of high CD incidence. The significance of this pathogen in the pathogenesis of CD worldwide is currently unknown. It is not clear whether AIEC is a pathogen worldwide or is restricted to some countries. Characterising AIEC in low but increasing incidence, and high incidence countries and different ethnic populations may allow the identification of specific causal factors in the microbiota. These data can potentially provide an insight into the relevance and role of AIEC in the global epidemiology of CD.
The ‘hygiene hypothesis‘ postulates that individuals raised in a sanitary environment are more likely to develop IBD. This hypothesis implies that the increasing frequency of immunological disorders can be attributed to the lack of childhood exposure to enteric pathogens, or alternatively to the loss of saprophytic microorganisms that may impact on regulatory T-cell development. In support of the hygiene hypothesis are the generally negative associations with the epidemiology of Helicobacter pylori129 and the inverse association to the prevalence of helminthic colonisation.130 ,131 Although Canada has one of the highest rates of IBD in the world, the low rates of IBD among First Nations Manitobans could be explained by the hygiene hypothesis. Many of the Manitoban First Nations live in crowded and poor conditions, and are infected with pinworms, hepatitis A and H pylori.
The suggested ‘cold chain hypothesis‘ represents a more direct explanation of a causal relationship between specific bacteria and the immunocompromised host, and originated from a molecular perspective postulating that CD is a result of a defect in the host recognition of pathogenic bacterial components that usually escape the immune response leading to an excessive host response to bacteria, such as Yersinia spp and Listeria spp, which can survive refrigerator temperatures.132 The definition relies on the introduction of refrigeration in society, which was related to the time of the rising incidence of CD. Case–control studies have supported this hypothesis, in combination with other socioeconomic risk factors.133 ,134
As IBD is most common in the northern hemisphere, most studies with regard to microbial risk factors have been performed in this region. While one might speculate that an improvement in sanitary conditions is responsible for reduced microbial diversity, industrial pollution in society might serve as another explanation for a changed environment. It is unlikely that the exogenous predisposition to IBD can be explained by one single environmental factor. At the moment, our knowledge regarding possible risk factors derived from industrialisation must be divided mainly into primary direct effects of endogenous dysbiosis as some risk factors may act earlier than dysbiosis and secondary effects on this microbial imbalance. The latter explanation will include all the risk factors that will either increase the microbial instability or increase the vulnerability of the host organism.
Infectious agents causing an episode of infectious gastroenteritis may play a role in the initiation and/or exacerbation of IBD. Several studies have shown that acute gastrointestinal infections135–137 are associated with the development of IBD, especially with Campylobacter and Salmonella, with an OR of 4.1 in the first year after infection when compared with unexposed controls. The risk of developing IBD was significantly higher among 13 148 patients exposed to Salmonella or Campylobacter gastroenteritis than among 26 216 control patients.137 In a study assessing the incidence of positive and negative stool tests among patients already diagnosed with IBD, the findings of high incidence rate ratios (IRR) for IBD the first year after both positive (IRR 5.4–9.8) and negative (IRR 53.2–57.5) stool tests suggest that increased rates of stool testing of patients with unclear gastrointestinal symptoms may lead to detection bias.138 In a study from Maryland using a military database, an episode of gastroenteritis increased the risk of IBD with an OR of 1.40. The risk was slightly higher for CD compared with UC.135
No evidence for causation of IBD by a single agent has been identified, whereas a number of microbes have been strongly associated with the presence of disease. Many of the features of a modern lifestyle observed in developing countries, including changes in domestic hygiene, family size, birth order, antibiotic usage, crowding and parasitism may be proxy markers of microbial exposure during childhood.130 Alterations in the gut microbiota could also be linked with a westernisation of diet, increased stress levels and obesity.3 New emphasis has also been placed on common viral infections as important environmental factors in the pathogenesis of IBD, and studies investigating the host interactions with the human virome in IBD are warranted.139
Antibiotics
The composition of the intestinal microbiota has been proposed as an important factor in the development of IBD. Antibiotics have the potential to alter the composition of the intestinal microflora, especially during the first year of life, as this is the period of stabilisation for commensal gut flora in the newborn.140 In a retrospective case–control study, Shaw et al141 showed a significant association between antibiotic use in the first year of life and the development of IBD, with an OR of 2.9 (95% CI 1.2 to 7.0) for all IBD and 5.3 (95% CI 1.6 to 17.4) for CD. In the recent nationwide Danish prospective cohort study in children, the RR of IBD was 1.84 for antibiotic users compared with non-users. This association appeared to be higher for CD (RR 3.41) and was strongest in the first 3 months following use (RR 4.43) and among children with seven or more courses of antibiotics (RR 7.32).142 The observation that antibiotic use was not associated with the onset of UC was an important negative finding, and supports the idea that CD and UC are two separate diseases with distinct pathogenic mechanisms. Two studies have shown that the use of antibiotics and the development of CD affects boys more than girls.141 ,143 No correlation could be firmly assessed between the type of antibiotics and the development of IBD. Only tetracycline and cephalosporins have been correlated with IBD.141 ,143 A recent study reported an association with antibiotic use 2–5 years before the diagnosis of IBD in adults.144 A dose–response effect of antibiotics has been reported in a study from the UK whereby the receipt of more than two antibiotic courses in childhood was more highly associated with the development of IBD than one to two courses of antibiotics.145
Although cumulative data suggest a possible triggering role of antibiotics in the onset of IBD, as with any observational study, causality or biological mechanisms cannot be inferred from these results.142 Methodological limitations also need to be addressed. In all studies, data were collected retrospectively from databases registering prescriptions or from questionnaires. Recall bias, particularly in controls who may hardly recall having used antibiotics (being otherwise healthy) could lead to an underestimation of antibiotic use in the controls. Nonetheless, these data support the hypothesis that alteration of gut microbiota by antibiotics in early childhood as the immune responses are becoming established or while the gut microbiome is becoming established may trigger CD. Alternatively, factors that necessitate the early need for antibiotics are also contributing to the development of IBD. It may also explain the dramatic increase in the incidence of childhood CD in recent years. For example, in Denmark the incidence of paediatric IBD has increased 15-fold in the past 30 years,146 whereas in Norway, there has been a marked rise in the incidence of childhood CD in contrast to no increase in UC compared with the figures from the past 15 years.147 ,148 Unlike many other environmental factors, antibiotic use can rapidly change the spectrum of bacterial species and composition in the gastrointestinal tract, and thus explain rapid changes in disease incidence in the paediatric population or in developing nations. However, it is unclear whether the effect of antibiotics on the microbiota is long-lasting, and the importance of transient changes on the microbiota remains questionable.
In summary, at least nine observational studies have shown an association between antibiotic use and the subsequent diagnosis of IBD, whether they were taken in early infancy, childhood or at any time before IBD diagnosis141–144 149–153 (table 3). It has been hypothesised that an imbalance in normal gut microbiota, due to antibiotic use, might have a sustained effect on gastrointestinal immune tolerance and sensitivity to pathogens, possibly favouring the onset of IBD. Alternatively, antibiotic use might be a surrogate marker for infectious processes leading to IBD, for instance the prescribing of antibiotics to children with intestinal symptoms of as yet undiagnosed CD could be one explanation. Studies investigating antibiotic use in developing countries are important to explore whether this is a contributing factor to the rising incidence.
Studies on association of antibiotics and IBD development
In a recent large prospective cohort study, the frequent use of non-steroidal anti-inflammatory drugs appeared to be associated with the increased absolute incidence of CD (HR 1.59) and UC (HR 1.87).154
Socioeconomic factors
Socioeconomic factors may be responsible for the variation in the occurrence of IBD reported worldwide. Several studies have reported on the increased incidence of both UC and CD in more densely populated areas.155 ,156 ,24 In a case–control study from Sweden, perinatal health events and infants from families with low socioeconomic status independently increased the risk of IBD,155 while a population-based study from Israel showed that surrogate markers of enhanced childhood hygiene were associated with the risk of IBD, including living in an urban environment (OR 1.38), small number of siblings in the family (for one sibling vs five or more, OR 2.63), and higher birth order (for birth order of five or higher vs one, OR 2.35).156 In a recent meta-analysis, living in urban environmental was associated with an increased risk of CD and UC.33
Further studies among German employees suggested that work in the open air and physical exercise were protective, while being exposed to air conditioned, artificial working conditions or extending and irregular shift working increased the risk of IBD.157 In population-based studies in Norway, the incidence of IBD was higher in rural areas with a recent increase in socioeconomic status, based on years of education, compared to urban areas with a stable high socioeconomic level.31 In an epidemiological study in the UK, the availability of a fixed hot water supply in childhood before the age of 11 years was associated with CD.34
Environmental exposures in early life have been implicated in the aetiology of IBD. Siblings have been used as proxy markers to characterise patterns of exposure relevant to the risk of IBD.
In a case–control study from the Swedish In-patient Register, both family size and the number of older siblings, as well as birth order, were related to the increased risk of UC, and with smaller families and few older siblings related to CD,158 which might be a sign that UC is more directly affected by environmental factors than CD. This explanation was also supported by a shorter interval between first-degree relatives acquiring UC compared to CD.159 The relationships between IBD and other household-related conditions, such as pets, are unclear.160–163 Overall, as IBD emerged in the developed world, it was considered a disease of higher socioeconomic standard of living; however, as reviewed this is not a uniform finding.
The greater environment
One underexplored area in relation to IBD is that of the greater environment, such as sun exposure, soil, climate or temperature change and air pollution,164 which may explain geographical variation. Studies from Europe suggest that low sunlight exposure may contribute to the pathogenesis of IBD, although the exact mechanism for this is not clear. It has been hypothesised that people in sunnier states may have higher exposure to ultraviolet light, leading to higher vitamin D levels, which help to regulate immunity and inflammation. A link between latitude and incidence rates of CD and UC has been supported by a large prospective study from the USA.165 By tracking the location and lifestyle information of approximately 175 000 female American nurses biennially over 20 years, the authors detected a greater increase in the incidence rates of CD and UC the further subjects lived from the equator. At age 30 years, living in southern latitudes was associated with a roughly halved risk of developing CD and approximately a 40% reduced risk of developing UC. In that study, most of the patients developed CD in their late 40s or early 50s, suggesting that latitude may play an important role in relatively late-onset CD. The results are consistent with European studies linking latitude with the development of IBD. This hypothesis also reconciles with the comparably high incidence rates of CD in Canada and in New Zealand,11 but does not reconcile with the increasing incidence in other counties such as India. The relationship between IBD and latitude might also be explained by changes in sunlight exposure and vitamin D. A protective effect of vitamin D on the risk of CD has been reported. Women with a higher level of vitamin D had a significantly reduced risk of CD (HR 0.38).166
In addition, temperature might represent the sole mechanistic explanation leading directly or indirectly to a change of microbiota. Latitude differences have also been described for other immune-mediated diseases, especially multiple sclerosis.167
Another environmental explanation for the north–south gradient could be exposure to the sun. In a geographical study from France using the national health insurance database, incidence rates of CD and UC were estimated for each of the 94 French administrative areas between 2000 and 2002. Low sunlight exposure was associated with an increased incidence of CD with no association with UC. Further studies are needed to determine if this association is causal.96
Based on these observations, the relationship between seasonal environmental risk factors may affect the outbreak of IBD differently according to the occurrence of risk factors around the world. Large nationwide studies might dilute important local variations, which might seem negligible when the results are not broken down into smaller regions, such as communities.168
Oral contraceptives
Several case–control and cohort studies from the USA and UK involving more than 80 000 women have reported an increased risk of CD169–171 following the use of oral contraception.172 ,173 In addition, studies have suggested that the risk of CD increased with the length of exposure to oral contraceptives.172 ,174–176 An earlier meta-analysis177 pooling the results of seven case–control and two cohort studies showed an OR of 1.4 for CD after adjusting for smoking among oral contraception users. A recent meta-analysis of 14 studies reported on a positive association between the use of oral contraceptives and both UC and CD,176 with a reduced effect on discontinuation. The pooled RR for CD and UC for women currently taking oral contraception was 1.46 (95% CI 1.26 to 1.70) and 1.28 (95% CI 1.06 to 1.54), respectively, after adjusting for smoking. Overall, there appears to be a modest association between oral contraceptive use and IBD, but the mechanisms for this link is not known.
Perinatal factors and vaccinations
Disease expression has been proposed to be influenced by early childhood events such as mode of feeding, domestic hygiene, perinatal infections or immunisations. Whether breastfeeding protects against the development of IBD remains unclear. While several studies have shown a protective effect of breastfeeding, others have shown no such association.173 ,178 A meta-analysis of 14 case–control studies showed that breastfeeding protects against CD and UC;179 this protective effect appeared to be greater in CD than UC,180 and may be modulated via the microbiota. The hypothesis that a paramyxovirus such as measles or vaccination against such viruses might cause IBD remains controversial.181 Although an initial study showed that patients who received measles vaccination were two to three times more likely to develop IBD,182 subsequent case–control studies in different countries have not been able to reproduce similar findings.183–185 A population-based study from Manitoba showed no association between having acquired measles, mumps, or rubella (by natural infection or through vaccination) and CD or UC. Seropositivity for measles and mumps was similar in controls, CD and UC subjects.178 ,186 In fact, a protective effect was evident in those seropositive for rubella.
Future directions
Although a strong body of evidence supports the role of environmental influence in the development of IBD, identifying conclusive environmental risk factors has proved to be difficult. Inconsistent results between observational studies may partly relate to differences in study methodologies.187 IBD has also been studied rarely in the context of complex interactions between susceptibility genes and environmental exposure. First, methodological standardisation is necessary to produce consistent environmental associations in cohort and case–control studies. Second, appropriate analytical techniques are required to control for all known confounders and to adjust for multiple comparison errors. Third, patients should be stratified into homogenous phenotype–genotype populations. Finally, results need to be replicated in an independent cohort.
To explore environmental factors in IBD, lessons can be learned from studies of other chronic immune disorders.188 Studies that aim to assess the risk of IBD before disease onset will be informative. Multicentre prospective cohort studies that follow large numbers of healthy individuals and at-risk first-degree relatives with high-risk genotypes to a new diagnosis of IBD are required to determine environmental risk factors. These studies should assess biomarkers specific to preclinical IBD, infectious and non-infectious exposures (diet, toxins, vaccinations) at regular intervals. Similar studies have been conducted successfully to identify environmental triggers for diabetes mellitus and metabolic syndrome. In Europe (ORIGIN study) and Canada (Genetic Environmental, Microbial), two long-term prospective studies are enrolling large cohorts of high-risk asymptomatic individuals, assessing in parallel infections and antibiotic use with analysis of microbiota and its evolution over time until the development of IBD.
Studying diet is complex and studying infections often relies on surrogate markers. It also remains unclear whether one or several infectious agents should be sought. The food frequency questionnaire is the dominant tool in nutritional epidemiology but has limitations especially when applied retrospectively. The prospective collection of dietary record over a prolonged period of time is possible, as has been demonstrated by the Nurses Health Study. This is particularly important in developing nations in which westernisation of diet is evident. The north–south disease gradient for CD in France has highlighted the importance of prospective cohort studies investigating the effect of the ‘prudent diet‘ (rich in fruit, vegetables, fish, olive oil and wine) on CD development. The observation that the timing of the introduction of certain foods or chemicals to infants affects the risk of developing diabetic autoimmunity and coeliac disease is also likely to be relevant to IBD.
Future efforts should be focused on targeting at-risk populations. Populations optimal for studies include paediatric populations, muliplex families and nations of increasing rates of disease if important environmental factors are to be captured. There can be a long latency period from environmental exposure to preclinical biochemical changes, subclinical intestinal inflammation and eventually clinical disease. Studying environmental exposure from early childhood will be important. The rising incidence of CD in children in northern France suggests that studies on CD risk factors should focus on the population under 20 years of age.
In recent years, instead of looking at one environmental exposure or a class of exposures at a time, it is possible to use a broad-based assessment to study exposures, a concept known as ‘exposome‘.189 Two such approaches exist. The first, known as the ‘bottom-up‘ approach, is a strategy whereby external sources of an individual's exposome (eg, air, water, food) are measured at multiple time points using innovations in global information systems, remote sensing or personal sensing devices.190 ,191 An alternative approach, called the ‘top-down‘ approach, focuses on biomonitoring (eg, blood sampling) to assess the internal milieu, including using technologies such as proteomics, transcriptomics and metabonomics.190 With the accumulation of a growing number of signatures of environmental exposures, it may become possible to develop high-throughput, multiplex assays to register each person's environmental exposures. In diabetes, an environment-wide association study, in which epidemiological data are comprehensively and systematically interpreted in a manner analogous to a genome-wide association study, have revealed novel associations between type 2 diabetes and specific chemical agents.192 Currently, the National Institute of Environmental Health Sciences is focusing on comprehensive approaches to define environmental factors in human disease, and one of their initiatives relevant to IBD is an exposure biology programme aimed at developing a better measurement of exposure.188 The majority of chronic human diseases are accounted for by environmental exposures. Innovative approaches and strategies to identify and measure environmental risk factors in several chronic human diseases, not excluding IBD, will continue to be an area of intense discussion. Development of IBD-specific prospective cohorts, enhancements in data sharing of established IBD populations and improvements in our ability to measure environmental exposures will all aid in future studies of environmental triggers of IBD. Ultimately, collaborative efforts between international consortium groups of IBD from different countries provide the best chance of unearthing the clues to aetiology.
Conclusion
IBD has become a global disease. Accumulating data suggest that the increased frequency of IBD in the industrialised parts of the world is mainly explained by environmental risk factors. Compelling evidence suggests that gut microbes participate in an important way in disease pathogenesis. The relationship to latitude might be explained by changes in sunlight exposure and vitamin D. Which aspects of the environment impact to the greatest extent and whether the timing of such exposure throughout one's life is important remain unknown. Of all factors identified, not a single one alone may, up to now, totally explain the worldwide epidemiology of IBD. This is partly due to a multiplicity of potential routes for disturbances in the interactions between microbe and host. Some issues studied may not be factors in themselves but rather markers for other unidentified influences. It is highly likely that genetic influences critically determine the role that individual environmental factors may play in triggering disease. It is also possible that the strength of influence by risk factors or lack of protective factors in a society is different, depending on geography or urbanisation. Selecting unique populations to assess disease development, for instance in immigrants, the paediatric population or in nations with increasing rates of disease incidence, will be potentially rewarding.
Acknowledgments
The authors are grateful to Sunny Wong and Thomas Lam, Chinese University of Hong Kong, for assistance in the illustration and literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
Footnotes
-
Contributors All the authors contributed to the manuscript concept, design and revision. SCN was responsible for drafting the manuscript.
-
Competing interests SCN has acted as speaker for Ferring, Janssen and Abbott Pharmaceuticals; she has received research grants from Ferring and Janssen Hong Kong. CNB is supported in part by the Bingham chair in gastroenterology. In the past 2 years he has provided consultation to Abbott Canada, Janssen Canada, Shire Canada, Vertex Pharmaceuticals and Bristol Myers Squibb and has received a research grant from Abbott Canada and educational grants from Axcan Pharma and Aptalis. MHV has received contributions from Abbott, MSD, Ipsen Pharma, Novartis, Tillotts, Pfizer and Genetic Analysis in the past 2 years. PLL has acted as speaker for Abbott, Ferring and MSD. In the past 2 years he has provided consultation to Abbott Hungary, Ferring Hungary and MSD Hungary and has received unrestricted research grants from Abbott and MSD Hungary. EVL has received research support from Abbott Labs, UCB, Janssen Biotech, Shire, Bristol-Myers Squibb, GlaxoSmithKline, Amgen, Pfizer, Braintree and Millenium-Takeda, and has provided consultation for Abbott Labs, UCB, Bristol-Myers Squibb and Pfizer. CT has acted as speaker for Ferring, MSD, AstraZeneca and Shire. CO'M has unrestricted research grants from Abbott and MSD. BM has acted as speaker for Abbott, MSD, Ferring, Tillotts, Pharma Cosmos and Swedish Orphan in the past 2 years. In the past 2 years he has provided consultation to Abbott, Ferring and MSD and has received research grants from Ferring, MSD and Centocor. JFC has being a consultant and received speaker fees from Abbott Laboratories, Amgen, Biogen Idec Inc, Boehringer-Ingelheim, Bristol Meyers Squibb, Cellerix SL, Chemocentryx, Inc, Centocor, Cosmo Technologies, Ltd, Elan Pharmaceuticals, Inc, Genentech, Giuliani Spa, Given Imaging, Glaxo Smith Kline, Immune Pharmaceuticals Ltd, Merck & Co, Inc, Millenium Pharmaceuticals Inc, Neovacs SA, Ocerra Therapeutics, Inc (previously named Renovia, Inc), Pfizer Inc, Prometheus, Sanofi, Schering Plough Corp, Shire Pharmaceuticals, Synta Pharmaceutical Corp, Takeda, Teva Pharmaceuticals, and Petah Tikva, Therakos, TXcell, UCB Pharma (previously named Celltech Therapeutics, Ltd) and Wyeth Pharmaceuticals.
-
Provenance and peer review Not commissioned; externally peer reviewed.